
Abstract
Synovial chondromatosis (SC) is a rare benign disorder characterized by the presence of metaplastic cartilage nodules originating from the synovial lining of joints, bursa, and tendon sheaths. The treatment option is usually open surgery for excision of loose bodies and synovectomy, while on literature review only few cases with arthroscopic management are reported. We present a 28-year-old male patient who was evaluated for pain, swelling, and limited range of motion of the right ankle joint. Both physical examination and radiographic investigations were suggestive of primary SC of the ankle joint and arthroscopic surgery was performed. Removal of loose bodies and synovectomy were successfully performed. Histopathology confirmed the diagnosis. SC of the ankle is a rare disorder, and its treatment strategies depend on patient complaint, age, and the stage of the disease. Open or arthroscopic surgery can be performed. This case report suggests that arthroscopic management can provide successful outcome in such cases.
Introduction
Synovial chondromatosis (SC) is a rare condition characterized by the formation of intra-articular cartilaginous nodules in the synovial lining of joints. 1 These nodules can be separated and become loose bodies within the joint and may undergo secondary calcification. 2 The exact etiology is still unknown; it could be genetic, infections, or traumatic. 3 SC originating from the knee, hip, and elbow joints is frequently reported while that of the ankle is an extremely rare condition. 4 The disease is commonly seen in males and more between third and fifth decades of life. 5
Due to its chronicity, if left untreated, progressive degeneration of articular structures secondary to loose neoplastic cartilaginous nodules in the joint space can occur. 6
Open excision of loose bodies with synovectomy is the most common surgical intervention. 6 Nowadays, the arthroscopic approach is frequently preferred for ankle pathologies. The advantages of arthroscopic approach are several such as decreased morbidity, thorough visualization, and treatment. 4
Case presentation
A 28-year-old male patient presented to the outpatient clinic of our hospital complaining from decreased range of motion, swelling, and progressive pain in the right ankle joint during movement. He had no history of trauma, no family history of bone or joint diseases, and no history of any comorbidities.
On physical examination, the patient had mild swelling, mild tenderness around the anterior ankle joint line, and on palpation, palpable loose bodies were detected. The range of motion was 15° plantar flexion and 5° dorsiflexion. No signs of instability appeared in the ankle joint. Dorsalis pedis artery was well felt, and intact distal sensation with no neurovascular affection.
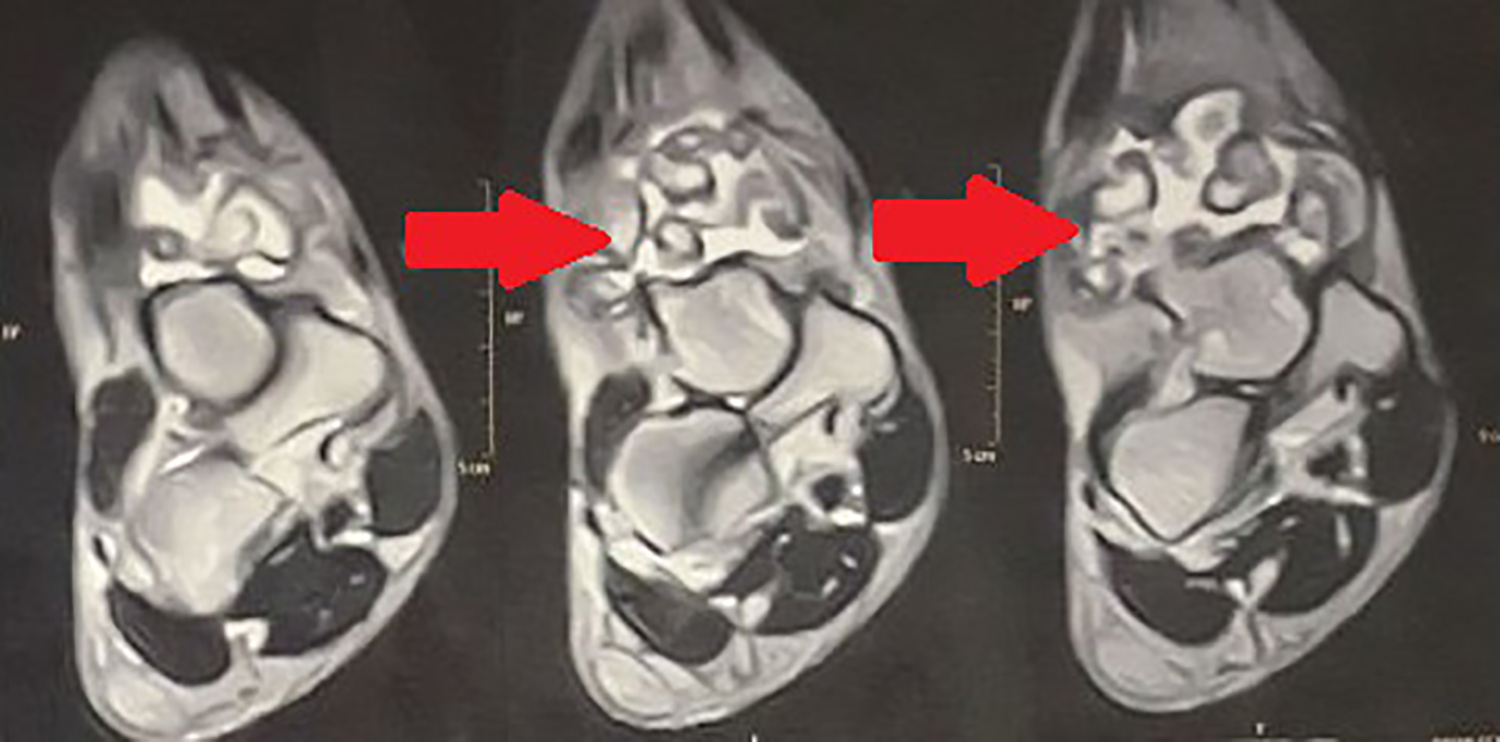
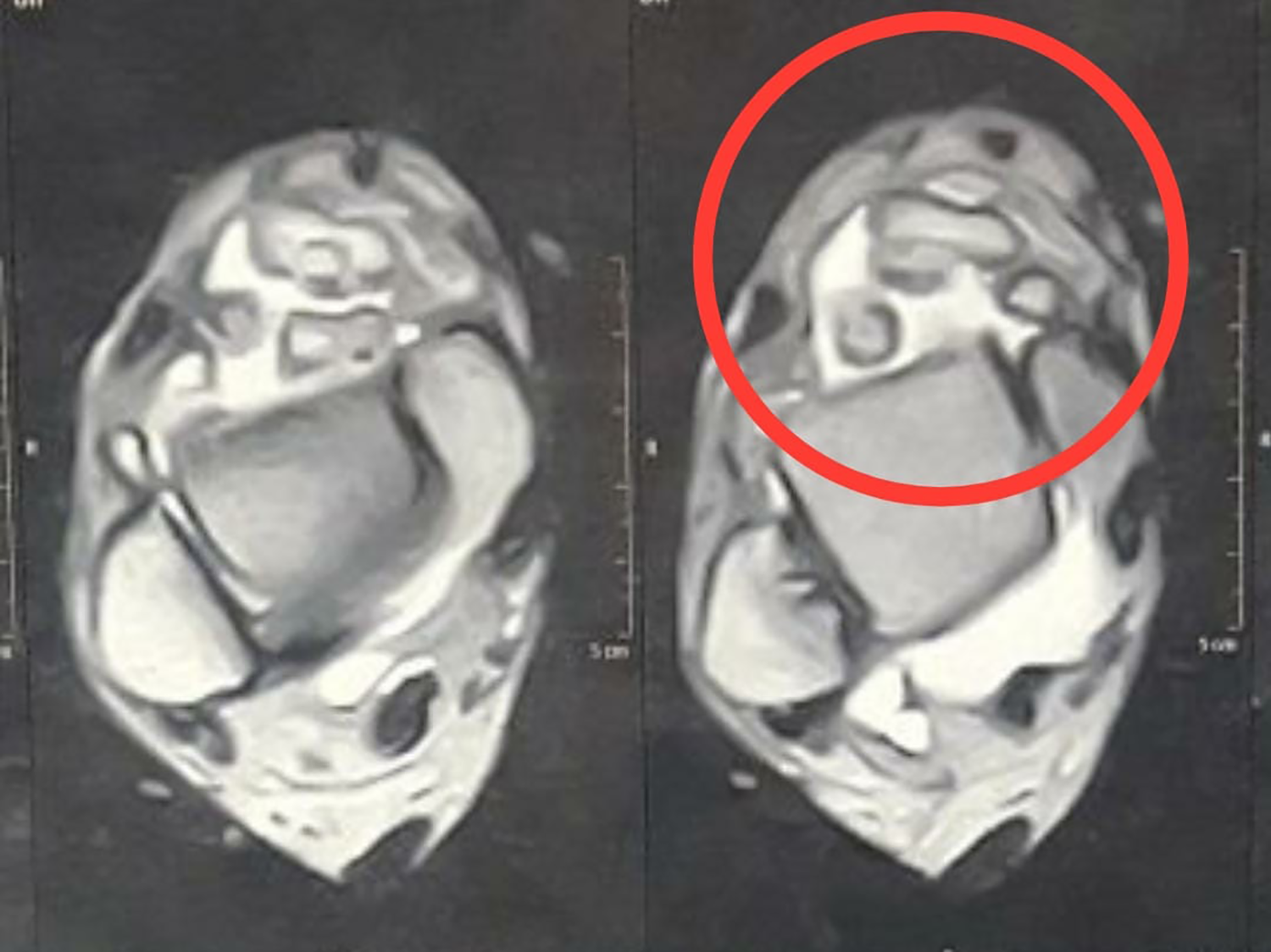
On plain radiography, multiple nodules about 3–9 mm in diameter of calcifications were seen at the anterior aspect of the ankle joint (Figure 1). Magnetic resonance imaging revealed multiple calcified well-circumscribed loose bodies at the same location and synovitis in the ankle joint (Figures 2 to 4).

Preoperative X-ray showed multiple nodules of calcifications at the anterior aspect of the ankle joint.
Coronal cuts of MRI of right ankle showed moderate joint effusion with multiple intermediate signal synovial hyprtrophy. MRI: magnetic resonance imaging.
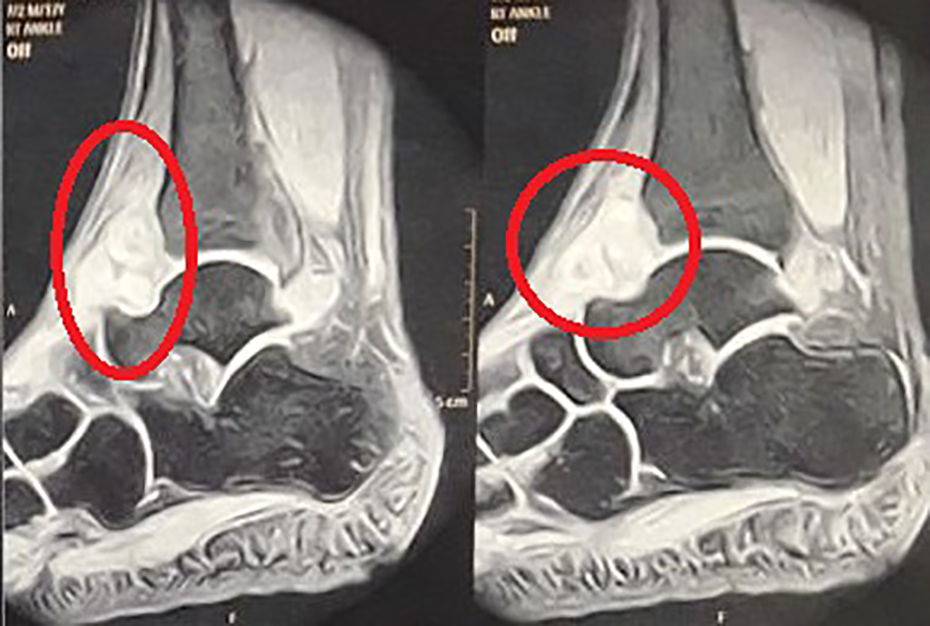
Sagittal cuts of MRI of right ankle multiple lobulated synovial hyprtrophy in anterior aspect of ankle joint. MRI: magnetic resonance imaging.
Axial cuts of MRI of right ankle multiple calcified well-circumscribed loose bodies in anterior joint space. MRI: magnetic resonance imaging.
Initial conservative measures including rest, physical therapy, and nonsteroidal anti-inflammatory drugs failed to provide adequate relief of symptoms.
Functional assessment was done using American Orthopaedic Foot and Ankle Society (AOFAS)-Hindfoot Scale. The preoperative score was 63 of 100 points.
The patient had ankle arthroscopy, under spinal anesthesia. Important landmarks were marked on skin using a permanent marker pen. This included tibialis anterior tendon, peroneus tertius tendon, and superficial peroneal nerve (SPN).
The patient was positioned in the supine position. The ankle joint was distended with 15 ml of sterile saline solution injected at the site of planned anteromedial portal, and accurate intra-articular injection was confirmed by passive dorsiflexion of the joint during injection and backflow from the syringe needle. The anteromedial portal was created first by a vertical skin incision just medial to the tibialis anterior tendon at the level of joint line, and then a mosquito forceps is used to spread the skin. The anterolateral portal created under vision using spinal needle with transillumination to avoid injury to the branches of SPN.
Routine arthroscopic examination of the ankle joint was made, and multiple loose bodies and hypertrophic synovial lining in the anterior ankle joint space were seen. Arthroscopic synovectomy using shaver blade and excision of loose bodies by arthroscopic grasper were performed. We used barrel sling technique as described by Ramataju and Schenk 7 with sterile elastic bandage for joint distraction and an accessory postrolateral portal was created under vision using a spinal needle inserted just lateral to the lateral border of Achilles tendon above the level of talar dome while the joint is distracted, and this portal was used to complete synovectomy of the posterior compartment. Skin incisions were closed using 2/0 prolene. Surgery took less than 45 min.
Postoperatively, range-of-motion exercises with partial weight-bearing using crutches as tolerated was encouraged from the first day.
Extracted tissues were sent for histopathological examination which confirmed the diagnosis of SC (Figure 5).

Intraoperative images of multiple loose bodies removed arthroscopically from ankle joint space.
We followed up the patient at our outpatient clinic at 2-week intervals. Sutures were removed after 2 weeks (Figure 6). Pain and limitation of motion improved within 2 weeks. Full weight-bearing started on the second week, while the active and passive range of motion and calf strengthening exercises continued for 6 weeks. Postoperative AOFAS score at 8 weeks was 91 of 100 points.

Anterolateral and anteromedial wounds after sutures removal with about 1 cm size.
Discussion
SC is a benign synovial metaplasia and multiple loose bodies formation. A review of the literature shows that reported ankle cases of this disease are limited. 8 No clear etiology is known, but classification of SC as described by Milgram 8 depended on the location of the loose bodies within a joint and the pathological findings of the synovium and loose bodies. He described this condition with three stages: first stage, cartilaginous loose bodies within the synovial membrane; second stage, intrasynovial involvement with loose bodies; and third stage, multiple free bodies due to synovial osteochondromatosis with tendency to calcify.
The recurrence rate has been reported to be from 11.5% to 37.5% postoperatively. A possible complication of SC is malignant transformation to chondrosarcoma, with a risk of about 5%. Malignant transformation is closely related to recurrence rate. 6
Main symptoms and signs are pain more with physical activity, joint swelling, decreased range of motion, joint clicking, locking, and palpable masses. 5
Imaging plays an important role to diagnose SC, in normal X-ray multiple intra-articular calcified loose bodies which are smooth and variable in size are usually seen in both anteroposterior and lateral views, while magnetic resonance imaging (MRI) could be useful if plain radiographs fail to demonstrate calcifications and are helpful in early stages to detect the exact localization of the disease and intrinsic property of the chondroid tissue. 9
The pathological confirmation of the disease allows the differential diagnosis of other conditions that gives same clinical and/or radiological picture of intra-articular loose bodies such as trauma, rheumatoid arthritis, tuberculosis arthritis, osteochondritis dissecans, and soft tissue chondrosarcoma. 6
In the early stages of the disease and in asymptomatic patients, an attempt of conservative treatment with regular follow-up can be an option. 10 Symptomatic patients are better managed surgically either open or arthroscopic. 5 Arthroscopic management of ankle SC is rarely discussed in the literature. 10 Advantages of arthroscopic surgery are to decrease wound exposure, to decrease risk of infection, being a less invasive procedure than open surgery, and can help in early rehabilitation. 4 Complete removal of such a large number of loose bodies in addition to performing synovectomy in both the anterior and the posterior compartments of the joint will require extensive simultaneous anterior and posterior approaches which will increase the risk of arthrofibrosis and prolonged rehabilitation. Arthroscopy also allows evaluation of the entire articular surface for potential degeneration including gutters and allows almost complete synovectomy. Achieving the two goals via open surgery is almost impossible. 4,11
In our case, young male who had clinical and radiological picture of SC, a trial of conservative management failed to improve pain and limitation of motion for 2 months, and these were the indications for surgical intervention. Arthroscopic loose bodies excision and synovectomy was chosen. Short-term follow-up showed satisfactory outcome as regards pain and range of motion that compares favorably to open surgical procedures in the literature.
Conclusion
SC is a rare but most often benign condition involving a single joint of unknown etiology, with formation of multiple cartilaginous loose bodies. Excision of these loose bodies and synovectomy can improve the condition. Synovial resection is the agreed-on treatment process for all joints, and arthroscopic approach is a valuable minimally invasive tool to achieve good outcome in these cases in the ankle joint.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.