
Abstract
Background:
Total knee arthroplasty is a common procedure for treatment of various non-infective arthritis. This study reviewed total knee arthroplasty cases up to 10 years of follow-up for the survival rate, reasons of revision and associated perioperative risk factors for revision.
Methods:
All cases to total knee arthroplasty performed in a single centre in the years 2007 and 2008 were reviewed. A total of 227 cases of total knee arthroplasty were performed during the 2-year period, with 156 cases followed up to 10 years. Perioperative information, follow-up information and information of possible complications were obtained.
Results:
The survival rate of total knee arthroplasty in this study is 98.2% at 5 years and 94.2% at 10 years of follow-up. The early post-operative complication rate was low, and majority of cases had improvement of function at 1 year after the operation. Early post-operative infection rate was low at 0.4%, and overall infection up to 10 years of follow-up was also low at 4.4%. Ten cases had undergone revision of arthroplasty by 10 years after operation.
Conclusion:
The survival rate of total knee replacement was high. The revision rate and infection rates were low up to 10 years of follow-up. The most common reasons of revision arthroplasty were infection and aseptic loosening. Cases which required revision arthroplasty had significantly longer operative duration compared with cases without revision at 10 years of follow-up (p = 0.01).
Keywords
Introduction
Total knee arthroplasty is a procedure of growing prevalence across the world. 1 –3 Total knee arthroplasty has been a treatment option for conditions including primary osteoarthritis and arthritis secondary to inflammatory disease, post-traumatic and joint deformity. In view of continually ageing population, 4 the demand for knee arthroplasty is expected to continue to grow. Life expectancy meanwhile had also constantly lengthened. 4 It is essential therefore for knee arthroplasty to achieve a low complication rate and sufficient longevity. Most midterm and long-term literature had reported good long-term survival and positive clinical outcome. 5 –8 However, there are still concerning conditions affecting survival of knee arthroplasty, mainly infection and aseptic loosening. 9 –11 The other concerns included persistent pain, malalignment, wear and lack of satisfaction. 11 –13 Various measures had been implemented or advocated with the aim to reduce occurrence of such problems. 13 These involve preoperative assessment of knee function, mental and physical health, 14 intraoperative guidance technology, 15 identifying and modifying risk factors of infection 16,17 and preventive measures against infective organism. 18 In this study, we reviewed total knee arthroplasty at the author’s centre, the Pamela Youde Nethersole Eastern Hospital (PYNEH), at 10 years of follow-up for the survival rate, post-operation function, complications like infection and aseptic loosening, and correlation to preoperative risk factors for complications and outcomes.
Methods
Data collection was first obtained utilising the Clinical Data Analysis and Reporting System (CDARS) of the Hong Kong Hospital Authority. Inpatient episode-based search for all cases with the operative procedure criteria of ‘knee arthroplasty’ performed in the author’s centre, the PYNEH, from January 2007 to December 2008. Unicompartment knee arthroplasty, excisional arthroplasty and revision knee arthroplasty were excluded.
Information obtained includes patient demographics, age, gender, radiographs, blood test results, microbiological laboratory test results and operative record. Clinical notes were reviewed for information of the initial knee arthroplasty, previous operations, indication of surgery, preoperative risk factors, co-morbidity, early post-operative complications, function at 1 year after operation, duration of follow-up, survival rate and indication of revision if present.
Statistical analysis was performed using Prism version 8.0 by GraphPad Software, Inc. All cases of knee arthroplasty retrieved were used for analysis of early post-operative outcomes, preoperative indications and survival analysis. Cases lost to follow-up were excluded for endpoint analysis of revision and infection at 10 years. Data for continuous values were described by means, standard deviations and range. Difference between groups were analysed with t-test. Data of categorical values were described in absolute and relative frequencies. Categorical values were analysed with Fisher’s exact test. Survival analysis was performed using log-rank (Mantel–Cox) test and Gehan–Breslow–Wilcoxon test. Statistical significance was deemed present with p value ≤0.05.
A total of 227 procedures of total knee arthroplasty were performed in 212 patients at the author’s centre from January 2007 to December 2008. Fifteen patients had bilateral sequential total knee arthroplasty within that period of time. One hundred and fifty-six cases had been followed up till 10 years after the operation. Seventy-one cases had lost to follow-up: 30 cases had passed away, 10 cases defaulted follow-up, 3 cases referred out and 28 cases lost to follow-up for unknown reasons. Mean age at operation for all cases was 69.6 years (SD 8.3, range 31–87). Cases lost to follow-up had significantly older mean age of 73.1 years (SD 6.5, range 55–87) compared with cases with 10-year follow-up (67.9 years, SD 8.5, range 31–85), or all the cases combined. There were more females with knee arthroplasty performed with female to male ratio of 177:50 (Table 1).
Demographics.
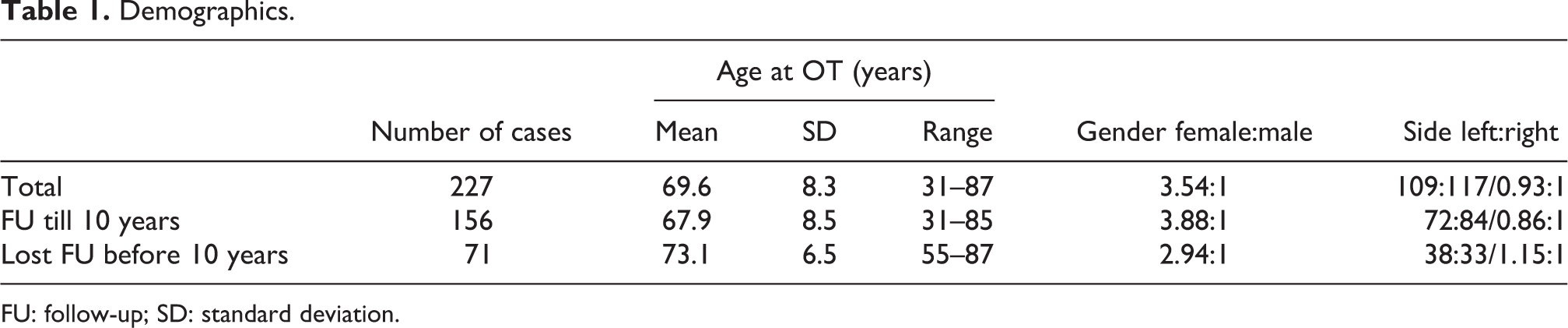
FU: follow-up; SD: standard deviation.
For indication of operation, a large majority was primary osteoarthritis, with rheumatoid arthritis, osteoarthritis secondary to trauma, malalignment or progressive osteoarthritis after previous corrective osteotomy. Various brands and models of implants were used. Three cases had constrained implants while all the others were posterior-stabilised implants. Four cases had mobile-bearing tibial insert, while all others were fixed-bearings.
Results
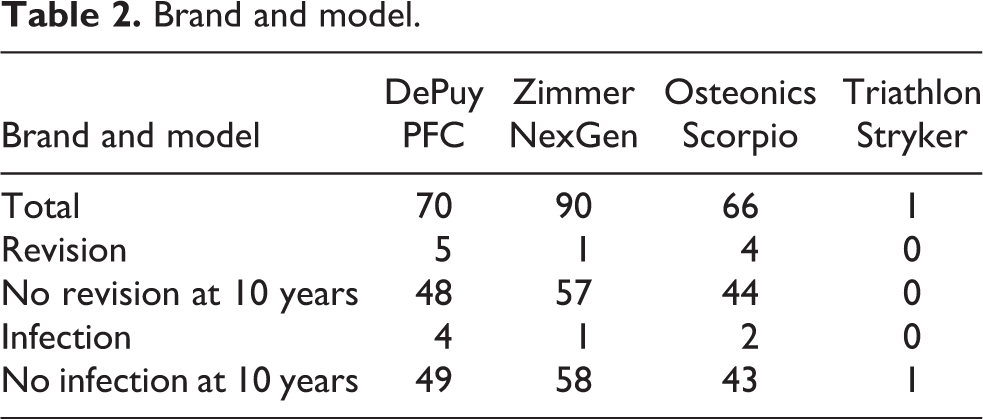
Survival analysis showed that the survival rate for all cases was 98.2% at 5 years and 94.2% at 10 years (Figure 1). Comparison between the three major brand models had not shown statistical significance (Table 2).
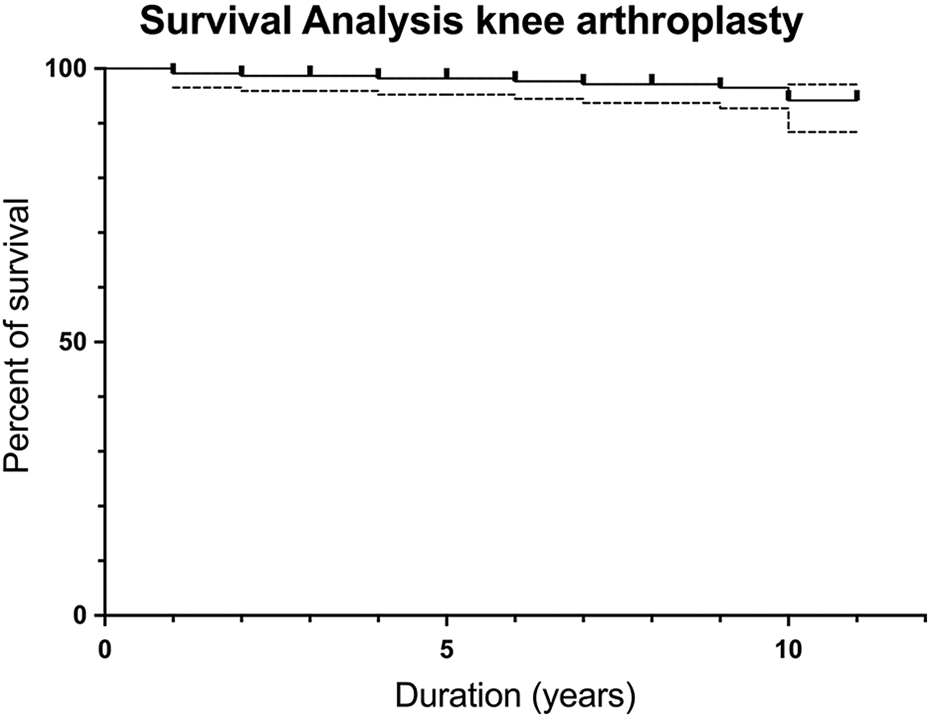
Survival curve.
Brand and model.
Incidence of intraoperative complications was low. Intraoperative complications included intraoperative fractures (three cases, 1.3%), and none had nerve or vascular injury. Early post-operative complications rate was low, these including deep vein thrombosis (seven cases, 3.1%), stiffness (two cases, 0.9%), malalignment (one case, 0.4%), early post-operative deep infection (one case 0.4%) and superficial wound dehiscence (one case, 0.4%). The case of early post-operative deep infection required revision at 2 months after initial operation, and the case of superficial wound dehiscence underwent debridement operation. None of the other cases with intraoperative or early post-operative complications had arthroplasty revisions.
On follow-up at 1 year after operation, 28.2% (64 cases) had a decrease in usage of walking aid, 68.7% (156 cases) had similar usage of walking aid and 3.1% (7 cases) had increased usage of walking aids. The improvement in knee range of motion was median of 10°, and less than 25% of cases had a reduction in range of motion (Figure 2).
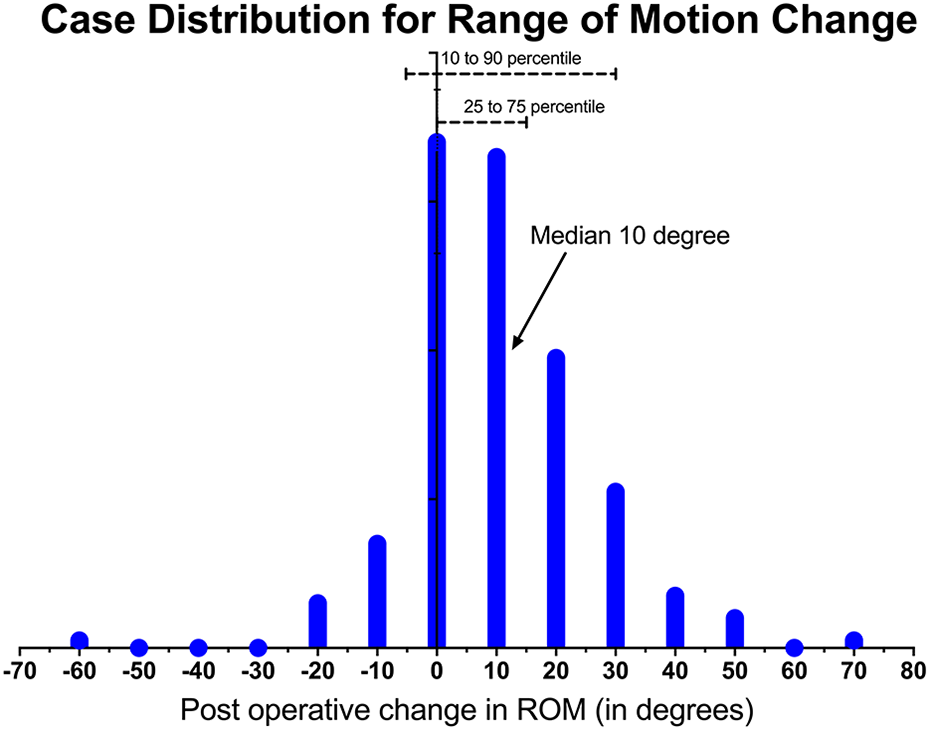
Range of motion change post-operation.
By the time of 10 years of follow-up, an overall total of 10 cases of knee arthroplasty had been revised. This study reference ‘Revision’ as cases with either single-stage revision, multiple-stage revision and removal of components with placement of antibiotic-load cement spacers. Cases with exchange of insert without removal of other components were excluded from the term ‘Revision’. Reasons for revision were as follows: infection (five cases, 50%), aseptic loosening (three cases, 30%) and traumatic loosening (two cases, 20%, loosening noted only after knee injury, not documented in previous follow-up X-ray).
A total of seven cases of arthroplasty had suffered from infection (Figure 3). Two of the cases had early infections. One case of early post-operative deep infection required revision at 2 months after initial operation. The other case of early superficial wound infection with dehiscence underwent debridement operation. By 10 years of follow-up after the operation, four cases had suffered from acute haematogenous infection (2.6%), and one case (0.6%) had a late chronic infection. Three cases of acute haematogenous infection and the one case of late chronic infection had undergone staged revision. One case of acute haematogenous infection had undergone operative debridement and exchange of polyethylene insert.
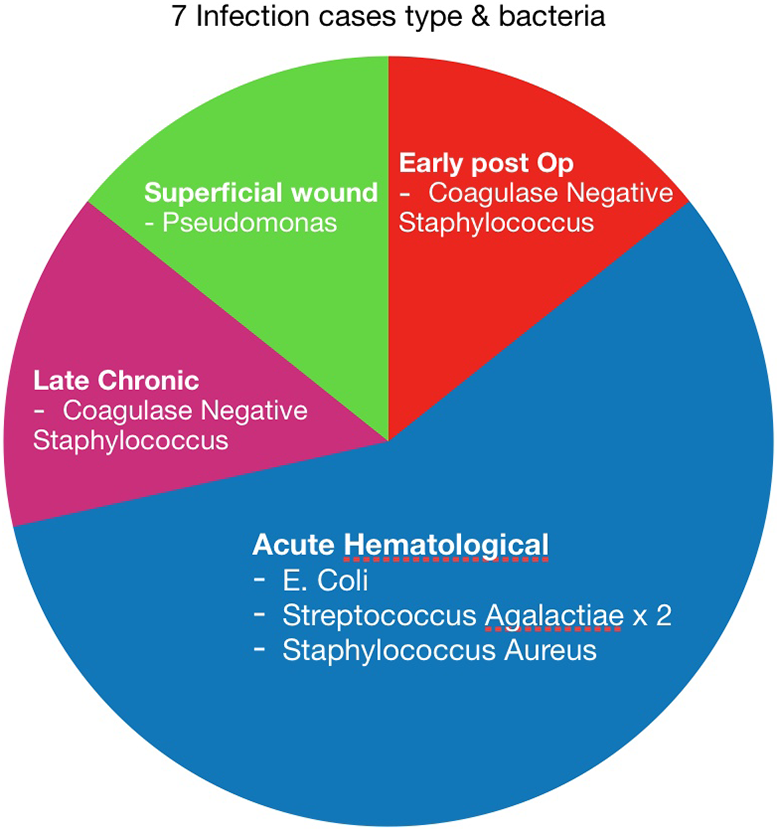
Knee arthroplasty infection cases.
Regarding other complications at 10 years of follow-up, one case (0.4%) had patella clunk which was treated with arthroscopic debridement, and another one case (0.4%) had peri-prosthetic fracture treated without revision of the arthroplasty.
Analysis of risk factors for revision and infection
Operative duration of initial arthroplasty which had subsequent revision (mean 115.7 ± 39.2 mins) was significantly longer than cases without subsequent revision (mean 97.4 ± 20 mins) with p = 0.01 t-test. Operative duration for cases with subsequent revision due to infection (117.6 ± 50.4 mins) was also significantly longer than cases without subsequent revision (p = 0.04). While cases with subsequent revision not for reason of infection had operative duration (113.8 ± 30.2 mins) just short of significance compared with cases without subsequent revision (p = 0.08).
Operative duration of initial arthroplasty of subsequent infection (without or without revision) had mean duration of 113.9 ± 42.6 mins, when compared to all cases without infection at 10 years (mean 97.2 ± 20.3 mins), the difference was just barely short of statistical significance (p = 0.054) (Table 3).
Operative duration.

FU: follow-up.
Although 12.5% of cases with post-operative blood transfusion had infection, compared with 2.99% of cases without transfusion, this difference was just short of statistical significance (p = 0.07 with Fisher’s exact test). Post-operative drop in serum haemoglobin level, meanwhile, had not been shown to affect infection or revision rate.
Regarding demographics, no statistical significance was demonstrated from age difference and gender, for the risk of infection or revision at 10 years of follow-up.
With regard to preoperative risk, no statistical significance was demonstrated between various operative indications (osteoarthritis, rheumatoid arthritis, osteoarthritis with prior osteotomy and post-traumatic osteoarthritis) for revision or infection up to 10 years of follow-up. Although 14.3% of infection cases had rheumatoid arthritis, compared with 4.6% of non-infected cases, statistical significance could not be demonstrated in this series (p = 0.28). No statistical significance of increase risk for infection or revision was demonstrated in presence of diabetes, other orthopaedic problem, and usage of steroids (Table 4).
Risk factor analysis.
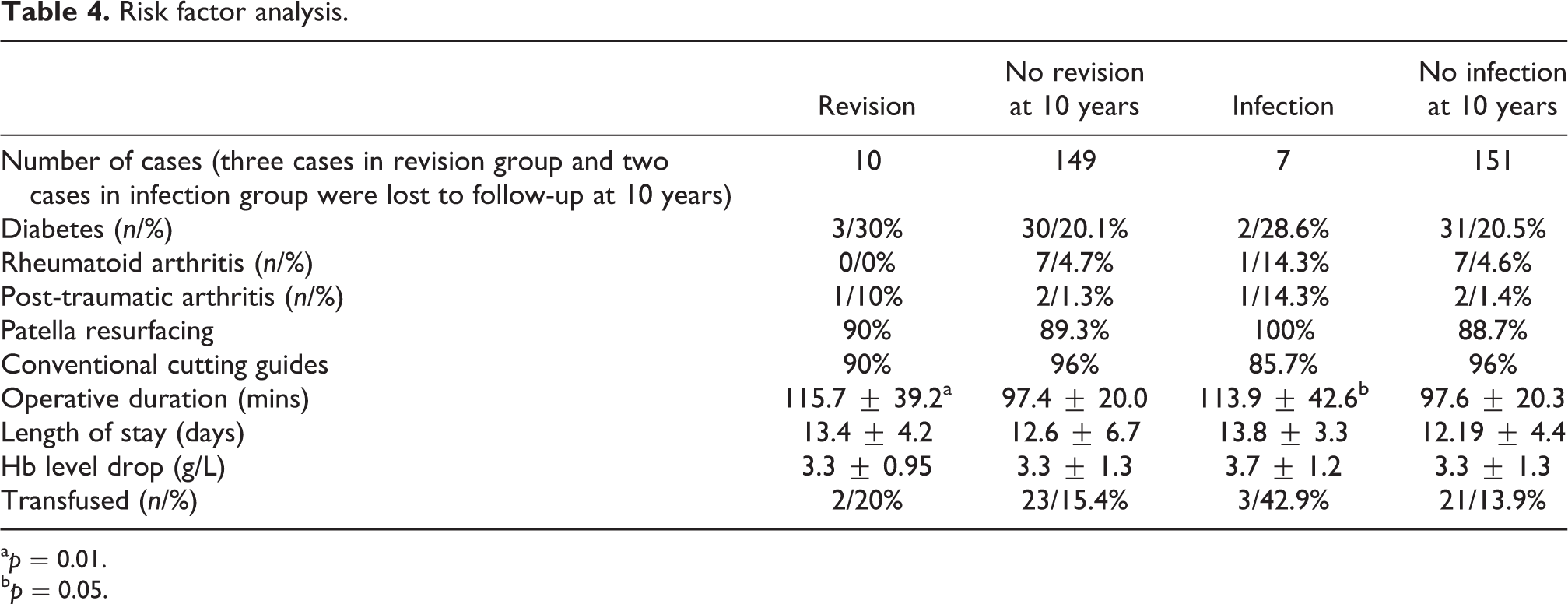
a p = 0.01.
b p = 0.05.
For intraoperative factors, data on patella resurfacing, bone cutting guides and intraoperative blood lost demonstrated no statistical significance for rate of infection or revision. Brands and model of implants had not shown statistical difference for infection or revision rates.
For post-operative length of stay, the case of early infection was not discharged before revision and regime of antibiotics, and was thus excluded from the analysis. Comparing inpatient length of stay between cases of revision and infection against the cases without revision and infection at 10 years of follow-up, no significant difference was noted (p = 0.71 and p = 0.36, respectively).
Discussion
Total knee arthroplasty was performed in a relatively elderly population. The age of total knee arthroplasty for United Kingdom was median 69 years old, 3 Norway mean 68.5 years old, 2 Swedish mean 68.8 years old 19 and Swiss mean 69.2 years old. 1 This study had a mean age of operation of 69.6 years which reflects the author’s centre had similar age as common registries.
Survival of total knee arthroplasty posterior-stabilised group was 96% at 10 years in the British Registry 3 and all total knee arthroplasty 96% in Norwegian 2 Registries. Our centre had demonstrated a similar survival rate of 94.2% at 10 years. Revision and combined infection rates were both low at 6.4% and 4.4% at 10 years of follow-up, respectively, similar to other local data 20,21 and international data. 5
The most common reasons for revision arthroplasty in current literature are infection and aseptic loosening. 10,12,22 –24 In this study, the main cause of revision arthroplasty was infection, followed by aseptic loosening, thus compatible with current literature. In this series, there is a total of seven cases with infection. The early post-operative infection rate was low at 0.9% (one deep and one superficial), and overall infection at 4.4% at 10 years of follow-up.
There had been conflicts among literature regarding post-operative length of stay on risk of infection. 25,26 Current literature had suggested that co-morbidity such as diabetes, anaemia, thyroid disease, heart disease, lung disease, liver disease and rheumatoid arthritis could result in increased infection risk. 18,21,26 Other factors that could increase infection risk include long operating time, 16,18 younger age, allogeneic blood transfusion 26 and posterior-stabilised implant. 27 In this study, operative duration of arthroplasty which had subsequent revision (mean 115.7 mins) was significantly longer than cases without subsequent revision (mean 97.4 mins) (p = 0.01). While cases which had subsequent infection seemed to have a longer operative duration (mean 113.9 mins) was just short of statistical significance (p = 0.054). In the study, cases that were complicated with infection seem to have a higher post-operative blood transfusion rate that was just short of statistical significance (42.9% vs. 13.9%, p = 0.07), likely due to the low number of infection cases. Operative duration of an arthroplasty could have been attributed by various factors. Norwegian Registry analysed by Badawy et al. 28 found up to 10 factors that could relate to longer procedural duration. With regard to other co-morbidity, this study was unable to demonstrate any statistical significant difference in relation with revision or infection. Further study with a larger database might be required to demonstrate this difference.
Conclusion
The 10-year survival rate of total knee replacement is high both in this study and current literature. The revision rate, early post-operative infection rate and overall infection at 10 years of follow-up were low. The most common causes of revision arthroplasty are infection and aseptic loosening. This study demonstrated that operative duration of the initial arthroplasty was significantly longer in cases which require subsequent revision.
Footnotes
Authors' Note
Tao Sun Tycus Tse is now affiliated with Department of Orthopaedics & Traumatology, Pamela Youde Nethersole Eastern Hospital, Hong Kong.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.