
Abstract
Introduction
Worldwide, with a trend of increased life expectancy, the incidence of hip fractures is projected to increase from 1.66m in 1990 to 6.26m by 2050. 1 Hip fractures have significant consequences: with mortality rates of up to 10% at 1 month and 30% at 1 year, as well as morbidity, with only approximately half returning to their previous mobility and 10–20% requiring discharge to nursing or residential care. 1 Due to the growing and rapidly ageing population, the absolute number of patients with hip fractures admitted to Singaporean hospitals per year increased from 1487 in 2000 to 2729 in 2017. 2
Ideally, hip fractures should be operated on within 48 h of admission, contingent on the surgery being able to proceed safely once patients are optimised, as this would allow patients to return to ambulation earlier and minimise complications of prolonged immobility. 3 Intra-capsular neck of femur (NOF) fractures make up almost half of proximal femur fractures in the elderly and patients usually undergo joint sacrificing surgery such as hemiarthroplasty (HA) or a total hip arthroplasty (THA). 4 HA is the most common treatment for NOF fractures worldwide3,5,6 and in our institution, though literature has described a faster post-operative return to function and better patient-reported outcomes in THA, in exchange for higher surgical morbidity and rates of dislocation.6,8
The NICE guidelines recommend using cemented implants with the rationale of less post-operative pain and reduced need for surgical revision. 9 Similarly, the American Academy of Orthopaedic Surgeons guidelines quote moderate evidence supporting the preferential use of cemented femoral stems, with the rationale that randomised controlled trials have largely failed to demonstrate differences, with the exception of fracture risk which appeared higher in non-cemented femoral stems. 20 However, proponents of uncemented techniques would cite the concern of bone cement implantation syndrome (BCIS) occurring in up to 25–30% of patients, with 5–7% of patients having severe BCIS, which is associated with higher early and late mortality as a reason for uncemented implants. 20
As the main goal of surgery for the elderly afflicted by an NOF fracture is to restore function and maintain quality of life, this paper seeks to compare the 3, 6 and 12 months mobility and quality-of-life outcome scores of cemented against uncemented HA for displaced NOF fractures, utilising the SF-36 20 physical and mental components, EQ5D score, 20 as well as the Parker mobility score (PMS). 20 There is currently a paucity of literature analysing mobility and quality-of-life outcomes comparing cemented and uncemented HA. Several studies claim that although cementing offers improved pain and faster recovery, it comes at the cost of increased operative timing, bleeding and complications.9,11 Our null hypothesis is that both cemented and uncemented bipolar HA give similar post-surgical mobility scores and quality-of-life indices.
Methods
This study was approved by the institutional review board of Singhealth (CIRB Ref: 2015/2134).
A retrospective review of collected registry data on HAs performed for NOF fractures in a tertiary institution between 2011 and 2019 was conducted. All patients were diagnosed as having NOF fractures based on standard anterior–posterior/lateral hip radiographs. Patients who had pathological fractures, bilateral hip surgeries, sustained other fractures within the same year or had incomplete 3, 6 and 12 months follow up were excluded; 308 patients remained in the dataset. From this dataset, 70 cemented HAs and 238 uncemented HAs were identified (Figure 1).

Patient selection flowchart nomenclature.
All patients underwent bipolar HA by either a consultant or a resident under the supervision of a consultant, performed via the posterior or lateral approach. Patients were placed in the lateral decubitus position prior to skin incision. After removal of the femoral head, sequential reaming of the femoral canal was performed. Subsequently, the femoral canal was sequentially broached until adequate axial and rotation stability was attained, without any evidence of broach movement within the canal. The trial femoral stem was then inserted together with the pre-determined, carefully measured trial bipolar head and neck prior to reduction of the hip to assess for stability and limb length discrepancy. Final implants were inserted using either a cemented or cementless technique before hip reduction and final stability, range of motion and limb length assessment.
The decision to cement was made pre-operatively by the consultant responsible for the case, based on a radiographic assessment of femur canal using Dorr classification. However, if the consultant deemed that the patient's bone stock was adequate or if the patient was deemed ‘high risk’ then an uncemented technique was utilised. At our institution, either Palacos + G: Antibiotic Loaded Bone Cement (Heraeus Kulzer Medical, USA) or Smartset GHV Gentamycin (DePuy Synthes, USA) was used. Cementing was performed using the fourth generation cementing technique with vacuum mixing, cement gun to achieve adequate pressurisation with femur canal preparation and use of centralizer.
Post-operatively all patients received an abduction pillow for the first 24 h . Patients underwent a standard post-operative rehabilitation protocol, which involved review by a musculoskeletal trained physiotherapist at post-operative day 1 to encourage early ambulation and mobilisation with full weight bearing as tolerated with or without the use of mobility aids such as walking frame or rollator frame after post-operative x-rays had been reviewed. Patients were also given a standard post-operative hip precaution advice to avoid hip flexion beyond 90°, to not cross their legs or squat and to avoid turning the operated leg inwards in a ‘pigeon toe position’.
All patients were evaluated at our institution's Orthopaedic Diagnostic Centre (ODC) and functional outcome measures were obtained by trained staff. The ODC is our clinical outcomes assessment unit, staffed with a team of independent assessors, consisting of allied health professionals such as physiotherapists and technologists, to perform and track post-operative clinical outcomes. For hip fracture patients, ODC performs a pre-fall assessment during the patient's hospitalisation, to document and score patient's functional and mental status prior to their fall.
Post-operatively, hip fracture patients are again assessed at 6 weeks, 3 months, 6 months and 12 months post-surgery at ODC, during specialist outpatient reviews, to determine functional recovery.
The primary mobility and quality-of-life outcomes were measured using the PMS, EQ5D and SF-36. The PMS is a validated scoring system that assesses a patient's mobility based on three main questions. (1) Is the patient able to get about the house? (2) Is the patient able to get out of the house? (3) Is the patient able to go shopping. 20 Each question is marked from 0 to 3 with a total of 9 points being given to the most mobile patients. 20 The PMS is a valid predictor of rehabilitation potential, 6-month functional outcomes and 1 year mortality. 20
The EQ5D (EuroQol Group, Rotterdam, Netherlands) is a well understood and extensively used health status instrument in the form of a self-completion questionnaire that assesses the quality of life through five health domains: (1) mobility, (2) capacity for self-care, (3) conduct of usual activities, (4) pain/discomfort and (5) anxiety/depression. 20 Each domain is scored from 0 (worst imaginable health state) to 100 (best imaginable health state). 20
The SF-36 (RAND Health, Santa Monica, California, United States) is a quality-of-life measurement assessment tool, which consists of eight domains: (1) physical functioning, (2) physical role, (3) bodily pain, (4) general health, (5) vitality, (6) social functioning, (7) emotional role and (8) mental health. Based on the above eight domains, the SF-36 calculated two component scores, a physical component score (PCS) and a mental component score (MCS). These two aggregate scores were found to have good validity in differentiating clinically meaningful groups. 20
Statistical methodology
A review of prospectively collected registry data of 308 bipolar HAs was conducted. From this dataset, 70 cemented bipolar HAs and 238 uncemented bipolar HAs were identified. Testing of normality was performed on these two groups of bipolar HAs using the Shapiro–Wilk test. Data for all continuous variables were observed to be non-normally distributed. Mann–Whitney U test was thus used to compare between both groups of bipolar HAs. For categorical variables, the chi-square test was used for analysis. A comparison of the delta change from baseline outcome scores was also performed.
Due to the uneven number of patients in the two groups, propensity score matching was next performed on these 308 bipolar HAs. The effect of patients with cemented bipolar HA (treatment) versus patients with uncemented bipolar HA (non-treatment) was investigated. Propensity scores were generated using logistic regression to adjust for confounding variables of age, sex, Charlson comorbidity index (CCI) and pre-fall scores (EQ-5D, SF-36 all domains and PMS). Each patient in the treatment group was matched with another patient in the non-treatment group with the closest propensity score using the nearest-neighbour method and a 1:1 matching without replacement. After matching, a comparison of the two groups was again conducted using Wilcoxon signed-rank test.
Data analysis was performed using R (Version 4.02) and statistical significance was defined as p<0.05.
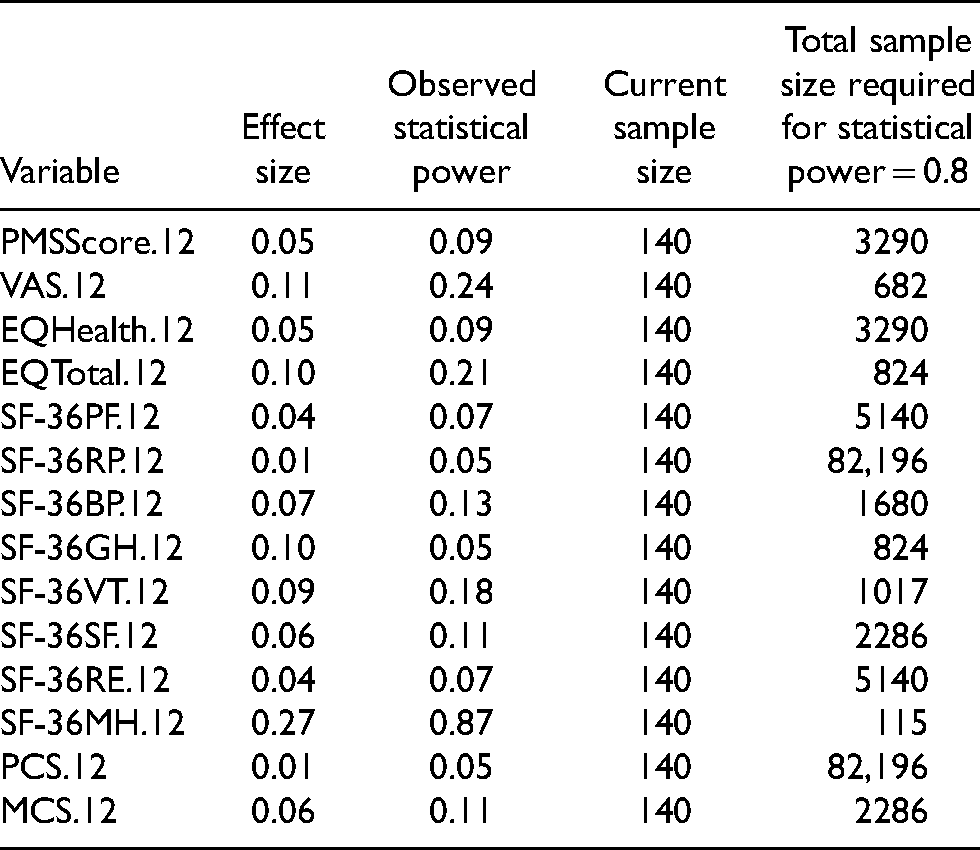
A priori power analysis was not performed for the study as this is based on the total number of patients treated in our institution from 2013 to 2016. Instead, we conducted a post-hoc statistical power analysis by calculating Cohen's d effect sizes from our observed data. From Table 1, the observed statistical power for almost all variables except for SF-36MH.12 are <0.8 or 80%. To meet the statistical power of 0.8 and assuming the effect sizes can be met, we determined that the minimum sample sizes ranges from 573 to 513,709. This is not likely to be achievable due to the retrospective nature of the study. Last, but not least, due to the one-to-one relationship between p values and observed power, low observed power will always be associated with non-significant p values. 20
Effect Sizes, Post-hoc Statistical Power and Sample Sizes Required for Minimum Statistical Power of 0.8 After Propensity Score Matching.
Results
Prior to propensity score matching (Table 2), there were 238 patients of which 176 (73.95%) were female with a median age of 76 years in the uncemented group (p < 0.001) The cemented group included 70 patients of which 60 (85.7%) were female with a median age of 81 years (p < 0.001).
Patient Demographics Before Propensity Score Matching.
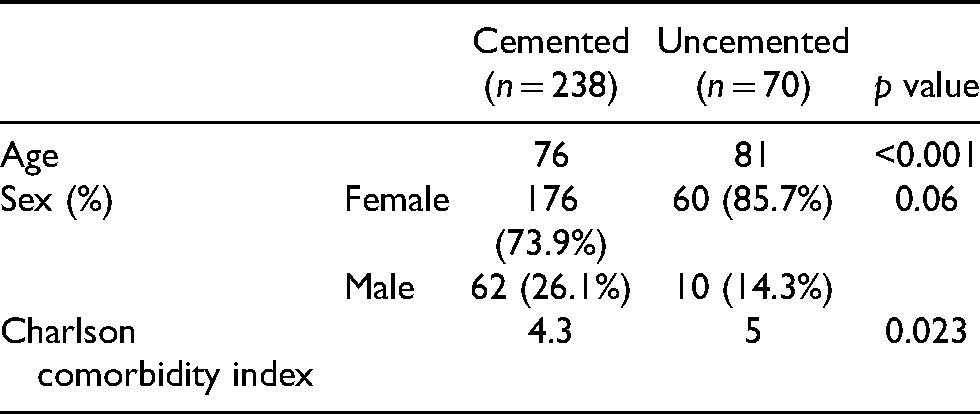
Correspondingly (Table 2), patients with cemented bipolar HA had a statistically significantly higher CCI as compared with patients with uncemented bipolar HA (p = 0.023). Patients with uncemented bipolar HA were also observed to have higher PMS at pre-fall (p = 0.037) and at 12 months (p = 0.035) as compared with patients with cemented bipolar HA. Comparing the delta changes from pre-fall before matching, no significant difference was observed (Table 3).
Patient Demographics After Propensity Score Matching.
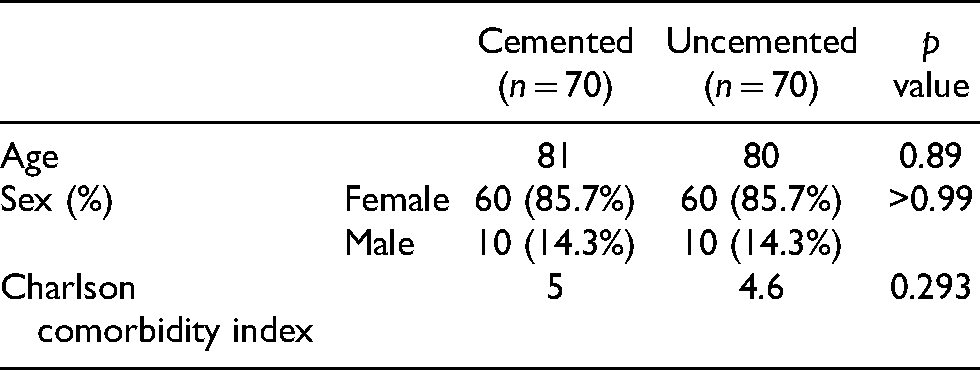
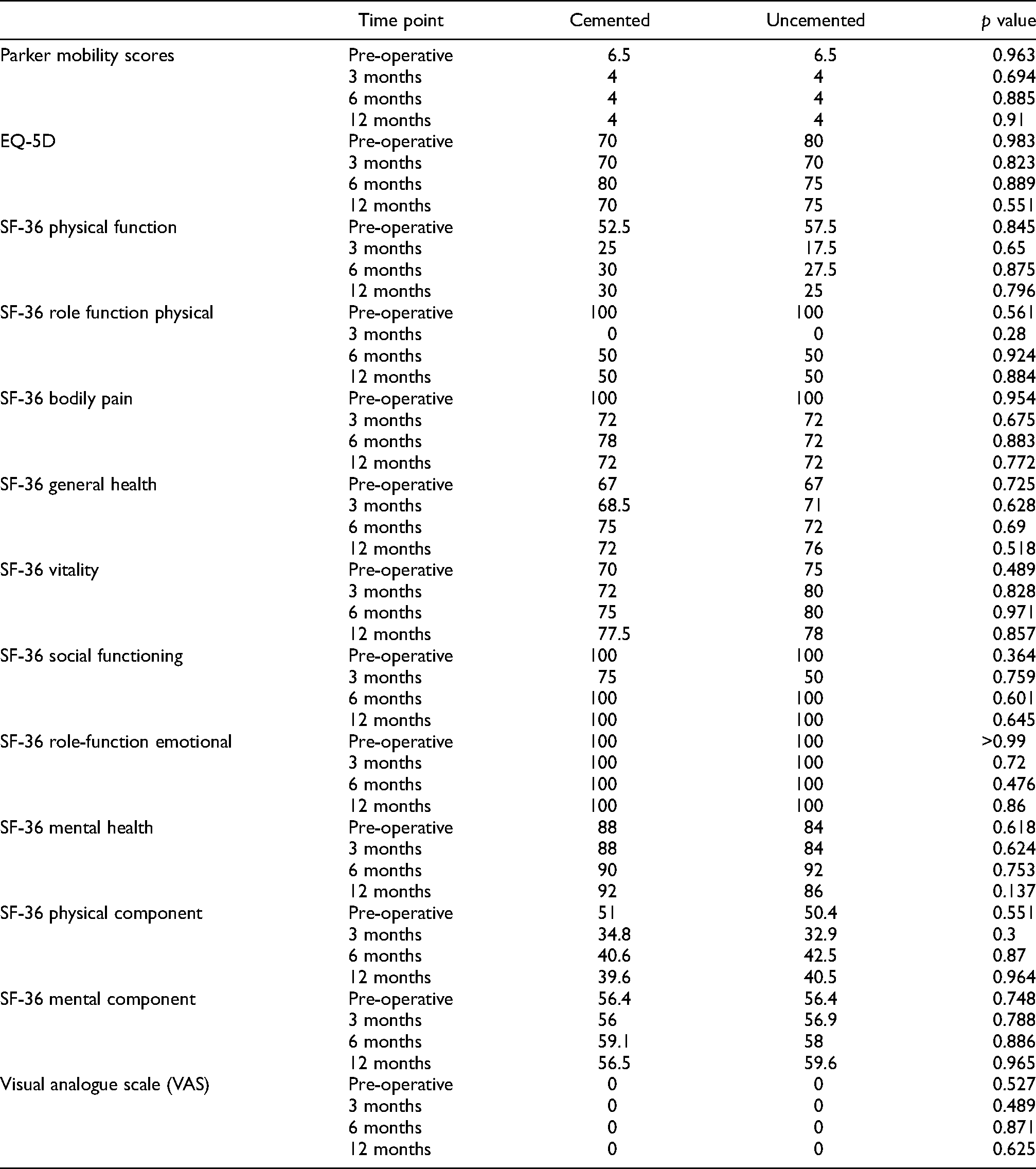
The two groups were well matched after propensity score matching (Figure 2). At both 6 and 12 months post-surgery, both groups had similar PMS, EQ-5Q, SF-36 and visual analogue scale (VAS) scores, with no statistically significant difference observed between the groups (Table 4). With respect to the delta changes from pre-fall after matching, there was no significant difference (Table 5). From the analysis of the matched set of data, treatment of NOF using cemented or non-cemented bipolar hip prosthesis resulted in similar Parker Mobility, SF-36 physical function, general health, vitality, physical component and mental component scores (Table 4).
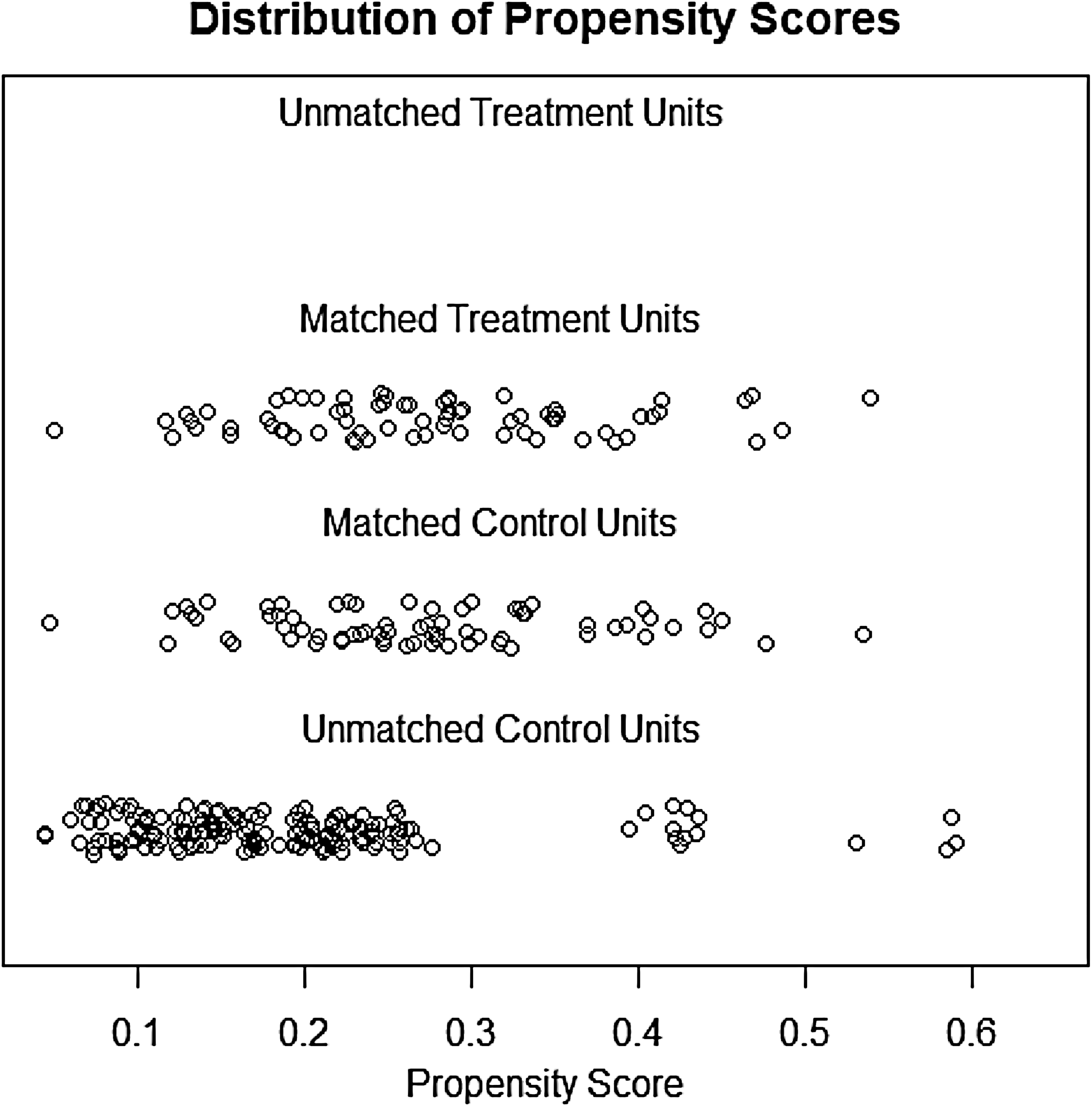
Distribution plots before and after propensity score matching.
Median Mobility and Quality-of-Life Scores After Propensity Matching.
Median Change in Outcome Scores After Propensity Score Matching.
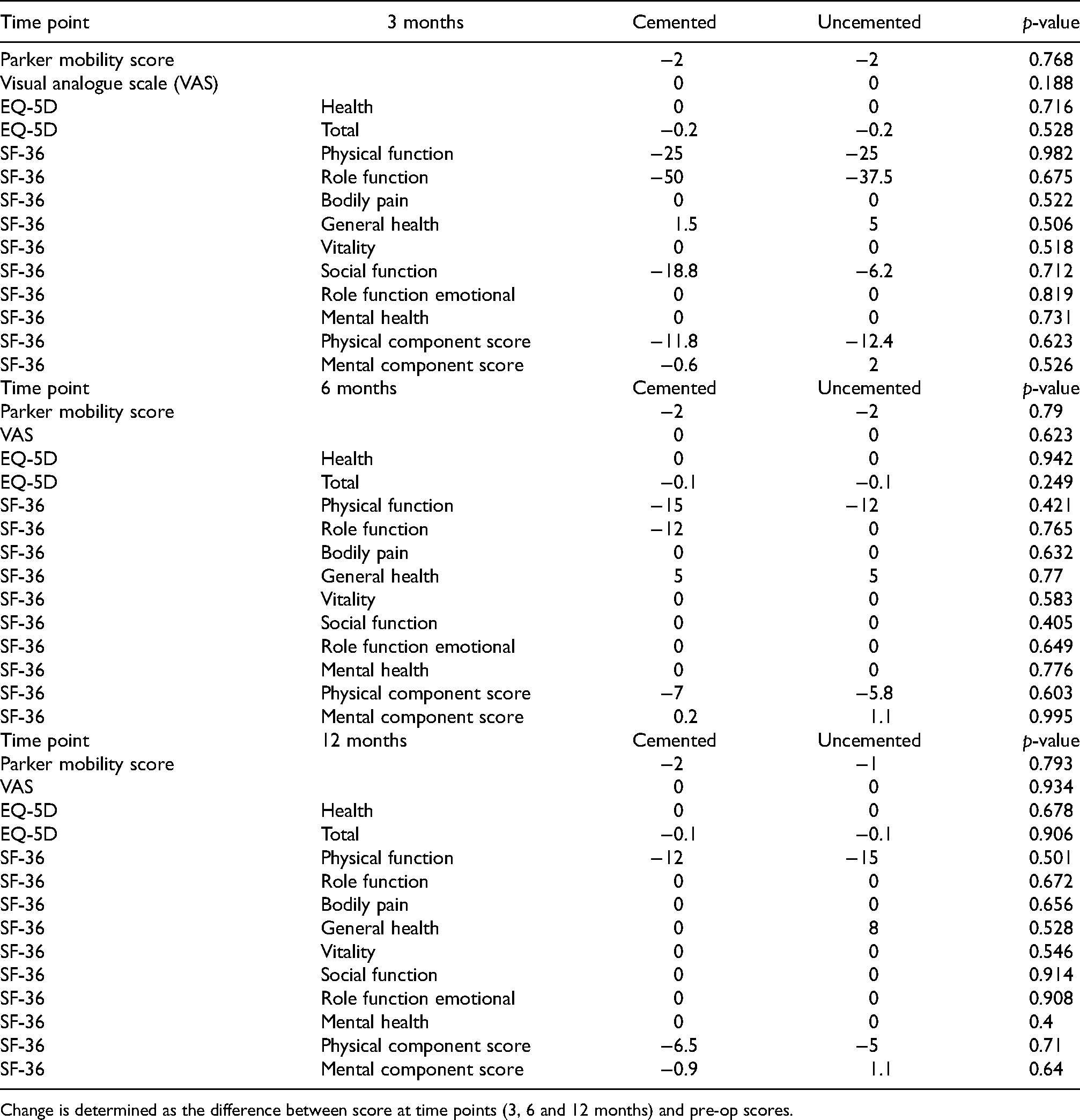
Change is determined as the difference between score at time points (3, 6 and 12 months) and pre-op scores.
Discussion
Displaced NOF fractures are prevalent in the elderly and result in both short- and long-term deterioration in functional outcomes. 20 In our institution, the majority who are fit for surgery undergo a HA in an effort to mitigate this deterioration. 20 Surgeons in our institution performed three times as many uncemented HAs (238 of 308: 77.3%) versus cemented HAs (70 of 308: 22.7%). The usual decision for a cemented HA is undertaken mainly in patients who are more osteoporotic, or have a Dorr C-type femoral canal, so as to lower the risk of an iatrogenic fracture. 20 This practice is echoed in our results, with the cemented population being significantly older and frailer, as inferred by the higher CCI. With the increased operative time and the spectre of severe BCIS, 20 the question exists if these are justified by better mobility and quality-of-life scores.
Mobility scores
Multiple studies show that cemented prostheses resulted in better mobility, less thigh pain and a lower revision rate. 20 In more recent literature, there is no clear consensus, with some studies showing no difference in mobility scores between cemented and uncemented HA in the short term, 20 some showing worse short-term mobility scores in the cemented group 20 and yet others showing better mobility in the cemented group against the uncemented group. 20 In our study, there were no statistically significant differences between cemented and uncemented groups at any time point which suggests that cementing alone does not impact post-operative mobility. This suggests that the decision for cementing should be based on the patient risk profile and not on the pre-operative mobility profile.
Quality-of-life scores
When assessing for quality-of-life scores, Ng and Krishna 20 did not find a difference in the Harris hip score (HHS) at 1 year in their study of 207 hips. Similarly, Langslet et al. 20 showed in their 220 patients that, EQ-5D scores were not different between the groups at 1 and even 5 years but did show a higher HHS at 5 years in the uncemented group. DeAngelis et al. 20 found that measures of activities of daily living and energy as well as self-efficiency levels were comparable between both cemented and cementless groups at 1 year. In terms of SF-36 scores, Peterson et al. 20 found that by 6 months vitality, social function, emotional role, mental health and general health seem to be close to their maximum levels and by 3 months, only physical role and physical function showed a statistically significant difference from the level at 1 year. In addition to this, Randell et al. 20 found in their study that patients after a hip fracture suffered significant reductions in physical and social functions as measured through SF-36 scores with particularly rapid decline at the 12–15 weeks following a fracture.
These findings are similar to our study which found no significant difference in EQ-5D or VAS scores at any time point. One interesting finding however is that the role functional physical component of the SF-36 score was markedly reduced at 3 months for both groups, and this score never reached pre-fall levels even at 12 months for either group. This would suggest that perhaps the choice to cement or not is an important factor in determining the recovery trajectory.
Parker mobility score
Our data compared well-matched patient groups of 70 cemented and 238 uncemented HAs to determine if there was a difference in mobility or quality-of-life scores measured at 3, 6 and 12 months follow-up intervals. As seen in Table 1, our analysis did not find a significant difference at any of the follow-up intervals in their PMSs. This echoes the findings of Kristensen et al. 20 and Santini et al. 20 , who found no significant differences in mobility scores following cemented or cementless HA.
EQ-5D
Our study also did not find any statistically significant difference at any follow up time point for EQ-5D scores between cemented and cementless HA. This echoes the findings of Fidved et al., 20 who also showed equivalent Barthel index, EQ-5D and HHS between the two groups; their study utilised the equivalence criterion, 20 proving that 60 hips in each group would be adequate for a power of 95% to prove that the mean HHS is the same in both groups. Having met that minimum number in our cohort, by extension, makes the chance of a Type II error less probable as well.
SF-36
Our study found that SF-36 scores across all the eight subscale domains did not show any statistically significant differences between cemented and uncemented HA. Both Peterson et al. 20 and Randell et al.29 found that quality-of-life scores as measured using SF-36 showed significant decreases following hip fractures, but with the exception of physical and social function, reverted back to pre-fracture levels between 6 and 12 months in their study of 38 and 61 patients, respectively. 20 Our study echoed these findings in both cemented and cementless HA with notable decreases across all domains at 3 months, with scores recovering and reaching pre-op scores by 6 months. One notable exception to this was the PCS, which by 12 months, still remained significantly lower than pre-operatively for both cemented and cementless groups (Table 4). One potential reason for this is that patients who undergo HA tend to be elderly and frail to begin with so the trauma and morbidity suffered from the fall and subsequent surgery and post-operative rehabilitation would significantly alter their future behaviour leading to reductions in confidence and increased dependence on caregivers.
To the best of our knowledge, this is one of the first studies of its kind to compare pre-operative and post-operative SF-36 scores between cemented and cementless HA.
We further analysed the data as seen in Table 3, to evaluate the change (delta) from pre-fall functional scores to post-surgery functional scores. These were also at 3, 6 and 12 months follow-up intervals. Again, we did not find a significant difference in the delta of their PMSs, EQ-5D scores and SF-36 scores between the cemented and uncemented cohorts at any of the follow-up intervals.
With no clear difference in the recovery rate and final mobility scores, counselling patients for their surgical options between cemented and uncemented HAs should then involve other issues such as upfront cost, BCIS risk and iatrogenic fracture risk. We believe that rather than a one size fits all approach, a balance can be struck via a selective process. Uncemented implants can be utilised in younger, less osteoporotic patients who are at lower risk of periprosthetic fractures, and the converse in older patients. In an elderly cohort, quality-of-life scores as assessed by the EQ-5D and SF-36 appear not to differ between both groups as well.
The study has a few drawbacks. Firstly, this was a multi-surgeon study, and this was not accounted for in the analysis. 20 Secondly, the cementing techniques and implant choices, were not standardised. Thirdly, the impact of the surgical approach was not analysed, and each surgical approach (posterior, lateral, anterolateral and anterior) has its own effect on functional outcomes. Lastly, patients who passed away within the time period or did not come back for follow up at 3, 6 and 12 months were excluded from the analysis.
Longer term follow-up outcome data would be ideal but it will be challenging to accurately follow up and analyse in view of the known high mortality rate of 20–35% within 1 year of sustaining a fractured NOF and hence there would be a significant proportion of patients lost to follow up after 1 year. 20
Conclusion
In our analysis, there was no statistically significant difference in the mobility or quality-of-life scores of the patients undergoing cemented versus uncemented HA for their displaced NOF fractures. Both groups of patients had significant reductions in their physical component quality-of-life scores. It may be prudent to continue the practice of selectively performing cemented HAs for older, frailer, Dorr-C type femoral canals on radiographs and more osteoporotic patients to balance the risk of complications in cemented implants against the increased cost and risk of iatrogenic fractures in uncemented implants.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.