
Abstract
Traumatic femoral shaft fractures distal to a hip resurfacing arthroplasty (HRA) are rare. Only four cases have been described in which an intramedullary nail was used to treat the fracture. We present the first case in the literature of a pathological femoral shaft fracture distal to a HRA, and describe its treatment with an anterograde intramedullary femoral nail with proximal locking screws placed into the femoral head overlapping the HRA stem. This demonstrates that the presence of a hip resurfacing arthroplasty does not preclude from utilising an intramedullary nail with recon screws to stabilise a pathological fracture.
Introduction
Hip resurfacing arthroplasty (HRA) was until recently a popular option used in the treatment of hip osteoarthritis, particularly in young active patients with high functional demands. 1 The components of HRA consist of highly polished cobalt chrome and the femoral component sits within the femoral neck preserving much of the bone stock lost in a traditional total hip replacement (THR). 2 HRA was previously popular as it avoided problems associated with THR such as loosening, volumetric wear and polyethylene debris, 3 and the large femoral head component of the HRA reduced the risk of dislocation particularly in younger patients. 3 Due to wear-related failures resulting in high metal ion levels and adverse local soft tissue reactions HRAs have become less popular than they were previously. 3 However, due to the large numbers of these prostheses implanted there are still common within the population.
Fractures of the proximal femur around an HRA are relatively common with an incidence of 0.5–4% reported.4–7 The majority of these are subcapital fractures related to an acute surgical complication, avascular necrosis or a delayed foreign body response to wear, but rarely there have also been intertrochanteric and femoral shaft fractures reported.
Pathological femur fractures are common. Bone is the third most common site for tumour metastases after the lungs and liver and up to 70% of patients suffering from malignant tumours develop bone metastases. The femur is one of the most commonly affected bones, and pathological fractures are a common complication of these malignant deposits. 8 There are a number of treatment options depending on the location within the bone, the extent of bone involved and the patients’ expected survival. Intramedullary nails are often favoured for intertrochanteric, subtrochanteric and diaphyseal fractures as they protect a long segment of bone, require only small areas of dissection and can provide rigid fixation using proximal and distal interlocking screws. 9
We describe the case of a patient with a HRA in situ who presented to our department with a pathological diaphyseal femoral fracture on the ipsilateral side to his HRA.
Case report
A 56-year old man was referred to our trauma unit following a stumble whilst an inpatient in an oncology ward. The patient did not fall to the ground, and there was no impact to his right femur during the incident. His past medical history included prostate cancer with known bony metastases and recently diagnosed small cell carcinoma with metastatic spread to bone, lungs and liver with known superior vena caval obstruction. His prostate cancer was diagnosed by biopsy 1 year prior to his fall with a subsequent bone scan demonstrating bony metastases of the vertebrae, anterior ribs, left scapula, left parietal skull, right SI joint and sternum. There were no signs or symptoms of femoral metastases at this stage, and there was no other imaging of his femur prior to his fall. He was treated with Bicalutamide hormone therapy 50 mg daily, without good response. Four months following diagnosis of prostate cancer the patient was admitted under the care of the general surgeons with colonic obstruction. At the time of laparotomy a liver lesion was noted, biopsied and determined to be metastatic small cell carcinoma of unknown origin. Subsequent radiological investigations during his palliative course revealed chest shadowing leaving the potential additional diagnosis of lung malignancy.
He had a right Birmingham Hip Resurfacing prosthesis (Smith & Nephew, London, UK) which had been implanted 8 years prior to this presentation (16/10/2006) for right hip osteoarthritis. The procedure was performed through an anterolateral approach and the patient had a routine follow up as standard for resurfacing arthroplasty in our unit with no issues of note. At his last orthopaedic clinic appointment 2 years prior to this presentation, he was mobilising without pain or walking aids and was independent with his activities of daily living and. Radiographs were satisfactory with no evidence of loosening or osteolysis, and Cobalt and Chrome ion levels were within normal limits.
Following the stumble, the patient complained of pain in his right leg and on examination his right leg was shortened and distally neurovascularly intact. Anteroposterior and lateral radiographs of the right femur revealed a fractured femoral shaft through a lytic femoral lesion (Figures 1 and 2). The closed fracture was stabilised in a Thomas splint and the patient was optimised for theatre. Surgical treatment was discussed with the patient and his family and informed consent was obtained.

Anteroposterior radiograph of the right femur following the stumble.
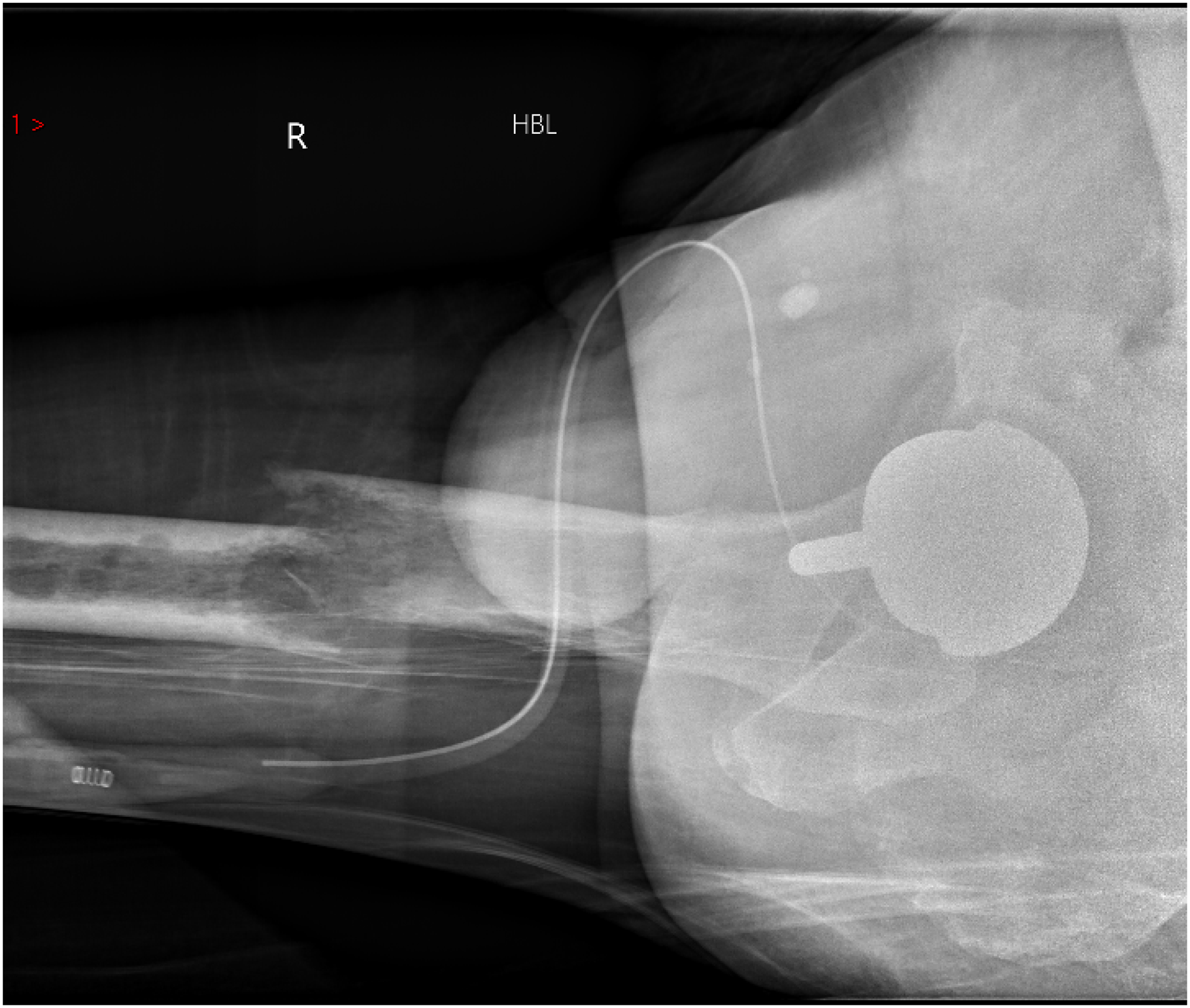
Lateral radiograph of the right femur following the stumble.
The patient underwent an anterograde femoral nail (Versa Nail, Biomet, Warsaw, Indiana, USA) two days following his fracture presentation. The fracture was reduced by the closed method on a traction table. A trochanteric entry point nail was used using a minimally invasive approach, as is normal practice within our unit. A trochanteric entry nail was used to keep the entry point away from the HRA stem and to avoid the increased hoop stresses associated with a piriformis nail. A recon nail was used to protect for undiagnosed weakness in the femoral neck, with the aim to overlap the proximal screws with the femoral stem to prevent a stress riser. Screw length was estimated by holding the measure over the anterior hip using X-Ray and extreme care was taken to avoid contacting the HRA when inserting the screws. Standard distal locking with two screws was performed as the screws are the weakest point of the construct and we anticipated possible delayed union due to the pathological nature of the fracture (Figures 3–6).

Anteroposterior radiograph of the proximal right femur following fixation.
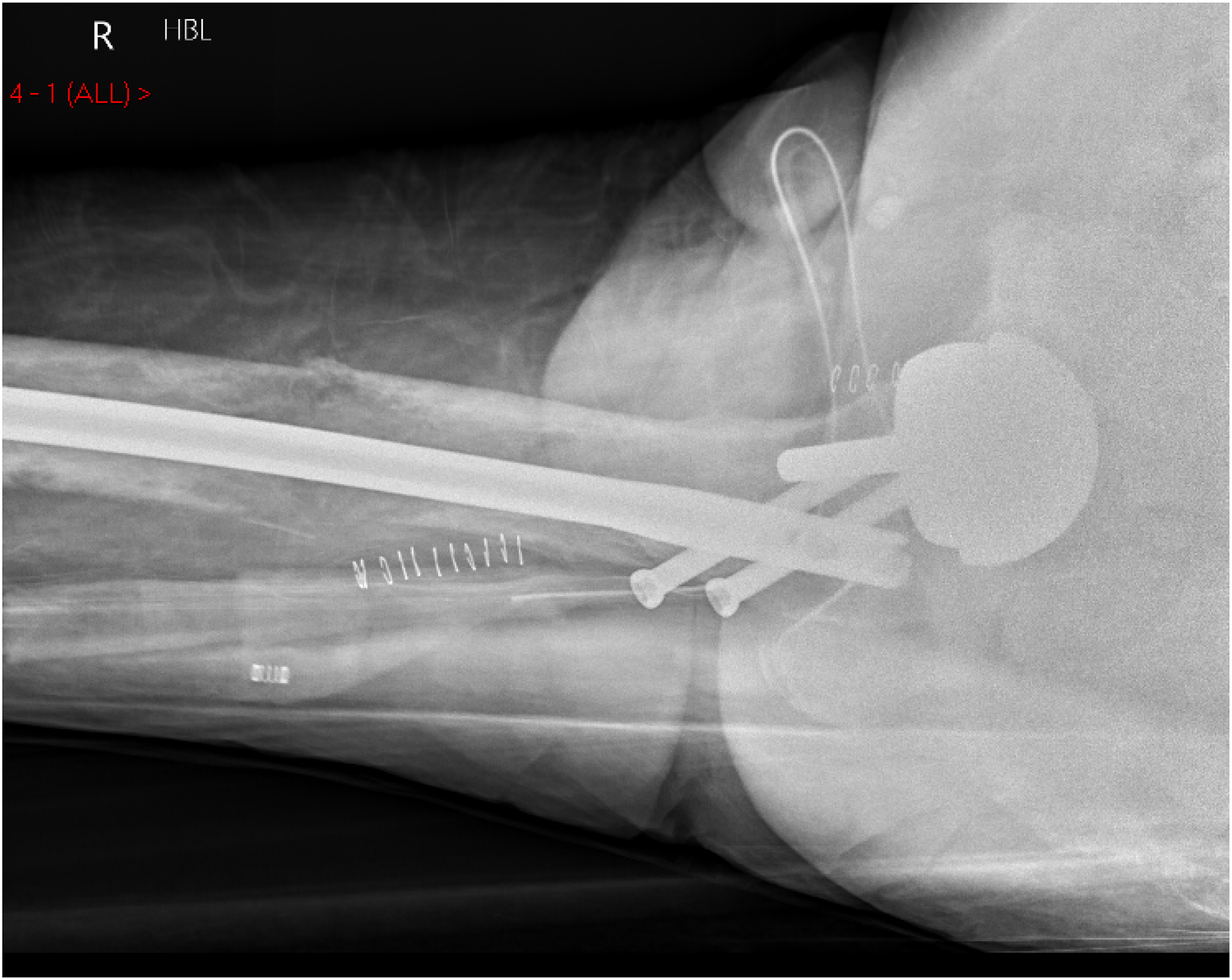
Lateral radiograph of the proximal right femur following fixation.

Anteroposterior radiograph of the distal right femur following fixation.

Lateral radiograph of the distal right femur following fixation.
Although minimal intraoperative blood loss was noted, post operatively the patient's haemoglobin fell to 79 g/l from 103 g/l preoperatively and he was subsequently transfused two units of packed red cells. Placement of the femoral nail significantly improved the patient's pain and he was then able to mobilise weight bearing as able on the ward using a walking frame post operatively. The patient's wounds healed and he had an otherwise uncomplicated recovery from an orthopaedic perspective. Samples of bone reamings taken at the time of nail insertion were consistent with his femoral lytic lesion being a small cell carcinoma metastatic deposit.
Unfortunately, the patient's systemic disease progressed over the next 6 weeks and he died after an episode of neutropenic sepsis following chemotherapy.
Discussion
Traumatic fractures to the femoral shaft in the presence of a HRA are rare, with only a few cases described in the literature. Pathological fractures to the femoral shaft in the presence of a HRA appear even rarer and we could identify no such cases in the literature.
A number of treatment options have been described for traumatic fractures including operative and non-operative approaches. The operative approaches include the use of an intramedullary nail,10,11 a femoral locking compression plate with or without cable systems and revision to a long stemmed THR. 12 In the case of a pathological fracture in the presence of a HRA it is important to consider that the pathological fracture is treated appropriately in addition to addressing the difficulty of managing the fracture in the presence of the HRA implant.
In our case, we elected to treat our patient using an anterograde trochanteric entry cephalomeduallary nail locked proximally and distally as this technique protected a long portion of metastatically infiltrated bone, provided rigid fixation allowing mobilisation, and required only minimal dissection. We were able to fix the implant proximally with screws into the femoral head despite the presence of the Birmingham Hip Resurfacing implant.
We were able to identify four cases described in with patients with a femoral fracture distal to a HRA were treated with an anterograde intramedullary nail. Two case reports described the treatment of femoral shaft fractures, and two described the treatment of intertrochanteric and pertrochanteric fractures. Bilkhu et al. 13 described a case in 2015 of a 72-year old female with a traumatic femoral shaft fracture in the presence of a Birmingham Hip Resurfacing. As in our case, they treated this with an anterograde, trochanteric entry point nail. However, they used a Stryker T2 (Stryker T2, Shonkirchen, Germany) intramedullary nail, rather than a recon nail, as we used to protect the femoral neck. Aning et al. 10 described the treatment of a 60-year old male with a resurfacing arthroplasty and femoral shaft fracture. As in our case, they used a reconstruction nail, but used a piriformis entry point rather than a trochanteric entry point entry nail, which we used to maximise the distance between our nail entry point and the tip of the HRA stem.
Choy et al. 9 described the treatment of a 51-year old male with an intertrochanteric fracture in the presence of a HRA using a Stryker T2 Recon (Stryker T2, Shonkirchen, Germany) nail. As in our case, they used an image intensifier to avoid contact between the proximal screws and the HRA stem, but they also used a more posterior entry point on the greater trochanter allowing eccentric placement of locking screws into the femoral neck. Peskun et al. 11 described two cases of males in their 40 s with HRAs, one with an intertrochanteric and one with a subtrochanteric fracture. Both patients were treated with a Gamma nail 2 (Stryker, Mahwah, NJ), rather than a recon nail, with a single lag screw through the nail into the femoral head. In both cases, the patients were instructed to mobilise touch weightbearing for several weeks postoperatively to protect their fixation. In our case, we mobilised our patient weightbearing as able to promote mobility which was especially important given his other comorbidities.
In conclusion, our case demonstrates the option of using an anterograde intramedullary femoral nail locked distally and proximally using locking screws placed into the femoral neck eccentric to HRA as an option for a femoral shaft fracture distal to a HRA. As stated above a small number of similar techniques have been described, but as far as we are aware no other case has been documented describing the treatment of a pathological femoral fracture distal to a HRA. As the population of patients with HRAs in situ become older this rare clinical problem is likely to become more common than it is currently. In cases of femoral fracture distal to a HRA it is important to protect the femoral neck to prevent femoral neck fracture after stabilisation of a shaft fracture, as this would have disastrous consequences. This is particularly important in cases of pathological fracture in which fracture healing is jeopardised by underlying pathology.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.