
Abstract
Background:
Atypical femoral fracture (AFF) is a serious adverse event associated with bisphosphonate therapy and prone to complications and delayed union. We propose a technique and management strategy to maximise bone healing and outcomes.
Methods:
We report on a cohort of patients with AFF using our novel technique of preparing the intramedullary canal and rigid fixation with cephalomedullary nailing. Patients were admitted under a multidisciplinary team with rehabilitation goals of early mobilisation and teriparatide initiation. Clinical and radiographic data were retrospectively reviewed.
Results:
Twenty-eight AFFs were treated with a mean follow-up of 58.5 weeks and a mean age of 75.2 years old. All cases achieved radiological union by a mean of 6 months and post-operative thigh pain experienced up to 8.7 weeks. No cases underwent revision or experienced intraoperative complication.
Conclusion:
Our surgical technique and multidisciplinary management are reproducible with excellent results in patients with this rare yet challenging injury.
Introduction
The use of bisphosphonates has been widely established to reduce the risk of fragility fractures in patients with osteoporosis and metabolic bone disease. 1 Bisphosphonates reduce bone resorption by inhibiting osteoclast activity leading to an overall increase in bone mineral density. 2
However, there has been growing concern over the risk of atypical femoral fracture (AFF) relating to long-term bisphosphonate therapy. 3,4 The exact mechanism of AFF is poorly understood though recent evidence suggests that bisphosphonates create focal areas of dense, brittle bone due to irregular and increased collagen cross-linking. The subtrochanteric region of the femur is particularly prone owing to the high tensile and compressive forces encountered in this region. Owing to poor bone turnover in these regions, microdamage and stress injury can occur, which progress to fracture. 5 –7
The duration of clinical bisphosphonate treatment is uncertain and in patients with high risk of fracture, treatment for up to 60 months may be recommended. 8 Epidemiological evidence suggests that AFFs are more common in patients who have had 3 or more years of treatment (median 7 years). The absolute risk of AFF is moderately low and ranges from 3.2 to 50 cases per 100,000 person years. 9 Nonetheless, as these fractures are pathological in nature, they are associated with delayed healing, nonunion and complex reoperation when compared to nonpathological fracture equivalents. 10,11 As a consequence, these can be very challenging injuries to manage.
We offer a variation in the surgical technique and management of AFFs. We hypothesise that our specific surgical technique of over-reaming the intramedullary canal by 2.5 mm greater than the diameter of the implant and static rigid fixation with a cephalomedullary nail improves fracture union and reduces intraoperative complication. Our multidisciplinary approach to rapid optimisation, establishing rehabilitation goals of early mobilisation and normalising bone homeostasis may lead to better functional outcomes and a shorter hospital admission. The aim of this study was therefore to assess union rates, risk of re-operation and length of stay in a cohort of patients with AFF using our novel, multifaceted strategy and whether it affords better outcomes than those currently reported in the literature.
Methods
Patient selection
A retrospective review was performed on adult patients who had undergone intramedullary nailing to treat acute bisphosphonate-related AFF at our trauma unit between the years 2015 and 2019 with a minimum follow-up of 9 months. Exclusion criteria included patients with neck of femur, high velocity, open or pathological fracture due to underlying malignancy and patients on steroid therapy. Fractures stabilised with plate osteosynthesis or other modes of fixation were also excluded.
This study comprised a cohort of 28 consecutive patients who had their procedures and follow-up at our single institution and all analyses were performed at the latest point in follow-up. A senior orthopaedic surgeon and orthogeriatrician clinically and radiographically assessed all patients preoperatively.
Radiographs were compared against the American Society for Bone and Mineral Research (ASBMR) radiological criteria
9
to confirm the diagnosis of AFF, which must satisfy four of the five following features: The fracture is associated with minimal or no trauma, as in a fall from standing height or less; The fracture line originates at the lateral cortex and is substantially transverse in its orientation, although it may become oblique as it progresses medially across the femur; Complete fractures extend through both cortices and may be associated with a medial spike; incomplete fractures involve only the lateral cortex; The fracture is non-comminuted or minimally comminuted; Localised periosteal or endosteal thickening of the lateral cortex is present at the fracture site.
Surgical technique
We employ the standard principles of intramedullary nailing for AFFs, which is in line with National Institute of Health and Care Excellence guidance on the management of subtrochanteric femoral fractures. 8 Bisphosphonate-related fractures are subject to prolonged healing times, which can cause persistent stress concentration at the fracture site, therefore, long, large diameter nails are preferred over short implants. 6 The patient is positioned supine with the ipsilateral limb in a traction boot to re-establish length and alignment. Anatomical reduction should be achieved using closed techniques or through minimally invasive incisions to allow the safe use of bone holding forceps or Schanz pins. After placement of a guidewire, the intramedullary canal is then prepared with sequential reamers (Figure 1(a) and (b)).
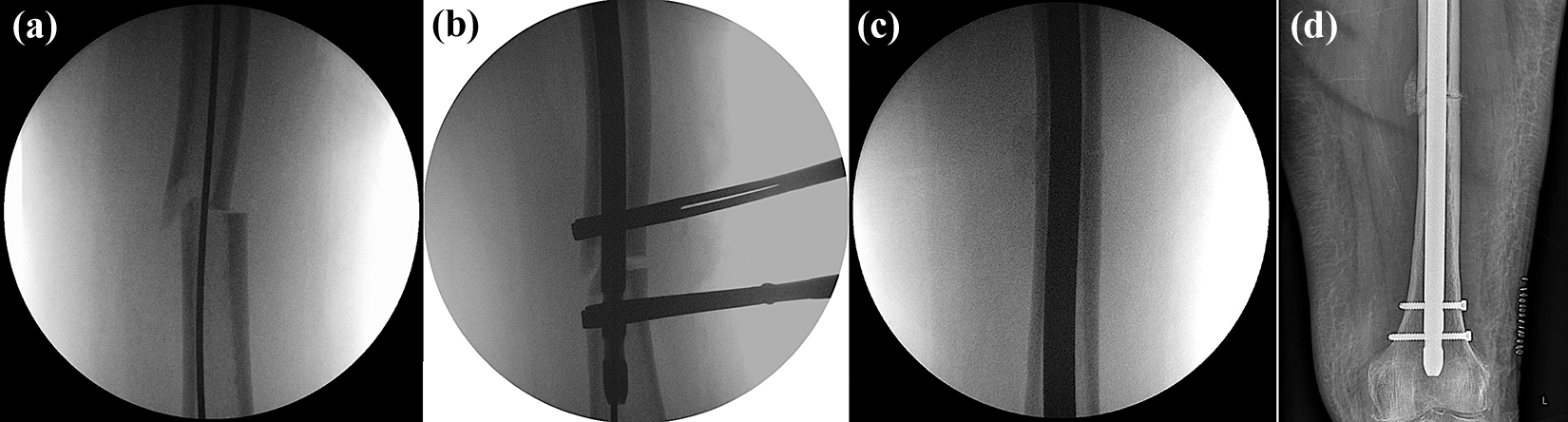
Seventy-four-year-old obese female patient presenting with a low energy atypical femoral shaft fracture after a 5-year history of bisphosphonate use. (a) Intraoperative fluoroscopy demonstrates a guidewire across the fracture site. (b, c) To avoid a varus malreduction, two bone clamps are placed through minimally invasive incisions to reduce the fragments before over-reaming, permitting a large diameter nail to be deployed with minimal fracture gap. (d) Immediate post-operative AP radiograph demonstrates bone grafting that occurs at the fracture site as a result of over-reaming the intramedullary canal.
Our critical steps involve over-reaming of the canal to a diameter 2.5 mm greater than the selected nail diameter. This technique reams the focal intramedullary sclerotic bone that would otherwise deflect the reamers and prevent safe nail entry. Furthermore, the authors suggest that over-reaming by 2.5 mm mechanically grafts the fracture site with skeletal progenitors, which stimulate angiogenesis and bone healing (Figure 1(c) and (d)). 12
For all cases, a Gamma3® long cephalomedullary nail (Stryker®) with 120° neck angle and 1.5 m radius of curvature was used. Static distal locking is always performed with two 5-mm screws to maximise the rigidity of fixation. The implant is composed of a titanium alloy with anodised type II surface treatment. Once the nail is deployed, the traction is released to mitigate any fracture distraction before static locking.
Multidisciplinary management and rehabilitation
Preoperatively, all patients are admitted and rapidly optimised by a multidisciplinary team, involving orthogeriatricians, orthopaedic surgeons and physical and occupational therapists. This includes resuscitation, optimising analgesia, correction of electrolyte imbalances and identifying rehabilitation goals. Bisphosphonates are discontinued and all patients are commenced on teriparatide therapy to promote fracture union and restore bone homeostasis. Post-operatively, the patients are supported to be fully weight bearing as per their pre-injury baseline mobility as early as the first post-operative day. Early mobilisation is well documented and widely accepted to be associated with a shorter hospital stay and improved post-operative outcomes. During subsequent follow-up, all patients undergo a thorough metabolic bone assessment that includes a bone densitometry scan; repeat radiographs and a holistic assessment delivered through the multiprofessional framework. All follow-up intervals are standardised at 8, 12, 24, 36 and 72 weeks with X-rays until union is achieved. Functional assessment includes gait analysis and an assessment of the patient’s home environment. This allows for the adaptation of their residence, such as the installation of handrails, stair lift, provision of mobility aids and washroom alterations.
Main outcome measures
The primary outcome measure was the time to radiological union, which was assessed from standard anteroposterior and lateral radiographs by two of the senior authors and a senior radiologist. Any discrepancies were further reviewed by a third author and final decision reached by consensus. Clinical outcomes and radiographs were evaluated and recorded at each follow-up. Secondary outcomes consisted of the duration of post-operative pain, rate of re-operation and post-operative complications. A retrospective review of case notes was performed to assess for co-morbidities, duration of pre-fracture symptoms, duration of bisphosphonate therapy and length of hospital stay.
Results
Twenty-eight patients were included in the study (27 females and 1 male) with a mean follow-up time of 58.5 weeks (range 36–208 weeks). The mean age was 75.2 years (range 50–99 years). Four of these patients also underwent prophylactic fixation of the contralateral femur though these femora were excluded from this study. The mean duration of bisphosphonate treatment was 7.02 years (range 2.5–15 years). Sixteen (62%) patients experienced prodromal ipsilateral thigh or groin pain prior to admission with a mean duration of 10.5 weeks (range 4 days–1 year).
The mean length of hospital stay was 8.2 days (range 3–15 days).
Ten patients (38.4%) reported post-operative thigh pain, ache or discomfort for a median of 3 weeks (interquartile range 2–8). All patients achieved radiological union by a mean time of 6 months (interquartile range 16–26 weeks, median 20 weeks). There were no reported complications or cases requiring revision surgery at the point of the latest follow-up.
Discussion
Our study reports superior post-operative outcomes with no intraoperative complication, such as iatrogenic fracture, which has a previously reported risk of 29.4%. 13 In addition to our critical steps, we employed well-documented and reproducible methods of anatomical reduction, restoring femoral length and alignment with intramedullary nailing through very small percutaneous incisions. All fractures achieved radiological and clinical union, which we attribute to our specific operative technique and multidisciplinary approach (Figure 2(a) to (d)).
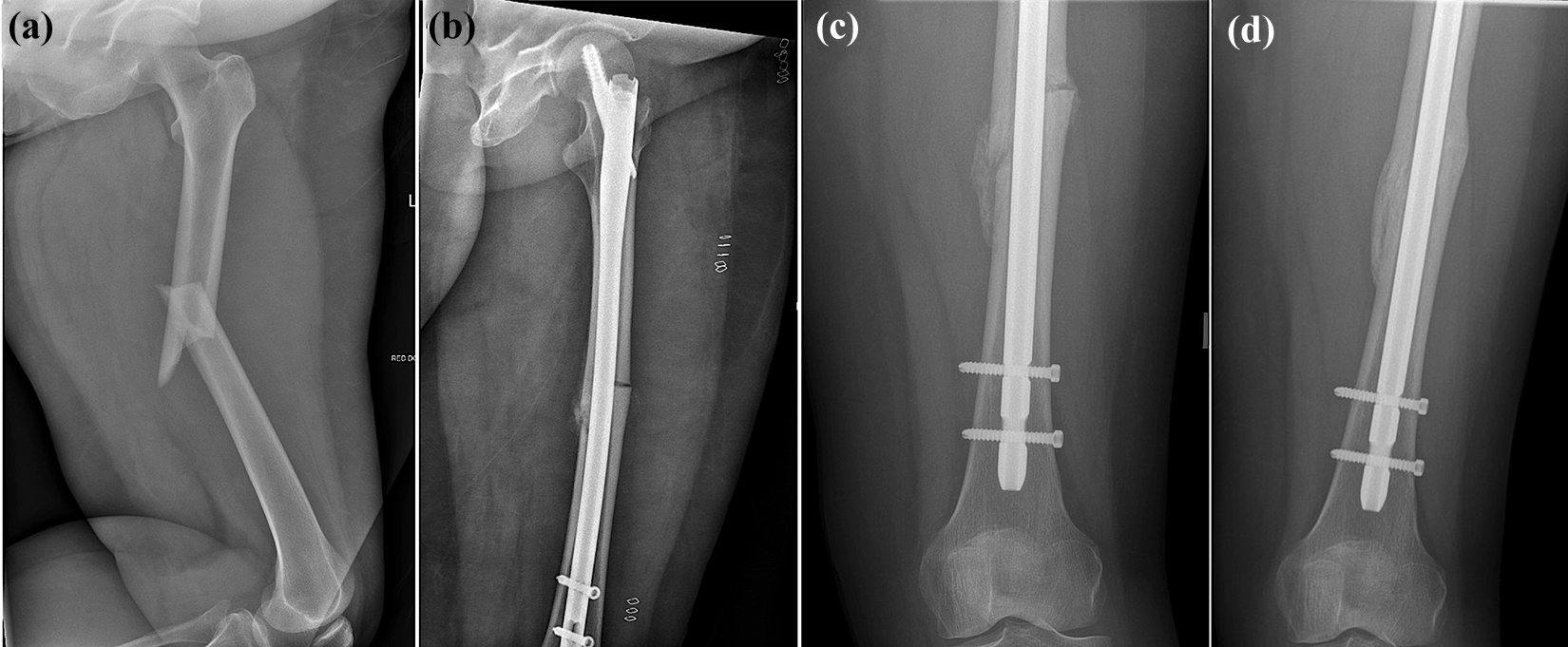
Fifty-eight-year-old female who sustained an atypical femoral fracture 8 years after commencing alendronate. (a) AP radiograph demonstrating a diaphyseal atypical fracture with lateral cortex “beaking” that was treated using our technique of over-reaming and rigid cephalomedullary fixation. (b) Mechanical bone graft can be appreciated at the fracture site. A multidisciplinary approach to rehabilitation and early mobilisation permitted the patient to be discharged on the sixth post-operative day. (c) At 6 weeks, the patient is mobilising at baseline with discomfort and (d) by 4 months, the patient has pain-free radiological union.
There can be a tendency for subtrochanteric fractures to be fixed in a varus malreduction due to the deforming forces of the abductors, therefore, in such cases, a minimally invasive incision can be made at the fracture site to allow a bone lever to assist reduction. These key strategies maintain soft tissue integrity and promote early weight bearing, a shorter post-operative recovery and length of stay.
According to the existing literature, healing time for AFFs has been reported to be between 2 and 31 months with an average of 7.3 months. Between 20.3% and 24% of nailed fractures required revision surgery due to non-union or implant failure. 11 A recent multicentre cohort study reported a median time to union of 7.3 months and a revision rate of 12% at a mean of 11 months. 4 Our study demonstrates a median time to radiological union of 6 months and no cases requiring revision during the mean follow-up time of 14.6 months.
AFFs arise due to strain occurring at the thickened anterolateral, tension side of the cortex. As AFFs are at risk of non-union, it is, therefore, imperative to reduce the fracture gap as much as possible. The same cephalomedullary nailing system was used for all cases, which we believe affords greater rotational stability and rigid fixation for AFFs than a conventional recon nail, while further preventing femoral neck fracture. 14,15 It is well described that patients with AFF experience greater stress concentration over a longer period of time due to slow healing, leading to delayed union and implant failure. 16 To reduce excessive micromotion at the fracture site and maximise fixation rigidity, we opted to always utilise two static distal interlocking locking bolts through the cephalomedullary nail.
A study by Rocha et al. suggested that intramedullary reaming has a multifocal and positive effect on fracture healing. Predominantly, the reaming process grafts the intramedullary fracture site with CD146+ skeletal progenitors. These multipotent cells actively perform ossification and also assist in neurovascular formation. Furthermore, reaming down-signals the local inflammatory state, which enhances the availability and action of the osteogenic and angiogenic growth factors bFGF and PDGF-AB. 12
We believe that our novel step of over-reaming by 2.5 mm allows for greater mechanical bone grafting than the standard accepted reaming technique. We also did not encounter any intraoperative complications, such as cortical penetration, with reamer or nail that can occur due to deflection from pathologically thickened cortical and intramedullary bone. Over-reaming the intramedullary canal can further remove any excessive brittle, focal sclerotic bone, which would otherwise deflect and medialise the nail and could result in a varus malreduction or iatrogenic fracture during entry of a large diameter nail. 17
Osteoporosis-related AFFs are associated with significant morbidity and mortality both in the immediate and long-term post-operative phases. Combined with an ageing population, the diagnosis and management of patients with AFFs are critical. 18,19 The mean age of patients in this study was 75.2 years and the majority had significant co-morbidities. We employed a multidisciplinary approach on admission and at follow-up, which involved a continued, coordinated review by orthogeriatricians and physiotherapists. This enabled rapid optimisation of fitness for surgery, early identification of rehabilitation goals and a return to pre-injury mobility and function. Our mean length of stay was 8.2 days, which is in contrast to 12.5 days, as reported by Davenport et al. 20
All patients had radiographs taken of their contralateral femurs to assess for bilateral disease. Four patients were found to have periosteal thickening and beaking of their lateral femoral cortices with the risk of impending fracture. Although they were asymptomatic from these contralateral lesions, all four patients underwent prophylactic fixation in the same manner. These femora were excluded from this study. It is becoming common practice to investigate the contralateral limb for stress reaction, as the pathology is often bilateral. 11 Prophylactic nailing for the asymptomatic lesion may be warranted as incomplete AFFs invariably progress to complete fracture. 21
Other than those with contraindication, we opted to cease bisphosphonates and initiate teriparatide therapy to re-establish normal bone homeostasis and increase turnover. 9,22 Bone-forming agents, such as teriparatide, have been shown to exert an anabolic effect on unhealed bisphosphonate-related AFFs. There is an increasing body of evidence to suggest that teriparatide after intramedullary nailing can promote faster healing of AFFs and a normalisation of bone turnover markers within 2 years of treatment. 23 –25
Our main limitation in the study was that the sample size was too small for statistical testing though, overall, our surgical techniques and perioperative management were shown to be successful. Despite our study centre being a regional hip fracture trauma unit, the occurrence of low energy AFF is still relatively rare. We also excluded two patients who had undergone intraoperative tension band plating alongside cephalomedullary nailing. These patients experienced prodromal pain for 12 months with significant thickening of the lateral femoral cortex, and thus, a high risk of non-union was anticipated. In line with general orthopaedic principles, this study recommends an early return to mobilisation combined with a holistic and supportive approach to rehabilitation. Though functional outcomes were not quantitatively assessed, the authors suggest that these factors have better overall outcomes for patients rather than to restrict weight bearing post-operatively.
Conclusion
Bisphosphonate-related AFFs are difficult to manage due to the high risk of non-union. We report successful outcomes of improved union rates and function. We attribute these to multidisciplinary care, specific surgical steps, including over-reaming the intramedullary canal by 2.5 mm greater than the nail diameter, rigid static locking of a cephalomedullary nail and the initiation of bone-forming agents. Given that these fractures are rare, our study adds to the growing body evidence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.