
Abstract
We report 2 cases of atypical femoral fracture displacement despite treatment with intramedullary (IM) nailing. Both patients had received more than 3 years of bisphosphonates. One patient had prophylactic fixation of an atypical femur fracture due to intractable pain. The other had undergone nailing previously for a traumatic shaft fracture. The patient then received bisphosphonate later and sustained an atypical fracture with the nail in place. Both femoral nails were slotted, cannulated stainless steel piriformis entry designs. These 2 cases are among the first reported failures of IM fixation in preventing displacement of a bisphosphonate stress fracture. We advice caution when using slotted nails in prophylaxis of atypical femur fractures because of its significantly reduced torsional stiffness compared to modern nonopen sectioned nails.
Keywords
Introduction
Atypical femoral fractures have been suggested to be associated with patients receiving bisphosphonates for more than 3 to 5 years. 1 –7 The etiology of atypical femur fracture is thought to be reduced bone turnover, leading to accumulation of unrepaired microfractures and eventual significant weakening of the bone. 8 The subtrochanteric and diaphyseal areas of the femur are subjected to high tensile load hence most susceptible to fracture after minimal or no trauma.
Patients may present at an early stage before fracture completion and displacement. These patients typically have cortical stress reactions in the femoral subtrochanteric or diaphyseal regions, presenting as lateral cortical beaking and cortical thickening. Some may also have prodromal pain and a “dreaded black line” representing an undisplaced stress fracture. 5,6,9 –12 Pain and the dreaded black line may indicate an increased risk of secondary displacement. Clinical studies have reported favorable results by prophylactically treating these patients with intramedullary (IM) nailing, successfully preventing secondary displacement and alleviating pain. 13 –18 We present 2 cases where an atypical fracture displaced despite previous IM fixation with a slotted stainless steel nail.
Case 1
A 71-year-old lady with a history of surgical menopause was prescribed alendronate for osteoporosis. Despite being on treatment, she sustained a displaced femoral neck fracture 4 years later. She was treated with a hemiarthroplasty. She continued to take the drug for a total duration of 5 years. The patient was maintained on calcium and vitamin D supplements. She was able to ambulate outdoors with a stick (Figure 1).
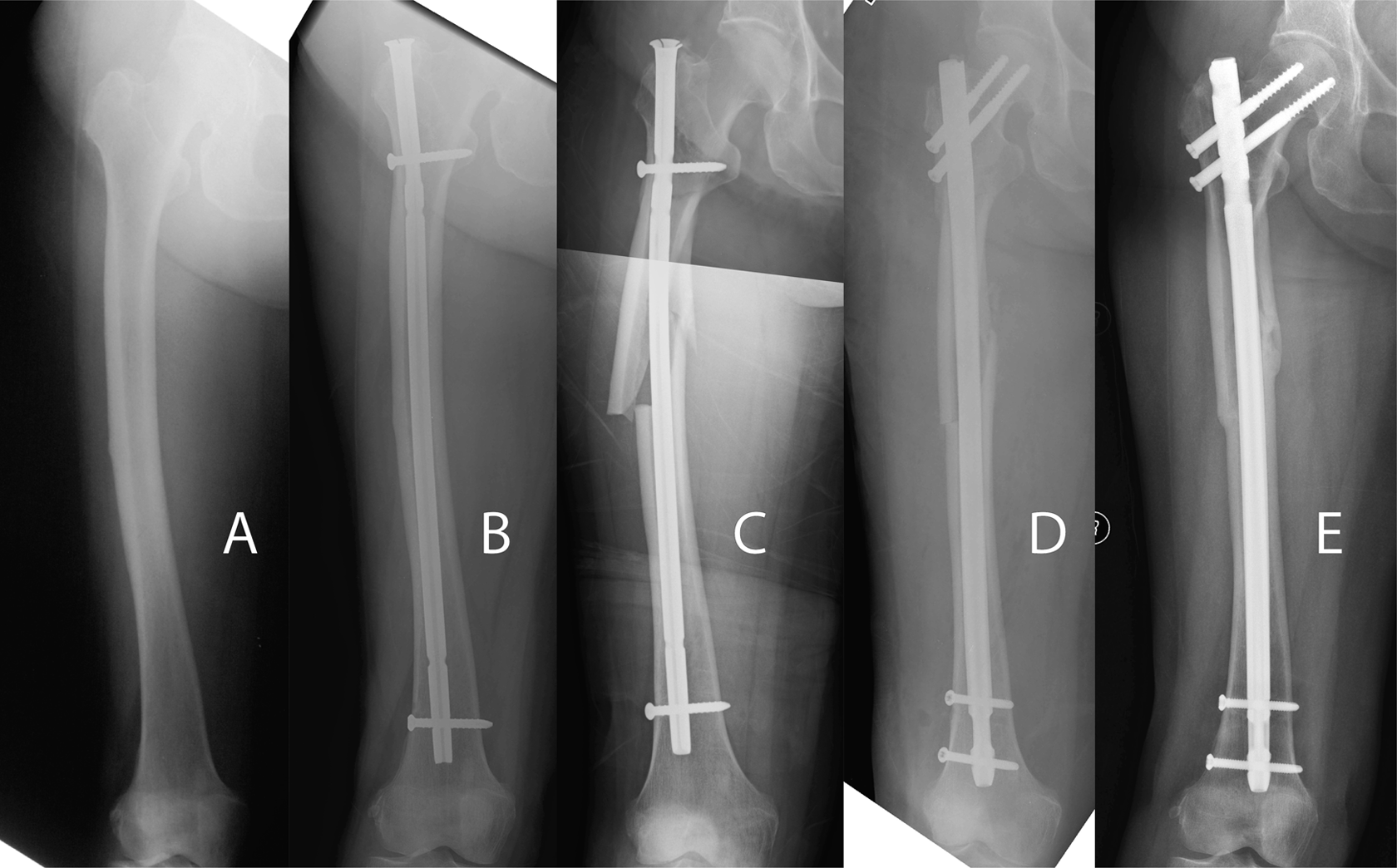
Case 1: A, A 77-year-old lady who previously received 5 years of alendronate presented with thigh pain, with x-ray showing features of an atypical cortical stress reaction at the mid diaphysis. B, Prophylactic fixation with a slotted stainless steel IM nail. C, The atypical fracture failed to heal and a secondary displacement occurred after a fall injury after 13 months. D, Revision with a cephalomedullary nail. E, Healing after 7 months. IM indicates intramedullary.
At the age of 77, around 14 months after stopping alendronate, she experienced right-sided thigh pain that worsened and became debilitating after 2 months. There was no significant pain over the contralateral limb with previous hemiarthroplasty. X-ray revealed cortical “beaking” and thickening over the mid diaphysis of her right femur. There was corresponding local tenderness. The diagnosis was an atypical femur fracture. She underwent prophylactic antegrade IM nail fixation to prevent secondary fracture displacement and to alleviate intractable pain.
Reaming was performed up to 12 mm with the use of a distal IM suction vent. A 10-mm piriformis entry stainless steel slotted nail (Universal Femoral Nail, Synthes, Oberdorf, Switzerland) was inserted with 1 static locking bolt distal and 1 proximal locking bolt in the dynamic position.
The patient recovered uneventfully after operation. She was allowed immediate full-weight–bearing walking. She remained to be on calcium carbonate and multivitamin supplements. Strontium ranelate was started 2 months after surgery. The patient had decreased pain but it was not completely alleviated by the surgery.
The patient then sustained a minor fall injury on level ground 1 year and 3 months after IM nailing. X-ray showed a displaced comminuted fracture of the femur propagating from the original site of the stress fracture despite the nail.
The patient was reoperated with nail exchange to a reamed trochanteric entry nonslotted cannulated titanium femoral nail (A2FN, Synthes, Oberdorf, Switzerland). Open reduction was performed. Reaming was performed to 13.5 mm and a 12-mm nail was used. In all, 2 reconstruction locking bolts were used proximally and 2 static locking bolts were used distally. She was rehabilitated with progressive weight-bearing walking exercise. The fracture united after 4 months and the patient was able to return to her prefracture functional status.
Case 2
A 78-year-old lady presented to the trauma unit 3 years ago when she missed a step while walking downstairs. She sustained an oblique fracture at the distal shaft of her right femur. She had good general health prior to this injury. The fracture was managed by IM nailing. An 11-mm piriformis entry slotted stainless steel nail was used (Universal Femoral Nail, Synthes). Reaming was performed up to 13 mm. In all, 2 proximal and 2 distal interlocking screws were placed at the static positions. The fracture united uneventfully and the patient was put on alendronate. The patient was eventually able to walk unaided with a pain-free lower limb (Figure 2).
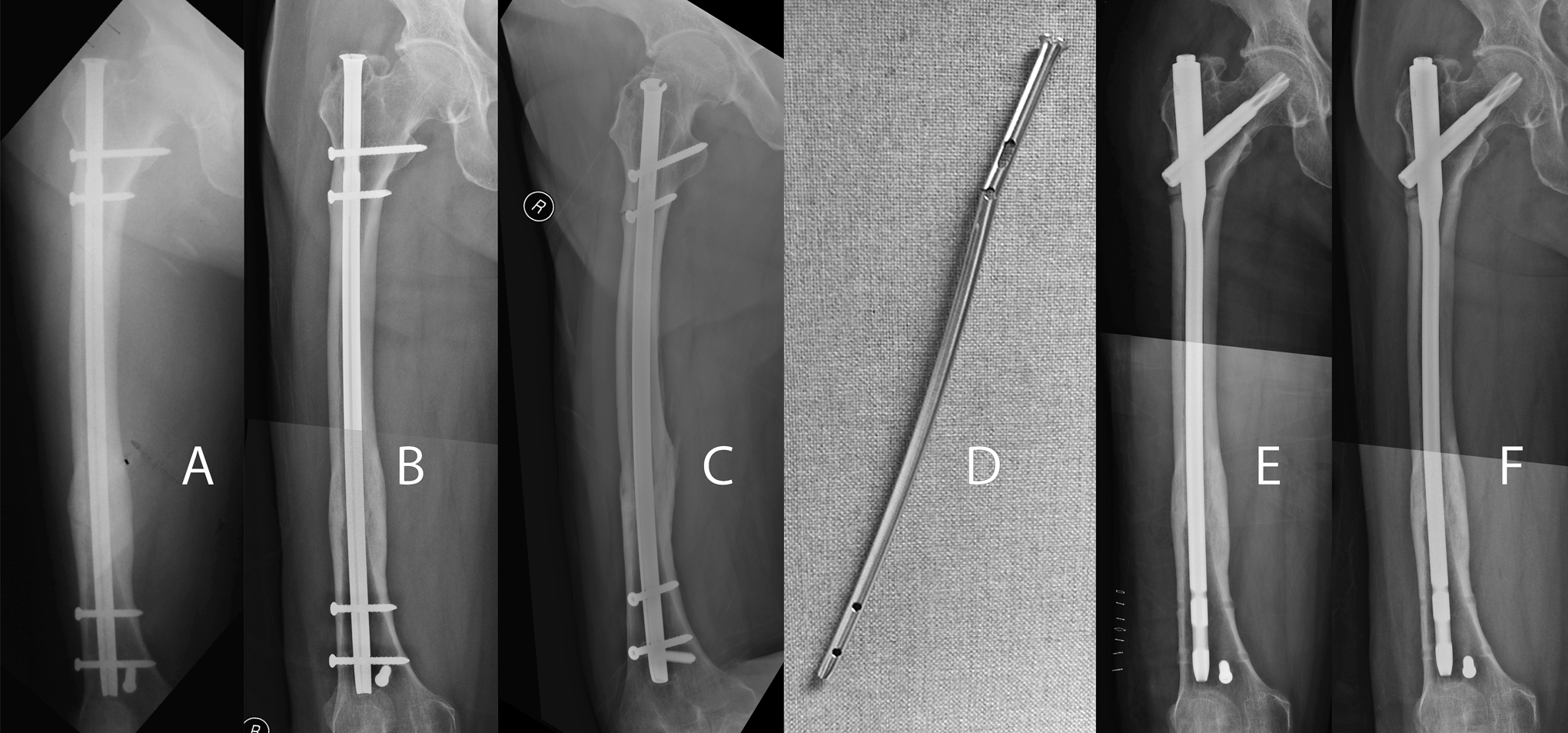
Case 2: A, A 78-year-old lady with previous distal diaphyseal femur fracture treated with IM nailing, with fracture healed 9 months afterward. B, Patient complained of prodromal hip plane with no definite x-ray changes on the anteroposterior view. C, Oblique view showing a subtrochanteric atypical fracture at the locking screw position. D, Retrieval of a broken slotted IM nail. E, Refixation with a cephalomedullary nail. F, The fracture has healed with patient pain free 4 months following revision surgery. IM indicates intramedullary.
Two and a half years after the initial fracture, the patient began noticing increasing pain over the operated hip. The patient continued to ambulate with a walking frame for 4 months.
The patient then had a low-energy fall and was readmitted into hospital. Radiographs on admission showed a displaced subtrochanteric stress fracture with bending of the IM nail. X-ray indicated a stress fracture with beaking and breakage of the lateral cortex occurring at the proximal screw hole.
The patient underwent surgical fixation of the fracture. The implant was exchanged to a long cephalomedullary nail (PFNA, Synthes, Oberdorf, Switzerland). The retrieved IM nail showed fatigue failure at its proximal locking screw hole.
Bisphosphonate therapy was stopped and the patient was rehabilitated with progressive weight-bearing walking exercise. The fracture eventually united on x-ray 4 months following surgery with alleviation of pain.
Discussion
Atypical femur fractures may be difficult to diagnose at an early, undisplaced stage. They may be appreciated by screening the contralateral femur in patients presenting with displaced fractures. The typical features are lateral cortical beaking, diaphyseal cortical thickening, or a dreaded black line with prodromal pain in patients who have been on a few years of bisphosphonates. Judicious use of magnetic resonance imaging and bone scintigraphy can assist diagnosis when x-rays alone are nonconfirmatory.
The recommend treatment is prophylactic surgical stabilization of these stress fractures. The indications for surgery are to prevent secondary fracture displacement and to alleviate prodromal pain. The reported rate of secondary displacement in unoperated cases is thought to be high. Banffy et al 14 reported fracture displacement occurring in 5 of the 6 patients who were not prophylactically stabilized. Ha et al 18 saw secondary displacements in 5 of the 14 femurs and another 5 had to be operated due to intractable pain. Koh et al 9 reported that patients with cortical stress reactions and subsequent fracture displacement were more likely to have pain and a dreaded black line on x-ray. Prophylactic stabilization was reported to be associated with shorter hospital stay 14,16 when compared to treatment after fracture displacement. 19 When there are persistent radiological features and prodromal pain after a drug holiday of 1 to 2 months, prophylactic IM nailing should be strongly advised.
Prophylactic treatment has shown to be generally effective. Ward et al 16 described 14 successful prophylactic fixations with reconstruction nails. Banffy et al 14 treated 6 with cephalomedullary devices. Capeci and Tejwani 15 reported 4 successful antegrade IM nailing as prophylaxis. Das De et al 13 reported success using both IM nails in 2 cases and dynamic condylar screw plates in 2 other cases where the canal was too narrow. Wang et al 17 reported 3 successful prophylactic fixations with nonreconstruction nails. Ha et al 18 reported 5 patients treated with plate or IM nails with similar success. Oh et al 20 reported 20 similar successes with IM nails. From all the reported cases, there were no failures noted.
In our 2 cases, both patients had atypical fracture displacement despite presence of an IM nail. In the first case, the fracture displaced despite antegrade nailing while in the second case fracture developed with the nail in situ. In the literature, there were no other reports of failures of prophylaxis in undisplaced fractures. Many authors have used newer generation solid nails with fixation into the femoral head.
As illustrated by these 2 cases, we call for caution if not total avoidance of slotted nails with bisphosphonate fractures. The torsional stiffness of slotted IM nails is only 2% of the intact femur compared to 13% for a solid nail. 21 We believe it is important to select a more rigid implant that can bear stress throughout an extended period of time for a biologically compromised femur to heal. Our centers have therefore resorted to routine use of cephalomedullary nails.
A bone scintigraphy can be used to confirm delayed union when patient complains of persistent pain despite prophylaxis. Anabolic agents for osteoporosis, such as teriparatide and strontium renelate, increase bone formation and osteoblastic activity. The latter is currently licensed for use in Europe and various other countries but not in the United States. 22,23 Both had early results that may enhance success after surgery in atypical femur fractures.
Extra effort has to be put in when tackling atypical bisphosphonate-related fractures due to the high reported rate of complications. 12 Despite reinforcing on preventive measures such as strict adherence to indications, close monitoring for complications, and cessation of the drug after 3 to 5 years, 1,23,24 it is likely that orthopedic surgeons will still increasingly face such fractures. The surgeon should make a prompt diagnosis, establish a clear understanding with the patient, provide a stable mechanical prophylaxis or fixation, respect the biology of the fracture, and maintain vigilance at follow-up to assure healing.
Footnotes
Authors’ Note
The 2 patients reported were informed that the data concerning the case would be submitted for publication and that each patient agreed to this.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Leung is the speaker for Synthes and has received research support from Synthes. Dr Lau has received research support from Synthes.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.