
Abstract
Purpose
Evaluate the clinical outcomes after arthroscopic treatment of synovial chondromatosis (SC) of the hip.
Materials and Methods
We evaluated patients who underwent arthroscopic management for SC of the hip from November 2008 to March 2017. Radiographic evaluation was made before and after surgery. The modified Harris Hip Score (mHHS), Hip Disability and Osteoarthritis Outcome Score (HOOS), visual analogue scale (VAS) score, and patient self-reported satisfaction were collected and analyzed before and after surgery. Complications and recurrence that occurred after surgery were recorded.
Results
Forty-one patients (27 men and 14 women) were the study cohort. The mHHS improved from 67.0 to 83.7, HOOS-Symptoms improved from 78.8 to 93.3, HOOS-Pain improved from 80.9 to 93.6, HOOS-Activity Limitations–Daily Living improved from 84.5 to 95.1, HOOS-Sport improved from 50.3 to 80.6, and HOOS-Quality of Life improved from 62.2 to 86.7. VAS scores decreased from 3.9 to 1.1. All results demonstrated significant improvement (P < 0.05). Thirty-three (80.5%) patients thought the outcome of surgery was “excellent,” 7 (17.0%) thought it was “good,” 1 (2.4%) thought it was “fair,” and no one thought it was “poor”. Two patients underwent revision surgery.
Conclusion
Hip arthroscopy for SC treatment of the hip showed good clinical results, good satisfaction from patients, and low recurrent prevalence.
Introduction
Synovial chondromatosis (SC) is a relatively rare and benign disease characterized by metaplasia of the synovial membrane and formation of multiple calcified nodules.1,2 Histology shows metaplasia of synovial mesenchymal cells. 3 The exact cause of SC is not known. The hip is the second most commonly affected joint after the knee. 4 Clinical presentation is usually characterized by pain, mechanical locking, and stiffness in the hip. 3
Surgical removal of loose bodies undertaken using open or arthroscopic approaches is first-choice treatment. 5 Conventional “open” surgery has shown good results,6,7 but prolonged rehabilitation and many complications have been highlighted as disadvantages.8,9 Recently, several scholars have described the arthroscopic approach to this condition with revealed good clinical outcomes.1,3,5,10-12 But the number of patients is relatively small.
We wished to evaluate the clinical outcomes and recurrence prevalence of patients undergoing hip arthroscopy for SC.
Materials and Methods
Patients
We evaluated patients who underwent arthroscopic management for SC of the hip from November 2008 to March 2017. Patients who underwent arthroscopic management and had a confirmed diagnosis of SC after pathology postoperatively met the inclusion criteria of our study. Patients with prior hip surgery were excluded from the present study. All participants provided written informed consent. The study protocol was approved by the relevant institutional review board.
Clinical and Radiologic Assessment
Supine anteroposterior hip radiographs, cross-table lateral radiographs, and computed tomography (CT) images were obtained for all patients preoperatively to measure the center-edge (CE) angle, alpha angle, joint space, and degree of femoral head–neck offset. The alpha angle was measured from CT images using the method described by Notzli et al. 13 The CE angle was measured from radiographs using the method described by Ömeroglu et al. 14 The joint space was measured from radiographs using the method described by Reis et al. 15 The offset was evaluated on cross-table lateral radiographs using the method described by Notzli et al. 13 Supine anteroposterior hip radiographs were undertaken to check for the existence and locations of radiopaque loose bodies. CT and magnetic resonance imaging (MRI) were carried out on all patients to confirm the diagnosis preoperatively. Supine anteroposterior hip radiographs and CT images were obtained for all patients on postoperative day 1 to evaluate residual loose bodies.
Surgical Procedure
Hip-joint arthroscopy was carried out by one surgeon with more one decade of experience of this procedure. Arthroscopic hip surgery was done in the supine position with a standard fracture table and custom perineal post. Standard arthroscopic portals (anterolateral and mid-anterior) were used in the present study.
The surgical procedure could be divided into 3 steps. First, the hip was moved into ~45° of flexion and the peripheral compartment explored without joint distraction. We used 30°-arthroscopes in this step. Most of the loose bodies could be removed by lavage, and larger ones could be removed using a grasper. Second, traction was applied to the operative extremity to ensure that, under fluoroscopic guidance, the hip-joint space on the operative side was 8 to 10 mm. In addition, the hip joint was brought into extension, abducted slightly, and rotated internally. A radiofrequency tool was used to complete capsulotomy. Detailed inspection of the central compartment was undertaken to assess the acetabular rim, acetabular labrum, articular cartilage, and ligamentum teres. We mainly used 70°-arthroscopes in this step. Removal of loose bodies and synovectomy was done ( Fig. 1 ). Labral repair/debridement was carried out according to the extent of the injury. Articular cartilage lesions of the acetabulum and femoral head were evaluated according to the Outerbridge classification. 16 Finally, the hip was moved into ~45° of flexion and various degrees of rotation for thorough inspection of the peripheral compartment again after traction release and removal of the custom perineal post. Full flexion and external rotation allowed for relaxation of the anterior capsule and better access to the most medial portions of the peripheral compartment. 11 Extension and internal rotation allowed better access to the most lateral aspects of the compartment. 11 If a “cam bump” in the head-neck junction or acetabular overcoverage was identified, femoral osteoplasty or acetabuloplasty was carried out. Residual loose bodies in the peripheral compartment were removed effectively by moving the leg through various positions. Removed loose bodies and synovium were sent for histopathology.
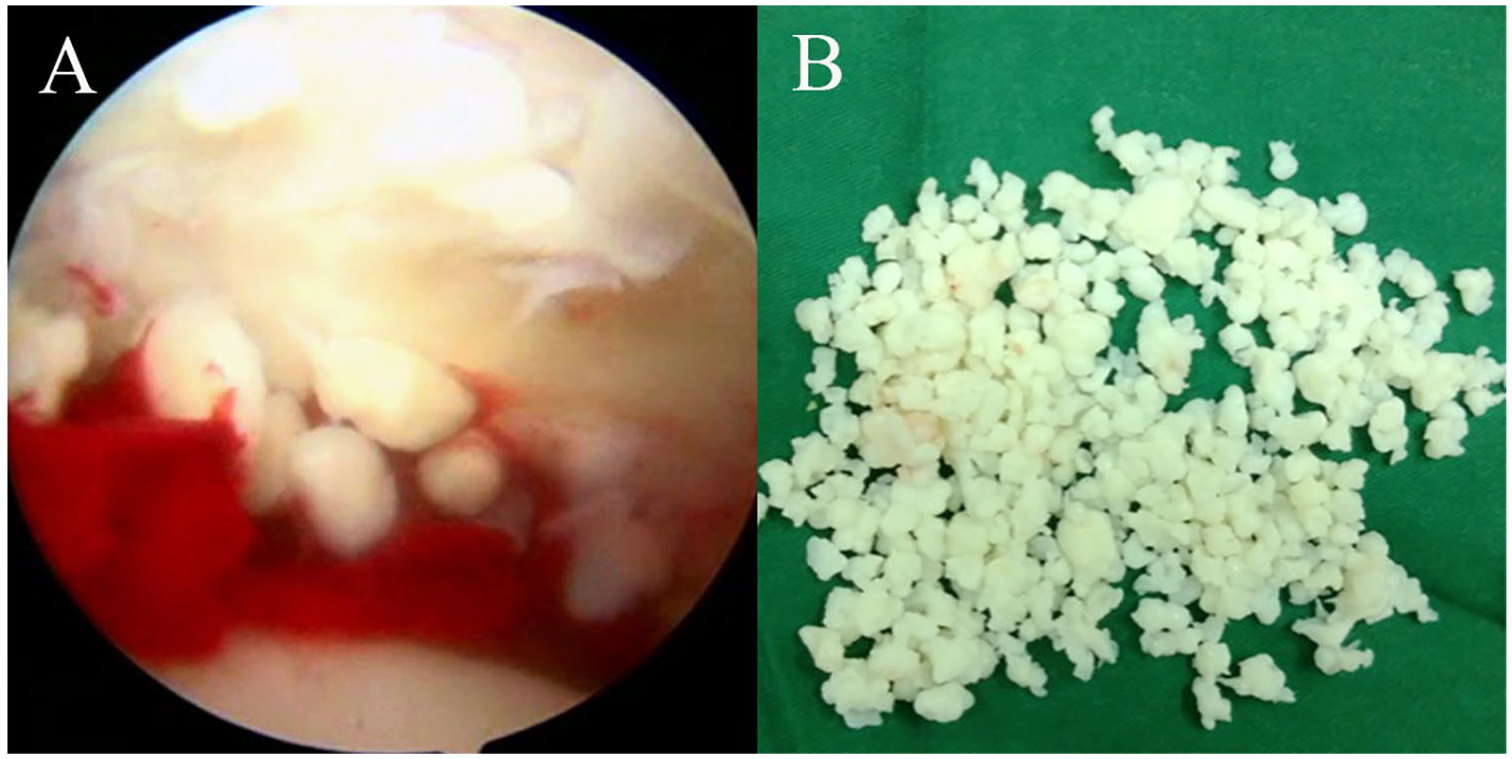
(
Outcome Measures
The modified Harris Hip Score (mHHS), Hip Disability and Osteoarthritis Outcome Score (HOOS), visual analogue scale (VAS) score, and patient self-reported satisfaction (“excellent,” “good,” “fair,” “poor”) with surgical outcomes were collected and analyzed before and after surgery.
The HOOS consists of 39 items assessing 5 patient-relevant dimensions: Pain, Symptoms (including stiffness and range of motion), Activity Limitations–Daily Living (ADL), Sport (Sport and Recreation function), and QoL (Hip-Related Quality of Life). To enhance interpretation, HOOS was transformed into a worst → best (0-100) scale.
Statistical Analyses
The paired t test (2-tailed) was used to evaluate significance between preoperative and postoperative groups. P < 0.05 was considered significant. Statistical analyses were carried out using SPSS v11 (IBM, Armonk, NY, USA).
Results
Demographics
Fifty-five patients were eligible for inclusion. Except for 14 patients lost to follow-up, 41 patients (27 men and 14 women) formed the study cohort. Follow-up was completed for 74.5% of patients. Mean age at surgery was 37.6 years (range, 14-69 years). The mean body mass index (BMI) was 23.8 kg/m2 (range, 18.8-31.4 kg/m2). Twenty-four cases had SC on the right side, and 17 cases had SC on the left side. The mean time for symptom onset preoperatively was 30.6 months (range, 1-144 months). The mean duration of postoperative follow-up was 48.7 months (range, 27-119 months). Patient demographics are presented in Table 1 .
Patients Demographics. a .
Values are the mean (range) unless indicated otherwise.
Radiology
As shown in Table 2 , the mean alpha angle preoperatively was 47.3° ± 10.1° (range, 34.4°-74.2°). The mean CE angle preoperatively was 39.5° ± 9.2° (range, 23.2°-59.6°). The mean joint space preoperatively was 4.5 ± 1.0 mm (range, 2.4-7.4 mm). The preoperative femoral offset was 6.2 ± 2.7 mm (range, 2.3-12.9 mm). As shown in Figure 2 , radiopaque loose bodies were presented on the preoperative radiographs of 19 patients. CT identified the shadows of loose bodies in 24 of 41 cases. MRI showed loose bodies in 20 of 41 patients. Fourteen patients had no evidence of loose bodies on imaging. Postoperative radiographs showed residual loose bodies in 7 patients, and CT identified residual loose bodies in 10 patients postoperatively ( Fig. 3 ).
Various Parameters Revealed on Preoperative Radiology. a .
Values are the mean ± SD (range) unless indicated otherwise.
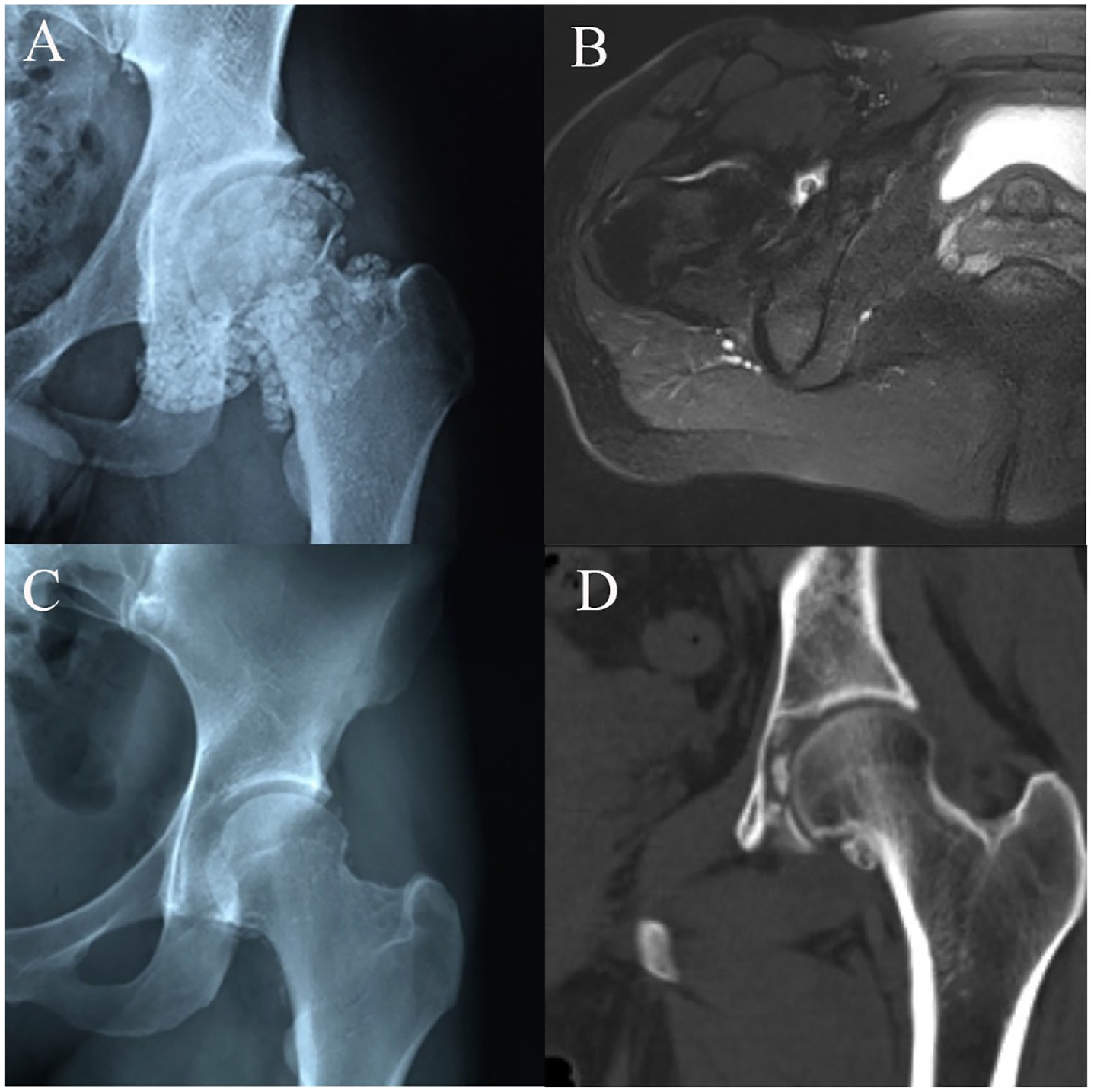
Synovial chondromatosis revealed on imaging. (
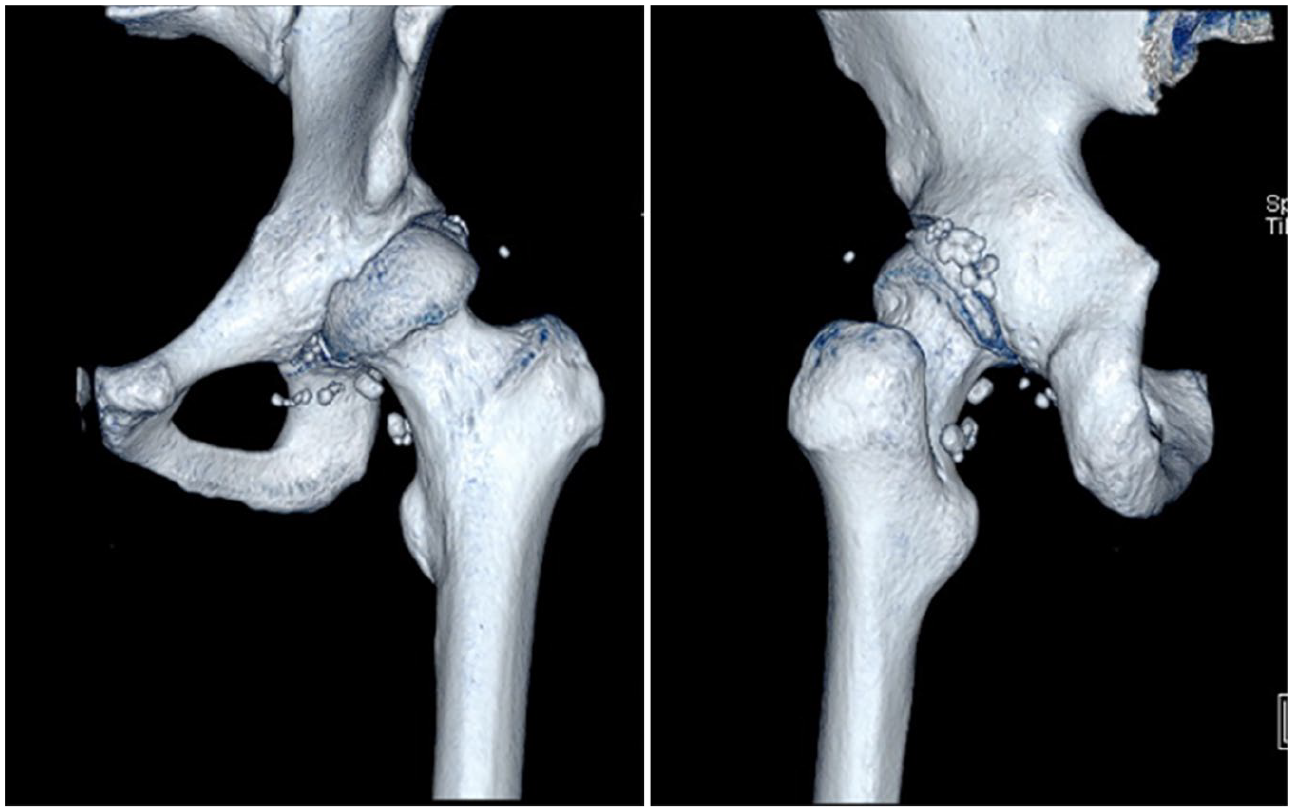
Residual loose bodies in the posterior hip joint, extra-articular and subcutaneous areas postoperatively.
Arthroscopy
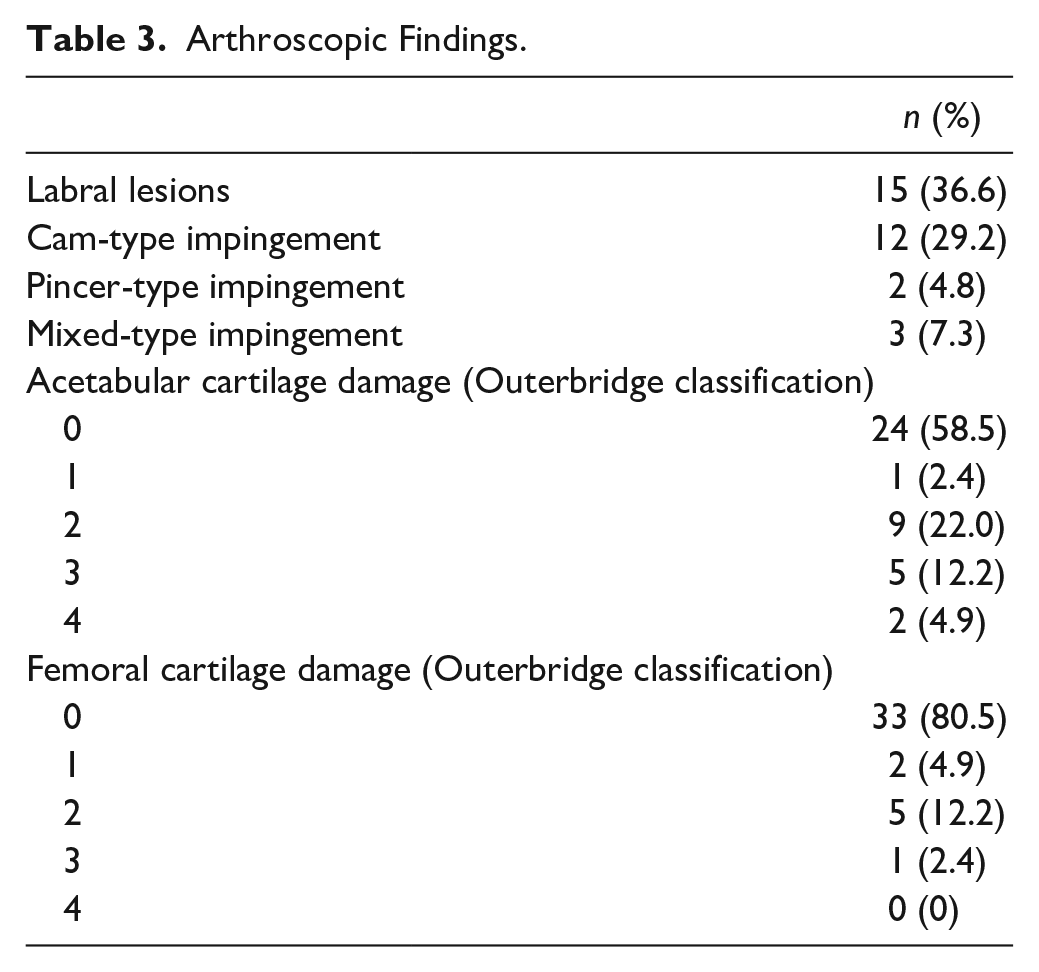
There were no loose bodies in the central compartment of four patients and no loose bodies in the peripheral compartment of 1 patient. The acetabular fossa was a common location of loose bodies. Most patients had countless loose bodies. Fifteen patients had labral lesions, and 5 of them underwent labral repair or debridement combined with loose-body removal. Twelve patients presented a cam-type impingement, 2 presented a “pincer”-type impingement, and 3 presented a “mixed”-type impingement. Nine patients underwent femoral osteoplasty or acetabuloplasty. Articular cartilage lesions were classified using the Outerbridge classification. Seventeen of 41 patients had cartilage lesions of the acetabulum: 1 case was at stage I, 9 cases were at stage II, 5 cases were at stage III, and 2 cases were at stage IV. Eight of 41 patients had cartilage lesions of the femoral head: 2 cases were at stage I, 5 cases were at stage II, and 1 case was at stage III. Arthroscopic findings are presented in Table 3 .
Arthroscopic Findings.
Patient-Reported outcomes
The mHHS improved from 67.0 ± 15.7 (range, 32-87) preoperatively to 83.7 ± 13.0 (range, 50-91) postoperatively and the mean improvement was 16.7 ± 13.4 (range, 0-49). HOOS-Symptoms improved from 78.8 ± 16.1 (range, 35-100) preoperatively to 93.3 ± 11.5 (range, 60-100) postoperatively and the mean improvement was 14.5 ± 14.6 (range, −5 to 55). HOOS-Pain improved from 80.9 ± 14.6 (range, 30-97.5) preoperatively to 93.6 ± 10.8 (range, 57.5-100) postoperatively and the mean improvement was 12.7 ± 13.1 (range, −5 to 67.5). HOOS-ADL improved from 84.5 ± 15.6 (range, 33.8-98.5) preoperatively to 95.1 ± 9.4 (range, 67.6-100) postoperatively and the mean improvement was 10.6 ± 13.9 (range, −5 to 58.5). HOOS-Sport improved from 50.3 ± 18.6 (range, 6.25-81.25) preoperatively to 80.6 ± 26.8 (range, 18.75-100) postoperatively and the mean improvement was 30.3 ± 21.5 (range, −6.25 to 58.5). HOOS-QoL improved from 62.2 ± 17.8 (range, 6.25-81.25) preoperatively to 86.7 ± 17.1 (range, 50-100) postoperatively and the mean improvement was 24.5 ± 14.1 (range, 0-50). VAS scores decreased from 3.9 ± 1.2 (range, 2-7) to 1.1 ± 1.4 (range, 0-5) and the mean decrease was 2.9 ± 1.4 (range, 0-7). No patient required total hip arthroplasty. Complications such as infection, neurovascular injury or hip dislocation/fracture were not reported. All results demonstrated significant improvement (P < 0.05). Thirty-three (80.5%) patients thought that the outcome of surgery was “excellent,” 7 (17.0%) thought it was “good,” 1 (2.4%) thought it was “fair,” and no one thought it was “poor.” Patient-reported outcomes are presented in Table 4 .
Patient-Reported Outcomes and Satisfaction.
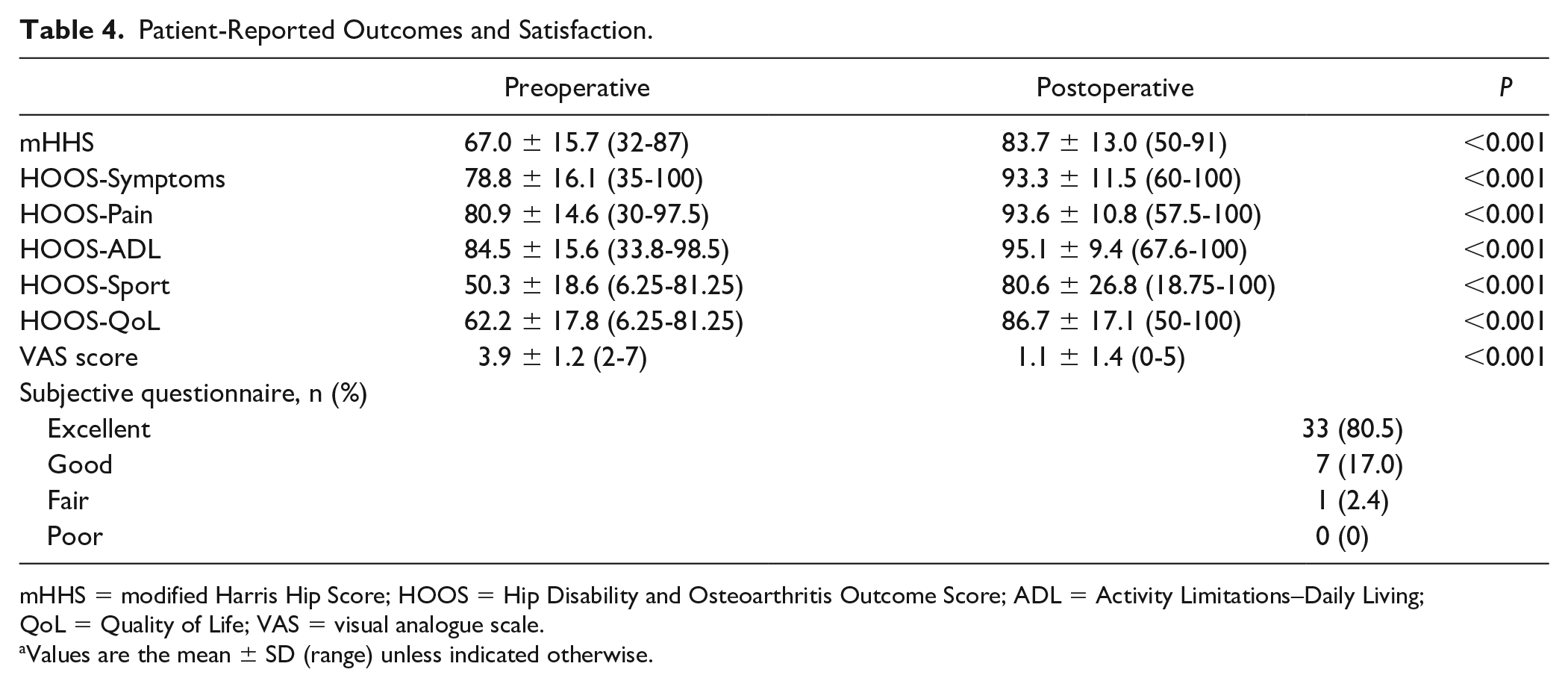
mHHS = modified Harris Hip Score; HOOS = Hip Disability and Osteoarthritis Outcome Score; ADL = Activity Limitations–Daily Living; QoL = Quality of Life; VAS = visual analogue scale.
Values are the mean ± SD (range) unless indicated otherwise.
During the study period, 2 patients underwent revision hip arthroscopy. One woman (42 years) underwent arthroscopic capsular release 20 months after the index procedure because of adhesions within the hip. No loose bodies were found during surgery. A man (44 years) underwent revision arthroscopy to remove loose bodies 17 months after the index procedure because of recurrent SC.
Discussion
SC is a relatively rare and benign idiopathic disease. Intra-articular loose bodies can cause articular cartilage damage and lead to joint degeneration. SC tends to recur, and malignant transformation into synovial chondrosarcoma or chondrosarcoma has been documented.1,3,17-19 Therefore, timely diagnosis and treatment are very important.
Milgram et al. 20 described 3 stages in the pathogenesis of SC. Stage I involves metaplasia in the synovial membrane without loose bodies. In stage II, progressive metaplasia leads to the detachment of loose bodies, which are surrounded partially by a synovial membrane. In stage III, there is no longer metaplastic activity in the synovial membrane. Many loose bodies in the joint can be observed. Diagnosing SC at stage I by MRI is challenging. MRI can be used to make a definitive diagnosis in stages II and III, but differentiation from pigmented villonodular synovitis (PVNS) can be difficult. In the present study, PVNS was diagnosed preoperatively but shown to be SC postoperatively in 1 patient. And 1 patient was misdiagnosed with SC preoperatively and shown to have PVNS postoperatively. These cases illustrate the difficulty in the differential diagnosis of atypical SC and PVNS. Hence, more attention should be paid to the clinical presentation and different examinations in the diagnosis and treatment of atypical cases. Also, various surgical options should be available for patients with features suspicious of SC on imaging.
Surgical removal of loose bodies using open or arthroscopic approaches elicits good results.1,3,5-7,10-12 Conventional open surgery carries an increased risk of infection, possibility of iatrogenic fracture, and prolonged rehabilitation.8,9,21,22 Patients undergoing arthroscopic surgery tend to have a shorter stay in hospital, less postoperative pain, fewer complications, and faster recovery.3,23 Our findings are similar to previous studies in that and we found arthroscopy for SC of the hip elicited good results.
The surgical procedure we used could be divided into 3 steps based on compartments: peripheral, central, and peripheral. This approach has the advantages of (a) ensuring the integrity of the peripheral compartment before capsulotomy and (2) reducing the risk of leakage of loose bodies in the peripheral compartment into the central compartment during traction. Some patients continued to have some residual loose bodies, as shown in postoperative imaging, especially in the posterior acetabular fossa, posterior capsule of the hip joint, extra-articular and subcutaneous areas. Lee et al. 1 reported on the difficulty of arthroscopy when approaching the posterolateral and posteromedial areas of the peripheral compartment. The symptoms and imaging of some patients with hip SC are atypical and some loose bodies cannot be seen on imaging, so we recommended thorough inspection of the joint intraoperatively. Therefore, hip arthroscopy has the dual functions of diagnosis and treatment.
Fifteen patients presented a cam-type impingement, 1 presented a pincer-type impingement, 7 presented a mixed-type impingement, and 24 patients had labral lesions. In recent years, several researchers have reported cases of hip SC combined with femoroacetabular impingement (FAI) and tried to reveal the relationship between them.11,17,18,24 Abolghasemian et al. 17 reported that hips with SC may present with clinical and radiographic features resembling those of cam-type FAI. They recommended consideration of SC in patients presenting with unilateral cam-type FAI before surgery. Ferro et al. 11 suggested that each patient undergoing hip arthroscopy for FAI should have a synovial biopsy if multiple loose bodies and extensive synovitis are observed after inspection. Padhy et al. 24 recommended an open approach to finalize debridement of the hip joint and excision of femoral and acetabular impingement deformities simultaneously. Considering that most FAI were anterior and that an open approach is more traumatic, we used arthroscopy to treat SC and cam-type FAI simultaneously.
Recurrence after open surgery for SC has been reported to range from 0% to 22%.1,25 Darren et al. 22 reported (in a systematic review) an approximate recurrence of 7.1% after arthroscopic removal of loose bodies and synovectomy. Boyer and Dorfmann 10 reported that SC recurred in 38.8% of cases, and revision surgery using open or arthroscopic approach was conducted. It was notable that 68% of patients in their study did not undergo inspection of the central compartment. Lee et al. 1 reported recurrence of 16.7%, and suggested that more synovectomy, loose-body removal and an additional medial portal are helpful to reducing recurrence risk. Zini et al. 3 reported no recurrence in 11 patients except for one patient undergoing hip replacement. Ferro et al. 6 reported 2 patients who underwent revision surgery and emphasized the importance of joint distraction and thorough systematic inspection. In the present study, 2 of 41 patients underwent revision arthroscopy because of adhesions within the hip or recurrent SC.
In conclusion, hip arthroscopy for SC treatment elicited good clinical results, good satisfaction from patients, and a low prevalence of recurrence.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by Peking University Third Hospital Institutional Review Board (IRB #000067612014205).
Informed Consent
All patients signed an informed consent form before participation.
Trial Registration
Not applicable.