
Abstract
Introduction:
Surgical site infection (SSI) is associated with increased morbidity and mortality, prolongation on length of hospital stay and cost of community healthcare. In 2010 and 2012, our centre experienced an unexpectedly high rate of SSI in geriatric hip fracture patients with hemiarthroplasty done. A multifaceted intervention programme – ‘bundle approach’ – consisting of preoperative microbiological screening, perioperative measures and postoperative wound care was implemented.
Method:
Preoperative methicillin-resistant Staphylococcus aureus (MRSA) screening was implemented. Intravenous vancomycin was given as prophylactic antibiotic of choice in those patients with positive MRSA screening. All patients will be bathed with chlorhexidine lotion 1 day before operation or on the day of operation. Standardized protocol of surgical site disinfection was implemented: a stringent first stage povidone-iodine disinfection, second stage waterproof extremity draping and sterile plastic sheet wrapping of non-surgical region and third stage ChloraPrep, followed by circumferential iodophor-impregnated plastic adhesive drape (‘Ioban’) covering the hip and thigh region. The surgical wound was dressed with Aquacel adhesive tape after wound closure.
Results:
The total numbers of infected cases were 17 from 2008 to 2012 and 9 from 2013 to 2018 (first quarter). The rates of infection were 7.02% from 2008 to 2012 and 3.16% from 2013 to 2018 (first quarter). There was a statistically significant reduction in the number of infected cases of hemiarthroplasty after the implementation of bundle approach (p = 0.0411).
Discussion:
The bundle approach showed to achieve an effective and sustained decrease in SSI for the geriatric hip fracture patients.
Keywords
Introduction
Surgical site infection (SSI) is one of the most commonly reported nosocomial infections apart from hospital-acquired pneumonia and urinary tract infection. It is associated with increased morbidity and mortality, prolongation of the length of hospital stay and increase in the cost of community healthcare.
Hip fracture is one of the most common and potentially devastating injuries. About 87–96% of hip fracture patients are 65 years of age or older. Geriatric patients have little physiological reserves to SSI and the operation itself. It may lead to uncontrolled sepsis and in the worst case may lead to death of affected individuals. The consequence can be debilitating in cases of operated hip fracture complicated with SSI.
SSI is increasingly seen as a performance indicator of the quality of healthcare. In 2010 and 2012, our unit experienced an unexpectedly high rate of SSI in geriatric hip fracture cases with hemiarthroplasty performed.
The SSI rate of cases with hemiarthroplasty performed in our unit was as high as 7.02% from 2008 to 2012 while the overall SSI rate of orthopaedic operations of all public hospitals under the Hospital Authority of Hong Kong, a statuary organization governing all public hospitals in Hong Kong and covering more than 90% of inpatient care in the territory, was around 1% in 2016. The root causes of increased rate of SSI were investigated. With multiple possible risk factors that can be accountable for the increased rate of infection, the whole clinical pathway of patients who suffered from fractured neck of femur requiring hemiarthroplasty was evaluated. A protocol of multifaceted intervention programme – ‘bundle approach’ – consisting of preoperative microbiological screening, perioperative measures and postoperative wound care was first described by Acklin et al. in 2011. 1 The protocol was implemented in our centre to optimize the treatment processes and to reduce the rate of SSI as soon as possible.
The objective of this study is to review the effectiveness of bundle approach on reducing SSI in geriatric hip fracture patients with hemiarthroplasty.
Methodology
Prior to 2012, there was no standard protocol regarding preoperative skin preparation and surgical draping in our centre. The disinfection of surgical site was performed according to the hospital routine practice with povidone-iodine. Postoperative wound dressing was also done according to chief surgeons’ preference at the time of operation.
Since 2012, we investigated the causes of SSI and developed a bundle approach to its occurrence. Measures were undertaken preoperatively, perioperatively and postoperatively with the aim to reduce the rate of SSI.
Preoperative methicillin-resistant Staphylococcus aureus (MRSA) screening was implemented. Intravenous vancomycin was given as prophylactic antibiotic of choice in those patients with positive MRSA screening result. All patients will be bathed with chlorhexidine lotion 1 day before operation or on the day of operation. To minimize patients’ discomfort during decolonization bath, we employed the use of electric patient lift with adequate manpower during the procedure. Adequate analgesic was ensured in order to optimize patients’ pain control.
Internal guideline was established to standardize perioperative surgical preparations. Choices of prophylactic antibiotic to be administered were standardized with departmental protocol. Intravenous cefazolin would be administered on induction of anaesthesia routinely. Intravenous vancomycin would be given as prophylactic antibiotic to patients with positive preoperative MRSA screening or to those with penicillin allergy. Prophylactic antibiotic was given once on induction of anaesthesia and was continued routinely for three more doses after operation.
Staff education was started on proper technique of perioperative skin disinfection. All staff in operation theatre would undergo proper training of handwashing technique according to standard handwashing method in hospital guideline. All newly recruited orthopaedic surgeons would be educated with proper method of skin disinfection before operation. Unnecessary traffic in operating room should be avoided.
Standardization protocol of surgical site disinfection was implemented: a stringent first stage povidone-iodine disinfection, second stage waterproof extremity draping and sterile plastic sheet wrapping of non-surgical region and third stage ChloraPrep (chlorhexidine gluconate and isopropyl alcohol), followed by circumferential iodophor-impregnated plastic adhesive drape (‘Ioban’) covering the hip and thigh region. The surgical wound was dressed with Aquacel adhesive tape after wound closure. The surgical site disinfection procedure is shown in Figures 1 –8.
First stage povidone-iodine disinfection.
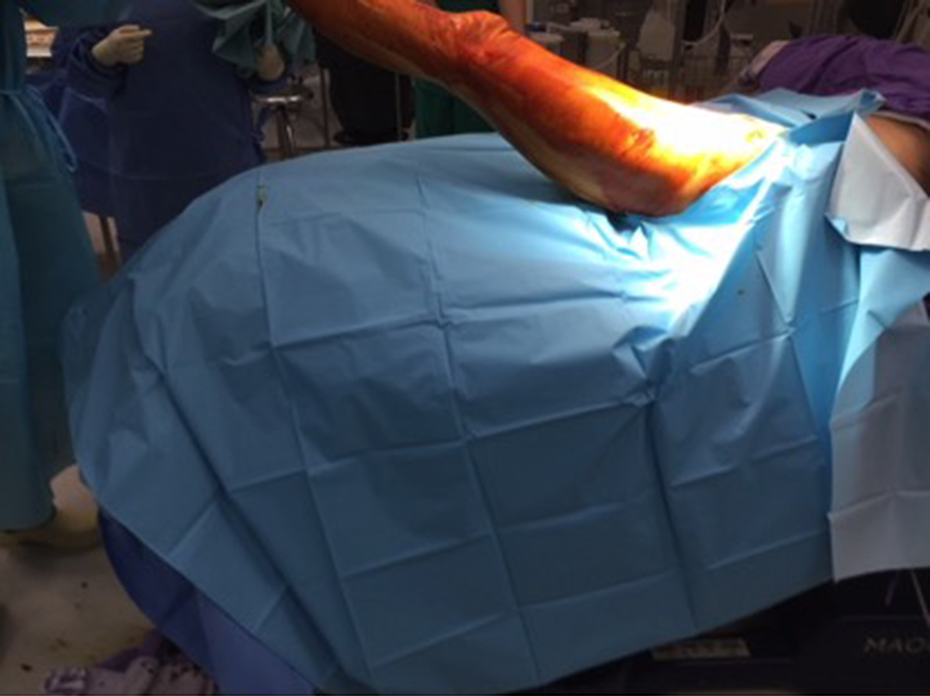
Waterproof extremity draping and sterile plastic sheet wrapping of non-surgical region (1).
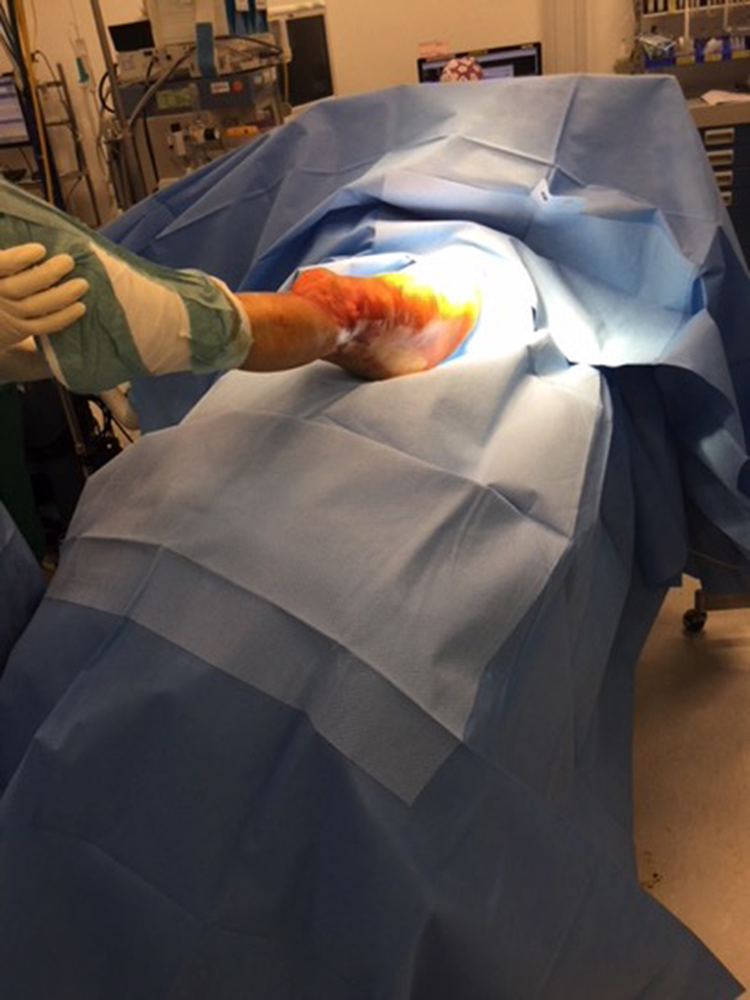
Waterproof extremity draping and sterile plastic sheet wrapping of non-surgical region (2).

ChloraPrep (chlorhexidine gluconate and isopropyl alcohol) disinfection.

Circumferential iodophor-impregnated plastic adhesive drape (‘Ioban’) covering the hip and thigh region (1).

Circumferential iodophor-impregnated plastic adhesive drape (‘Ioban’) covering the hip and thigh region (2).

Circumferential iodophor-impregnated plastic adhesive drape (‘Ioban’) covering the hip and thigh region (3).

Aquacel adhesive tape after wound closure.
All cases of geriatric hip fracture (age >65 years) with hemiarthroplasty from 2008 to 2018 (first quarter) (n = 527) performed at our centre were reviewed. Cases with different modes of hemiarthroplasty including Austin Moore hemiarthroplasty, monopolar and bipolar hemiarthroplasty with cemented or cementless femoral stem were included in the study. In the cases of hemiarthroplasty with cementation, antibiotic-loaded cement was used. The cases complicated with SSI were identified with reference to the database of the hospital infection control team.
The rate of SSI was measured as an outcome indicator. The rate of SSI after the implementation of bundle approach (2013–2018 (first quarter)) was compared with that before the implementation (2008–2012).
Most cases would be transferred to rehabilitation hospital where regular wound assessment and review would be done. All cases would be assessed at least once in the period of 6 months postoperatively at our specialist outpatient clinic.
SSI was categorized according to Centers for Disease Control and Prevention guideline into superficial and deep infection. All infected cases were treated with intravenous antibiotic according to bacterial sensitivity result. Selected cases of superficial infection were treated with surgical debridement if antibiotic treatment failed. All cases with deep infection were treated with removal of implant and surgical debridement.
Results
From 2008 to 2018 (first quarter), a total of 527 cases underwent hemiarthroplasty, in which 242 cases were performed from 2008 to 2012 and 285 cases were performed from 2013 to 2018 (first quarter).
Average operative time was 87 min for the 2008–2012 group while that for the 2013–2018 group (first quarter) was 72 min. The difference was statistically insignificant (p = 0.588).
The total number of infected cases was 17 from 2008 to 2012 and 9 from 2013 to 2018 (first quarter). The rate of infection was 7.02% from 2008 to 2012 and 3.16% from 2013 to 2018 (first quarter). Of the infected cases from 2008 to 2012, nine were cases of superficial infection and eight were cases of deep infection. The rate of superficial infection for the 2008–2012 group is 3.72% while the rate of deep infection is 3.31%. There were five cases of superficial infection and four cases of deep infection in the 2013–2018 patient group. The rate of superficial infection in this group is 1.75% while the rate of deep infection is 1.40%. The number of infected cases and the rate of infection of both groups are shown in Table 1.
Rate and number of cases of hemiarthroplasty with infection.

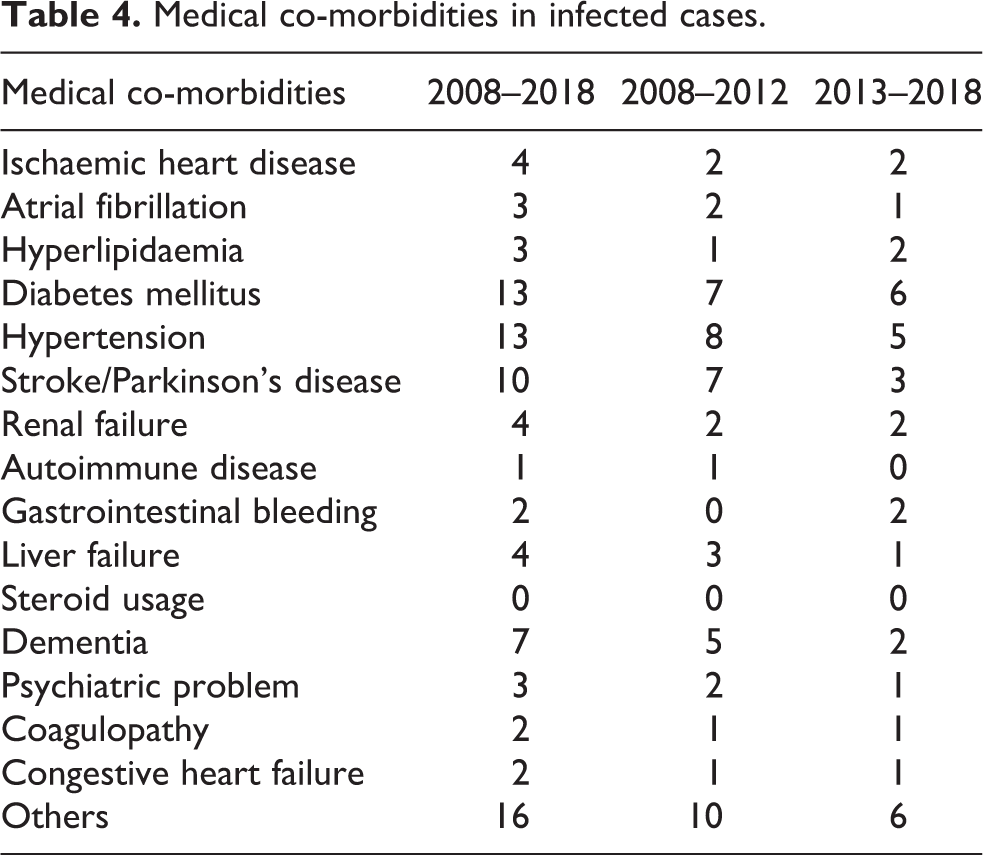
There was a statistically significant reduction in the number of infected cases of hemiarthroplasty after the implementation of bundle approach (p = 0.0411 by χ 2 test) as shown in Table 2. The majority of the cases of hemiarthroplasty complicated with infection were associated with multiple co-morbidities. Diabetes mellitus (DM) and hypertension were the most common medical co-morbidities involved. The most common organism found in positive culture in this study is S. aureus. Of all the infected cases, 12 were found to yield S. aureus in culture result, while the second most common pathogen was Pseudomonas species. The responsible pathogens and medical co-morbidities of both groups are summarized in Table 3 and 4 respectively.
χ 2 test for rate of infection between two groups.

a First quarter in 2018 included.
Summary of pathogens yielded in tissue/wound swab culture result.
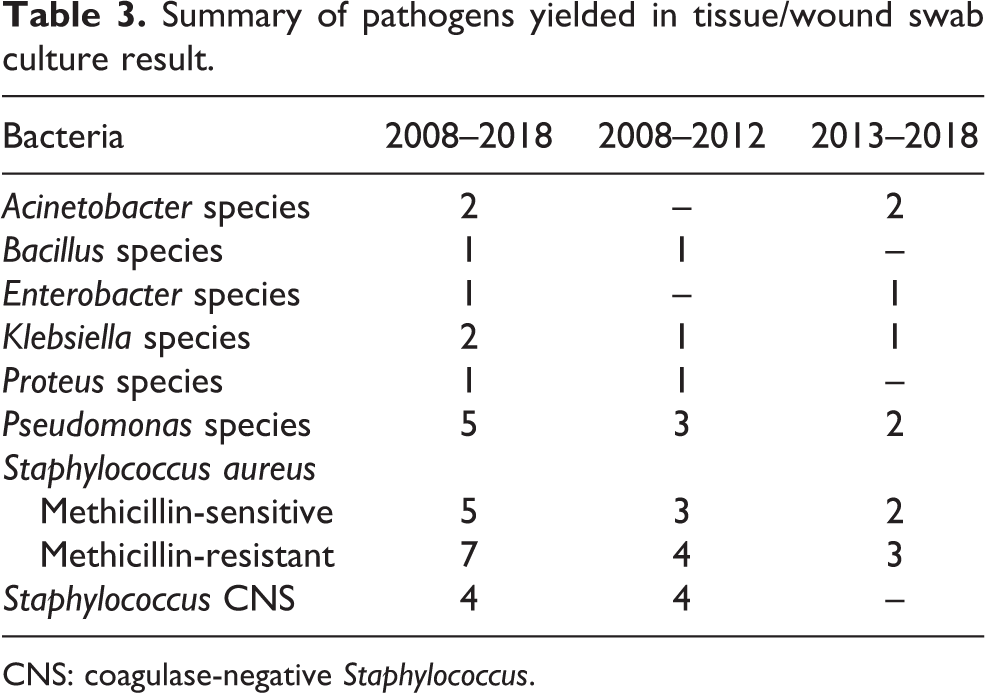
CNS: coagulase-negative Staphylococcus.
Medical co-morbidities in infected cases.
All patients diagnosed with superficial infection were treated with antibiotics and 17.7% of them required multiple surgical debridement. For patients with deep infection, 82.4% of them were initially treated with surgical debridement, however, all of them required removal of implant at the end.
Discussion
Every orthopaedic surgeon has his own approach to minimize the occurrence of SSI. Bundle approach provides a standardized approach to tackle the problems that may lead to increased risk of infection preoperatively, perioperatively and postoperatively. 2 –4
Rationale of MRSA screening and vancomycin prophylaxis
According to our centre experience, the most common pathogen leading to SSI in patients who underwent hemiarthroplasty is S. aureus. S. aureus is a common but yet a pathogen able to cause a diverse spectrum of disease from asymptomatic colonization to life-threatening infection. The blooming emergence of antibiotic resistance of S. aureus was found in recent epidemiological study. 5 MRSA was classically found in clinical setting (e.g. hospital ward and nursing home), however, an increased prevalence was found in community acquired infection. 6,7 MRSA is becoming a major problem in orthopaedic surgery as it may affect the risk of SSI but yet routine culture and sensitivity screening may not be available during preoperative period for administration of appropriate choice of antibiotic.
Altered penicillin-binding protein (PBP2a) encoded by externally acquired mec DNA is accountable for the S. aureus resistance to β-lactams. It facilitates cell wall formation and bacterial growth at the level of β-lactams that are normally inhibitory to original PBP. 7
In our protocol, vancomycin would be used as antibiotic of choice if preoperative MRSA screening was positive. Vancomycin acts on C-terminal end of late peptidoglycan precursors and inhibits cell wall formation in gram-positive bacteria. 8
Traditionally, first- or second-generation cephalosporin is used as prophylactic antibiotic of choice in surgical setting. Vancomycin has also been recommended as prophylactic agent in patients with penicillin allergy. 9 –11
It was concluded in two systemic reviews that cephalosporins are as effective as vancomycin for the prevention of SSIs. 12,13 In these studies, the rate of SSIs in patients receiving antibiotic prophylaxis with a glycopeptide (either vancomycin or teicoplanin) was compared with that in patients receiving a β-lactam agent. However, most studies included in these two reviews were conducted more than a decade ago and they may not be able to represent the current situation given the change in prevalence of resistant strand of S. aureus. It was also suggested by some authors that vancomycin should be used as surgical prophylaxis when an institution has a high prevalence of MRSA, but there was no definite consensus over the definition of high MRSA prevalence. 14,15 Elliott et al. suggested the use of vancomycin as prophylactic antibiotic when the rate of MRSA SSIs was ≤0.15% and the rate of non-MRSA SSIs was ≥0.1% or when the rate of MRSA infections was ≤0.20% and the rate of other infections was ≥0.2%. Combination therapy (e.g. vancomycin plus a cephalosporin) was suggested when the rate of MRSA SSIs was ≥0.25% and the rate of non-MRSA SSIs was ≥0.2%. 16
Rationale of decolonization programme
Rao et al. concluded in his study of preoperative decolonization programme that preoperative S. aureus screening combined with intranasal mupirocin and chlorhexidine bath is effective in reducing SSI caused by S. aureus in patients undergoing total joint arthroplasty. In their study, they yielded zero case of SSI in the treatment group of 164 patients while the rate of SSI in the control group as 3.5% (12 infected cases in 345 patients, p = 0.016) with 1-year follow-up. 17
A randomized control trial by Wendt et al. studied the effect of chlorhexidine body wash in eradicating MRSA colonization. They found significant reduction in MRSA colonization at groin area between the chlorhexidine body washing and the placebo group. However, they found no significant reduction in MRSA colonization at other areas. They concluded that whole body washing can reduce MRSA skin colonization but extended eradication measures were needed if complete eradication deemed necessary. 18
In our bundle approach protocol, intranasal mupirocin was not included and S. aureus screening result is for the guidance of choice of prophylactic antibiotic. Chlorhexidine body wash was routinely done in all patients who were to undergo hemiarthroplasty. From the literature review, it may be beneficial if the application of intranasal mupirocin on S. aureus carrier was included in our protocol of bundle approach for cases with positive S. aureus screening. There was also a need for review of our current protocol concerning the selection criteria of patient for chlorhexidine body wash in order to optimize manpower utilization and cost-effectiveness.
Rationale of two-staged skin preparation
We used standard two-staged skin preparation technique in this protocol: use of first stage aqueous-based iodophors (povidone-iodine) skin disinfection, followed by second stage alcohol-based chlorhexidine.
Free iodine released from aqueous-based iodophors acts by destroying microbial DNA. It has good antimicrobial coverage to multiple pathogens especially gram-positive bacteria. Povidone-iodine has intermediate rapidity of action and its activity is limited by length of contact time. The use of povidone-iodine at first stage skin preparation allows appropriate length of exposure time for its action to be carried out.
Alcohol-based chlorhexidine acts by disrupting bacteria cell membrane. It improves antimicrobial coverage to gram-negative bacteria, mycobacterium and fungus. The onset of its action is rapid and its profile is suitable for second stage skin disinfection.
Alcohol-based iodophors are now also available in market. The advantages of this type of solution are the short dry time of a minimum of 3 min on skin and the formation of a waterproof film on skin that maintained its antimicrobial action for up to 48 h. Due to the waterproof nature of this protective layer, the antimicrobial activity of the solution can be sustained at a relatively-higher extent compared to other preparation of disinfectant during the course of operation. Study also showed that DuraPrep (iodine povacrylex (0.7% available iodine) and isopropyl alcohol, 74%) could lead to sixfold bacterial log reduction in 1 min of contact when compared to aqueous iodophor application. 19,20
The efficacy of three different surgical skin preparation solutions, DuraPrep (0.7% iodine and 74% isopropyl alcohol), Techni-Care (3.0% chloroxylenol), and ChloraPrep (2% chlorhexidine gluconate and 70% isopropyl alcohol), in eliminating potential bacterial pathogens from the foot and ankle in 125 patients was studied in a prospective study by Ostrander et al. 21 Quantitative culture samples were taken from anterior tibia, hallux and toe site after skin preparation and draping. Of the three study solutions, disinfection with ChloraPrep showed a statistically lower positive culture rate at the hallux and toe site when compared to skin preparation with the other two types of solution.
Effect of DM on SSI
Diabetes is a known risk factor of SSI in total arthroplasty. The actual reason of diabetes causing increased rate of SSI is not clear. According to a meta-analysis by Everhart et al., diabetes is an independent risk factor of SSI irrespective of the blood glucose level at times of surgery. 22 The result may suggest the role of diabetes in SSI may go well beyond its effect of increasing blood glucose level during the perioperative period. The exact mechanism of diabetes in increasing the rate of SSI is not clear. Possible effects of diabetes on white blood cell function and vascular status may contribute to diabetic effect of increased SSI. Few studies have assessed the relationship between severity of diabetes and the rate of SSI and concluded that more effort is needed to improve the surgical outcome of diabetes patients.
One of the limitations of our study was the failure to accurately correlate the effect of diabetes on SSI and to eliminate its effect on determining efficacy of bundle approach. On tracing of the medical record or documentation for patients with diagnosis of certain medical conditions such as diabetes, often we were unable to trace a complete and detailed record for the disease control. This also applied while we were investigating other co-morbidities of the patient. There were often no detailed records of the diagnostic criteria, time of diagnosis and the severity of disease for different conditions. We acknowledged this limitation and suggested that closer collaboration between orthopaedic surgeons and geriatricians might help to improve this situation leading to better interdisciplinary communication and patient care.
Limitation of bundle approach and its application
Part of our bundle approach involved measures employed to reduce possible MRSA infection. We found that there was a reduction in SSI rate by MRSA after its implementation (from 1.65% to 1.05%). However, this difference is statistically insignificant (p = 0.55). As for preoperative decolonization bath, it is a possible effective practice for reducing the load of bacteria skin flora not only limited to MRSA and thence possibly contributed to the reduced overall SSI rate. However, the involved MRSA screening and the measures followed including the change in choice of prophylactic antibiotic may lead to unnecessary waste of resources and delay in surgical timing.
The reason why our centre have the capacity to perform MRSA screening preoperatively was due to our undesirable but unavoidable long waiting queue for operation. Due to the service limitation of our hospital, our unit did not have emergency operative session but tight elective lists in our operative theatre prior to 2018. All geriatric patients admitted with hip fracture would be put to elective operative sessions which were available only during weekdays. From the year 2008 to 2017, the average waiting time for operation was around 7–8 days (7.47 days from 2008 to 2012, 7.91 days from 2013 to 2017) while MRSA screening of our centre usually took 2–3 days to complete. One of the internationally accepted standards of managing geriatric hip fractures is early operation within 48 h from admission. In other centres where emergency operative sessions were available or centres with shorter waiting queue for operation, earlier operation would still be the recommended standard management of choice as it was proven to be effective in reducing both short-term and long-term mortality and morbidity of Hong Kong Chinese elderly patients. 23
Our study involved only a relatively small study population to determine the efficacy of bundle approach focusing on its effect on SSI. Centres with a short waiting time for geriatric hip fracture operation might need to face the dilemma of possible delay of operation and the related complications while implementing its measures. Further studies of a larger study scale with a longer follow-up would be necessary to determine whether such delay in operation was worthy.
Conclusion
According to our centre’s experience, by practicing the standardized bundle approach, we can reduce the risk of SSI in our patients who underwent hemiarthroplasty.
The same principle may be applied to patients who underwent other operation apart from hemiarthroplasty. However, further studies need to be continued for adequate power for formal analysis of feasibility.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval
Ethics approval was obtained from the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (CREC number: 2018.577).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.