
Abstract
Background/Purpose:
To clarify the relationship between body mass index (BMI) and quality-of-life (QOL) recovery in individuals who underwent total knee arthroplasty (TKA).
Methods:
This prospective cohort study included 80 individuals who underwent TKA. The dependent variable was the Japanese Knee Osteoarthritis Measure used for assessing the QOL, and the independent variables were age, sex, BMI, and the Kellgren–Lawrence grade. A hierarchical multiple regression analysis was used to clarify whether BMI was a significant independent variable after accounting for other factors.
Results:
Sex was found to be the only significant predictor (β = 0.29, p < 0.05), and BMI was not related to QOL recovery in individuals who underwent TKA.
Conclusion:
This result suggests that sex was related to QOL recovery and should be assessed and that BMI was not related to QOL recovery in individuals who underwent TKA. These results may help health-care providers to identify individuals who might struggle with QOL recovery.
Introduction
Knee osteoarthritis (OA) is a degenerative and prevalent disease of the knee joint in older adults. It is estimated that knee OA occurs in 19% of American adults aged 45 years and above. 1 In Japan, the prevalence of knee OA in the age group of 70–79 years was 48.2% in men and 71.9% in women. 2 Knee OA is believed to be highly prevalent in developed nations because of a high life expectancy and recent increases in body mass index (BMI). 3 High BMI has become epidemic in developed nations and is a well-known risk factor for knee OA. 4,5
When treatment with non-pharmacological and pharmacological interventions are unsuccessful, surgical intervention is considered. Total knee arthroplasty (TKA) is an effective procedure for treating end-stage knee OA and improves knee pain, activities levels, and quality-of-life (QOL). 6 –9 However, a satisfactory improvement in QOL may not always be achieved in individuals after TKA. Approximately 10% of individuals show no improvement in health-related QOL after TKA. 10 Thus, it is important for both individuals and rehabilitation therapists to clarify factors related to QOL recovery after TKA.
To clarify factors related to QOL recovery after TKA, the relationship between BMI and QOL recovery has been examined because BMI has been reported to impact knee OA. 11 –14 Some studies have examined the influence of BMI on physical activity limitations in QOL assessed using SF-36 after TKA, 11 the majority of previous studies have concluded that high BMI was not a significant predictor of physical function and QOL recovery after TKA. 12 –14
Although previous studies showed no significant relationship between BMI and QOL, most results were obtained from data in the Western countries. According to a previous study by the World Health Organization (WHO), 15 BMI of the Asian populations was lower, and the Asian populations have different associations between BMI and health risks compared with the European populations. In fact, Japan has one of the lowest BMI population among the Organisation for Economic Co-operation and Development countries. 16 Furthermore, Lynch et al. 17 found that the Asian/Pacific Islander had the highest risk of QOL decline with an increase in BMI among the five racial/ethnic groups. Therefore, the impact of BMI in Japanese needs to be analyzed in detail, and there is a possibility that BMI has a greater influence on QOL recovery after TKA in the Japanese population than in the Western populations. However, no study has examined the relationship between BMI and QOL recovery in Japanese individuals who underwent TKA.
The aim of this study was to clarify the relationship between BMI and QOL recovery in Japanese individuals who underwent TKA, including other potential factors.
Methods
Participants
The selection criteria were hospitalization for scheduled primary TKA, participants who could walk independently with and without canes, and participants who consulted and visited a hospital 1 month after TKA. Participants with rheumatoid arthritis, systemic lupus erythematosus, dementia, psychiatric disease, neurological problems, cancer, TKA complications, and/or previous TKA were excluded. Eighty participants (18 men and 62 women) with a mean age of 74.1 ± 7.9 years (mean ± standard deviation: SD) were recruited in this study (Table 1).
Baseline characteristics of all participants and univariate analyses between the groups.
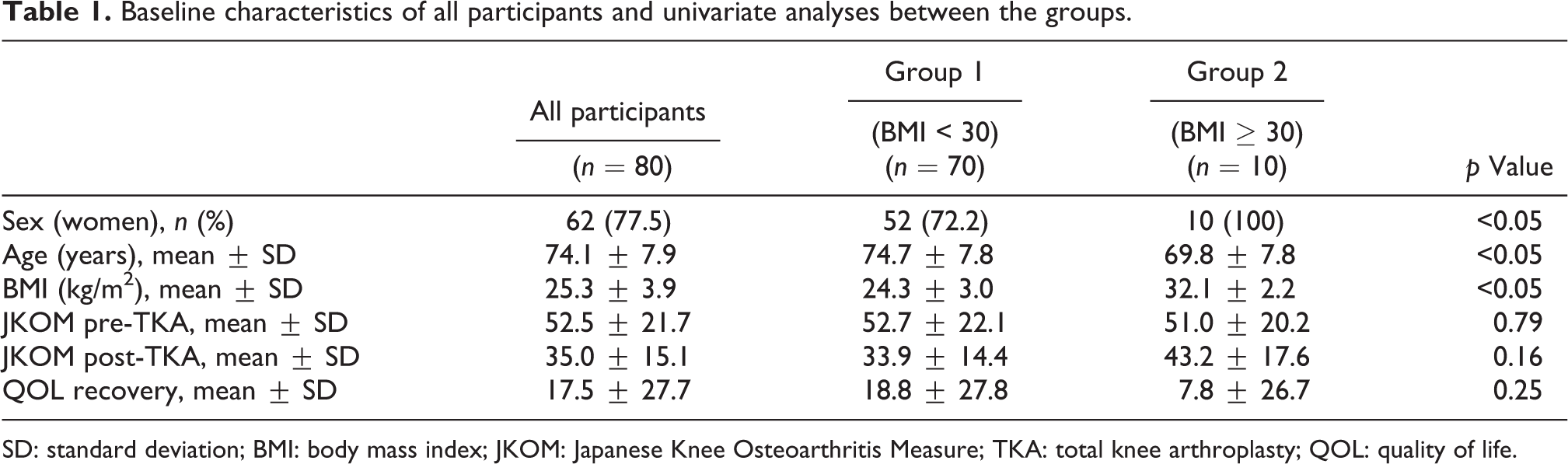
SD: standard deviation; BMI: body mass index; JKOM: Japanese Knee Osteoarthritis Measure; TKA: total knee arthroplasty; QOL: quality of life.
Ethics
This study complied with the principles of the Declaration of Helsinki and was approved by the institutional review board of the authors. All participants provided written informed consent prior to participating in the study.
Study design and setting
This prospective, multicenter study was conducted in five hospitals between July 2013 and September 2016. Type of TKA was recorded from surgery record as minimally invasive surgery or conventional surgery techniques: minimally invasive surgery was defined as a skin incision of 5 inches or less based on a previous study. 18 Participants received a standardized rehabilitation program that was directed by a clinical pathway (CP), and discharge was scheduled within 21 days. The CP was similar between most hospitals, although there were some small variations. A common CP for TKA in Japan consists of progressive resistive training of the lower extremity, including hip abductor, hip extensor, knee extensor and ankle exercise, transfer training, and walking training. A CP has been shown to be effective at reducing the length of hospital stay. 19 Discharge is permitted after the wound is checked by a medical doctor in the hospital participating in this study. Medical costs were covered by the national health insurance in Japan.
Independent variables
Participants’ demographics, age, and sex were recorded. These factors were selected based on a previous study 20 : this previous study showed that higher age, female sex, and higher BMI were all independent risk factors for delayed functional recovery after TKA at acute phase, whereas surgical factors such as blood loss, tourniquet time, and postoperative morphine use did not affect the recovery. Female sex was coded as 0. BMI was calculated using body weight in kilograms and height in meters (kg/m2). Based on the criteria of WHO, 21 participants were categorized, 3 for “Underweight: BMI < 18.5,” 41 for “Normal range: BMI 18.8–24.9,” 26 for “Preobese: BMI 25.0–29.9,” 9 for “Obese class I: BMI 30.0–34.9,” and 1 for “Obese class II: BMI 35.0–39.9.” There was no participant who was “Obese class III: BMI ≧ 40.0.” In addition, participants were categorized into two groups: BMI of 29.9 or less (group 1: nonobese group) and BMI of 30 and greater (group 2: obese group). These groups were coded as 0 and 1. The severity of knee OA was measured using the Kellgren–Lawrence grade (K-L grade). The grades were classified from grade II dysplasia (coded as 0) to the most severe grade IV (coded as 2) by orthopedic surgeons or by physical therapists. To avoid measurement bias, all physical therapists completing the K-L grades were trained by orthopedic surgeons using a standard measurement manual. The inter-rater reliability of the K-L grade was previously demonstrated to be high. 22 Age, sex, BMI, and the K-L grade were treated as independent variables.
Dependent variable
The Japanese Knee Osteoarthritis Measure (JKOM) was used for assessing QOL. The JKOM is a self-administered, disease-specific measure. The JKOM was assessed 1 day before TKA (JKOM pre-TKA) and 1 month after TKA (JKOM post-TKA). We measured JKOM 1 month after TKA as the JKOM post-TKA because it was clarified that QOL levels at acute phase of TKA were related with patient satisfaction, walking limitation, and fall risk at 1 year after TKA. 23 –25 Clarifying the factors related to QOL recovery at acute phase is important to consider appropriate intervention for obtaining a better long-term outcome. The JKOM was designed to incorporate the concepts of the International Classification of Functioning, Disability and Health (WHO, 2001) and to reflect the Japanese cultural lifestyle, which differs from that of the Western countries. 26 Knee flexion is required for daily activities in Asian countries such as squatting position for sitting on the floor and making a bed. These aspects of movement required in Asian countries were reflected in this assessment tool. The JKOM comprises 4 categories (pain and stiffness, condition in daily life, general activities, and health conditions) and 25 subcategories. The subcategories were consisted of 8 items for “pain and stiffness,” 10 items for “condition in daily life,” 5 items for “general activities,” and 2 items for “health conditions” (Appendix 1). Each subcategory is scored from 0 to 4, yielding a total score within the range of 0 (good condition) to 100 (bad condition). The high levels of reliability of the JKOM for assessing Japanese individuals with knee OA has been previously demonstrated: The Cronbach’s α coefficient was 0.911. 26 QOL recovery was defined as the changed value of the JKOM in pre- and post-TKA, and it was treated as the dependent variable. A high value of QOL recovery indicated improvement.
Data analysis
Mann–Whitney U tests were used for comparing age, BMI, JKOM pre-TKA, JKOM post-TKA, and QOL recovery between the groups. Chi-squared test was also used for comparing sex between the groups. In addition, paired t-test was performed for comparing JKOM pre-TKA and JKOM post-TKA. A hierarchical multiple regression analysis was used to clarify whether BMI was a significant independent variable after accounting for other factors. First, independent variables such as age, sex, and the K-L grade were entered into the model using forced entry. Second, BMI was entered into the model with forced entry. All data were analyzed using SPSS (version 25.0, SPSS Inc, Chicago, Illinois, USA), and values of p < 0.05 were considered to indicate statistical significance.
Sample size
The α value was set at 0.05, and the power was set at 0.80. Based on the previous study, 27 the hypothesized effect size f 2 was set at 0.35 (meaning large effect size). The number of predictors was 5. Consequently, it was estimated that total 43 cases were required in this study.
Results
In this study, 95% of participants had TKA with minimally invasive surgery technics. The mean BMI of all participants was 25.3 ± 3.9 kg/m2. The mean BMI of group 1 was 24.3 kg/m2 (SD = 3.0) and that of group 2 was 32.1 kg/m2 (SD = 2.2). The K-L grade of all participants was categorized as 2 for grade II, 43 for grade III, and 36 for grade IV. Baseline characteristics of all participants are summarized in Table 1. There were significant differences in sex, age, and BMI between the groups (Table 1). The paired t-test identified that the JKOM post-TKA (35.0 points) was significantly improved compared with JKOM pre-TKA (52.5 points).
A hierarchical multiple regression analysis was used to identify whether BMI was associated with QOL recovery after accounting for other factors. The regression analysis revealed that BMI was not a significant predictor and that sex was the only significant predictor (β = 0.29, p < 0.05). Female sex was related to a worse QOL recovery in this study (Table 2).
Results of the hierarchical multiple regression analysis.
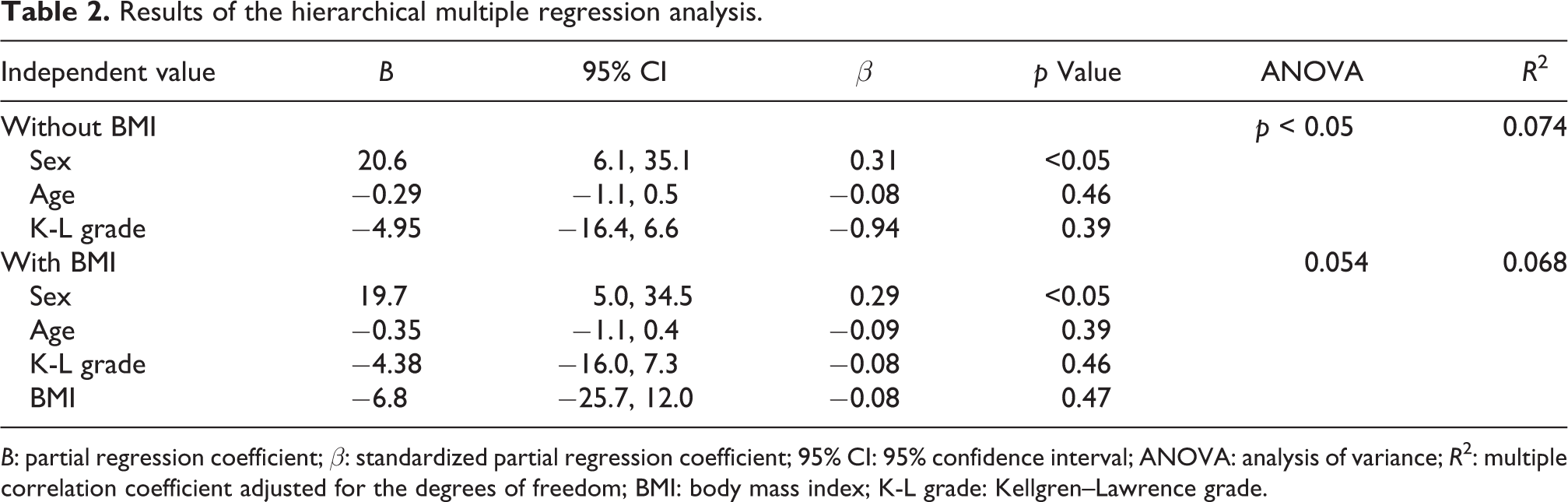
B: partial regression coefficient; β: standardized partial regression coefficient; 95% CI: 95% confidence interval; ANOVA: analysis of variance; R 2: multiple correlation coefficient adjusted for the degrees of freedom; BMI: body mass index; K-L grade: Kellgren–Lawrence grade.
Discussion
The present study examined the relationship between QOL recovery and potential factors including BMI in individuals who underwent TKA. We hypothesized that BMI had a significant impact on Japanese individuals who underwent TKA because the Asian populations, including the Japanese population, have different associations between BMI and health risks compared to the Western populations. 15 –17 Although JKOM post-TKA was significantly improved, BMI was not a significant predictor in the final regression model. Previous studies in the Western countries showed that BMI was not related to QOL recovery after TKA. 12 –14 The result of this study on Japanese individuals who underwent TKA is in agreement with these previous results. This study is the first to clarify the relationship between QOL recovery and BMI in Japanese individuals who underwent TKA. Health-care providers can use the results of this study to identify individuals who may struggle with QOL recovery.
A previous research determined that BMI influences outcomes after TKA despite no relationship obtained between these in the present study. 28 One potential explanation for this discrepancy is that participants in this study were different to those included in the previous study. The previous study demonstrated that only participants who were morbidly obese (BMI > 35.0 kg/m2) showed increased pain severity and limited physical activity after TKA. In this study, participants in group 2 had an average BMI of 32.1 kg/m2 and a SD of 2.2. Therefore, even though participants with BMI > 30.0 kg/m2 were assigned to group 2 in this study as obese group, the recruited Japanese participants had a lower BMI than that of participants in the previous study. There is a possibility that if participants who have a BMI >35.0 kg/m2 are recruited in a future study, BMI will be associated to QOL recovery.
Female sex was only related with poor QOL recovery in this study. Hoogeboom et al. 20 clarified that female sex was the independent risk factor for delayed functional recovery after TKA after accounting for surgical factors. Our results support this findings. Similarly, Paterson et al. 29 clarified that changes in gait biomechanics after TKA were influenced by sex but not preoperative obesity. After TKA, man experienced a decrease in peak knee adduction moment (KAM) and KAM impulse whereas women did not. The influence of sex on improvements in the peak KAM and KAM impulse is likely driven by the peak knee frontal plane angle becoming more valgus in men but not women, given male body weight did not change after TKA. Walking ability is important to obtain a better QOL. Thus, these sex differences of changes on body weight and biomechanics after TKA may influence QOL recovery in this study.
In this study, multiple correlation coefficient adjusted for the degrees of freedom was 0.068. This suggests that there are other factors associated to QOL recovery after TKA. A systematic review suggested that sarcopenic obesity is a more important factor for predicting a recovery after TKA than BMI. 30 Oosting et al. 31 determined that obesity with muscle weakness was related to outcomes such as delayed independent walking and prolonged hospital stays compared with obesity alone in individuals with total joint arthroplasty. Hence, it is necessary to determine the relationship between sarcopenic obesity and QOL recovery in a future study.
This study has several limitations. Firstly, this study did not include a long-term follow-up. Secondly, this study did not recruit individuals who were morbidly obese. Zusmanovich et al. 32 examined the influence of morbid obesity in individuals with knee OA and BMI > 40 kg/m2. These individuals demonstrated more infectious and medical complications, longer operating times and length of hospital stay, and a high rate of follow-up surgeries after TKA. However, it may need to consider that there are few people who has BMI > 40 kg/m2 in Japanese. In fact, according to a previous study, the incidence of “Obese class I” was 34% in the United States but 2.9% in Japan. 33 This limitation might be resolved in large sample size. Thirdly, although sex was significant, only 6.8% of the explained variance in QOL recovery was captured. This suggests that there are other significant factors such as surgeon factors, treatment factors, and sarcopenic obesity that should be considered. Therefore, we need to perform a future multivariate longitudinal study with large sample size to include people who are morbidly obese.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Grant-in-Aid for Young Scientists (B) of Japan Society for the Promotion of Science (grant number JP25750245).