
Abstract
Internal fixation is commonly used to treat fractures in the hip. However, failure of proximal femoral fracture fixation is common and treated with total hip replacement (THR). The aim of this study is to present our midterm results of dual mobility (DM) THR for failed internal fixation of proximal femur fractures. Between 2010 and 2015, a total of 28 cases of failed internal fixation for hip fractures were treated through DM total hip arthroplasty. Two patients died during the early postoperative period due to medical complications. The average follow-up was 3.4 years. We had one patient with superficial surgical site infection which was managed by local wound debridement and dressings. The average Harris hip score was 85. DM THR is the procedure of choice for revising failed internal fixation for hip fractures in our patients with good clinical outcome.
Introduction
Osteoporotic fractures of proximal femur are more common in femoral neck and trochanteric region. 1 This is a major cause of morbidity and mortality in elderly with survival rates comparable to breast and thyroid cancer patients. 2 The incidence of failed fixation is 41% for displaced neck femur fractures, 5% for undisplaced neck femur fracture, and 15% for undisplaced peritrochanteric fracture. 3 The optimal salvage procedure for these failed fixations is total hip replacement (THR). 4 This procedure has been shown to have high rate of complications such as intraoperative fracture and early dislocation. 5 –8 However, the use of dual cup THR reduces the risk of postoperative dislocation following failed internal fixation of proximal femur fracture. 9 We present our midterm results of dual mobility (DM) THR in these high-risk patients.
Materials and methods
We conducted a retrospective mono-center cohort study of all patients with failed fixation of proximal femur facture managed by DM THR. The data were prospectively collected from our hospital patient database (HIMS), from January 2010 to January 2015. There were a total of 28 cases included (15 males and 13 females), with the average age of the patients being 68 years (59–92 years). There were 20 cases of failed peritrochanteric fracture (group A) and 8 cases of failed fixation of fracture intracapsular neck femur (group B). The patients undergoing primary replacement for proximal femur fracture, pathological fracture, salvage of failed hemiarthroplasty, and periprosthetic joint infection were excluded from the study. The primary method of fixation and mode of failure in both the groups are shown in Table 1. The average time from primary fixation to salvage arthroplasty was 30 months. The indication for salvage was nonunion, avascular necrosis of femoral head, implant failure and cut out and dislocation.
Method of fixation and modes of failure.
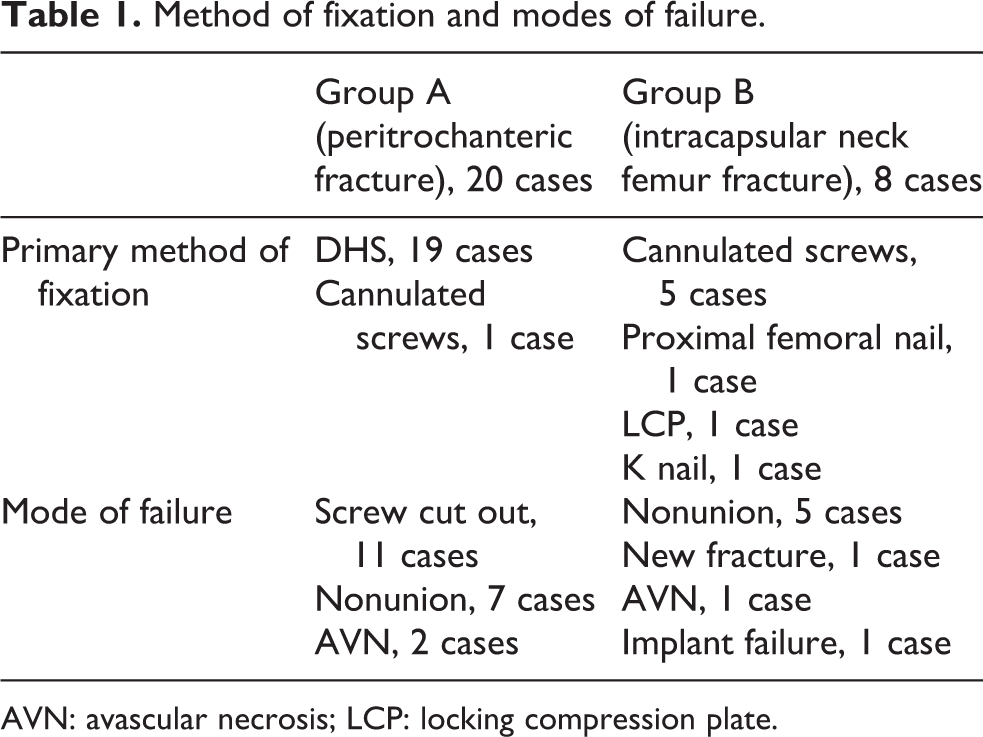
AVN: avascular necrosis; LCP: locking compression plate.
All the cases were American Society of Anaesthesiologist (ASA) grade 3 with 22 patients having associated comorbidities. We used a posterolateral approach in all cases and hip was dislocated before removing the implant to avoid intraoperative fractures of femoral shaft. Avantage privilege DM system from Biomet (Indiana, Warsaw, USA) was used in all the cases (Figure 1) . The implant fixation was cemented, uncemented, and hybrid in 18, 6, and 4 cases, respectively, based on the quality of bone. Standard bimetric stem was used in 16 cases and long stem in 12 cases.

X-ray of a 59-year-old operated with DHS for peritrochanteric fracture 2 years back showing screw cut out with secondary osteoarthritis.
The bearing surface was metal on highly cross-linked poly in all cases. Low molecular weight heparin (LMWH) was used in all the cases for postoperative prophylaxis and there was no complication of deep vein thrombosis (DVT) or pulmonary embolism (PE). Two patients died during the early postoperative period due to medical complications. The average follow-up was 3.4 years. A telephonic interview was conducted for all the patients for the purpose of this study.
Results
The mean follow-up of the patients was 3.4 years (average 1–6 years). The mean duration of the surgery was 180 min (standard deviation = 18.6). Intraoperative periprosthetic fracture (PPF) was encountered in four patients while broaching for uncemented stem and was stabilized with cables (Dall-Miles cable system, Stryker, NJ, USA). Intraoperative hypotension was encountered in one patient while preparing the femoral canal. Physiotherapy was started from next postop day and average time to start walking was 5 days. Four patients had leaky wound with bruising around the surgical scar for which LMWH was stopped and aspirin was used as thromboprophylaxis. We had one patient with superficial surgical site infection which was managed by local wound debridement and dressings. There were no hip or intraprosthetic dislocations. The mean Harris hip score was 85 (65–90). The Kaplan–Meier survival index is shown in Figure 3.
Discussion
Failure of proximal femoral fracture occurs due to osteoporosis, unsatisfactory reduction, infection, and postoperative weight-bearing. 3 It is seen with both dynamic hip screw (DHS) and proximal femoral nail (PFN). 10,11 The modes of failure as reported in literature 6,12 –16 were observed in our study, in addition we had a case of early postop dislocation which has no mention in previous studies. A multicenter study demonstrating high complication rates following re-osteosynthesis recommended THR as the only valid salvage procedure for failed proximal femur fixation. 4 These patients are high ASA due to associated comorbidities and modification of bony landmarks, loss of bone stock, and presence of holes after removal of internal fixation hardware present intraoperative challenge in management of these cases. 5,6,16,17
We followed the described technique to dislocate the hip prior to implant removal 14 and avoided femoral shaft fractures arising due to osteoporosis, stiffness, and screw holes acting as stress risers. Zhang et al. 6 reported overall complication rate of 47% while treating failed proximal femur fractures.
We had calcar fracture while broaching for uncemented stem in initial cases and hence we used cemented stem fixation. Screw holes have resulted in femoral shaft fracture while inserting uncemented stems. 18 We did not plug 19 or graft 18 the cortical holes during injecting or pressurizing the cement. We believe that cement enters and obliterates them and prevents them from acting as stress risers. For many elderly patients, cemented fixation is advantageous, particularly with bone quality and wide modularly canal.
Many authors have recommended standard stems. 6,14 –16 We used monoblock long stem in 12 cases and did not encounter postoperative PPFs in our series. There is reported incidence of 7.5% PPF in these patients. 20
Trochanteric nonunion has been managed by tension band wire 19 or trochanteric slide 14,21 to preserve the abductor function and facilitate implant placement. We have used a 3.5 mm distal tibial locking plate in patients with trochanteric nonunion (Figure 2). There was no postop skin problem encountered with these low-profile plates. Union of the fragment was achieved in five cases and patients were not symptomatic even if the trochanteric fragment failed to unite.

Patient operated with DM total hip arthroplasty. Distal tibia plate was used to fix trochanteric fracture. DM: dual mobility.
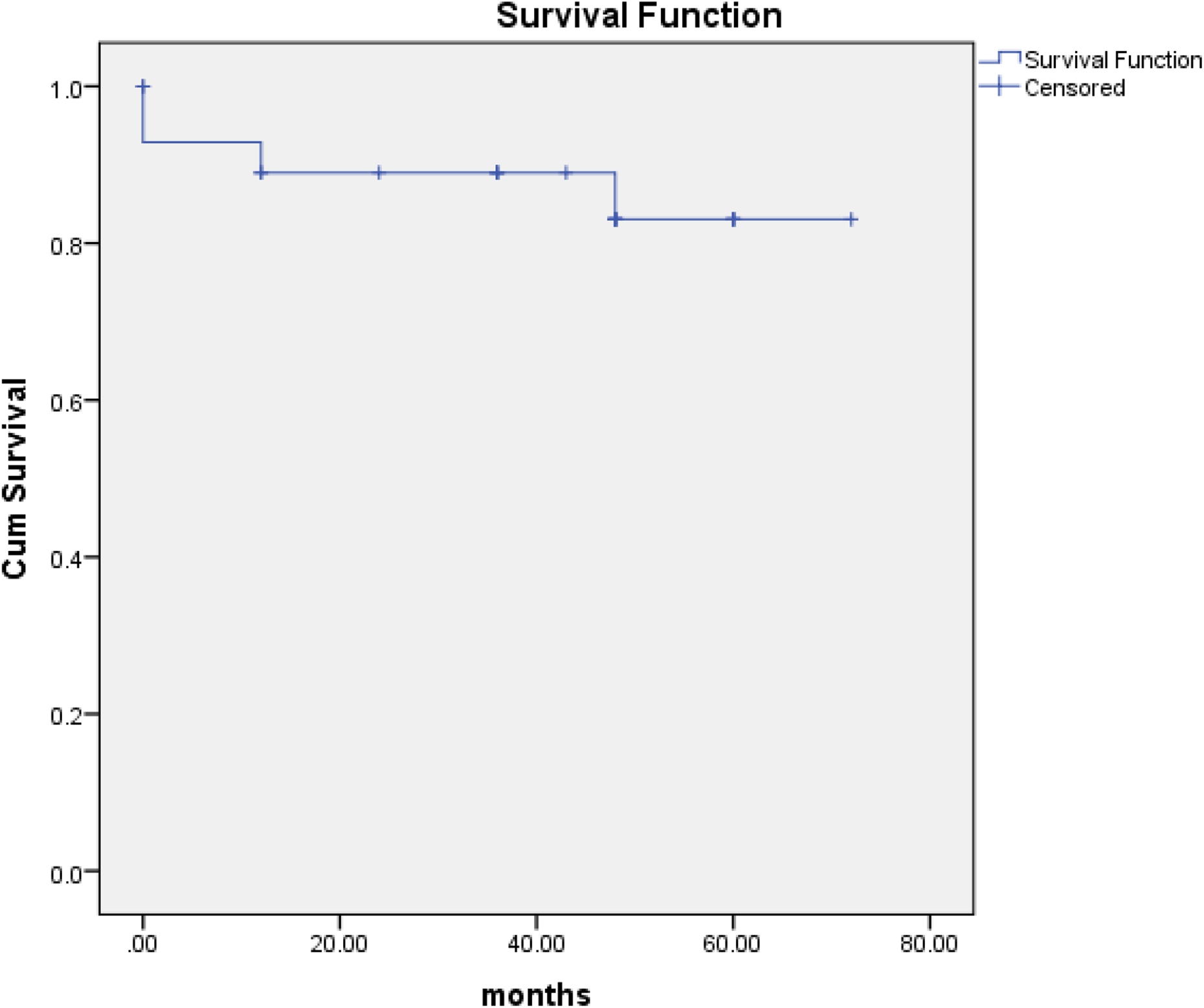
Kaplan–Meier survival index.
THR after failed osteosynthesis has higher dislocation rates. 5,22,23 Use of larger head size can help to reduce postoperative dislocation. 24 The smaller average pelvic size in our cohort of population does not permit femoral head more than 28 mm.
Recent literature has shown that the use of DM arthroplasty following failed osteosynthesis of proximal femur fracture helps to reduce the risk of dislocation and it is recommended in cases with high risk of instability. 9 However, complications such as intraoperative dislocation and polyethylene wear have been reported with use of DM implant, especially with early design. 25,26 In addition, there is concern regarding long-term survivorship of DM cups compared with THA. We have used DM cup in all our cases. This combines the two concepts of low-friction arthroplasty of Charnley 27 with lager head low dislocation rates of McKee Faraar. 28 The reported low dislocation rate of DM cup 29 –31 is supported by our study which had no postoperative dislocation despite using posterior approach in all the cases.
There are limitations of the study. A small number of cases were reviewed and studied in our series. In addition, no objective or radiological hip scores were used to assess patient outcome after surgery. Another limitation is the lack of long-term evaluation of our cases.
In conclusion, salvage DM hip arthroplasty following failed osteosynthesis of proximal femur increases hip stability and has good overall satisfaction but functional outcome varies due to age and comorbidities. Harris hip scores vary from good to fair in multiple studies and our results have shown similar outcome.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.