
Abstract
Purpose:
Massive bone defects represent a challenge in revision total hip arthroplasty (THA). Wagner self-locking (SL) stem is a favorable option for this technique; however, its long-term outcomes with bone allograft have rarely been reported. The purpose of this study was to investigate the long-term outcomes of this stem with bone allograft for Paprosky type II and III bone defects in revision THA.
Methods:
A total of 38 patients (40 hips) who underwent revision THA with the Wagner SL stem were retrospectively reviewed. Bone allograft was placed in every patient. Clinical outcomes were determined using the Japanese Orthopedic Association’s hip scoring system (JOA hip score). Stem subsidence, stem fixation, and remodeling of the grafted bone were assessed radiographically. The survival rate of the stem was assessed by Kaplan–Meier survival analysis.
Results:
The mean JOA hip score at the latest follow-up was 75.3 points. Stem subsidence of ≥10 mm was observed in four hips (10.0%). Moreover, 67.5% (27/40) of hips were stable, and 27.5% (11/40) had fibrous fixation. Bone restoration was observed in 25 hips (62.5%). At a mean follow-up of 15.7 years, the cumulative stem survival rates were 96.6%and 91.7% with “stem re-revision for loosening” and “stem re-revision for any reason” as the end points, respectively.
Conclusion:
The Wagner SL stem with bone allograft for proximal femoral bone defects in revision THA is a clinically beneficial procedure.
Introduction
Acceptable results of various techniques, such as cemented components, modular tapered components, and extensively porous-coated stems, for revision total hip arthroplasty (THA) have been reported. 1 –3 Nevertheless, severe proximal femoral bone defects is challenging for revision THA. 4,5 Wagner self-locking (SL) revision stem, established by Prof. Wagner in 1986, was identified as a favorable option for bone defects and periprosthetic fractures. 6,7 However, it was reported that this stem had a high dislocation rate. 8 Furthermore, the long-term results of the Wagner SL revision stem with bone allograft have rarely been reported.
Various methods, such as impaction bone allograft, allograft prosthesis composite, and distal press-fit fixation, are available for the reconstruction of severe proximal femoral bone defects in revision THA. At our department, we use Wagner SL stem with the impaction bone allograft technique for Paprosky type II and III bone defects as well as interlocking stem with allograft–prosthesis composite for Paprosky type IV bone defects. The present study aimed to assess the long-term outcomes of the Wagner SL stem with bone allograft for Paprosky type II and III bone defects in revision THA.
Methods
Patients
From 1993 to 2005, 38 consecutive patients (40 hips) underwent revision THA using the Wagner SL stem (Zimmer Inc., Warsaw, Indianna, USA). The mean follow-up duration was 15.7 (5.5–22.8) years. Patient demographics are reported in Table 1. Among the 38 patients, 25 were women and 13 men. The mean age at the time of surgery was 62 years (range 41–80 years). Diagnoses at the primary THA were osteoarthritis in 24 cases, femoral neck fracture in 7 cases, femoral head necrosis in 7 cases, and rheumatoid arthritis in 2 cases. In a previous primary THA, a cemented stem was used in 4 hips, and a cementless stem was used in 36 hips. Indications for revision THA were aseptic loosening in 32 hips, infection in 6, and periprosthetic fracture in 2. Bone defects were classified according to Paprosky classification 9 : type II in 7 hips, type IIIA in 22, and type IIIB in 9. According to the Vancouver system, 10 both hips with periprosthetic fracture were classified as B3. This consecutive series of surgeries was performed by two senior surgeons in the same department, who reviewed the patients preoperatively, 1 month, 3 months, 1-year postoperatively, and then annually. The follow-up data were directly obtained by two surgeons who were not involved with the operation. All patients provided informed consent, and the study was approved by our institutional review board.
Patient demographics.

Operative technique
All surgeries were performed via the extensile posterior approach in the lateral position. Preoperative planning was performed to decide the optimal size and length of the acetabular and femoral components using radiographs and computed tomography images. Trochanteric osteotomy was performed in 37 hips (92.5%), and transfemoral osteotomy was performed in 1 hip (2.5%). A medullary cavity of the femur was prepared by a series of reamers of increasing size. Bone allograft was placed in all hips, including impaction morselized bone allograft in 28 hips, block bone allograft in 4 hips, block and impaction morselized bone allograft in 5 hips, and cortical bone plate in 3 hips. The morselized bone was impacted with a thin-reaming instrument. For impaction of the morselized bone, we used fibrin glue. The Wagner SL stem was inserted until it achieved a stable position in the host distal femoral bone. However, at the time of surgery, we did not have a trial system of the Wagner SL revision stem at our institution. Acetabular revision was performed in 19 hips (47.5%) simultaneously. The stem size is presented in Table 2. Weight-bearing was encouraged within 2–8 weeks of surgery.
Size of the Wagner SL stem.

SL: self-locking.
Clinical evaluation
Japanese Orthopedic Association’s hip scoring system (JOA hip score) was used to evaluate the clinical function before surgery and at the latest follow-up, and the results were classified as excellent (90–100), good (80–89), fair (70–79), or poor (<70). 11 Similar to the Harris hip score, 12 the JOA hip score includes analysis of pain (0–40), range of motion (0–20), ability to walk (0–20), and daily activities (0–20). Because thigh pain was included in the JOA hip score, we did not evaluate it separately. Complications, such as dislocation, intraoperative fracture, and infection, were reviewed according to the medical records.
Radiographic evaluation
The standard anteroposterior and lateral hip radiographs at the latest follow-up were compared with immediate postoperative images, and the radiographs in the intervening period were also reviewed. Parameters, including stem subsidence, remodeling of the proximal femoral bone, bone restoration, stem fixation, incorporation of allograft bone, and heterotopic ossification, were separately examined by two surgeons (JTZ and KU).
Stem subsidence was measured using the distance from the tip of the greater trochanter to the stem shoulder. 13 If the stem subsidence was >10 mm, it was considered as significant. 7 Remodeling of the proximal femoral bone was classified as A (developing defects), B (stable defects), or C (osseous restoration). 14 Bone restoration of the femur was quantitatively measured as the ratio of the width of the cortical and cancellous bone and the outside diameter of the femoral shaft at a level 1 cm distal to the inferior margin of lesser trochanter. 15 Stem fixation was graded as stable, fibrous stable, or unstable. Stability was defined as a stem with no progressive migration and minimal or no radiopaque line formation around the stem. Fibrous stability was defined as a stem with no progressive migration and extensive radiopaque line formation, and instability as progressive subsidence or migration and divergent radiolucent lines surrounding the stem. 16 Incorporation of the grafted bone was evaluated according to the trabeculae between the grafted and the host bones. 7 Heterotopic ossification was classified into four stages according to the criteria by Brooker et al. 17 We recorded the heterotopic ossifications that were more severe than Stage III.
Statistical analyses
Kaplan–Meier survivorship analysis with 95% confidence intervals (CIs) was performed to evaluate the survival rates. The end points were (1) stem re-revision for aseptic loosening, (2) stem re-revision for any reason (aseptic loosening, infection, dislocation, and periprosthetic fracture), and (3) stem re-revision for any reason and stem subsidence ≥10 mm as end points. The preoperative JOA hip score was compared with that at the time of the latest follow-up using Student’s t-test. Cox regression analysis was used to analyze the influence of intraoperative fractures on the survival rate of the Wagner SL stem. The values of p < 0.05 were considered to indicate significant differences. Statistical analyses were performed using SPSS statistics 21 (SPSS Inc., Chicago, Illinois, USA).
Results
Forty hips (38 patients) were available for review at a mean follow-up of 15.7 years (range 5.5–22.8 years). We could review the intact JOA hip score of 30 patients. The mean JOA hip score increased from a preoperative value of 46.0 (range 10–64) to 75.3 (range 44–96) at the latest follow-up (p < 0.001).
We evaluated the radiographic data of all 40 hips (38 patients). The radiographic results are presented in Table 3. The mean stem subsidence was 2.3 mm (range 0–30 mm). Four (10%) hips had subsidence ≥10 mm (mean 19.8 mm; range 12–30 mm). Two hips (5%) had symptoms suggesting stem loosening, and there was no progressive subsidence in the other 38 stems. Bone ingrowth was identified in 27 hips (67.5%) and fibrous fixation in 11 hips (27.5%). Restoration of the proximal femoral bone was observed in 25 hips (62.5%). Radiographic signs implying incorporation of the grafted bone were noticed in 28 hips (70.0%).
Radiographic results.

Complications included dislocation in 2 hips (5.0%), intraoperative femoral fracture in 10 hips (25%), heterotopic ossification Stage III in 1 hip (2.5%), greater trochanteric osteotomy nonunion in 4 hips (10.0%), and infection in 2 hips (5.0%). Seven of the 10 intraoperative femoral fractures occurred during insertion of the Wagner SL stem, and 3 during removal of the initial stem. Cox regression analysis showed no influence of intraoperative fractures on the survival rate of the Wagner SL stem (p = 0.367).
The 15.7-year Kaplan–Meier survival rates were 96.6% (95% CI 89.9–100), with “stem re-revision for aseptic loosening” as the end point, 91.7% (95% CI 82.5–100) with “stem re-revision for any reason” as the end point, and 88.7% (95% CI 78.1–99.3) with “stem re-revision for any reason and stem subsidence ≥ 10 mm” as the end point (Figure 1(a)–(c)).
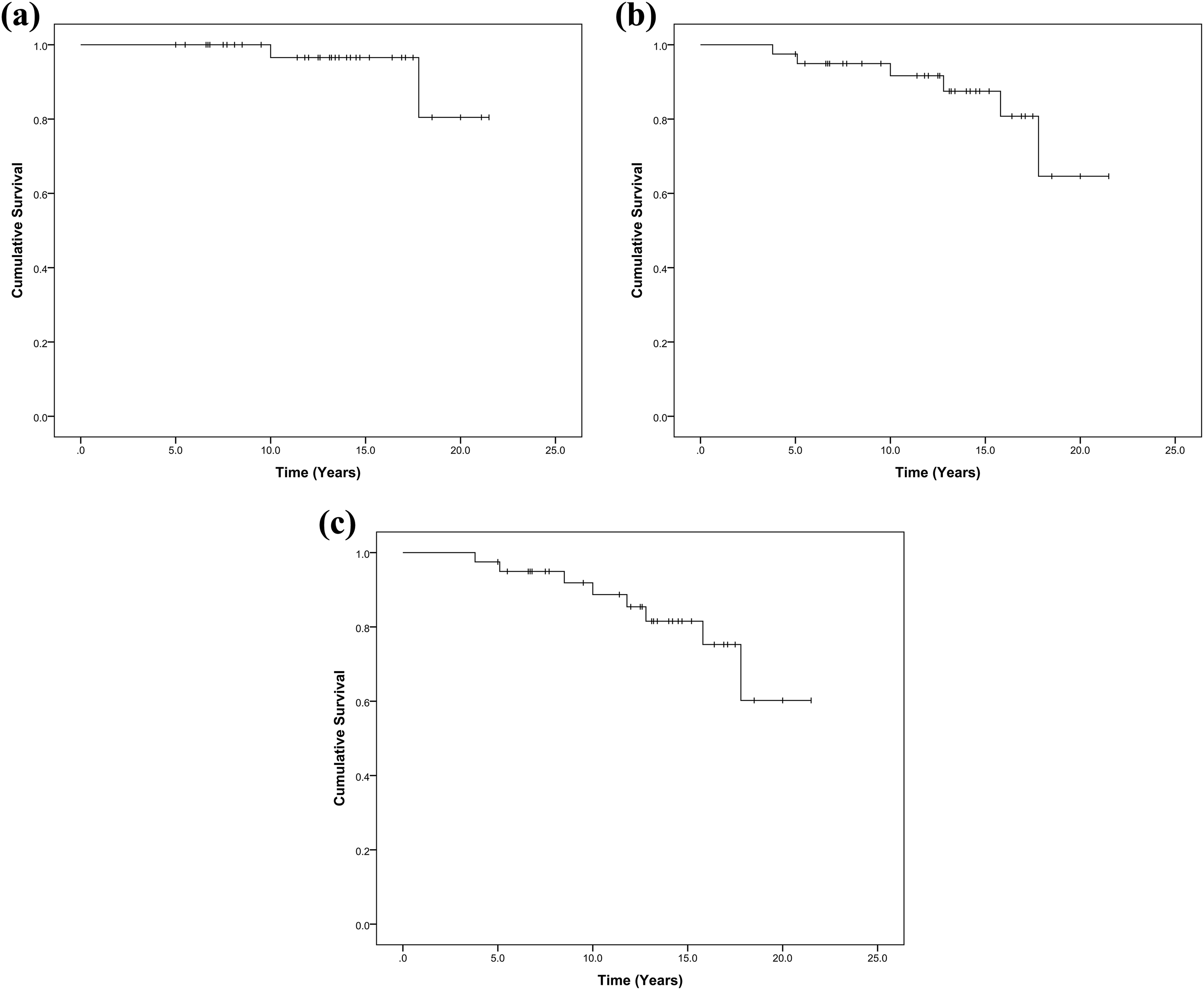
Kaplan–Meier survivorship curve with (a) “stem re-revision for aseptic loosening” as the end point, (b) “stem re-revision for any reason” as the end point, and (c) “stem re-revision for any reason and stem subsidence ≥10 mm” as the end point. The small vertical lines show the follow-up duration of censored event.
Re-revision was performed in 6 hips: one hip was re-revised for aseptic loosening after 17.8 years; one hip that had aseptic loosening accompanied by dislocation was re-revised after 10 years; one hip was re-revised for dislocation after 12.8 years; one hip was re-revised for periprosthetic fracture after 5.1 years; and two hips were re-revised for infection after 3.8 and 15.8 years, respectively.
Discussion
Severe proximal femoral bone defects are challenging for performing revision THA. 4,18 According to the degree and extent of bone defect, various methods of reconstruction, such as impaction bone grafting, structural allografts, and allograft prosthesis composite, have been described. 19,20 For Paprosky type II and III bone defects, we performed the impaction bone grafting technique with the Wagner SL stem. However, for more massive bone defects, such as Paprosky type IV, allograft prosthesis composite was used. 21 In this series, the Wagner SL stem and bone allograft for Paprosky type II and III bone defects were reviewed. The bone allograft technique was described in a recent paper. 21 All allografted bones were provided by the bone bank in our department. For reconstruction of the proximal femur, morselized bone was encased in fibrin glue. At the time of the latest follow-up, radiographic signs implying incorporation of the grafted bone were noticed in 28 hips (70.0%). Gutiérrez et al. 8 also reported incorporation of the grafted bone in their study on the Wagner SL stem. We believe that the preservation of blood supply of the proximal femur and the excellent histocompatibility of the Wagner SL stem are essential for the incorporation of grafted bone. 22
With a fluted tapered design, the Wagner SL stem could be stably fixed in the distal portion of femur, where enough bone stock was preserved. Compared with modular stem, one advantage of the Wagner SL stem is the low risk of stem fracture. Modular stem was designed with variable anteversion to reduce the dislocation rate. However, Regis et al. 23 compared the results of the Wagner SL stem and a modular stem (Profemur R) and found that the modular stem had no effect in reducing the dislocation rate. Furthermore, the Wagner SL stem has a low risk of stress shielding, which was reported to be associated with extensively porous-coated stem. 18
A few authors have reported their results of the Wagner SL stem with bone grafting, and the mean follow-up periods vary from 2.3 to 8.4 years (Table 4). 5,8,18,22,24,25 The advantage of our study is the long period of follow-up. In a mean 15.7-year follow-up period, the cumulative survival rate was 96.6%, which was comparable to that reported in previous studies. 5,7,16,22 Two stems were re-revised due to loosening. Loosening in one stem might be associated with the deformed femoral union at the tip of stem after femoral osteotomy, and the other one had a progressive subsidence for low-grade infection. When the latter stem was re-revised because of dislocation, the subsidence was 30 mm. We believe that the dislocation was associated with massive progressive subsidence for low-grade infections.
Published results of revision THA with the Wagner SL stem and bone grafting.

THA: total hip arthroplasty; SL: self-locking.
In this study, the dislocation rate was 5%, which is similar to that of a previous study 22 and slightly lower than other studies. 7,23 Two stems were re-revised due to infection and four greater trochanters were absorbed after nonunion.
There was a major disadvantage in the revision procedures with the Wagner SL stem. At the time these serial surgeries were performed, a trial system of the Wagner SL stem was not available in Japan, which may be associated with a high rate of intraoperative fractures. Seven intraoperative fractures occurred when we were trying to insert the new stem. However, the other three intraoperative fractures occurred when we were trying to remove the initial stem. All of these were fixed using the cable system. We believe that the careful preoperative measurement and intraoperative implantation would be helpful to solve this problem. Fortunately, Cox regression analysis showed that intraoperative fractures had no negative influence on the survival rate of the Wagner SL stem. This study is retrospective in nature and does not have a control group. We only used the Wagner SL stem in Paprosky type II and III bone defects, and thus, there could have been a limitation of selection bias.
Conclusion
This study demonstrates for encouraging long-term results of the Wagner SL stem with bone allograft in revision THA. This method allows incorporation of the grafted bone into the host bone. Except for the incidence of intraoperative fractures, we did not find an increased number of complications. We believe that the Wagner SL stem with bone allograft is a clinically beneficial option for Paprosky type II and III bone defects in revision THA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.