
Abstract
Purpose:
Degenerative disk disease is a global and common debilitating condition with substantial healthcare and economic costs. Disc-Fx is a relatively new minimally invasive, percutaneous nucleo-annuloplasty procedure aimed to alleviate symptoms of discogenic back pain via manual discectomy with nuclear and annular modification via means of radiofrequency ablation. The aim of this retrospective study is to report the 1-year outcomes, efficacy and safety of the percutaneous nucleo-annuloplasty procedure for treatment of discogenic back pain in the local Hong Kong population.
Methods:
This retrospective study consists of 16 patients with a total of 24 levels from 2017 to –2019 with at least 6 months of chronic back pain failing conservative management, MRI-confirmed disc degeneration, and who have undergone percutaneous nucleo-annuloplasty via Disc-Fx procedure. All patients had plain radiography and magnetic resonance imaging prior to procedure. Percutaneous nucleo-annuloplasty was only performed in patients with confirmed discogenic back pain via a positive provocative test on discography.
Results:
The mean functional outcome of Oswestry Disability Index improved from 46.25 points preoperatively to 24.12 at the of 1-year follow-up (p-value = 0.00). The Numerical Pain Rating Scale improved from 6.25 points to 4.4 points (p-value: 0.01) and 14.56 points to 8.85 points (p-value = 0.01) at preoperative to 1-year post-procedure respectively. There were no reported procedural related complications in the study population.
Conclusion:
The procedure of percutaneous nucleo-annuloplasty shows to be a relatively safe procedure that can be considered in patients with discogenic back pain. Larger studies would be desired to draw further conclusions about its efficacy.
Introduction
Chronic low back pain is a global and common debilitating condition associated with significant healthcare and economic costs 1 —degenerative disc disease is just one of many causes of low back pain. The true prevalence of degenerative disc disease is difficult to ascertain as often disc degenerations appear asymptomatic. 2 Among patients with chronic low back pain, a positive discography along with disc degeneration on imaging has been shown to be present in up to 37%. 3
Discogenic back pain is generally treated conservatively—namely with rest, analgesia, activity modification, and physiotherapy. However, there were previously limited options for those with discogenic back pain that has failed conservative management. Disc-Fx is a relatively new minimally invasive, percutaneous nucleo-annuloplasty procedure aimed to alleviate symptoms of discogenic back pain via manual diskectomy with nuclear and annular modification via means of radiofrequency ablation. As of writing, there are no current studies examining the outcomes of the local Hong Kong population treated with percutaneous nucleo-annuloplasty and radiofrequency ablation. Results from early studies, 4,5 as well as studies from a Chinese population 6,7 suggest that nucleo-annuloplasty may be a reasonable treatment option in those with degenerative disc disease. The aim of this retrospective study is to report the 1 year outcomes, efficacy and safety of the percutaneous nucleo-annuloplasty procedure for the treatment of discogenic back pain within our local Hong Kong population spanning 2 years from January 5, 2017 to January 5, 2019.
Materials and methods
Ethics review
The study was approved by the Hong Kong East Cluster Research Ethics Committee at our institution.
Methodology
This retrospective study consists of 16 patients with a total of 24 levels from 2017 to 2019 with at least 6 months of chronic back pain failing conservative management, with MRI-confirmed disc degeneration with or without annulus tears, who have undergone percutaneous nucleo-annuloplasty via disc-Fx procedure. All patients had plain radiography and magnetic resonance imaging prior to procedure. Percutaneous nucleo-annuloplasty was only performed in patients with confirmed discogenic back pain via a positive provocative test on discography.
Technique
The procedures were performed in the operating theater with the patient prone under monitored anesthetic care. The site of needle entry was first marked under fluoroscopic guidance to locate and guide entry to the level of the targeted disc(s). The surrounding skin was prepared using aseptic technique, and the surrounding soft tissue and skin anesthetized with local lignocaine infiltration.
The first step of the procedure consisted of the entry of the spinal needle toward the targeted disc via transforaminal technique to perform a discogram. With fluoroscopic guidance, the needle was guided towards the dorsal aspect of the intervertebral disc. Once the spinal needle’s location was confirmed on both anteroposterior and lateral views on fluoroscopy, a small amount of contrast (<3 mL) was injected. Discography was deemed positive if concordant pain was reported by the patient after the injectate was given. As a positive discography was dependent on the patient’s response and reporting, it was communicated with our anesthetic colleagues that sedation was either not given or minimal at this point of procedure to prevent any potential masking of positive discography results. If the provocative test was negative, and no other targeted disc levels were present, the needle was withdrawn and the procedure was aborted. If other targeted disc levels were present, the discogram was again repeated at the other levels.
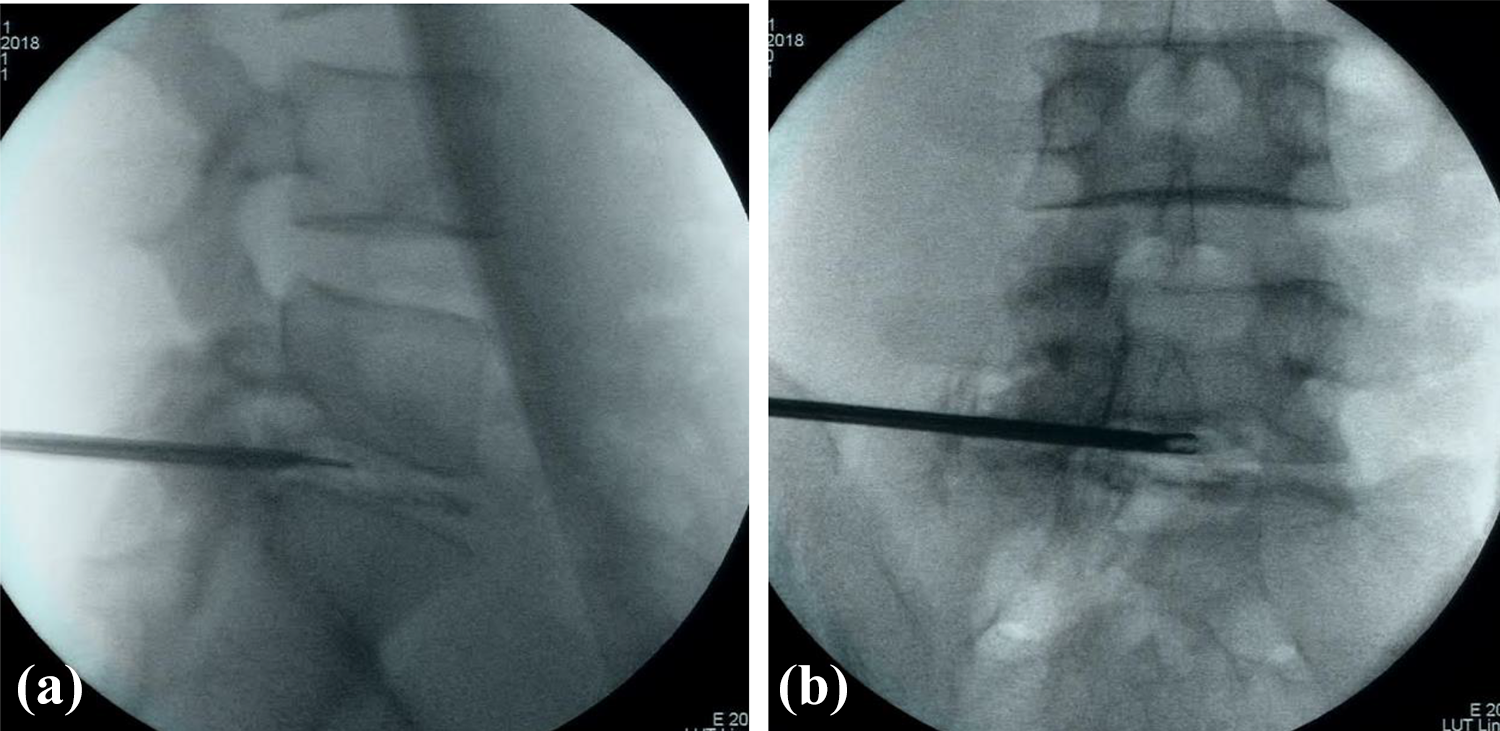
If the patient responded with a positive discography provocation, further sedation was given to the patient, with a small skin incision was made at the site of prior spinal needle entry. A guidewire was threaded through, with subsequent dilation with dilators to allow a 4.3 mm working cannula to be introduced. Manual diskectomy was performed using a grasping forceps, with diseased discs removed by piecemeal. Disc nuclear ablation was done using a flexible-tip bipolar probe after confirming correct position via fluoroscopy. The procedure was repeated at up to six rotational angles for adequate ablation of the nucleus. Annular modification by means of radiofrequency was performed with the flexible-tip bipolar probe with reported temperatures in-vitro up to 40 8 and 44°C 9 at the region of the annulus. The cannula was irrigated with normal saline throughout the procedure for cooling and for clearing out of any debris or materials. The procedure is demonstrated in Figures 1 and 2.
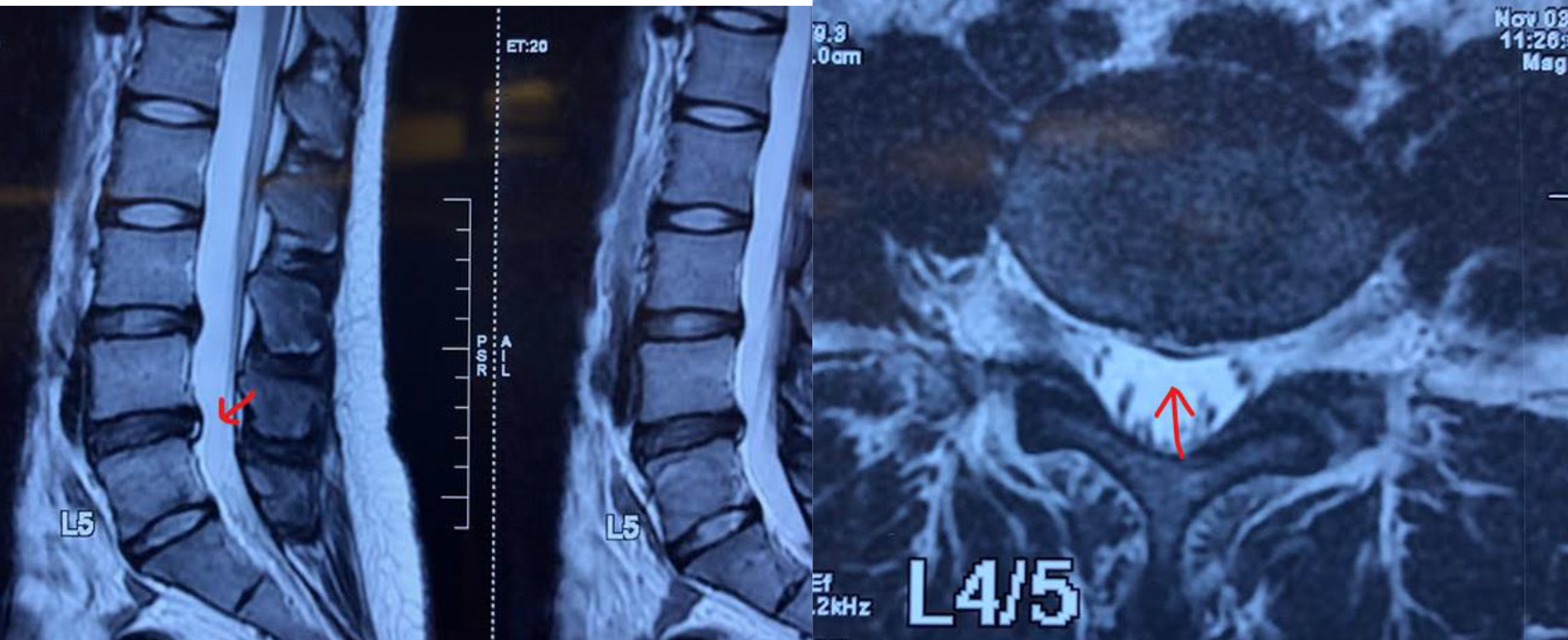
Magnetic resonance imaging of one of the patients with evidence of annular tear at level at L4/5 intervertebral disk (red arrow).
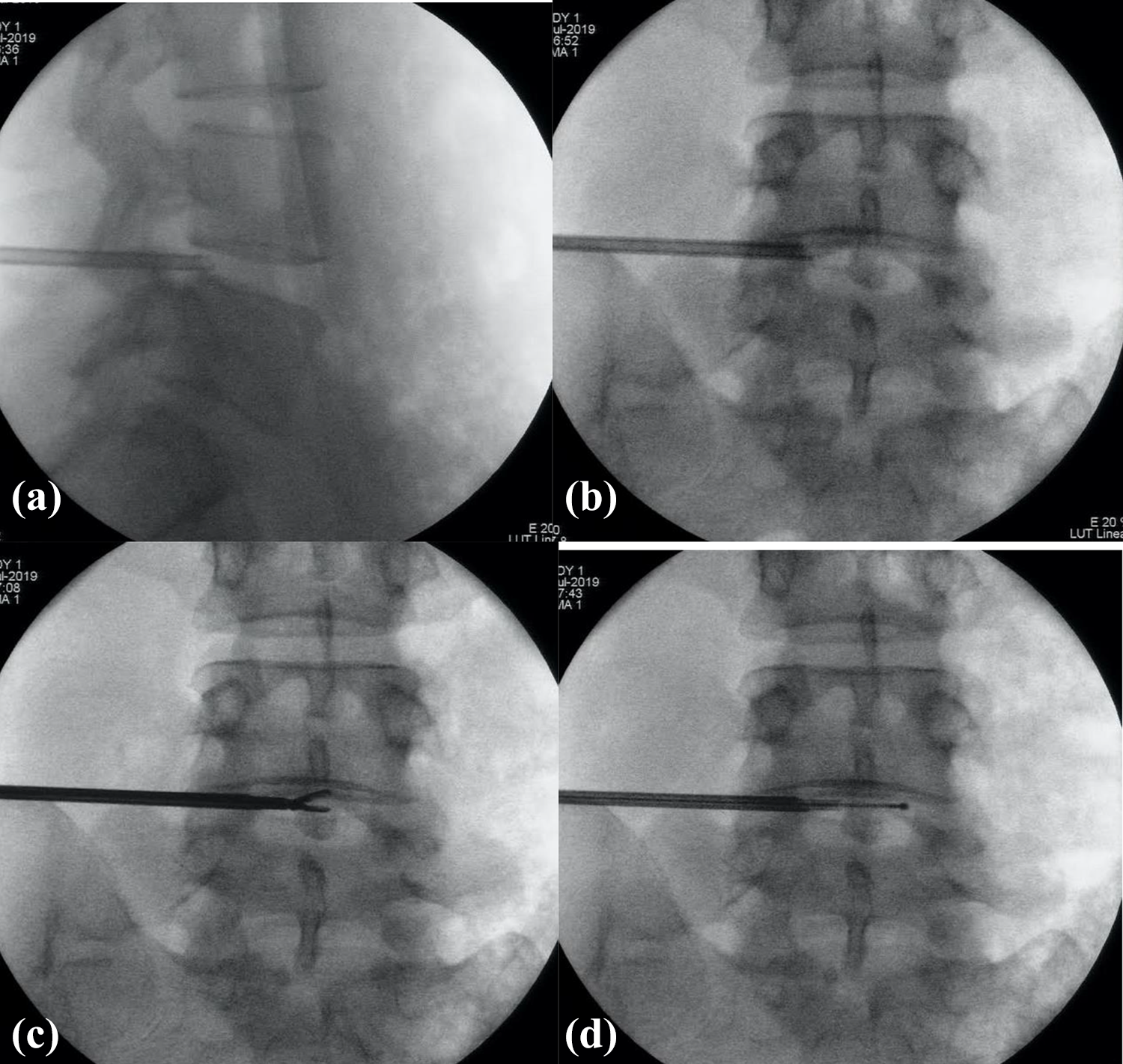
a, b (top two images). The spinal needle is confirmed to be at the correct position and level via fluoroscopy with AP and lateral views. c (bottom left). Manual diskectomy is performed with grasping forceps. d (bottom right). Annular modification by means of radiofrequency was performed with the flexible-tip bipolar probe at the region of the annulus.
In patients with multilevel discogenic back pain, the initial discography was targeted at the most severe level. If the patient presented with a positive discography, manual diskectomy and nuclear ablation as mentioned was performed to the targeted level. The procedure was repeated at the other levels, without further discography as the patient would have been sedated at the time of procedure.
After adequate irrigation, the working cannula was withdrawn, wound closed with a single nylon suture and a simple dressing was given to cover the wound.
The procedure was performed in a day surgery setting, aiming to discharge on the same day after a few hours of observation. Most patients received the procedure in our study as a day procedure. One patient required one additional day of hospital stay due to post-procedural pain. Another patient had the procedure performed during a psychiatric inpatient stay.
One patient had a concurrent percutaneous endoscopic lumbar diskectomy in the same session. Another one patient also had concurrent transforaminal epidural steroid injection along with selective nerve root block in the same session.
The above mentioned procedure when repeated at the L5/S1 level presents with different challenges as the high iliac crest may obstruct positions of inserted instruments— requiring modification of trajectory from the intended posterolateral approach. On occasion, the inserted working cannula was found to be bent in an attempt to accommodate for the high iliac crest position. However, as both the grasper and bipolar probe are flexible, the presence of a bent working cannula did not prevent the rest of the procedure.
One such patient with the procedure done at L5/S1 is as shown in Figures 3 –6.
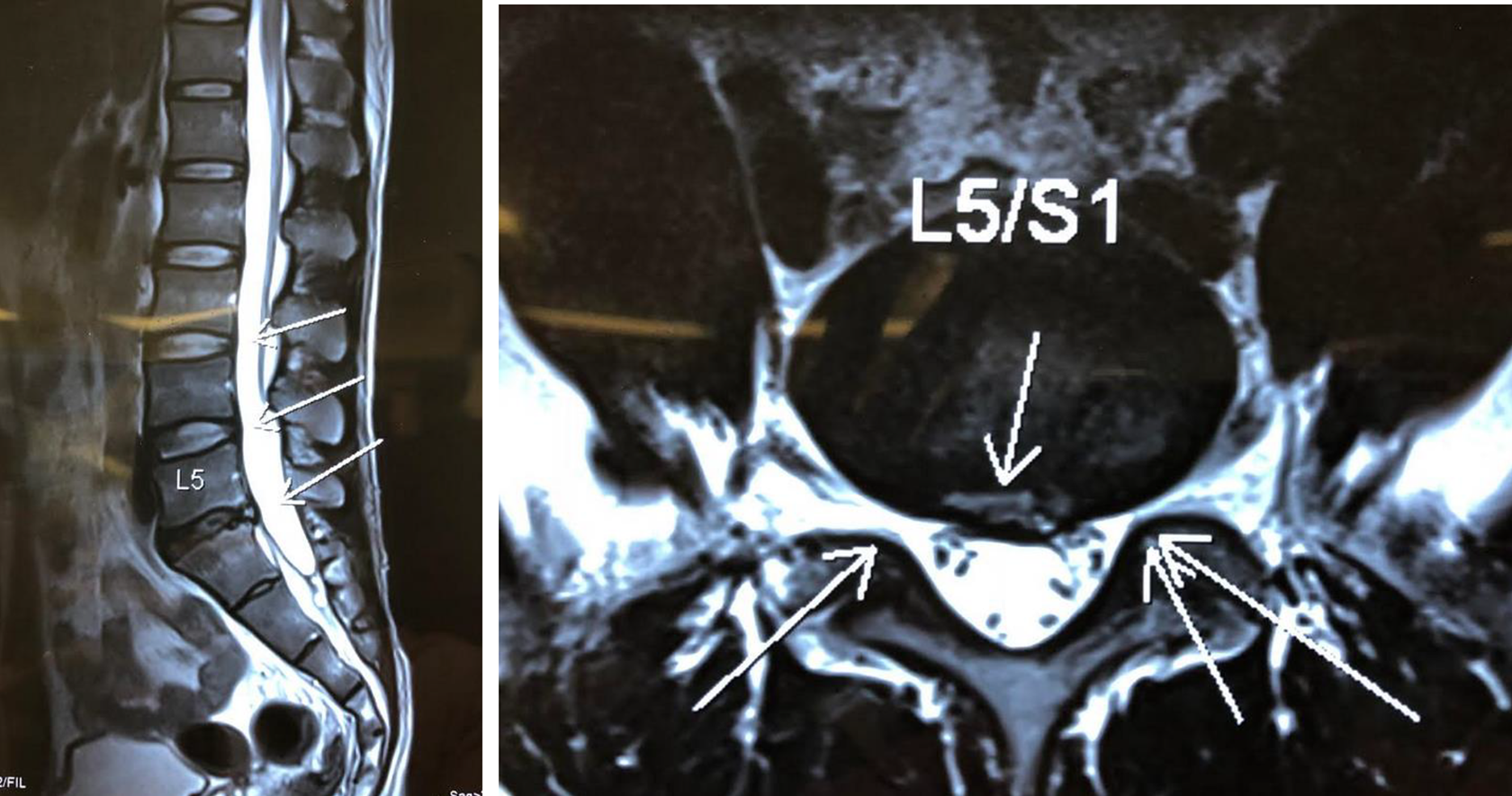
Magnetic resonance imaging of a patient with evidence of annulus tear noted at L5/S1 level.
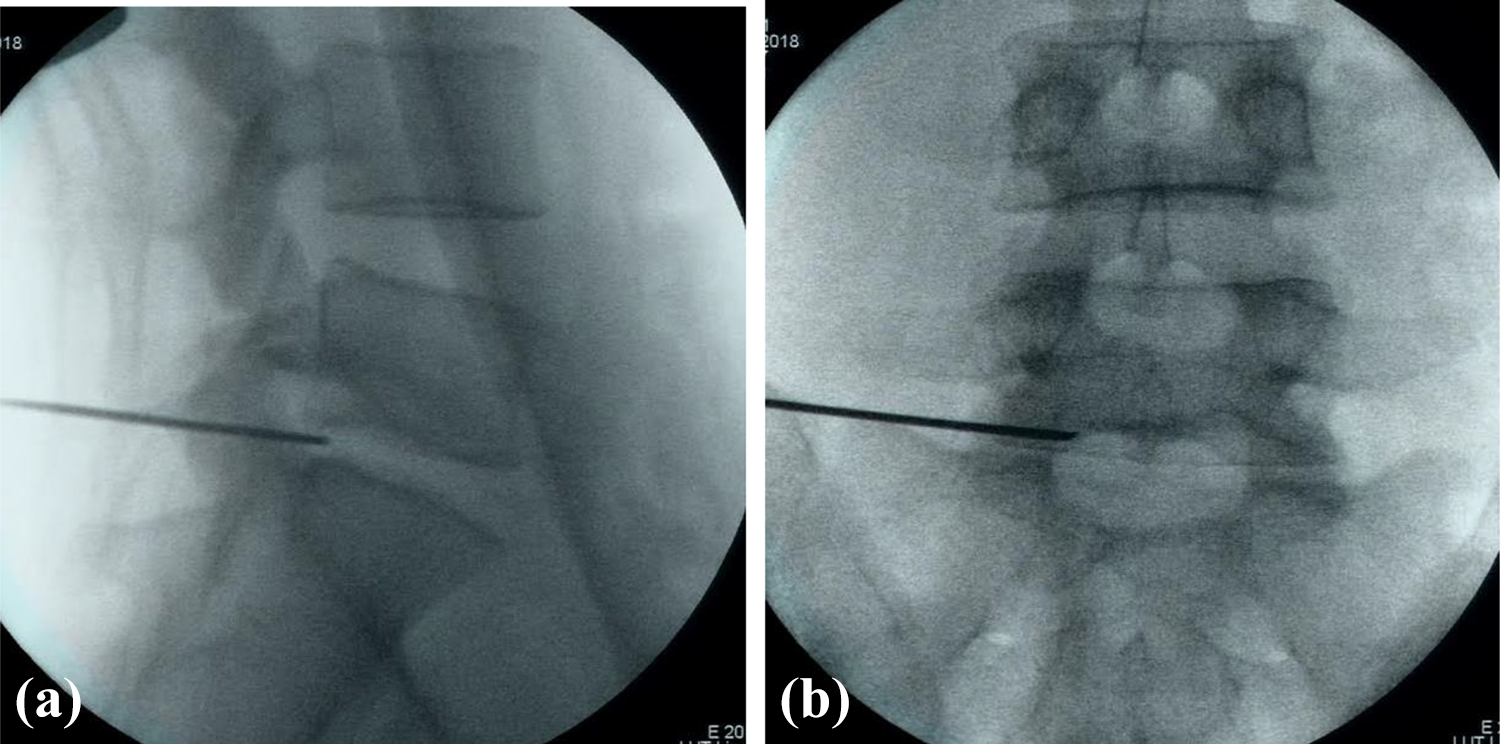
a, b (top two images). The spinal needle is inserted and confirmed to be in the correct position with fluoroscopy on both AP and lateral projections.
a (left). After the working cannula is inserted, the discogram is performed with an injection of a small amount of contrast. Patients with positive discography and concordant pain proceed to the rest of the procedure. b (right). Manual diskectomy is performed with a grasping forceps via the inserted working cannula.
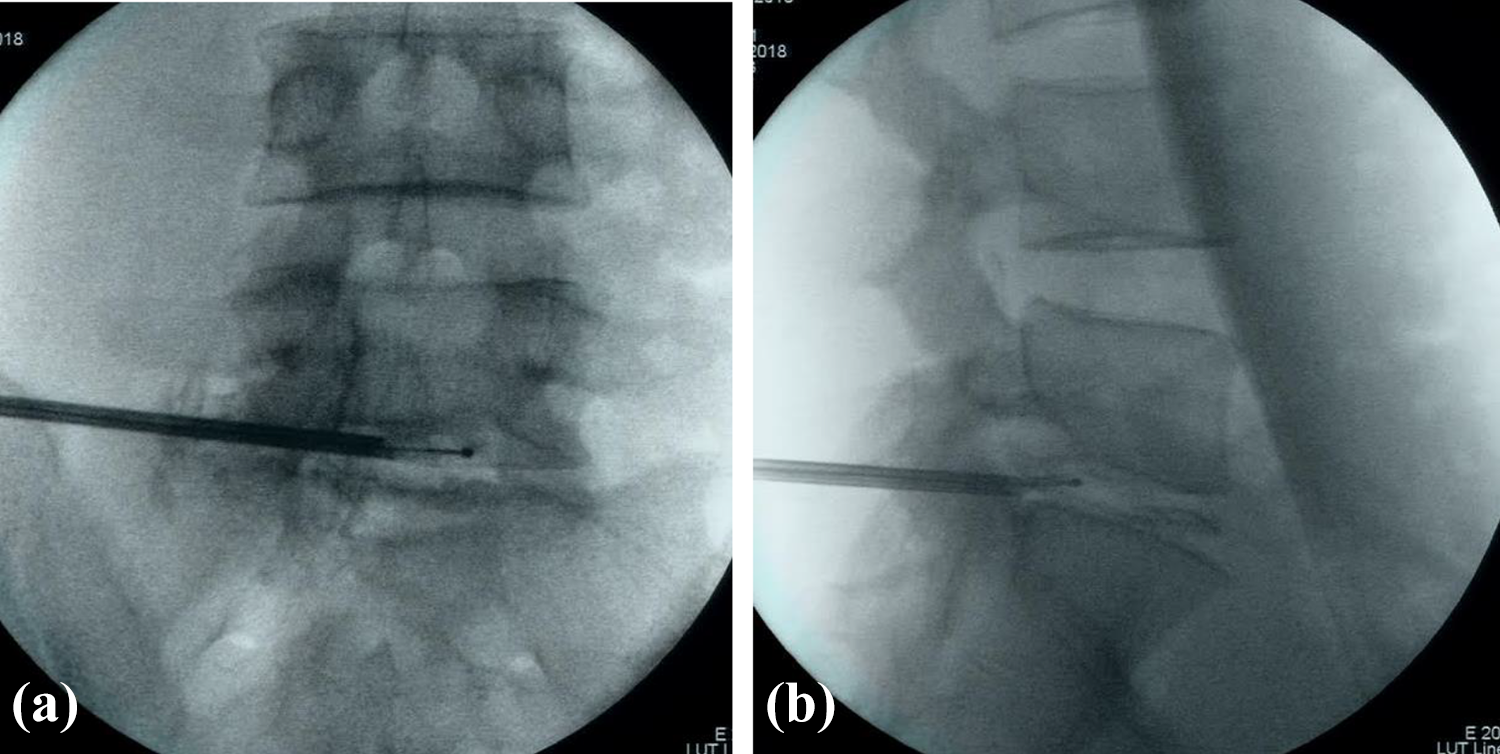
a and b. Radiofrequency ablation is performed with use of a flexible-tip bipolar tip probe.
Statistical analysis
The patients’ demographic and clinical data were analyzed descriptively. Functional outcomes scores such as Numeric Pain Rating Scale (NPRS), Roland Morris Disability Questionnaire (RMDQ) and Oswestry Disability Index (ODI) were compared with preoperative functional scores using the paired two-tailed t-test. Four patients eventually defaulted further functional scoring and follow-up, and the outcomes at 1 year represents the patients that have remained with the study. Rates of re-intervention and complications are descriptively summarized.
Patient characteristics
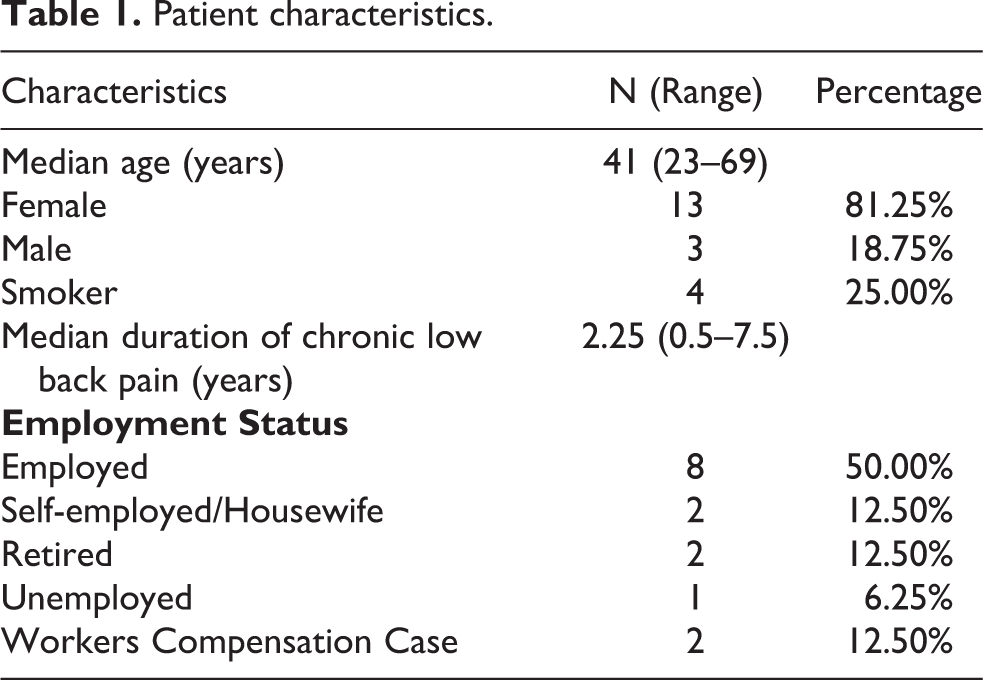
16 patients with a total of 24 levels were included in our study. The mean age was 44.6 (range 23–69) with 3 male and 13 female patients included in our study. Patient characteristics are as listed in Table 1. All patients fulfilled the inclusion criteria, namely the patient: has at least 6 months of degenerative discogenic back pain, has MRI-confirmed disc degeneration, has not responded to non-operative treatment (e.g. bed rest, physiotherapy, medications, spinal injections, and/or TENS) for a period of 6 months, has confirmed discogenic back pain via positive provocative test on discography, and at least 18 years of age and skeletally mature at the time of surgery who have undergone percutaneous nucleo-annuloplasty via disc-Fx procedure within our center from January 2017 to January 2019. Subjects who have had prior spinal fusion at the involved or adjacent spinal levels, morbidly obese as defined by body mass index >40, and/or with any presence of active malignancy or prior history of malignancy were excluded from the study.
Patient characteristics.
Results
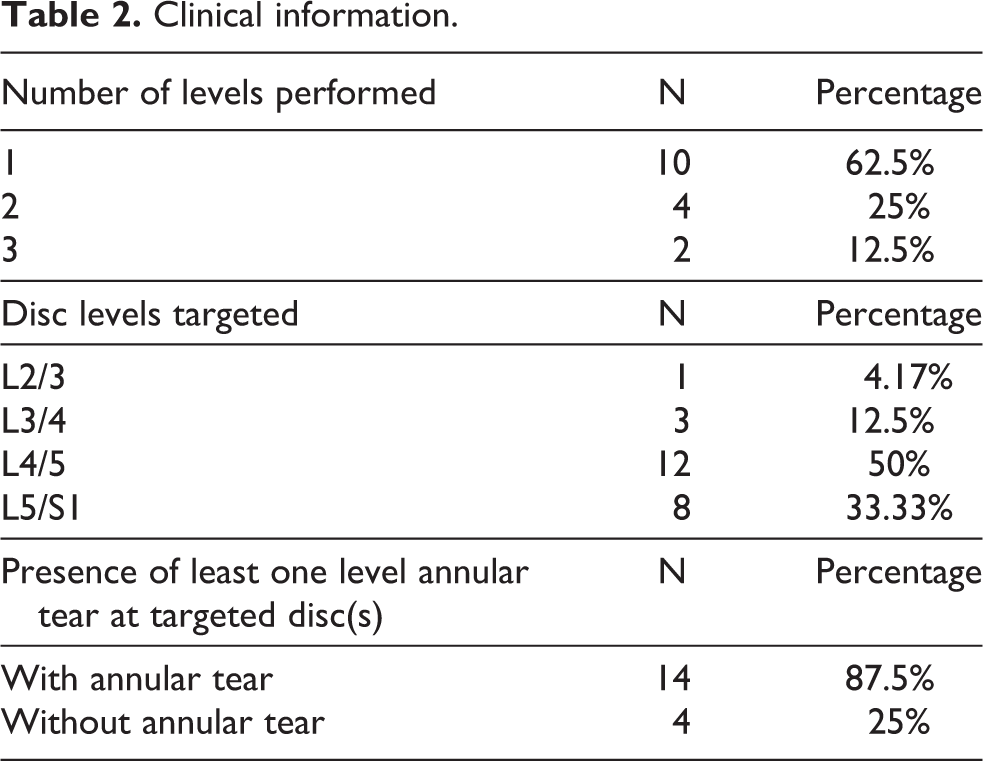
There were a total of 16 patients included in our study, with the radiofrequency ablation procedure performed in one level in 10 patients, two levels in 4 patients, and three levels in 2 patients. The minimum duration of follow-up for all patients was 6 months, with four patients subsequently lost to follow-up by 1 year. Patients’ Numeric Pain Rating Scale, Roland Morris Disability Questionnaire, and Oswestry Disability Index outcomes were charted at intervals of pre-procedural status, 3 months, 6 months, and 1-year post-procedure, and are shown in Table 2.
Clinical information.
The mean ODI values for the entire study population improved from 46.25 to 28.7, NPRS values improving from 6.25 to 4.47 and RMDQ value from 14.56 to 8.94 from preoperative status to 6-months post-procedure (see Table 3). This improvement in functional scores are all statistically significant. There is further improvement at 1-year post-procedure, although functional scores have excluded four patients who have defaulted subsequent follow-up.
Overall outcomes.
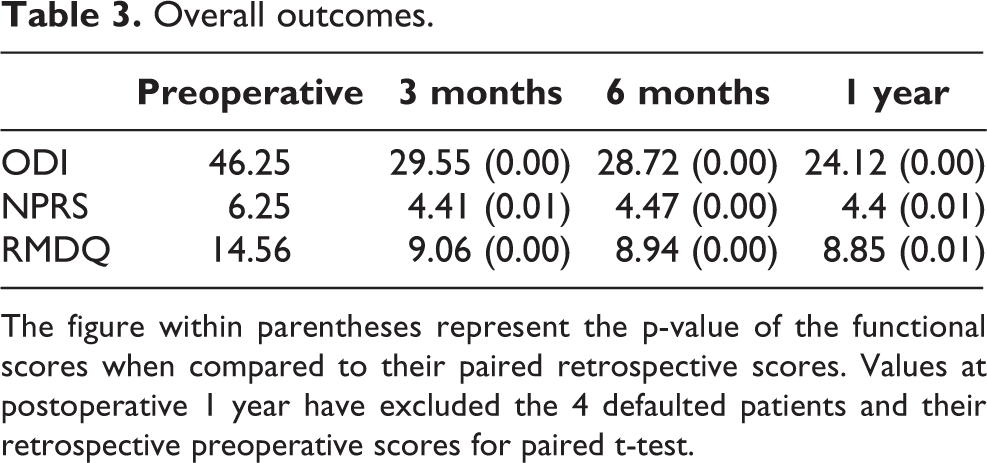
The figure within parentheses represent the p-value of the functional scores when compared to their paired retrospective scores. Values at postoperative 1 year have excluded the 4 defaulted patients and their retrospective preoperative scores for paired t-test.
Within the study population, 10 patients had single-level procedures, 4 patients had two-level procedures, and 2 patients had three-level procedures. Patients who have undergone either two-level or three-level were grouped in the multilevel subgroup. Both subgroups had two patients defaulted at 1-year follow-up.
Statistically significant improvement ODI scores was seen by an average of 18.15 in single-level intervention subgroup (p-value = 0.005), whereas the ODI improvement in multilevel group was 27.25 (p-value = 0.011). Statistically significant improvement in pain scores are also evident in the multilevel intergroup with an average improvement from 7.3 to 5.5 (p-value = 0.035) (see Table 4).
Outcomes in single level and multilevel involvement.
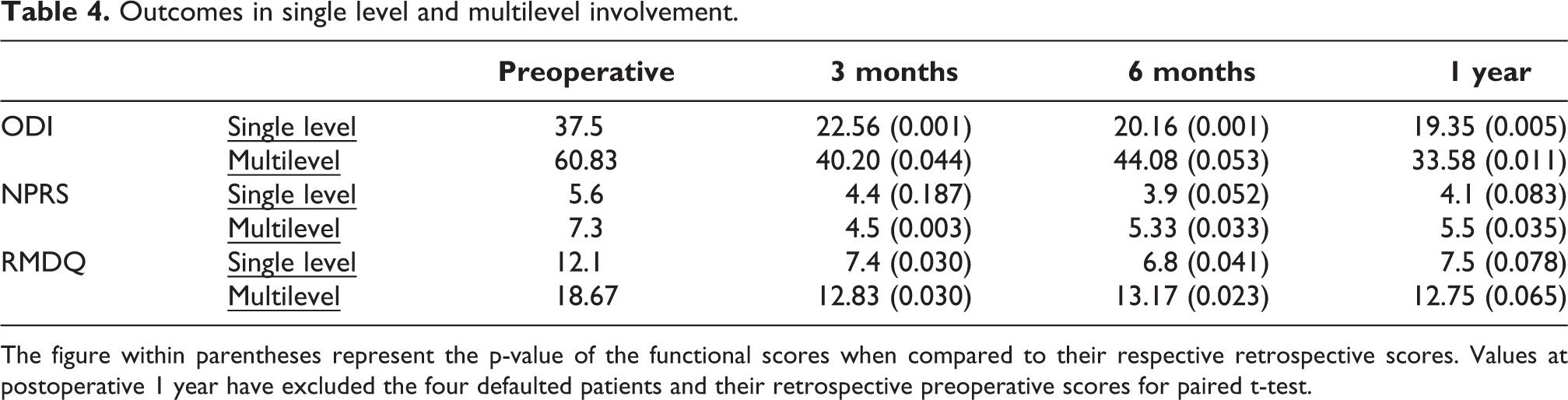
The figure within parentheses represent the p-value of the functional scores when compared to their respective retrospective scores. Values at postoperative 1 year have excluded the four defaulted patients and their retrospective preoperative scores for paired t-test.
Four patients within the study population had no annular tears present in preoperative MRI, whereas 14 patients had annular tears in at least one level in preoperative MRI. One patient from the no annular tear subgroup and three patients from the annular tear subgroup defaulted by 1-year follow-up. Statistically significant improvement in ODI, NPRS and RMDQ scores can be seen in the annular tear subgroup, compared to the subgroup with the absence of annular tears (see Table 5).
Outcomes in presence or absence of annulus tears.
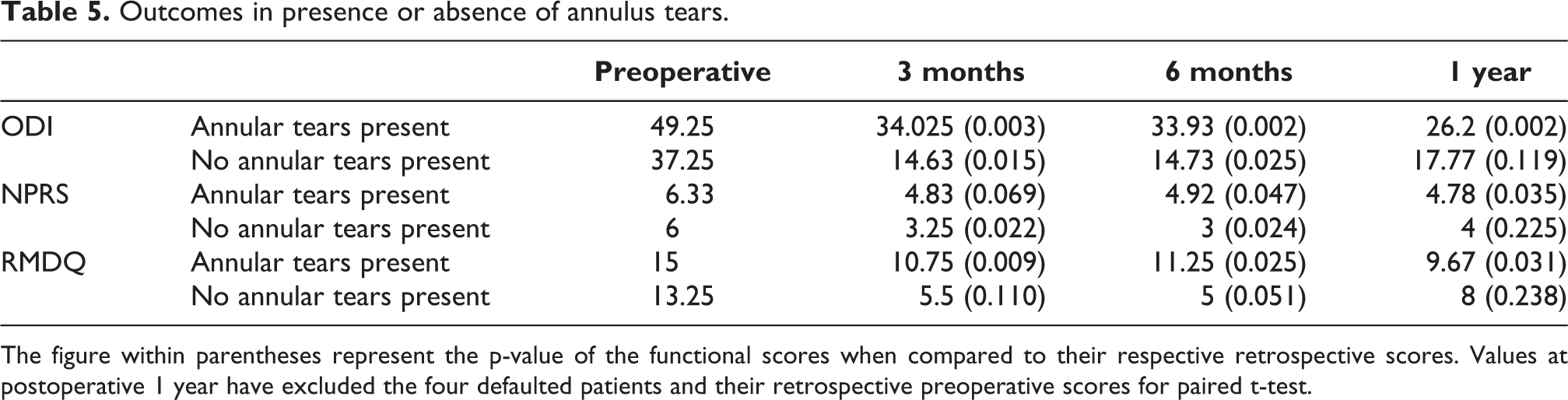
The figure within parentheses represent the p-value of the functional scores when compared to their respective retrospective scores. Values at postoperative 1 year have excluded the four defaulted patients and their retrospective preoperative scores for paired t-test.
Re-intervention was seen in one patient, who proceeded to a spinal decompression procedure at another center and defaulted subsequent follow-up. Three additional patients were lost to subsequent follow-up and assessments.
There were no reported procedural related complications in the study population.
Discussion
Lumbar back pain is a global debilitating condition, with more than at least 80% of the world’s population expected to be burdened by back pain at least once in their lifetime. 10 It is also one of the top reasons for medical consultation. 11 Among patients with chronic low back pain, a positive discography with disc degeneration on imaging has been shown to be present in up to 37%. 3
Discogenic back pain was generally treated by means of conservative treatment—via activities modification, physiotherapy, pharmacotherapy with analgesics, etc. Use of radiofrequency ablation itself as a procedure with potential relief of back pain was first used by Shealy in 1975—at the time using the high frequency energy to coagulate the articular nerves which supply the facet joints. 12
However, current theories postulate that neurogenesis at the posterior aspect of the intervertebral disc—along with any potential compressive effect on surrounding nerve roots, is the potential cause of discogenic back pain. 13 Following this theory, procedures and techniques of using thermal or radiofrequency ablation to target aforementioned nerve fibers have arisen and developed as a potential method of pain relief. Radiofrequency waves and thermal energy could be used to shrink the intradiscal collagen fibers and thereby decrease intradiscal pressure, subsequently decreasing pain and symptoms arising from the triggered nerves within the posterior edge of the disc.
Saal and Saal 14 used intradiscal electrothermal therapy in 1999, using a heating coil at the annular region as an attempt of thermocoagulation of pain nociceptors and fibers. Although widely used, larger studies seem to suggest that there is inconclusive evidence of benefit from the procedure. 15 In recent years, there have been many different types of minimally invasive procedures and interventions aimed to target discogenic back pain. Limitations also included limited reach to the annular region.
The Disc-Fx procedure used in our study is a percutaneous minimally invasive procedure which utilizes radiofrequency and heat ablation to allow for shrinkage of intradiscal pressure. The insertion of the working cannula allows for the ability of for manual discectomy and debulking of the disc via instruments such as the grasping forceps. An advantage with the Disc-Fx procedure is the bipolar aspect of its heating probe. The bipolar probe allows for a focused area of thermal energy to be concentrated to the targeted diseased site—which is especially important given its close proximity to neural elements. Its flexible-tip also allows for a more extended reach to allow the surgeon to target the posterior annulus.
Our study results are comparable with recent studies regarding use of radiofrequency ablation including Park et al involving 43 patients with lumbar disc herniation, 16 Hellinger’s prospective study of 58 patients 17 and Kumar et al.’s 4 prospective analysis of 51 patients with Disc-Fx interventions which suggest that Disc-Fx may be helpful in providing improvement or favorable outcomes in discogenic back pain.
Earlier aforementioned studies also suggest that the disc-Fx procedure can be effective in the presence or absence of annular tears. Our study suggests that patients with annular tears present with statistically significant improvement post-procedure as opposed to those without annular tears. However, it is important to note the small population size of patients without annular tears, likely limiting the statistical significance of the results in the subgroup.
In Kumar et al.’s 4 study, patients who had negative discography with single-level disease still underwent the radiofrequency ablation despite discordant results as the authors believe that preoperative investigations have ruled out other potential anatomic causes of pain. Our study has included only patients with positive discography results, which may also affect the efficacy of pain relief in the studied population. Patients that did not present with positive discography results did not proceed with Disc-Fx procedure in our institution. The disc-Fx radiofrequency ablation and annular modification was performed on multiple levels when accompanied by concordant provocative discogram results. Previous studies mostly reviewed single-level interventions—although functional outcomes from our study show statistically significant improvement even in patients with multilevel intervention.
Limitations
Our study is limited by the small sample size of 16 patients. Although the results show that there is a statistically significant improvement in functional outcomes, the outcomes at 1 year may not be representative in view of the four defaulted patients. As described earlier in the study, one of the patients proceeded with spinal decompression surgery at another center. Three other patients defaulted—whether it is due to relieved symptoms or intractable symptoms cannot be determined. Two patients had concurrent spinal procedures done in same session which targeted another site in addition to the targeted level of discogenic back pain, which may also affect our studied sample being representative.
Furthermore, the study compares subjects pre- and post-procedure. Potential studies with control groups would be desirable to further delineate the therapeutic efficacy of this radiofrequency ablation.
Lastly, the study mainly focuses on the reduction of pain scores or functional assessments as a result of the procedure. Whether or not subsequent spinal fusion surgeries or other spinal interventions are needed in long-term are yet to be determined.
Conclusion
The procedure of percutaneous nucleo-annuloplasty shows to be a relatively safe procedure that can be considered in patients with discogenic back pain. No major complications were reported in the retrospective study of 16 patients in our department. Early outcomes seem to suggest that some patients are able to benefit from the procedure, although a larger study would be desirable to draw further conclusions regarding its efficacy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.