
Abstract
Background
The Insall-Burstein posterior-stabilized knee design was first developed in 1978 by adding a central cam mechanism to the articular surface geometry of the total condylar prosthesis to correct its problems being not “rolling back”. Since then, the use of posterior-stabilized (PS) implants in total knee arthroplasty (TKA) is becoming increasingly popular. However, one of the main disadvantages of PS designs is related to the amount of bone removed during femoral box osteotomy to create the housing of the PS mechanism, the clinical value of removing more or less bone during primary TKA remains to be fully established. The objective of this study was to compare the incidence of early postoperative periprosthetic fractures in the cruciate retaining (CR) and posterior stabilized (PS) knee prosthesis.
Methods
An institutional high volume arthroplasty unit database was reviewed to identify all patients who sustained a postoperative periprosthetic fracture following primary TKA between January 2014 and May 2018. A retrospective chart review was performed to collect clinical, radiographic, and operative report data. A total of 352 patients with 600 primary TKAs were identified. (300 cases of cruciate retaining TKAs from 178 patients and 300 cases of posterior stabilized TKAs from 174 patients) were retrospectively reviewed.
Results
Eleven patients (1.83%) sustained periprosthetic fractures in the postoperative setting following primary TKA. All of the fractures were located on the femur and were treated surgically. Only one knee (one patient) from the CR group sustained a periprosthetic fracture, while 10 knees (from 10 patients) from the PS group sustained a fracture. The relative risk of sustaining a fracture in the CR group was 0.10 times relative to the PS group (RR = 0.10, 95% CI 0.0129 – 0.776).
Conclusion
Posterior stabilized total knee arthroplasties (TKAs) significantly increase the risk of periprosthetic fractures in obese Asian patients compared to cruciate retaining TKAs.
Introduction
Total knee arthroplasty (TKA) is one of the common orthopedic procedures performed worldwide for the treatment of osteoarthritis. The different designs of the total knee arthroplasties include the unconstrained posterior cruciate retaining (CR), the unconstrained posterior cruciate substituting (posterior stabilized), the constrained nonhinged, and the constrained hinged. The most commonly used TKAs consist of the posterior cruciate retaining and the posterior cruciate substituting designs.
The posterior stabilized (PS) knee design was first developed in 1978 to replace the function of the posterior cruciate ligament (PCL) and to allow femoral rollback during flexion, thus preventing flexion instability and increasing the knee flexion. This was done by adding a central cam mechanism to the femoral implant. Nevertheless, one of the main disadvantages of PS TKA design is the greater amount of femoral bone removed needed to house the PS mechanism. Although bone preserving techniques are generally preferred by orthopedic surgeons, the clinical impact of the additional bone resection of the PS design is still under debate. Theoretically, this may affect the knee kinematics, increase the risk of periprosthetic fractures, decrease the bone stock available for future revision surgeries 1 . Despite these disadvantages, posterior stabilized total knee arthroplasties are the most commonly used worldwide.
The distal femur is the most frequently involved in the case of periprosthetic knee fractures, with an incidence of up to 2.5% of all total knee replacements, while the tibia is only fractured in up to 1.7% of the total knee replacements 2 . In the current literature, there is little data regarding the incidence of periprosthetic fracture in posterior stabilized and in cruciate retaining total knee replacements.
We hypothesize that resection of a larger amount of bone from the intercondylar notch might have an influence on the overall survivorship of the implant even in the short term. The objective of this study was to compare the incidence of early postoperative periprosthetic fractures in the cruciate retaining (CR) and posterior stabilized (PS) knee prosthesis.
Methods
We retrospectively reviewed an institutional database in a high-volume hospital for 300 primary PS TKAs and 300 primary CR TKAs between January 2014 and May 2018. The presence of postoperative periprosthetic fracture, patient demographics, clinical data, radiographic measurements, bone density scan (DEXA scan), and surgical reports was recorded. Osteopenia and osteoporosis were diagnosed using DEXA scans according to the World Health Organization criteria 3 .
We excluded patients with systemic inflammatory disease, body mass index (BMI) less than 30, preoperative varus-valgus deformity more than 15 degrees, and flexion deformity more than 10 degrees. Following this query, a total of 352 patients with 600 primary TKAs were identified. A total of 300 cases of cruciate retaining TKAs from 178 patients and 300 cases of posterior stabilized TKAs from 174 patients were retrospectively reviewed (Table 1). All of the TKA procedures were performed by a single high-volume arthroplasty surgeon using modified a subvastus approach and using Zimmer Persona System. This study was approved by the Institutional Review Board of our Hospital, (IRB no. E10023).
Number of CR versus PS implants.
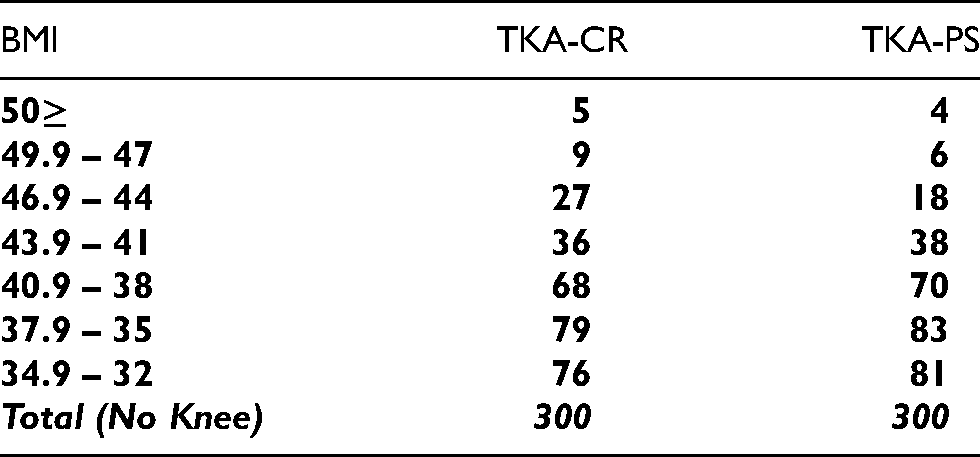
Statistical analyses were performed using STATA software version 15.1. Pearson's Chi-Square test of independence was performed to test the association between the implant group and whether a fracture was sustained. Due to the small sample size of the outcome measure, we also performed inferences using the exact distributions as Chi-Square is typically used for large sample approximations. Fisher's Exact Test was utilized to test the association between fractures and implant group. All tests were performed using a 0.05 type I error, a two-sided alternative hypothesis, and a power of 0.80 for detecting a difference between the study groups of knees. Patient demographics were balanced between both CR and PS groups, and there was no significant difference between BMI categories (p = 0.33 by Chi-Square testing) (Table 2).
BMI in CR versus PS patients’ group.
Results
Eleven patients (1.83%) sustained periprosthetic fractures in the postoperative setting following primary TKA (Table 3). All of the fractures were located on the femur and were treated surgically. Only one cruciate retaining TKA (9%) sustained a periprosthetic fracture, while ten posterior stabilized TKAs in 10 different patients (91%) sustained a fracture.
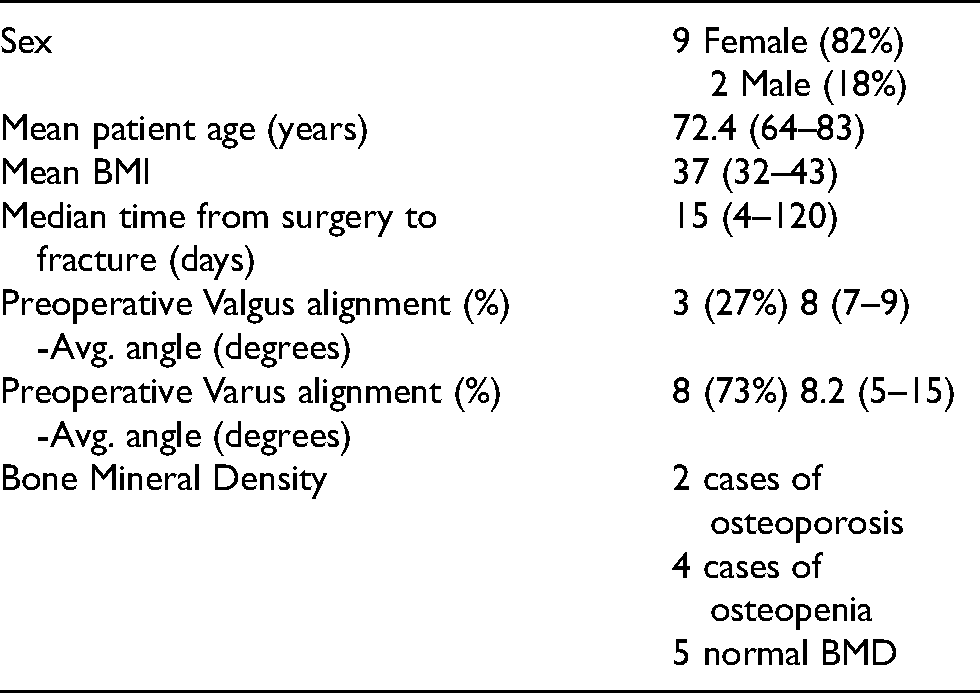
Characteristics of the 11 patients with the periprosthetic fractures.
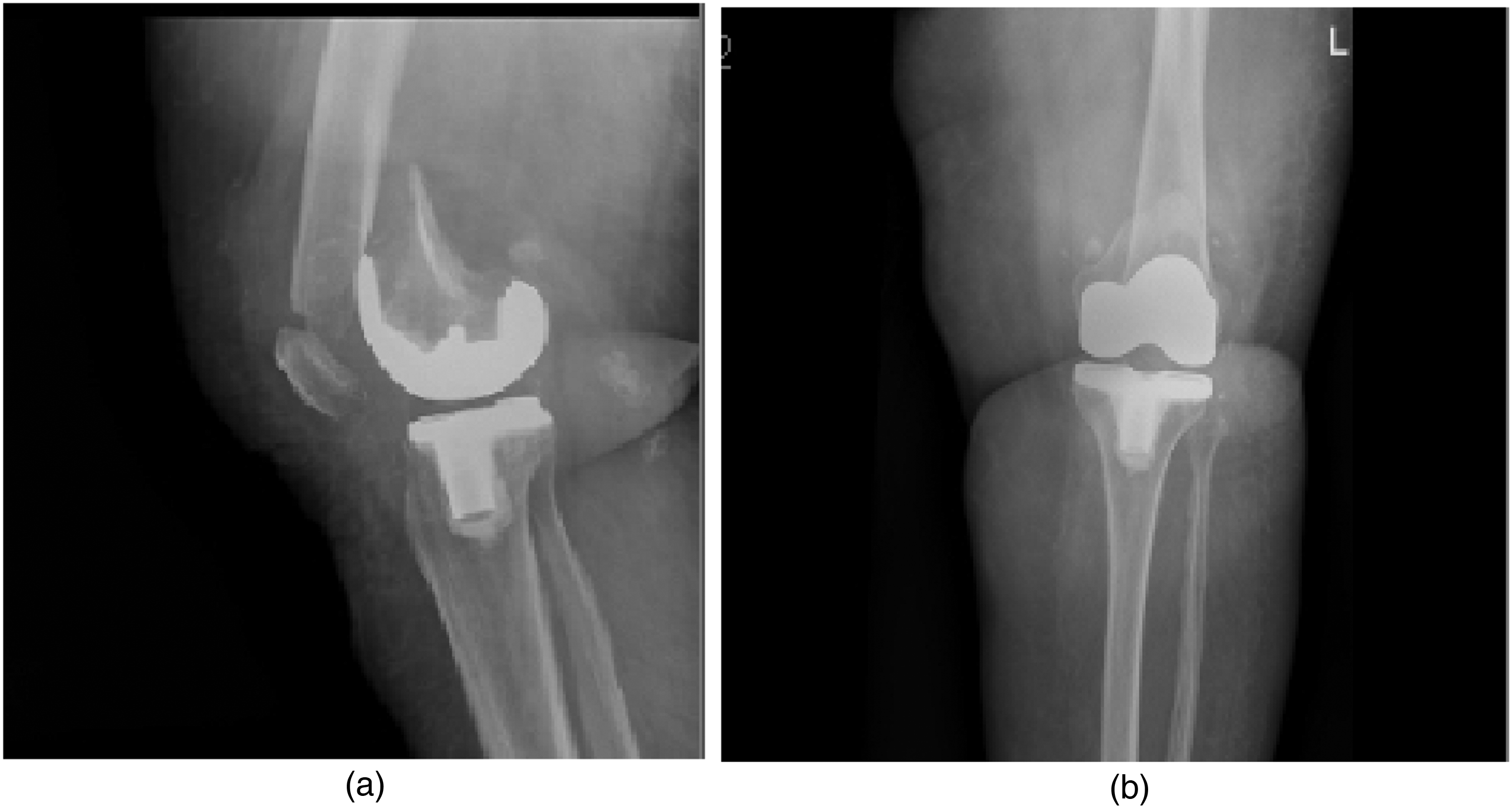
Four patients developed insufficiency femoral condylar fractures (Figure 1) while 7 patients developed supracondylar femoral periprosthetic fractures (Figure 2).

(a and b) Insufficiency femoral condylar fracture (fracture line can be hardly seen).
(a and b) Supracondylar femoral fracture.
The insufficiency fracture occurred in the early postoperative period, with an average of 22.2 [12–34] days from the surgery. No history of trauma was reported in none of the cases. All of the cases had preoperative varus malalignment and sustained a fracture of the unloaded lateral femoral condyle; however, the fracture line was seen extending to the medial femoral condyle as well in two of the cases. Three of them had a PS knee implant, while only one had a CR knee implant. All of them underwent early intervention, two were managed with hinged knee prosthesis, one with stemmed femoral component (Figure 3) and the fourth required a distal femoral replacement secondary to significant femoral bone loss. Such pattern of fracture has been previously described in literature4,5.

(a and b) Post-operative X-Ray.
The remaining seven patients developed standard supracondylar femoral periprosthetic fractures after an evident history of trauma post knee replacement. PS knee implant was the case in all of them, and they all were managed by a distal femoral locking plate (Figure 4).

(a and b) Post-operative X-Ray.
The relative risk of sustaining a fracture in the CR group was 0.10 times relative to the PS group (RR = 0.10, 95% CI 0.0129 – 0.776). The Pearson's Chi-Square test of independence showed a statistically significant association between the implant group and whether a fracture was sustained among the unique knees in the study (χ2 7.50, p-value 0.006). An additional sensitivity test was performed to obtain the exact inference for small samples of knees. The Fisher's Exact Test of independence showed a statistically significant association between the implant placed and sustaining a perioperative fracture (p-value 0.011) (Figure 5).
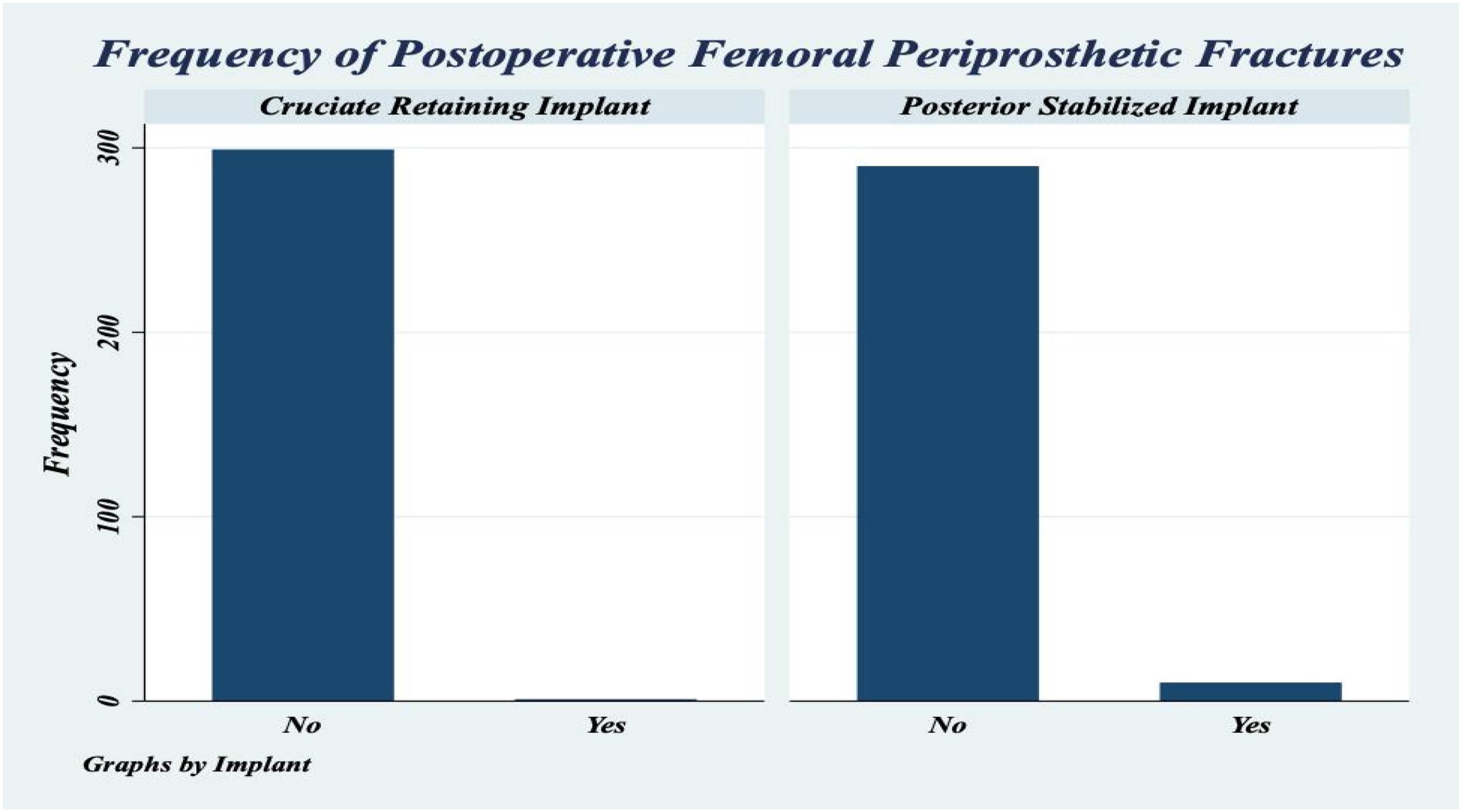
Frequency of postoperative femoral periprosthetic fractures in CR and PS implants.
Discussion
With a reported incidence between 0.3 and 5.5%, and mainly occurring in the supracondylar region of the femur, many risk factors for periprosthetic fractures have been described in literature such as osteoporosis, and rheumatoid arthritis6,7. Obesity, defined as a body mass index over 30 kg/m², has also been related to many complications such as an increased rate of infection 8 . However, there is little evidence in the literature about the relationship between obesity and periprosthetic fractures around the knee 9 .
Furthermore, several studies showed that Asian knees are smaller than Caucasian knees, having lower mediolateral (ML) and anteroposterior (AP) dimensions of the distal femur compared to those in Western populations with a decrease in the aspect ratio (ML/AP %) and an increase in the anteroposterior distal femoral dimensions10,11,12.
For the reasons mentioned above, we have only included in our study obese Asian patients, due to their increased risk of sustaining periprosthetic fractures.
Despite the overall high success rates of TKA, there is still controversy regarding to preserve or to sacrifice the PCL 13 . The original posterior stabilized cruciate substituting total knee arthroplasty design was introduced in 1978 14 . Several studies compared the CR and PS TKAs with most of them showing no difference in clinical scores, ROM, midterm survival rate, and functional outcomes15-18. Assuming the functional outcomes are similar, implants that minimize bone removal are generally advantageous. One of the goals of knee replacement surgery is to preserve bone stock as long as there are no other drawbacks.
In this study, we are not aiming at comparing which design is better than the other in terms of function or survival, rather than simply identifying whether the two most common types of implants, cruciate retaining (CR) and posterior stabilized (PS), can influence the risk of postoperative periprosthetic fracture in obese Asian patients. We hypothesize that resection of a larger amount of bone from the intercondylar notch might have an influence on the overall survivorship of the implant even in the short term.
The incidence of intraoperative femoral fractures in PS knees is documented in the literature, but to our knowledge, there is no data regarding the rate of postoperative periprosthetic fractures in PS knees 19 . We believe that the incidence of postoperative periprosthetic fractures in PS knees is underestimated in the literature.
Delasotta et al. reported an incidence of intraoperative periprosthetic distal femoral fracture of 0.32%, 0%, and 3.13% in patients with a posterior stabilized, cruciate-retaining, or semi-constrained implant, respectively 20 . Lombardi et al., found that the incidence of intraoperative condylar fractures in PS TKAs was 4.5% 21 . Alden et al. reported an incidence of 0.39% for intraoperative fractures during primary TKA in a large series of patients, mostly in women (80.6%) and in the femur (73.1%) 19 .
In this study, our focus was on the occurrence of early postoperative femoral periprosthetic fractures. All of the 11 patients who sustained such kind of fractures in this study enjoyed a pain-free period for a minimum of 4 days and up to 3 months, during which weight-bearing and range of motion exercises were allowed without any reported intraoperative complication at the time of surgery.
To our knowledge, this is the first study to assess the influence of TKA type on the risk of postoperative femoral periprosthetic fractures. The higher incidence of periprosthetic fractures in the PS group compared to the CR group could be due to the larger bone resection (25%-30%) in the intercondylar notch to accommodate the post included in the posterior stabilized design.
Furthermore, the increase in the constraint level in PS knees rather than CR knees is considered, theoretically, to be an additional stress factor on the bone and the bone-implant interface. These effects will be exaggerated in patients with narrow femurs which is the case in Asians, especially in presence of any additional risk factor such as osteoporosis and obesity.
Several studies compared the differences in the amount of bone resected during various PS implant designs. Bozkurt et al. compared ten implants from five different total knee arthroplasty implant manufacturers, using a total of 50 sawbones models. They found a significant difference between implant designs in terms of preserving bone stock, especially in the femoral notch cut 22 .
Wragg et al. compared the amount of bone removal between PS and CR designs on saw bone models, showing that PS implants require much more bone removal, up to 25% which might be hazardous intraoperatively, and affect the longevity of the prothesis 23 . Hass et al. found a similar conclusion when he compared in Vivo bone loss between five different types of PS implants 1 . Pugh et al. conducted a cadaver study that showed that newer posterior stabilized designs may accommodate high flexion with less bone resection 24 .
Huten et al. demonstrated that previous bone excisions are the most important reasons behind bone loss in revision total knee arthroplasty 25 . Graceffa et al. found that the Persona cutting jig always removed much less bone than did Vanguard and Sigma PS 26 . However, most of these studies were either on sawbones, in vitro or cadaveric studies, also they didn’t establish a direct clinical relevance of removing more or less bone at primary TKA, but only suggesting that if a PS design is indicated, it is preferable to select a model which possibly resects less distal femoral bone without comparing the actual clinical hazards nor directly correlating it to the type of implant whether CR or PS knee.
Our study represents a direct clinical correlation to the design difference between PS and CR knees and a real-life implication to the consequences of larger bone resection of the PS group compared to the CR group. We were able to retrospectively review 11 cases of postoperative periprosthetic fractures, only one of them occurred postoperatively in the CR group patients. This patient was a 70-year-old female with a BMI of 36.2 and preoperative osteoporosis, with an insufficiency pattern of fracture 34 days after surgery without any trauma. The size of the femoral implant, which was a Zimmer Persona size 7 standard femur, a relatively bigger size compared to the other patients, reflecting more the bone pathology rather than implant design as a more direct predisposing factor for this postoperative femoral periprosthetic fracture.
The remaining three patients with insufficiency fracture pattern were all with PS implants in narrow small femurs (two of them size 5 persona femur standard and one of the sizes 6 femur persona narrow)
On the contrary, all the patients with supracondylar femoral fractures were with PS implants, and small femoral implant sizes (4 knees size 5 femur, 2 knees size 4 femur, 1 knee size 6 femur narrow). The metaphyseal location of the fracture site reflects the abnormal loading and increased bone stresses in an unintended manner with increased bone resection in the intercondylar notch especially the anterior dense cortical bone. The increase in the constraint level in PS knees rather than CR knees is an additional stress factor on the bone and the bone-implant interface. All of these changes are critical in presence of any other risk factors which is already the case in Asian patients with narrow femurs (Table 4).
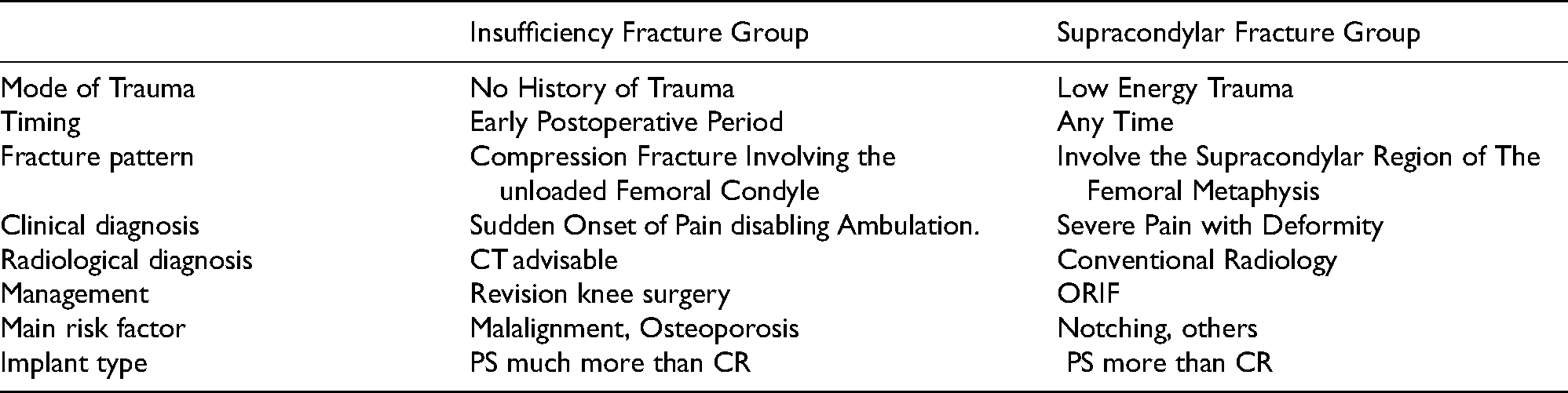
Comparison between the two patterns of periprosthetic fractures.
The Zimmer Persona design was based on the experience of the Insall-Burstein PS knee (Zimmer), which had a post-and-cam articulation at 60° of knee flexion, and the Nex-Gen Legacy (Zimmer), which showed initial post-cam engagement at 100° of knee flexion 27 . Both of these implants showed satisfactory clinical results 28 . Based on manufacturer estimation, a Persona CR femur implant preserves 32% more bone than a classic PS femur design, which requires a box cutout (Figure 6).
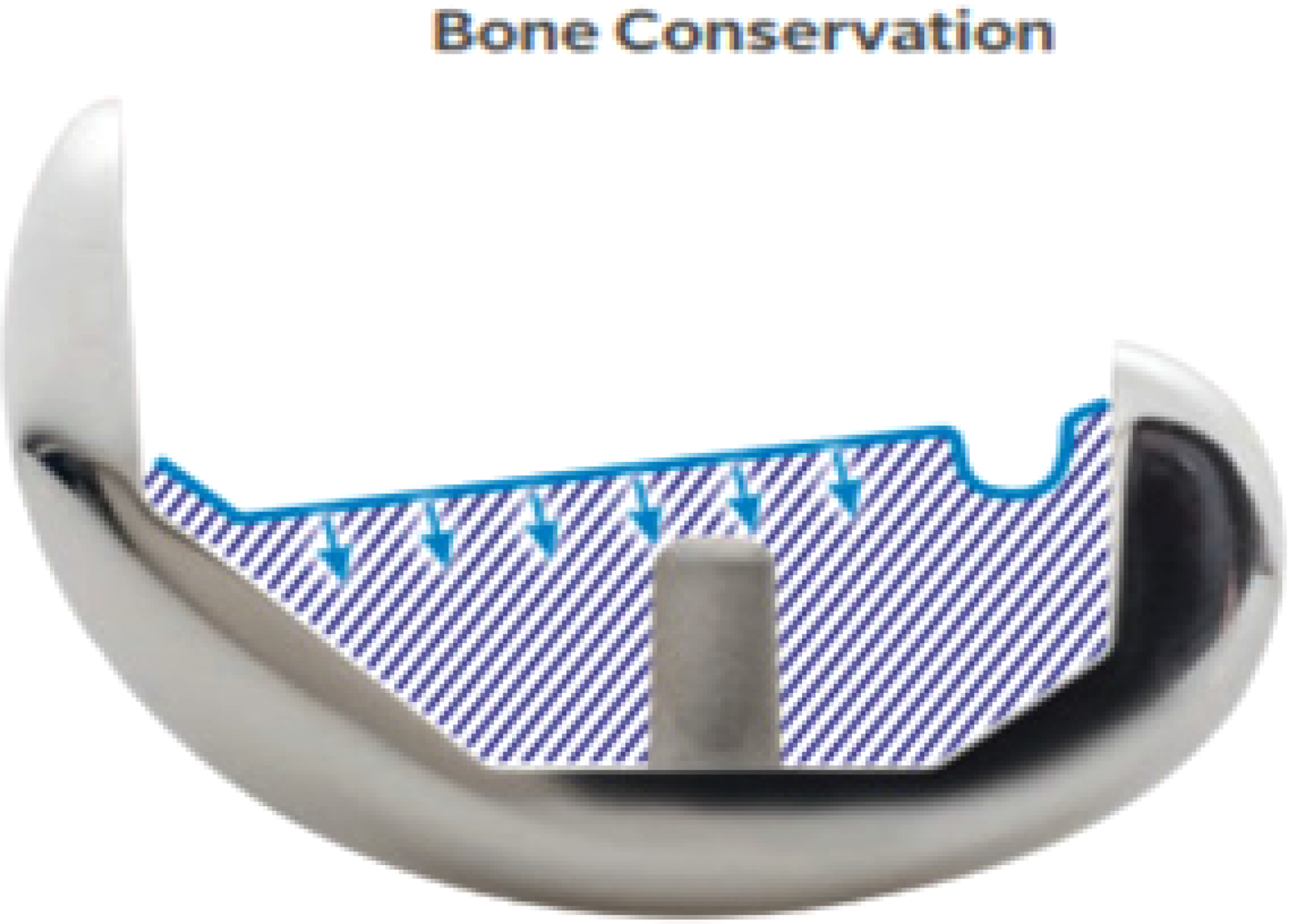
Persona CR femur implant preserves 32% more bone than a classic PS femur design. (Zimmer Biomet package insert)
Our study has some limitations such as its retrospective nature, small sample size, and the difference in the confounding factors between the CR and PS groups mainly due to the indications for each group. In addition, the overall incidence of postoperative periprosthetic fracture with each implant type requires long-term follow-up of patients who have undergone TKA. However, it is still one of the rare studies enlightening these underestimated complications of posterior stabilized total knee arthroplasties in terms of postoperative periprosthetic fractures if compared with cruciate retaining knees.
Conclusion
Posterior stabilized total knee arthroplasties (TKAs) significantly increase the risk of periprosthetic fractures in obese Asian patients compared to cruciate retaining TKAs. In the absence of specific indications for a posterior stabilized knee, consideration should be given to a cruciate retaining prosthesis.
Footnotes
Authors’ contributions
All authors contributed equally to the manuscript. ME and ST generated the concept, literature search, manuscript preparation, and reviewing; FH, AD and AO contributed by defining the intellectual content, literature search, manuscript preparation and editing; ME, YA and ST contributed by manuscript editing and reviewing. All authors read and approved the final manuscript.
Availability of data and materials
The datasets obtained and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Informed consent was obtained from the patients following the guidelines set forth by our institution and by the Declaration of Helsinki and Good Clinical Practice. This study was approved by the institutional review board of our institution.
Consent for publication
Each author certifies that he has participated sufficiently in the preparation of this article and has read and agrees with the contents of the manuscript.
Each author further represents that the article is original, that it is not under consideration by another journal, and that it has not been previously published.
This assignment is to take effect only if the work is published in the journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.