
Abstract
Extensively coated long femoral stem revision hip arthroplasty is based on the principle of distal fixation at diaphyseal region, which can overcome the problem of proximal femoral bone stock deficiencies causing inadequate support and unstable fixation when using conventional length femoral stem. We performed a retrospective cohort analysis of 43 cases of revision hip arthroplasties using extensively hydroxyapatite-coated long femoral stem performed in our department from Jan 1998 to Dec 2005. Patients’ background demographic data, operative details and clinical outcome were analyzed. The mean age at revision surgery was 63.7 (32–84). The mean follow-up period was of 13.8 years (11–17.5 years). In the latest follow up, all patients reported either no or mild hip or thigh pain. 29.2% of patients were able to walk unaided, 25.0% were able to walk with stick, and 33.3% were able to walk with quadripod. The average Harris hip score measured in the latest follow up was 78.8 (55–100). 4.7% were complicated with implant loosening requiring re-revision and 4.7% were complicated with implant infection requiring implant removal. The survival rate was 89.9% at 17.5 years. The femoral stem without femoral fixation augmentation had better survivorship as compared with those with augmentation (p = 0.038). Extensively hydroxyapatite-coated long femoral stem is a good option for revision hip arthroplasty with good clinical outcome and high survival rate.
Introduction
With the aging population and the increasing life expectancy in Hong Kong, the incidence of hip pathology, including hip fractures, arthritis and osteonecrosis, are increasing. Operative treatment is required to treat these hip conditions if conservative means failed. Complications arising from operative treatments, including periprosthetic fractures and implant failure, are inevitable. Revision hip arthroplasty, aiming at pain relief and functional improvement, is expected to increase proportionally. Chiu et al. reported that the revision rate for primary total hip arthroplasty in Hong Kong is 12.8%, 1 the intra-operative and post-operative complication rate for revision total hip arthroplasty is 16.0%, in which 6.4% of them need to be re-revised. 2 Stable fixation is of paramount importance in revision hip arthroplasty to allow early mobilization, especially the fragile elderly patients.
One of the most important challenges for revision hip arthroplasty is proximal femoral bone loss which preclude stable fixation using standard femoral prosthesis. 3 Extensively hydroxyapatite-coated long femoral stem revision hip arthroplasty is based on the principle of distal fixation at diaphyseal region. It can overcome the problem of proximal femoral bone stock deficiencies causing inadequate support and unstable fixation when using conventional length femoral stem, which exist during many femoral revision arthroplasties. The operative technique was less demanding compared with femoral impaction bone grafting, and patients were allowed full weight bearing walking after the operation. The short- and mid-term clinical outcomes reported in the literature were satisfactory, 4 but the long term clinical outcome and survivorship has not been widely reported. Complications of femoral shaft fracture can occur, especially in osteoporotic bone. 5,6 Femoral stem subsidence and stress shielding were also the main concern in extensively-coated revision femoral stem. 7 This study is conducted to determine the long term clinical outcome and survivorship of revision hip arthroplasty with long femoral stem. It would be crucial to investigate the outcomes of these patients so that a more accurate decision on whether this major surgery should be offered to patients suffering from complications after surgical interventions of hip diseases.
Method
We performed a retrospective cohort analysis of 43 cases (41 patients) of revision hip arthroplasties using extensively hydroxyapatite-coated long femoral stem (Restoration HA, Stryker Howmedica Osteonics, Allendale, NJ) performed in our department from Jan 1998 to Dec 2005. Data were retrieved from Hospital Authority’s Clinical Management System (CMS) and review of patient record. If a patient had more than one revision hip arthroplasties on ipsilateral hip, the index operation for this study was the first revision hip arthroplasty using long femoral stem done in our department.
Patients’ background demographic data including their age at the time of revision hip arthroplasty using long femoral stem, their sex, their primary hip pathology, the implant used for primary hip surgery and indication for revision hip arthroplasty were analyzed. Operative details including intraoperative proximal femur fracture and perforation of femoral shaft, whether any bone graft used and other femoral fixation augmentation needed for reconstruction were analyzed. All patients were assessed both clinically and radiologically using antero-posterior and lateral X-rays during follow up in our department. Clinical outcome including any hip and thigh pain reported by patients, their mobility status and Harris Hip score (HHS) documented in their last visit were analyzed. Kaplan-Meier survival analysis was performed to analyze the survivorship of extensively hydroxyapatite-coated long femoral stem in revision hip arthroplasty. Log-Rank test (Mantel-Cox) was performed to determine if there was any statistical significant difference between different patient parameters related to the survivorship.
Results
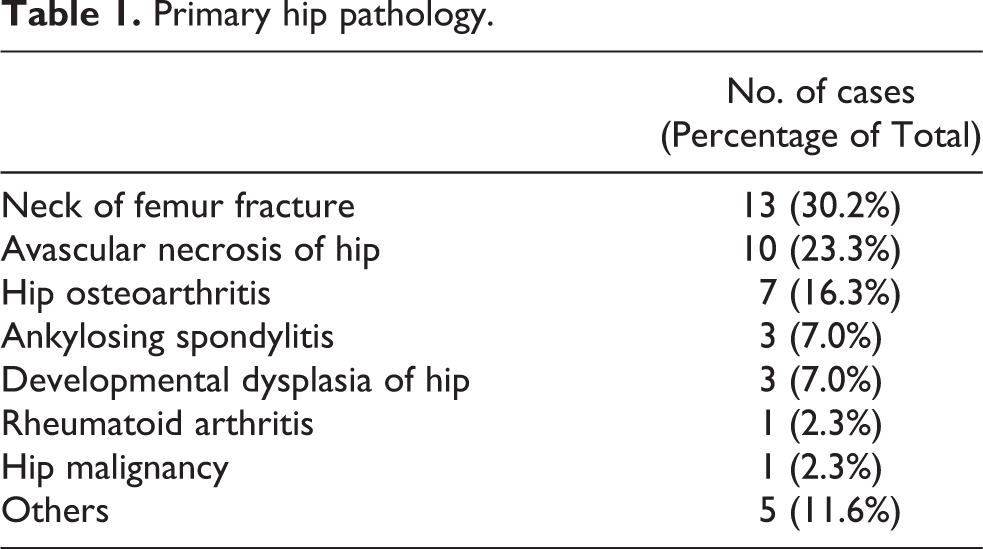
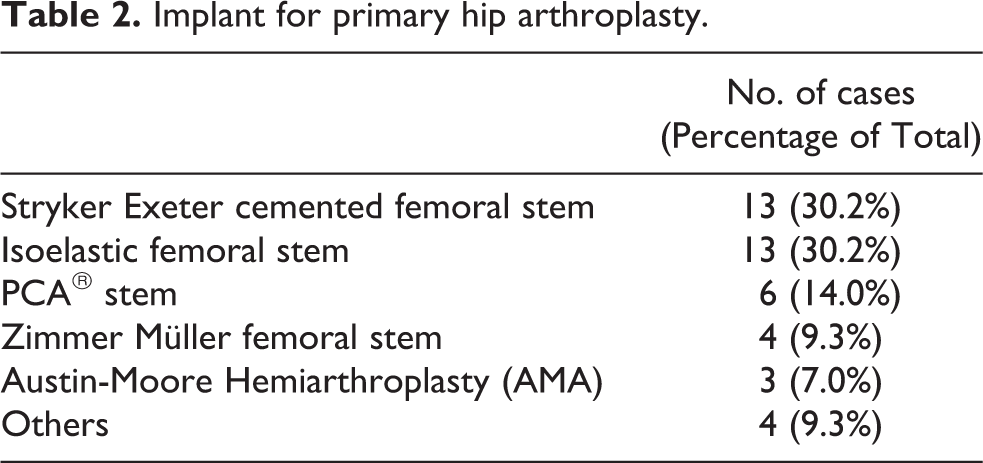
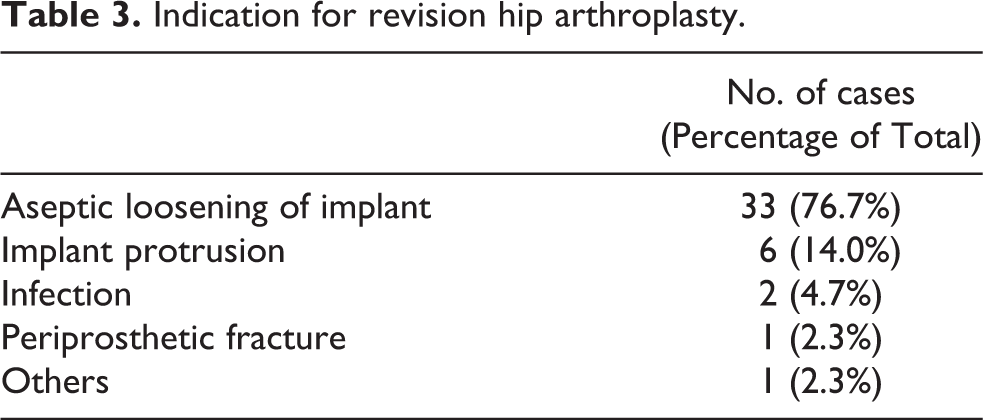
There were 17 male and 24 female patients receiving revision hip arthroplasties using extensively hydroxyapatite-coated long femoral stem in our department from Jan 1998 to Dec 2005. The mean age at revision surgery was 63.7 years old (32–84 years old). Table 1 –3 summarize their primary hip pathology, the implant used for primary hip surgery and indication for revision hip arthroplasties. The femoral defect was classified as Paprosky type I, II, IIA in 8 hips (18.6%), 28 hips (65.1%) and 7 hips (16.3%) respectively. 3
Primary hip pathology.
Implant for primary hip arthroplasty.
Indication for revision hip arthroplasty.
There were 12 cases (27.9%) of intraoperative fracture, including 4 (9.3%) proximal femur fracture, and 8 (18.6%) femur shaft perforation during operation. Eleven cases (25.6%) occurred during removal of previous stem and cement, and only one case (2.3%) of proximal femur fracture occur during reaming for insertion of new stem. Thirty-four cases (79.1%) required bone graft reconstruction, including 22 (51.2%) cases using morselized graft only, 4 cases (9.3%) using strut graft only and 8 cases (18.6%) using both morselized and strut graft. Twenty-one cases (48.8%) required further femoral fixation augmentation, including 15 cases (34.9%) using cables and/or wires only, 3 cases (7.0%) using cable plate and 3 cases (7.0%) using greater trochanter reattachment device.
The average follow up was of 13.8 years (11–17.5 years). Nineteen (44.2%) cases (17 patients) died of unrelated diseases during follow up. In the latest follow up of the remaining 24 patients, 16 cases (66.6%) reported no hip and thigh pain, 8 cases (33.3%) reported mild hip and/or thigh pain, and no patient reported moderate to severe hip and/or thigh pain. Seven patients (29.2%) were able to walk unaided, 6 patients (25.0%) were able to walk with stick, 8 patients (33.3%) were able to walk with quadripod and 3 patients (12.5%) were able to walk with frame. The average Harris hip score measured in the latest follow up was 78.8 (55–95).
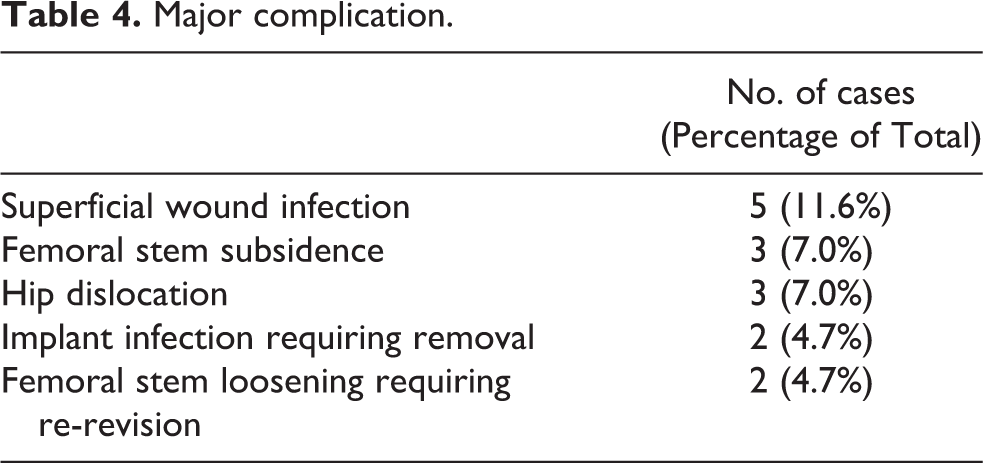
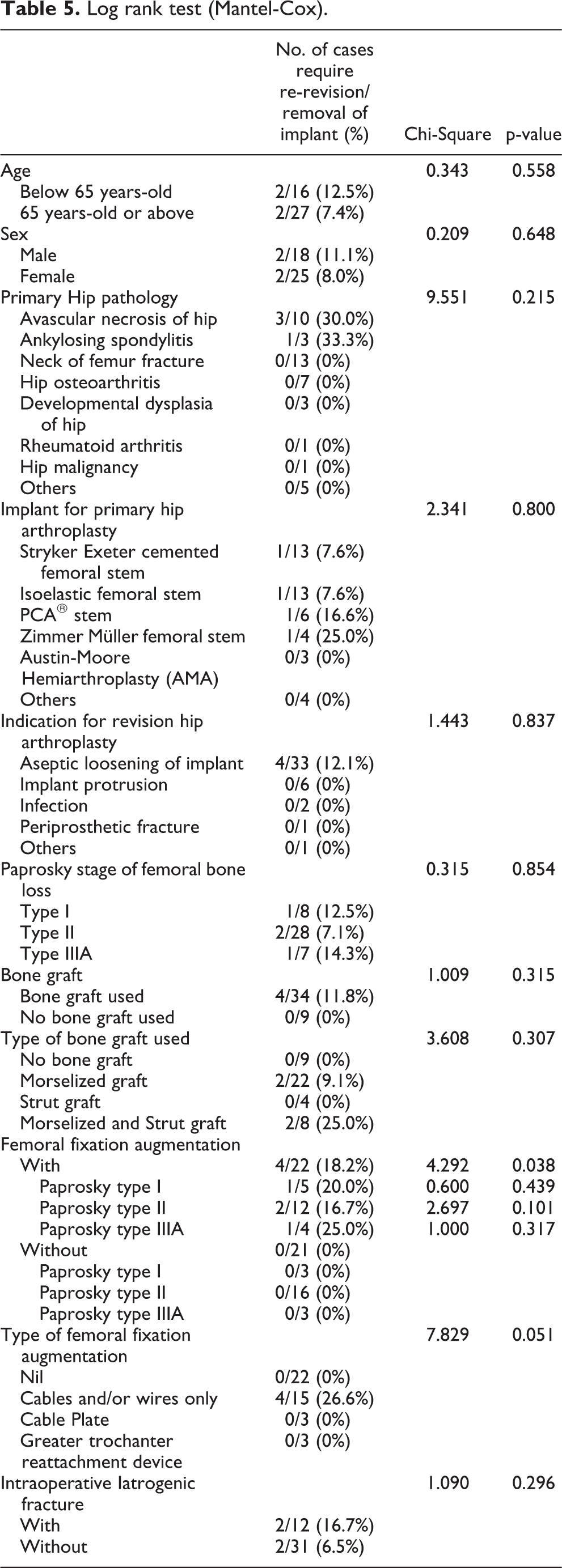
Complications were listed in Table 4. Five cases (11.6%) of superficial wound infection treated with antibiotics. Three cases (7.0%) were found femoral stem subsidence in follow up X Rays and became stabilized afterward. Three cases (7.0%) were complicated with hip dislocation. Two cases (4.7%) complicated with femoral stem loosening with subsidence required re-revision at 1.3 years and 6.3 years after revision arthroplasty respectively. In these two cases, the femoral stems were found to be undersized during re-revision surgery. Two cases (4.7%) were complicated with implant infection requiring implant removal at 3.9 years and 9.3 years after revision arthroplasty respectively. In these two cases, the revision arthroplasty using extensively hydroxyapatite-coated long femoral stem were the 2nd and 3rd revision surgery performed respectively. Also, one patient had co-existing diabetes mellitus, another patient was suffered from cervical cancer with radiotherapy done including the hip region before revision arthroplasty, these may contribute to the risk of implant infection. Kaplan-Meier survivorship, using either re-revision of femoral stem or removal of implant as end point, was 95.3% ± 3.3% (96% confidence intervals) at 5 years, 89.9% ± 4.8% at 10 years and remain constant afterward (Figure 1). Log-Rank test (Mantel-Cox) was performed. The femoral stem without femoral fixation augmentation had better survivorship as compared with those with augmentation (p = 0.038). Other parameters did not have any significant statistical significance (Table 5).
Major complication.
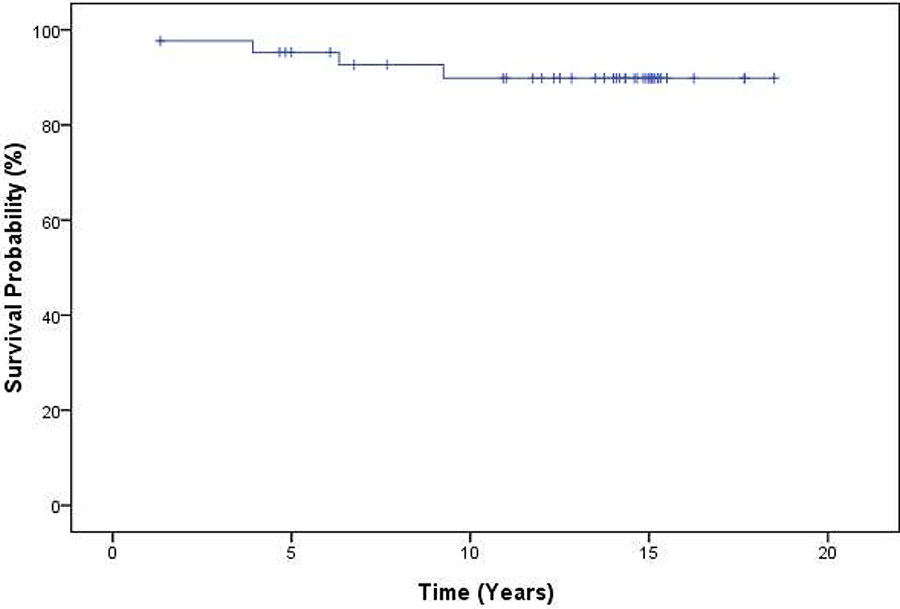
Kaplan-Meier survivorship of extensively hydroxyapatite-coated long femoral stem in revision hip arthroplasty.
Log rank test (Mantel-Cox).
Discussion
Revision hip arthroplasty of failed femoral components are technically challenging with high surgical risk. Significant osteolysis occurs as a result of polyethylene wear debris and cement particles. 8 Removal of old implants and the cement (if any) can be difficult and causing additional damage to the already compromised femur and resulting further bone loss. The remaining proximal femur with various degree of bone stock deficiency and altered femoral geometry is difficult to provide stable fixation for standard length femoral stem.
Historically there were three options described in the literatures. Proximally-coated femoral stem was used in revision hip arthroplasty, but the results reported from previous studies were not satisfactory. Berry et al. reported 38% loosening rate and 17% re-revision rate at mean follow up of 4.7 years, 9 and Malkani et al. reported the mechanical failure rate as high as 28.7% at 2.8 years follow up. 10 The other option is femoral impaction bone grafting. It was first developed in 1987 using morselized cancellous bone graft impacted into the femoral canal followed by femoral stem cementation. 11 The clinical outcomes reported were excellent with high survival rate. The 20-year survival rate was 87.7% reported by Wilson et al., with 34.2% found stem subsidence during follow up and the re-revision rate was 10.8%. 5 However, the technique of femoral impaction bone grafting was highly demanding with very steep learning curve. Compliance to protected weight bearing post-operatively is often necessary but is always difficult to our elderly. Compared with both proximally coated femoral stem and femoral impaction bone grafting, our study showed that using extensively hydroxyapatite-coated long femoral stem in revision hip arthroplasty had a comparable high survivorship (89.8%) and lower stem subsidence rate (11.6%) and re-revision rate (4.7%).
Concerning the complications, complication of eccentric reaming, femoral perforation and femoral fracture using extensively porous-coated femoral stem reported by Issack et al. was 0.1%, 6 and the intraoperative fracture of femur in revision total hip arthroplasty with a fully hydroxyapatite-coated stem reported by Rothem et al. was 20%. 12 Our study showed a higher intraoperative femur fracture of 27.9%. However, 25.6% of the intraoperative fracture occurred during removal of old implants and the cement (if any) which was not related to what type of new femoral stem used. In only one case (2.3%) the intraoperative fracture occurred during reaming for insertion of new stem.
The mechanical failure rate was 11.6%. There were three cases (7.0%) of femoral stem subsidence which stabilized afterward and all these three radiographs were reviewed which the femoral stems were found to be undersized. In the latest follow up, all of them did not complain of any hip or thigh pain, and their average Harris hip score was 75.0, which was comparable to the average Harris hip score of all cases (78.8). The average survivorship of these three cases was 14.1 years. There were two cases (4.7%) of femoral stem loosening requiring re-revision arthroplasty at 1.3 years and 6.3 years after revision arthroplasty respectively, and both of these two femoral stems were found to be undersized during revision surgery. We proposed that correct sizing of femoral stem is important to provide long term stability in extensively hydroxyapatite-coated long femoral stem in revision hip arthroplasty. The femoral stem without femoral fixation augmentation had better survivorship as compared with those with augmentation (p = 0.038). This may suggest that requiring further femoral fixation augmentation is an indicator for severe underlying bone stock deficiency which could not provide stable fixation for long femoral stem even at diaphyseal region. For the 4 cases require re-revision or removal of implant, one case with Paprosky type I, two cases with Paprosky type II and one case with Paprosky type III. There was no statistical significant difference between each Paprosky type (p = 0.854). Comparing cases with same Paprosky type, there was no statistical significant difference between with or without femoral fixation augmentation. (The p-value for Paprosky type I, II and IIIA were 0.439, 0.101 and 0.317 respectively.) This may due to the sample size of this study is small. Further studies with larger sample size are needed to analyze the relationship between Paprosky type, femoral fixation augmentation and survivorship. Form our experience, other than the two cases of implant infection requiring implant removal at 3.9 years and 9.3 years after revision arthroplasty respectively, there was no further failure noted up to 17.5 years after revision surgery, it shows that extensively hydroxyapatite-coated long femoral stem has a good long lasting survivorship in revision hip arthroplasty when it was stable.
Bryan et al. reported the survivorship for 1100 revision total hip arthroplasties performed between 1986 and Aug 2005 with mean follow up period of 6 years using second revision as endpoint was 82% at 10 years and 72.6% at 15 years, and the re-revision rate was 12.8%. 13 Our study showed the long femoral stem in revision hip arthroplasty has a higher survival rate (89.8%) at 10 years and at 15 years, and lower re-revision rate (4.7%) in long term follow up.
The strength of this study is that this is a long term study with 11- to 17.5-years follow up. It is also a local study focusing only the femoral stem revision in revision hip arthroplasty using extensively hydroxyapatite-coated long femoral stem. The clinical outcome was also analyzed using Harris hip score. On the other hands, there are limitations of our study. First, the sample size was small (43 cases). Second, we had no control group for this study.
Conclusion
Extensively hydroxyapatite-coated long femoral stem is a good option for revision hip arthroplasty with good clinical outcome and high survival rate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.