
Abstract
A 76 year old female, with a background history of eczema and iatrogenic Cushing syndrome, received a right total knee replacement for her knee osteoarthritis. In the early post-operative period, a small amount of discharge was noted from the surgical wound. The wound swab culture of the discharge yielded candida species. It was regarded as contamination initially. Half year later, she presented with a subcutaneous abscess around the right knee. Aspiration and culture confirmed infection of Candida parapsilosis. The patient was treated conservatively with fluconazole because she had initially refused operative treatment. The infection progressed to abscess formation afterward. A two-stage revision arthroplasty with cement spacer was performed subsequently. In addition, we have reviewed the literature regarding fungal periprosthetic joint infection.
Keywords
Introduction
Periprosthetic joint infection (PJI) is a severe complication for total joint replacement with the incidence rate of about 1%. 1 Bacteria remains the most common pathogen of PJI. Meanwhile, fungal periprosthetic joint infection constitutes for approximately 1% for all PJI.2–6 Currently there is still no standardized management guideline developed for fungal PJI. A wide variety of surgical and antimicrobial management protocols have been reported.3–6 This report describes a rare case of candidia parasilosis periprosthetic joint infection seen at the author‘s center.
Case report
A 76-year-old Chinese lady initially presented to us with chronic bilateral knee pain with the diagnosis of knee osteoarthritis. Her past medical history included eczema and hypertension. She had undergone total knee replacement of her right knee in view of persistent knee pain. Prophylactic antibiotics of cefazolin was given on induction; operative time was 90 minutes. The in-patient post-operative period was uneventful.
During early follow up on post-operative day 13, a small amount of blood-stained discharge was noticed over the proximal part of the surgical wound. A wound swab has been taken for culture. An empirical course of cloxacillin was also prescribed to the patient. Daily dressing was prescribed to the patient. The wound condition seemed to improve and heal gradually. Gram stain of the wound swab showed nil white blood cell count and no microorganisms. Subsequently, the culture result showed scanty growth of candida species. On reassessment, the wound already healed well; patient has no knee pain and minimal knee effusion. It was regarded as contamination as no clinical signs of infection at that time.
The patient then suffered from slip and fall at the post-operative four weeks, resulting in a 6 centimeter superficial laceration of her right anterior knee. The laceration was documented to be superficial and not involving knee replacement components. The wound was treated with irrigation and suturing.
Subsequently the patient encountered other medical problems. She developed puritic skin rash after taking cloxacillin and was suspected to be allergic to cloxacillin. With the background history of eczema, she also developed flare-ups of generalized skin rash. Besides, the patient had episodes of syncope. She was found to have cortisol insufficiency after investigation. Glucocorticoid replacement therapy was prescribed. Subsequently, she developed iatrogenic Cushing syndrome.
At 6 months post-operatively, she presented with a spontaneous painful swelling of her right knee, progressively increasing in size for one week. Patient remained afebrile all along. Physical examination showed a four centimeter superficial erythematous fluctuant swelling around the inferolateral aspect of her right anterior knee, at the location near the tibial tuberosity. Xray showed suspicion of loosening over the medial aspect of the tibial implant. (Figure 1) Inflammatory markers were elevated. (WBC: 13.0*10^9/L, CRP 88.2 mg/L, ESR 74 mm/hr). Aspiration of the fluctuant swelling under aseptic technique yielded small amount of blood stained fluid. The culture of the blood-stained fluid showed Candida parapsilosis.
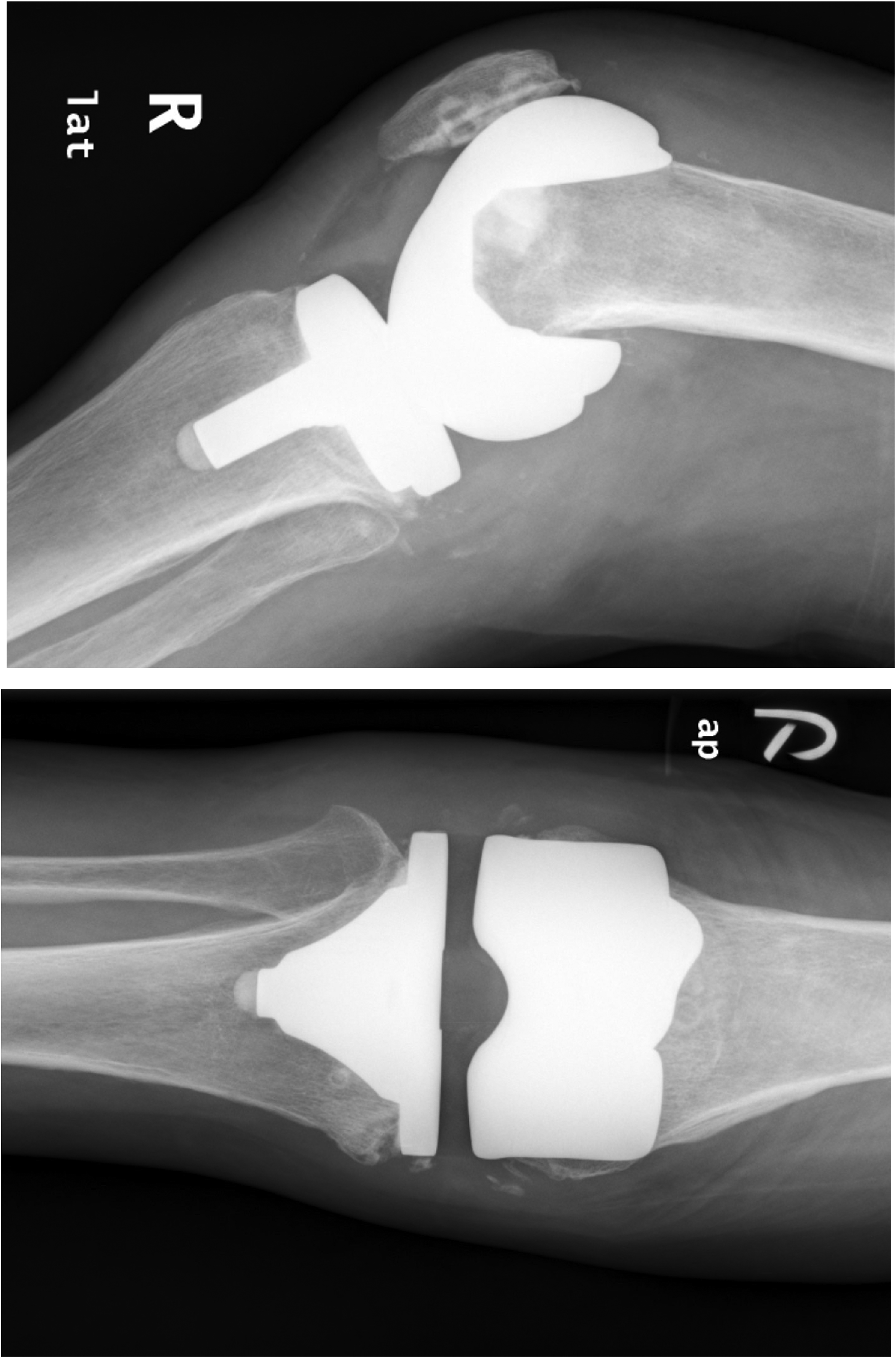
Post-operative 6 month xray right knee after primary total knee replacement.
Bone scintigraphy and Gallium scintigraphy for the patient was perofrmed. It showed an increase blood-flow and blood pool activity around the right knee with mildly increase gallium uptake at the superolateral aspect of the right knee. Marked increase MDP uptake and less intense gallium uptake was seen in the bone prosthesis interface of right distal femur and right tibial plateau. Operative treatment was planned. However, the patient refused operation. Anti-fungal treatment with oral fluconazole 50 mg capsule daily for 6 weeks was prescribed. With the anti-fungal therapy, the abscess decreased in size and infection appeared to subside afterwards.
At post-operative 10 month, the patient presented again to us with a similar problem of right knee painful fluctuant swelling. Yellowish fluid with sediment was aspirated from the abscess. The fluid culture result showed the growth of the same fungal organism of candidia parapsilosis. The abscess subsequently ruptured, draining pus and creating a one centimeter gap over the surgical scar of the knee replacement.
Patient eventually agreed for surgical management after repeated episodes of abscess formation. First stage of two-stage revision right total knee arthroplasty was performed at post-operative 22 months (Figure 2). Implant components together with the cement were removed; Fibrogranulation tissue was excised; a vancomycin loaded CMV cement spacer was inserted. Intra-operatively, a pocket of turbid fluid was found around the lateral tibial plateau region with communication to the prosthetic knee joint. Operative time was 80 minutes. Femoral bone, tibial bone, abscess wall tissue and knee synovium were taken as specimen for microscopy and culture. Initial gram smear showed no obvious fungal element, but scanty growth of candida parasilosis in fungal culture was detected in all four specimens.
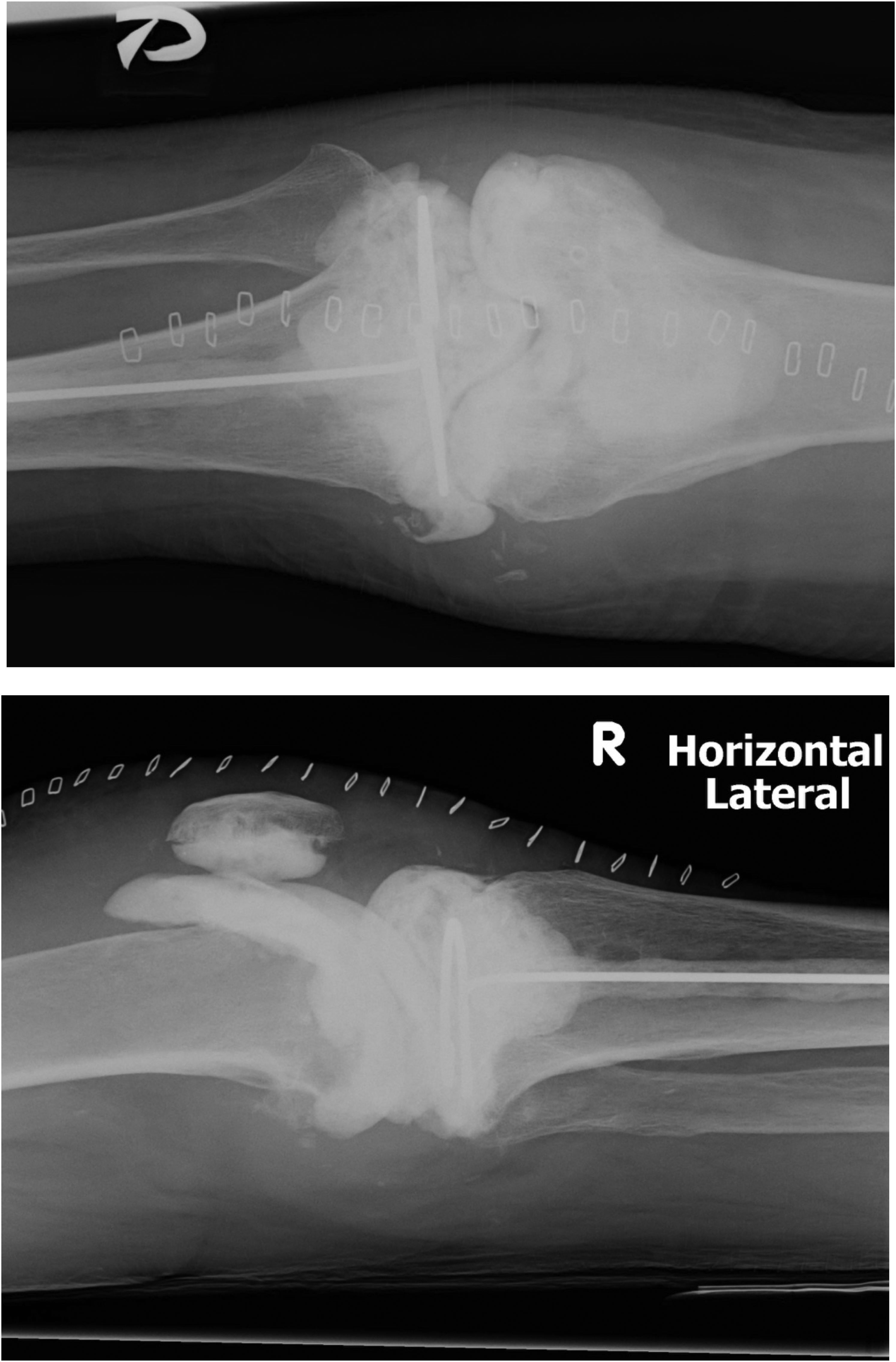
Post-operative xray right knee after 1st stage of 2-stage knee revision surgery.
Microbiologists suggested intravenous fluconazole of 400 mg daily. Inflammatory markers decreased in the early post-operative period. (CRP: 94.7 mg/L to 5.0 mg/L on post-operative day 19) After 2 weeks of Intravenous administration, fluconazole was switched to oral 400 mg daily. The patient remained afebrile and the wound was healing well. She was transferred to rehabilitation unit for further training. Patient could walk well in frame independently, and was discharged after two months of in-patient care. Total course of fluconazole was given for 6 months. On follow up, there were no clinical signs of infection and inflammatory markers remained low (CRP: 12.4 mg/L, ESR 33 m/hr in December 2012).
2nd stage of the revision right total knee replacement was scheduled in February 2013. However, it was noted to have a large amount of fibrogranulation tissue inside the right knee intra-operatively. In view of the suspicion of residual infection and unfavorable soft tissue conditions, new prosthetic implants were decided not to be implanted. Debridement of fibrogranulation tissue and irrigation was performed. The previous vancomycin cement spacers were replaced with new ones. After the operation, Inflammatory markers remained slightly elevated (CRP: 28.1 mg/L, WBC: 11.51 x10^9/L in May 2013), And the intra-operative culture from the samples of the 2nd operation were all negative. Microbiologist was consulted. Anti-fungal treatment was not to be given as there were no definite features of infection other than raised inflammatory markers.
Further revision surgery was then performed 4 months later. Intra-operative frozen section of synovial tissue showed less than 5 neutrophils per high power filed. (x40 22mm nikon) The cement spacer was removed; The fibrous granulation tissue around the knee was debrided; Bone was cut. New prosthetic implants were fixated and cemented with antibiotics loaded cement. Tissue cultures obtained from this surgery showed no bacteria or fungus growth.
Post-operatively, the patient received rehabilitation with further training and monitoring. During rehabilitation, the wound was complicated by stitch abscess with staphylococcus aureus infection. Stitches were removed and there were two tiny superficial wound cavities associated with discharge and surrounding erythema. No definite sinus tract or exposed implant was seen. The wound swabs culture yielded positive growth of methicillin-susceptible Staphylococcus aureus but no positive growth of fungi. She was treated with IV route of vancomycin for 2 weeks. Daily dressing was prescribed. ESR and CRP remained normal. The wound subsequently healed, and erythema decreased. In subsequent follow up, there was no clinical evidence of recurrence of periprosthetic joint infection was noted more than 5 years after the revision surgeries for her right knee. The recent blood tests were normal and X-ray was shown here (Figure 3). The clinical course of the patient is summarized in the form of a timeline (Figure 4).
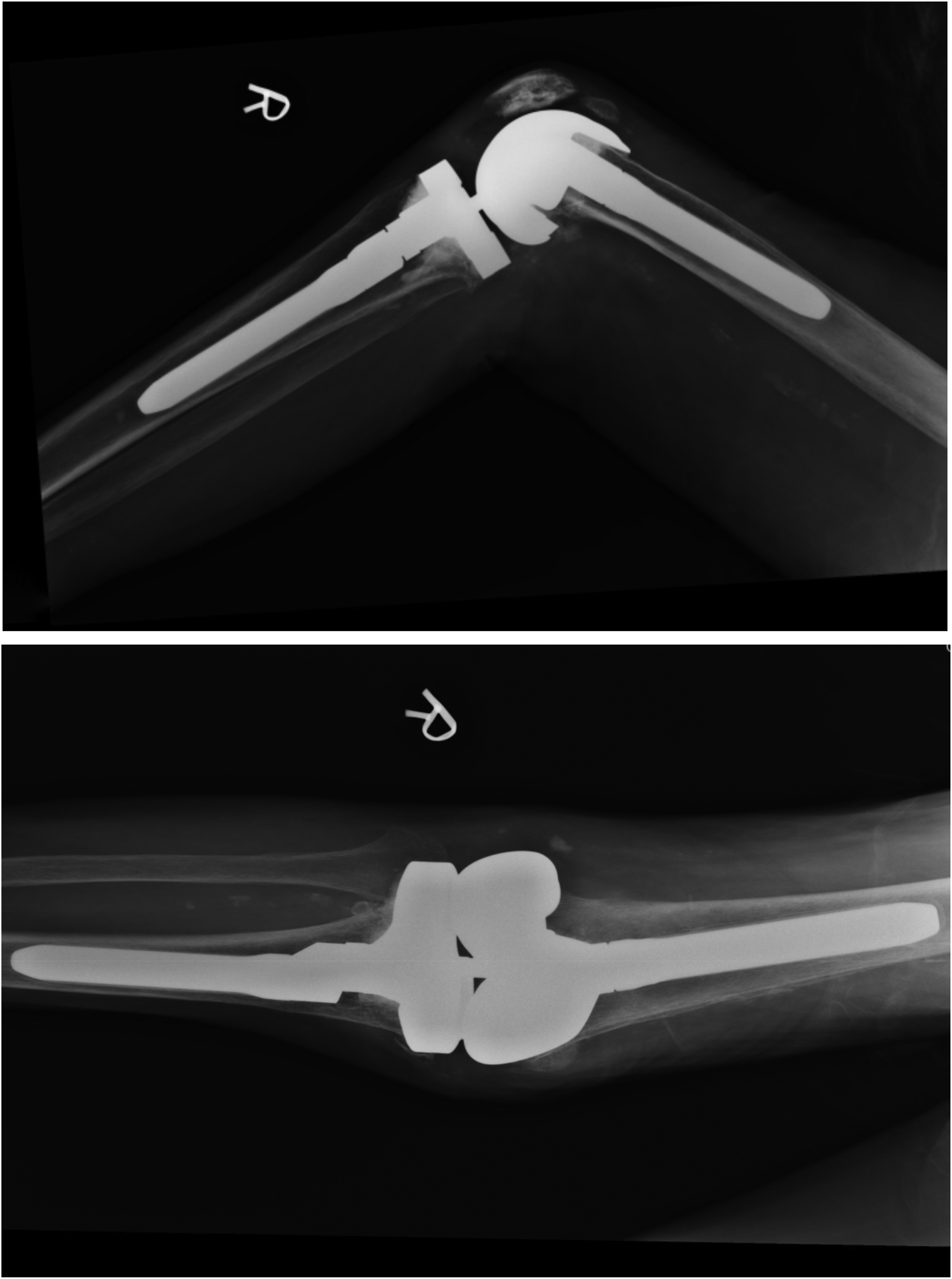
Post-operative 5 year xray right knee after 2-stage revision surgery.
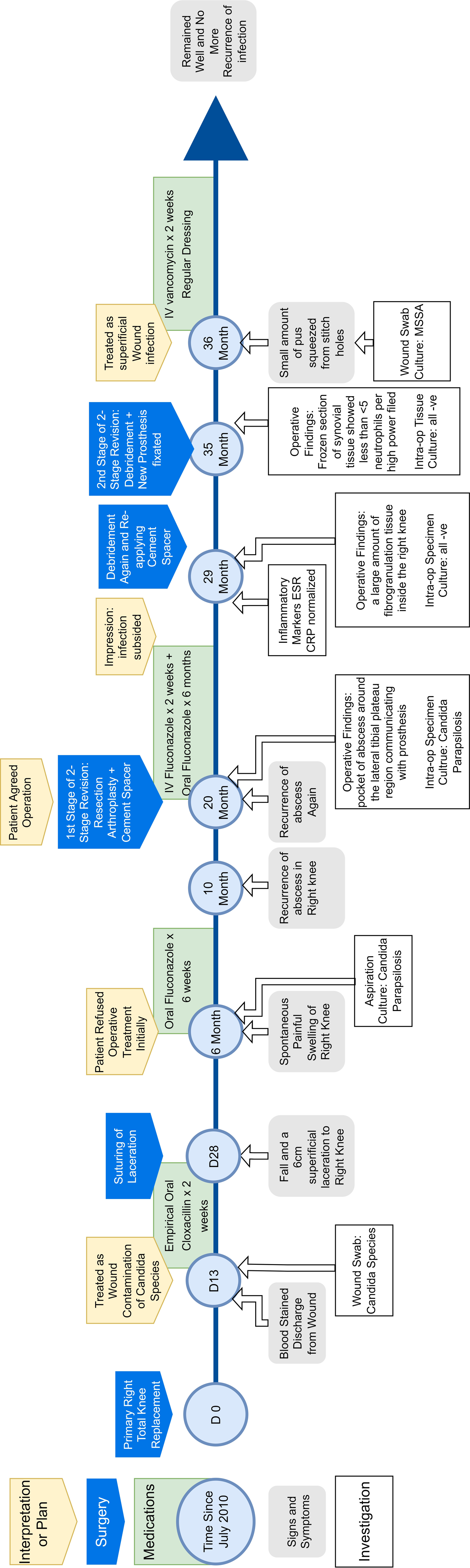
Timeline of the patient‘s clinical course.
Discussion
Current literature reported about 1% of periprosthetic joint infection are fungal in origin.7,8 It is a rare phenomenon, but also a deliberating complication to both patients and surgeon. More cases of fungal PJI are reported in recent years possibly due to the increasing incidence of joint arthroplasty. Risk factors of fungal PJI include immunosuppression, prolonged use of antibiotics, rheumatoid arthritis, diabetes mellitus, obesity, psoriasis, prior surgery at the site of the prosthesis. 9 In the patient included in this study, the main risk factor of fungal PJI included immunosuppression with iatrogenic Cushing syndrome after excessive steroid supplement, obesity and her age. Biofilm formation has a significant role in the development of fungal PJI in terms of the ability of fungi within the biofilm to withstand host immune defenses. 10 In a recent study by the author‘s center, fungal PJI is also shown to be rare. Revision result of fungal PJI seems promising with adequate treatment. 11
Pre-operative findings and diagnosis
Presenting symptoms of fungal PJI include pain (51%), local signs of infection (eg. Erythema, swelling and local warmth) [84%] and occasionally systemic signs of infection (eg. Fever and night swear) [11%]. 7 However, the onset of symptoms in fungal PJI is often insidious and slow in development. The relatively mild symptoms pose a significant diagnostic challenge to orthopedics surgeons. Elevated serological inflammatory markers are also reported, but there was no detailed analysis of serological markers in the case of fungal PJI because of limited data.
In one series, signs of loosening were shown in radiograph in 51% of patients (60 out of 118 patients). 12 These cases having X-ray evidence of loosening could be misdiagnosed as aseptic loosening especially those with normal serum inflammatory markers. 13 Repetitive aspirations and collection of tissue samples remain the most important step to diagnose a fungal PJI. 7
Another challenge is to elucidate whether the presence of Candida species in samples can be considered as a contaminant or not. In our patient, the culture of discharge from the surgical wound on post-operative 2 weeks yielded scanty growth of candida species. It was regarded as wound contamination in view of clinical findings. it is possible that candidia parasilosis had already entered the surgical wound. In a systemic review in 2013, Kuiper et al. revealed fungal culture results were initially considered to be contamination in 21% of all patients. 12
Treatment
Currently, the mainstay of treatment is a two-stage arthroplasty exchange with initial radical debridement, possible use of cement spacer, appropriate antimicrobial therapy, and delayed re-implantation. It is reported as the treatment strategy with the most promising outcome, but its success rate in infection control is still controversial. A study including 28 patients of fungal PJI reported a success rate of 93% for short-term infection control with two-stage arthroplasty and additional post-operative 6 months of oral antifungal agent. 14 Meanwhile, a systemic review including 21 studies shows that 77.3% of fungal PJI can be controlled with this staged treatment strategy. 15 Successful one-stage arthroplasty exchange in fungal PJI of the knee has been reported in several cases.3,16,17 However, the experience of one-stage arthroplasty exchange in fungal PJI is limited and needs further evaluation.
To conclude, the rarity of fungal PJI limits our understanding of fungal PJI. Diagnosis and management of fungal PJI remains a significant challenge to orthopedic surgeon. Currently, there is still no consensus or guideline in managing patients with fungal PJI. 8 ,18,19 Diagnostic criteria and management guidelines need to be established.
Footnotes
Authors’ note
Yau Chun Chong is now affiliated with Department of Orthopaedics & Traumatology, Pamela Youde Nethersole Eastern Hospital, Hong Kong.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
The patient and her family gave her informed verbal consent or the inclusion of her information in this publication.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.