
Abstract
Introduction:
Reconstruction of acetabulum in case of bone defects can be challenging. The aim of this retrospective study was to investigate the 10-year survival of trabecular tantalum metal (TM) acetabulum component in revision hip arthroplasty operations and to evaluate complications.
Methods:
A total of 100 consecutive acetabulum revision hip arthroplasties (100 patients) were operated on between May 2004 and October 2006 at Kuopio University Hospital. The mean follow-up time was 9.4 years and the median was 11.5 years (SD 4.118; range 0.1–13.4 years). Kaplan-Meier survival analysis was performed to study the survival of patients to re-revision surgery. Intra- and postoperative complications and reasons for re-revision were evaluated.
Results:
The Kaplan-Meier analysis showed a cumulative proportion of revision hip survivorship of 66% at 13.4 years (SE 0.403, 95% CI, 10.886–12.466) based on the need for further re-revision surgery for any major reason. The Kaplan-Meier survival analysis of time to re-revision surgery due acetabular component loosening showed a cumulative proportion of survivorship of 98.9% at 13.4 years (SE 0.136; 95% CI, 12.998–13.529). There were a total of 41/100 complications and the most common complication was dislocation (24/100). Re-revision for any major reason was performed on 18/100 of the revision arthroplasties. The mean time to re-revision was 4.9 years (SD 5.247; range 0.1–13.2 years).
Discussion:
The trabecular TM acetabular component gives excellent outcomes regarding stability and fixation to the acetabulum in acetabulum revision hip arthroplasty at a minimum of ten years of follow-up. However, acetabular component malposition and the small head size (28 mm) are risk factors for dislocation.
Introduction
Osteolysis and aseptic loosening remain the leading indications for revision total hip arthroplasty. 1 Bone defects in acetabular revision of total hip arthroplasty are challenging due to unsatisfactory bone stock for implant fixation. Since the 1970s, bone grafting with cemented acetabulum component fixation or a reinforcement cage has been the standard treatment for bone defects. 2 However, after 10 years of follow-up, a high failure rate of these type acetabulum revisions has been reported. 2 Risk factors for acetabular component loosening have be found to be young age, male gender, rheumatoid arthritis, incomplete cementation and elevated cup position. 3 1 solution to reduce high failure rate of revised acetabulum components is to use trabecular metal (TM) components (Trabecular Metal Revision Component, Zimmer, Warsaw, IN, USA), which are relatively inert in vivo, corrosion resistant and have good biocompatibility with similar elasticity to subchondral bone. 4 Trabecular TM acetabular components have advantages over cemented acetabulum components and reinforcement gages, with less reported periprosthetic stress shielding and rapid infiltration of fibrous and osseous tissues, leading to excellent attachment strength. 5
The typical complications after revision hip arthroplasty are dislocation, periprosthetic joint infection, nerve injuries, periprosthetic fractures and acetabulum component loosening.6,7 Trabecular TM acetabular components have shown good mid- and long-term results with less acetabulum component loosening in acetabular revision even with significant acetabular bone deficiency.8,9
In this retrospective study, we investigated the 10-year survival and complications of the first 100 consecutive trabecular TM acetabulum components used in revision operations at Kuopio University Hospital (KUH).
Methods
Study design
This was a retrospective single-centre (KUH) study. The primary outcome was survival of revised patients. Secondary outcomes were intra- and postoperative complications.
Patients
A total of 100 acetabular revision hip arthroplasties in 100 patients were performed between May 2004 and October 2006. These patients were the first 100 consecutive acetabular revision hip arthroplasty patients in whom we used a trabecular TM component. The patients were identified from our department’s longitudinal database. The patients were routinely clinical followed with a 3-month postoperative visit and some patients were seen after that in extra follow-up evaluations from 1–5 years after the revision surgery. All of these 100 consecutive patients lived in our hospital district and we are able to check all of the radiographs taken or revision surgeries performed during the follow-up period. The mean follow-up time was 9.4 years and median was 11.5 years (standard deviation [SD] 4.118; range 0.1–13.4 years). None of the patients was lost to follow-up. Follow-up ended on 31 December 2017 or with major re-revision surgery or death. Major revision surgery was defined as femur or acetabulum component change due to aseptic loosening or periprosthetic fracture or infection. There were 2 minor revision surgeries during the follow-up; 1 was postoperative haematoma evacuation on the 1st postoperative day and 1 was trochanter plate removal 3.2 years after revision surgery. A total of 37/100 (37%) of the patients had died during follow-up and the date of death was collected from the patient’s medical records. 1 patient died due to infection complications following revision surgery. Demographic data (age, gender, side, indication for surgery, date of surgery) and surgical details were collected from medical records.
There were 50 males and 50 females. The mean age of the patients at the time of revision was 69.8 (SD 8.0; range 48.0–91.0) years and a median body mass index was 27.5 (SD 3.7; range 18.8–36.1) kg/m². The mean time from the index or previous hip surgery to revision surgery was 9.8 years (SD 4.4; range 21 days–23 years). The left hip was revised in 45/100 patients. Diagnoses leading to revision surgery and surgical approach are given in Table 1. A total of 13 consultant orthopaedic surgeons performed the operations, and the mean surgery time was 136 (SD 51.4; range 43–300) minutes. Allograft bone was used in 56 hips and the femur component was revised in 7 hips. Postoperative full weight-bearing was allowed for 53 hips, partial weight-bearing for 46 hips and no weight-bearing for 1 hip. All the patients had enoxsaparin antithrombotic prophylaxis and antibiotic prophylaxis with cefuroxime in 99 hips and vancomycin in 1 hip. Mean blood loss was 1137 (SD 716.1; range 100–3600) ml and blood transfusion was given for 53 hips with donor blood in 11 hips, cell saver in 24 hips and with both of these supplied in 17 hips.
Revision hip arthroplasty indications and surgical opening.
Implants
An uncemented trabecular TM acetabular component was used in all patients. The shell was made entirely from porous tantalum and there were monoblock and revision type options, which allow the use of screws and augmentation. Monoblock components were used in 35 hips and revision components in 65 hips with additional screws in 45 hips and augmentation in 5 hips. The median number of screws was 2 (range 2–6). All liners were unconstrained and 10° or 20° of orientation heightening was used in 65 hips (10° orientation in 10 hips and 20° orientation in 35 hips). Orientation heightening was approximated to inclination angles so that 10° elevation lowered it by 5° and raised anteversion by 5°. 20° orientation lowered inclination by 10° and raised anteversion by 10°. The head size was 28 mm in all hips.
Radiological analysis
Radiological assessments were conducted from the anteroposterior (AP) full weight-bearing and true-lateral postoperative radiographs at a follow-up visit 3 months postoperatively. Acetabular bone defects were classified according to the method of Paprosky, Perona and Lawrence. 9 Preoperatively, 22/100 patients had a Paprosky Type I defect, 7/100 Paprosky Type IIA, 30/100 Paprosky Type IIB, 32/100 Paprosky Type IIC, 6/100 Paprosky Type IIIA and 3/100 Paprosky Type IIIB. Anteversion and inclination angles of the acetabular component were measured according to the methods described by Widmer and Murray.10,11 The number of acetabular components that were positioned within the safe zone (5–25° anteversion and 30–50° inclination angles) described by Lewinnek was analysed. 12 Picture archiving and communication system (PACS) was used (Sectra Workstation IDS7 [ver.15.1.8.5] PACS) for image evaluation.
Statistical analysis
Kaplan-Meier analysis was used to study implant survival. The primary outcome was re-revision surgery for any reason or due to acetabular component loosening. The comparison of continuous data was carried out using a Mann-Whitney U-test. For categorical data, a chi-square test was used. Independent samples t-tests were used for functional score analyses. The Cox proportional hazard model was used due to the heterogeneity of the involved variables affecting the risk of re-revision surgery. Selected variables for the Cox analysis are known to be potentially cofounding factors for arthroplasty register database studies. The selected variables were age, gender, body mass index, operation diagnosis, Paprosky classification and acetabulum component position. The selection of these adjustment variables was based upon our own hypotheses and previous literature. All p-values ⩽0.05 were considered statistically significant. All data were analysed using SPSS (SPSS Inc., Chicago, IL, USA. Ver. 25.0.0, IBM).
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. No informed consent was required. The Ethical board of Kuopio University Hospital (KUH) approved study (ETMK: 168/2016).
Results
The Kaplan-Meier analysis showed cumulative proportion of revised hips survivorship of 66% at 13.4 years (standard error [SE] 0.403; 95% confidence interval [CI], 10.886–12.466) using the need for further re-revision surgery for any major reason as the endpoint (Figure 1). The Kaplan-Meier survival analysis of time to re-revision surgery due to acetabular component loosening showed cumulative proportion of survivorship to be 98.9% at 13.4 years (SE 0.1; 95% CI, 13.0–13.5) (Figure 2).
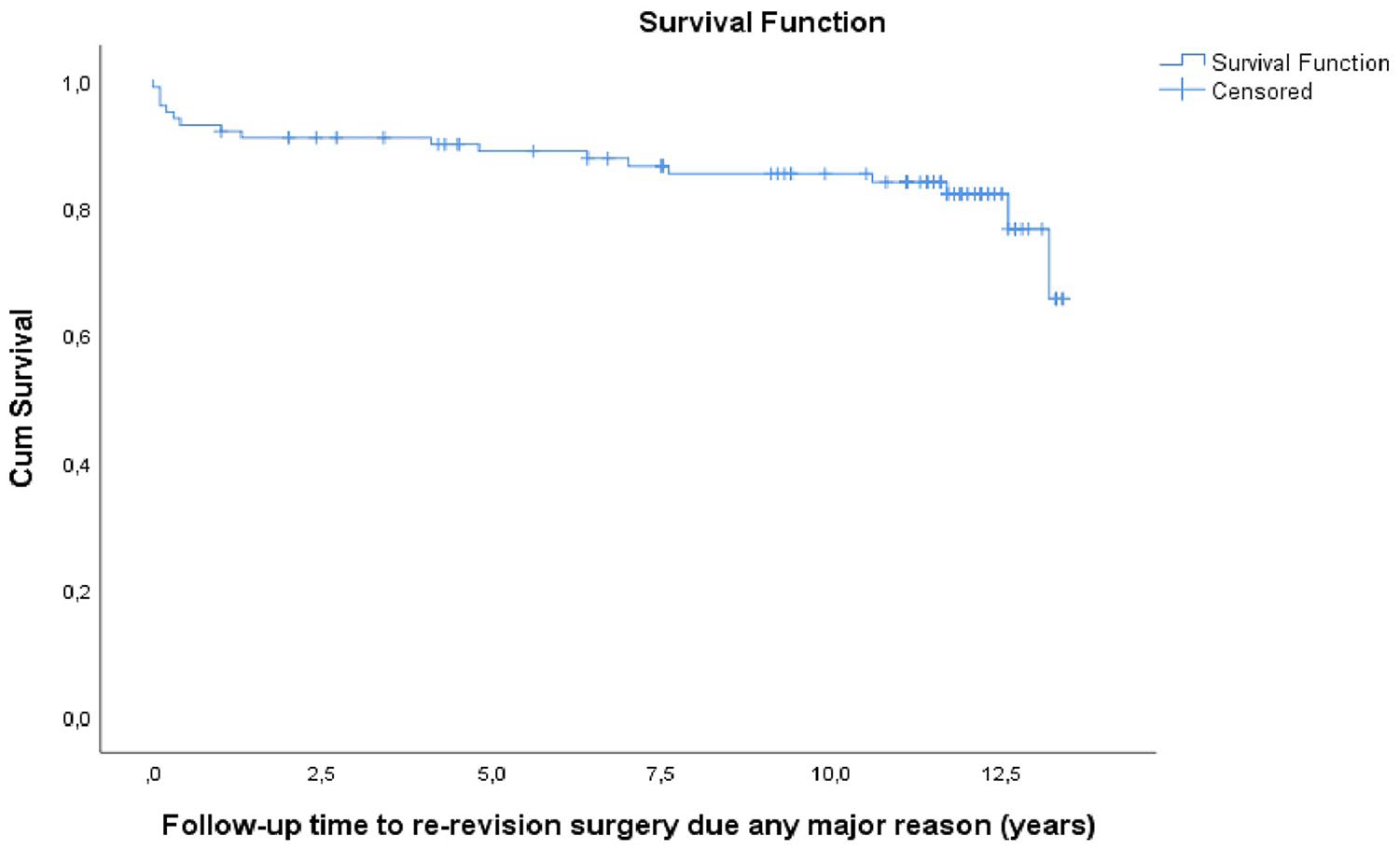
The Kaplan-Meier survival analysis of time to re-revision surgery for any major reason showed a cumulative proportion of survivorship of 66% at 13.4 years (SE 0.4; CI 95%, 10.9–12.7).
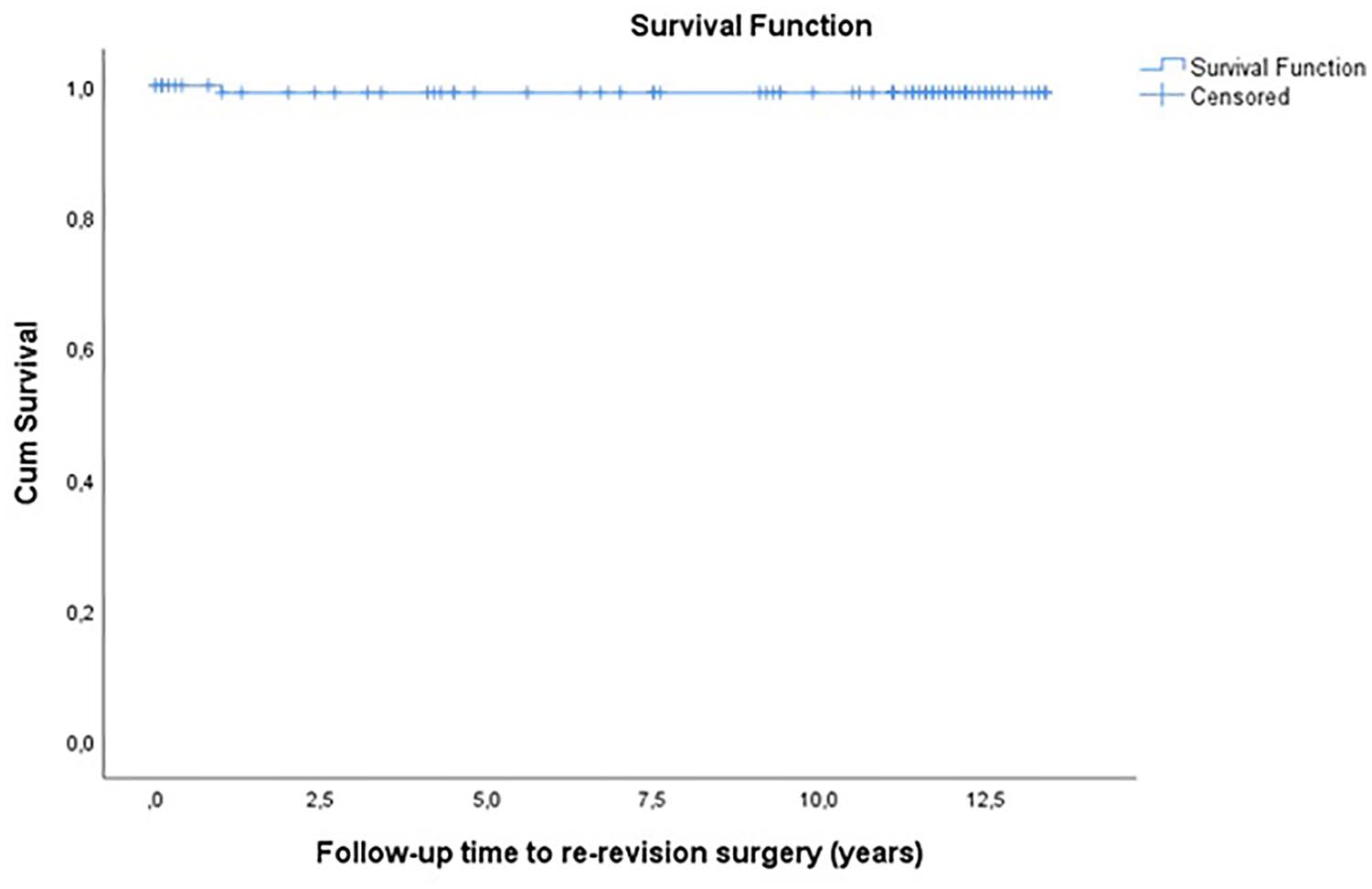
The Kaplan-Meier survival analysis of time to re-revision surgery due to acetabular component loosening showed a cumulative proportion of survivorship of 98.9% at 13.4 years (SE 0.1; 95% CI, 13.0–13.5).
There were 24 different types of primary total hip arthroplasty systems in 99 patients; the earliest index primary hip arthroplasty was performed in 1983. There was one patient who had a failed acetabulum fracture surgery which led to a later hip dislocation and later on to total hip arthroplasty with a TM acetabular component. The mean time from the index surgery to revision surgery was 9.8 (SD 4.428; range 21 days–23 years) years.
There were 41/100 (41%) complications intra- and postoperatively (Table 2). A total of 20/100 (20%) patients were underwent re-revision surgery during the follow-up time and 2 of these were minor re-revisions. The mean follow-up time to major re-revision surgery was 4.9 years (SD 5.247; range 0.1–13.2 years). The reasons for major re-revision are given in Table 2. The major re-revision patients (n = 18) were analysed in more detail and compared to non-revised patients with the Cox proportional hazard model (Table 3). Male gender and monoblock type acetabulum component were statistically significant risk factors for re-revision surgery (Table 3).
Complications and reasons for re-revisions after revision surgery.
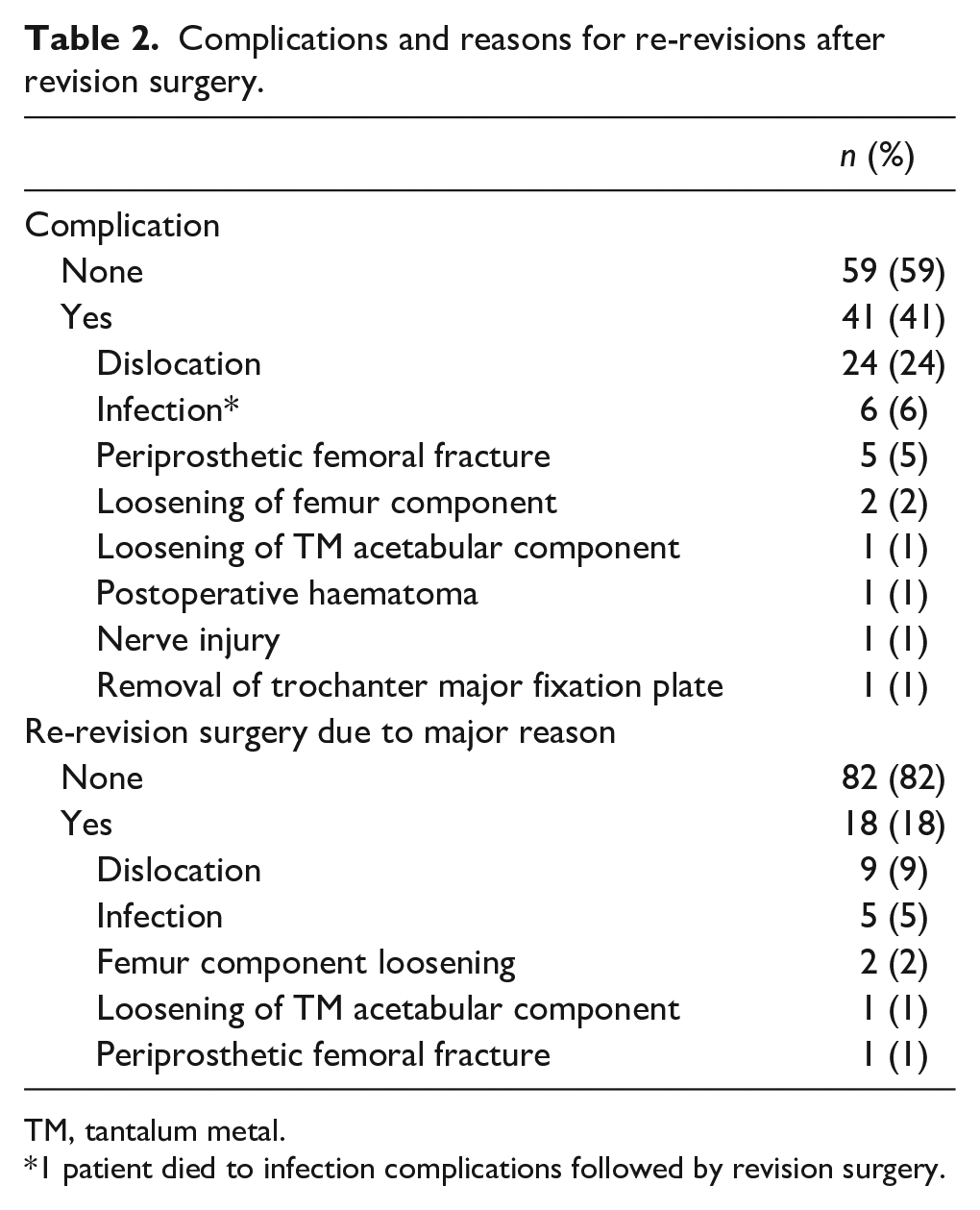
TM, tantalum metal.
1 patient died to infection complications followed by revision surgery.
The Cox proportional hazard model of re-revised patients compared to non-revised patients.
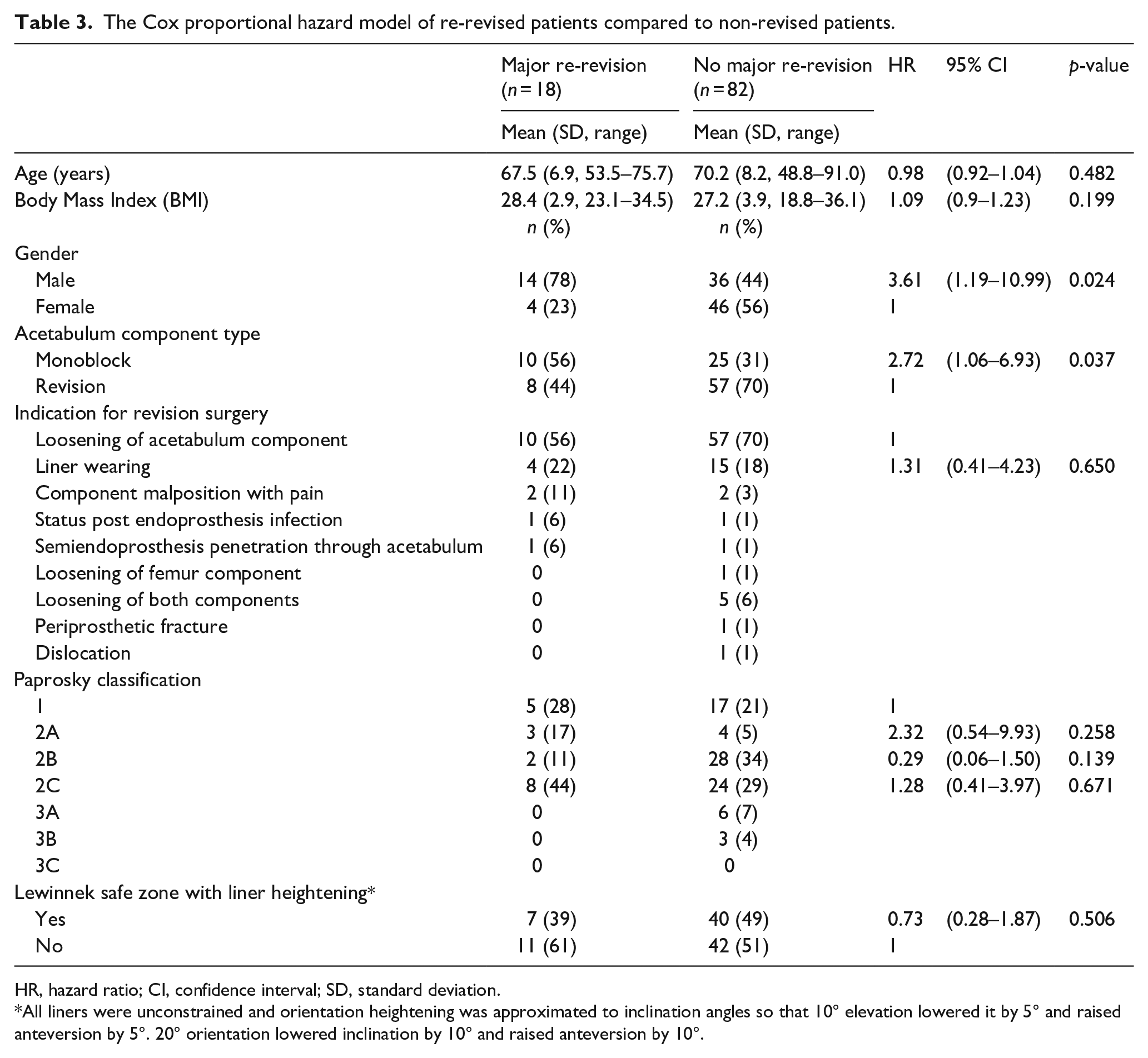
HR, hazard ratio; CI, confidence interval; SD, standard deviation.
All liners were unconstrained and orientation heightening was approximated to inclination angles so that 10° elevation lowered it by 5° and raised anteversion by 5°. 20° orientation lowered inclination by 10° and raised anteversion by 10°.
The mean acetabulum component anteversion and inclination angles are given in Table 4 and an approximation of elevation liner rim hike is also shown in Table 4. Acetabulum component positioning was not a statistically significant risk factor for revision (Table 3).
Postoperative radiographic findings of revised acetabulum components with patients imaged while standing.
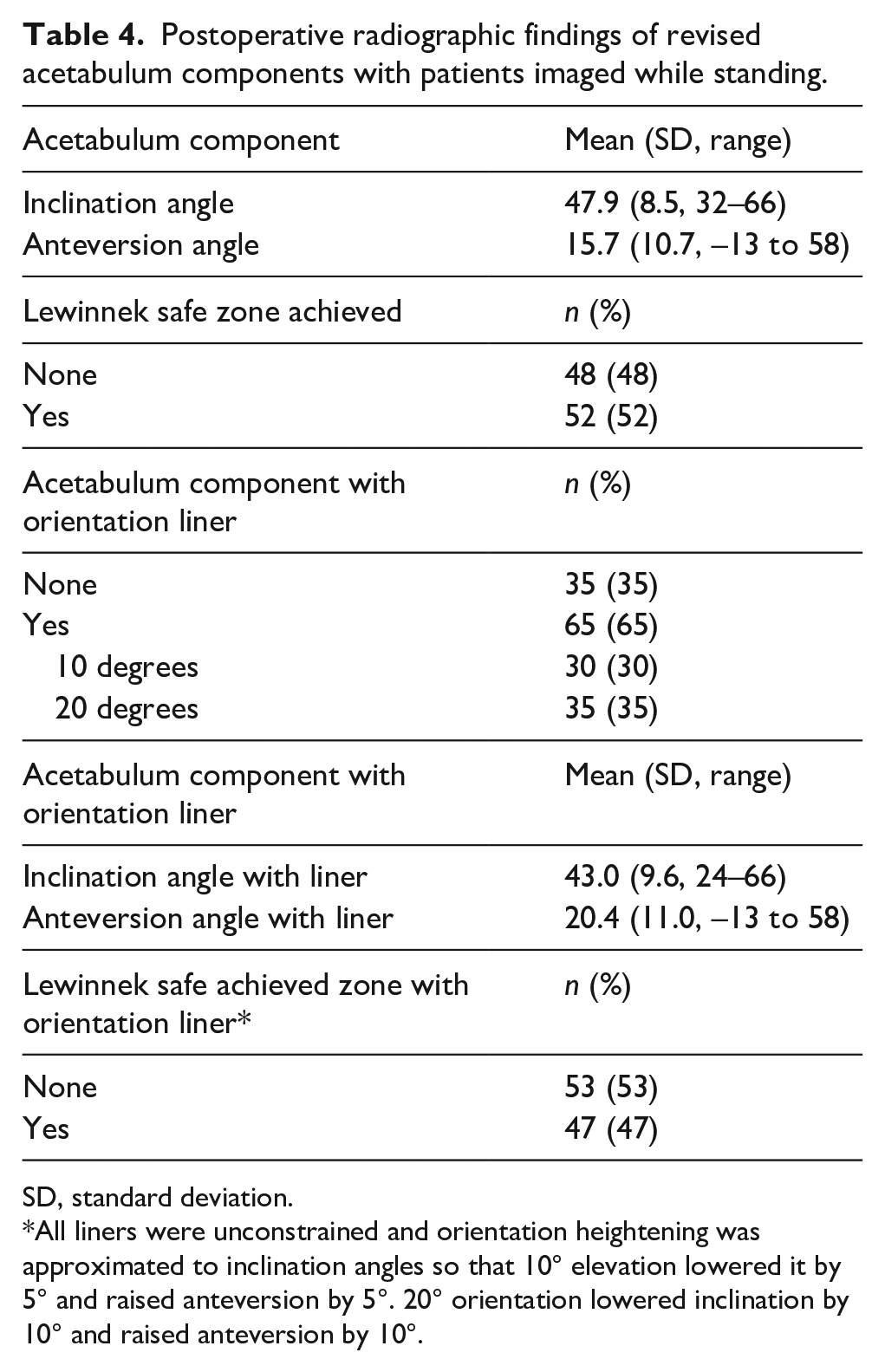
SD, standard deviation.
All liners were unconstrained and orientation heightening was approximated to inclination angles so that 10° elevation lowered it by 5° and raised anteversion by 5°. 20° orientation lowered inclination by 10° and raised anteversion by 10°.
Discussion
Over the past decade, porous trabecular metal in general and trabecular metal made of tantalum have gained popularity over traditional cemented and cementless acetabulum components for reconstruction of a failed acetabular component. Compared to traditional components, porous tantalum has some advantages, such as high porosity, high frictional characteristics and a low modulus of elasticity. 5 Furthermore, porous tantalum has a low migration rate, which predicts good long-term survival, and the use of additional screws improves fixation. 13 These advantages have been shown to lead to excellent early- and medium-term outcomes due to the stability and longevity of the components. Porous tantalum has been used as a primary fixation with any type of bone loss and shown good results.2,14 A recent 5-year follow-up showed 97% survivorship of porous tantalum revision components. 15 A minimum of 10-year follow-up study showed survivorship of 96% when the further revision of the acetabulum component was used as the endpoint and 92% when any reason for revision was used as the endpoint. 6 Our findings agree with these studies since only 1 acetabular component loosening occurred. The revision rate due acetabular component loosening was 98.9% at 13.4 years in our cohort. However, overall survivorship was 59.6% when the end point was revision due to any reason. A total of 20 patients were re-revised of which 18 were due to major reason. Previous studies have reported a similar incidence of re-revision (15.8–19%) after revision total hip arthroplasty.16,17 Penrose et al. 16 found more re-revisions in females and in patients under 69 years, while in our study there were more revisions carried out on males and on more elderly patients. The reasons for our finding are somewhat unclear, but it might be that older males have more dislocations leading to revision due to suboptimal acetabular component positioning and weakened muscle strength.
The most common complication in the present study was dislocation with a prevalence of 24%. The commonly reported incidence of dislocation after revision hip arthroplasty varies between 14.4–33.3%, which is similar to our study.18,19 Risk factors for dislocation have been found to be surgical approach and technique, operative diagnosis, arthroplasty type, hip anatomy, patient compliance and other diseases affecting movement and muscle strength. 20 However, the risk factors for instability after revision hip arthroplasty are not necessarily the same as those after primary hip arthroplasty. Underlying soft tissue deficiency after previous surgery may have a significant impact on joint stability. 18 Dislocation after revision hip arthroplasty has been reported to lead to a re-revision surgery rate as high as ⅓ or even ½ of cases due to recurrent instability. 17 We had similar results, as dislocation led to re-revision surgery in 9/24 (38%) dislocated hips. We found that there were more dislocations in males (14/24) and patients with a posterior approach (18/24) and with an acetabulum component position outside of Lewinnek’s safe zone (15/24). 1 possible reason for the high rate of dislocation in our study might be that all head sizes were 28 mm, which is a well-known risk factor for dislocation compared to larger 36–40 mm head sizes. 21
The rate of infection after revision total hip arthroplasty has been reported to vary between 8.3–11.0%11,12 In our study, the infection rate was 6%, which is lower compared to other studies, but higher compared to rates after primary total hip arthroplasty.8,11,12 Infection led to re-revision surgery in 5 patients and for 1 patient it was not possible to operate due to poor condition; this patient died from a serious infection. In infection-revision cases, the head component was changed in all patients and no re-re-revisions surgeries were needed during the follow-up time for these infection patients. In a large sample size study, the re-revision rate after infection was 38%. 17 The incidence of periprosthetic fracture after revision hip arthroplasty has been reported to vary between 1.1–12%.22,23 We reported an incidence of periprosthetic femoral fracture of 5% (5/100), and 3 of these cases were treated conservatively. In a previous study, similar results were shown as re-revision surgery due to periprosthetic fractures being carried out in 39% of cases. 22
To our knowledge, there are no previous studies of revision trabecular TM acetabular components with the same size of population and as long follow-up of consecutively operated patients, as in our study. However, our study has several limitations. This was a retrospective study based on patient record data and the typical deficiencies of register studies influence our study, although all the patients were followed up after the primary revision hip arthroplasty. 1 defect of this study is the lack of patient reports of their outcome measurements. A large number of patients died during the follow-up period for some other reason than revision hip surgery or related complications. Natural mortality is a competing outcome for re-revision. Patient comorbidities were not evaluated in this study, but it has been shown that they increase mortality rate, as does ageing. 17 In patients >85 years of age, the 1-year mortality rate after revision total hip arthroplasty was 4 times higher than in patients <69 years of age. 17 In our study, the mean age of the patient at the time of revision surgery was 69.8 years with a median follow-up time of 11.4 years, which means that patients had a mean age >80 years at the end of follow-up.
In this study, 91% of the patients had a Paprosky Type I or II bone defect in which cup-bone contact is classically >50% and primary stability of the implant is obtained with a cementless cup. Excellent results in the treatment of Type I and II bone deficiency patients have been shown with porous tantalum acetabular components with survivorship of 100% in 4 years of follow-up and survivorship of 96% with a minimum of 10 years of follow-up. 14 Our findings are similar, as there was only 1 case of acetabular component loosening, which occurred in a Paprosky Type IIC patient; this re-revision was done 1 year after revision arthroplasty. The advantage of trabecular tantalum porous metal has been shown to be greater in Paprosky Type III when compared to other cementless cup materials.14,24 In Paprosky Type III, cup-bone contact is <50% and, under these conditions, biological fixation is uncertain, with loosening rates as high as 70% after 5 years of follow-up.14,25
Conclusion
This study investigated the first consecutive 100 TM acetabular component revision hip arthroplasties performed in our clinic. TM acetabular components shows good longevity and can be regarded as an excellent choice in acetabulum revision; however, acetabular component malposition and small head size (28 mm) are risk factors for dislocation. To show good longevity, we have continued using this component, and today we have performed over 800 trabecular TM acetabular component procedures in our clinic.
Footnotes
Acknowledgements
We thank Tuomas Selander MSc for participation in the interpretation of the results and analyses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.