
Abstract
Background
While previous research has demonstrated potential advantages of unicompartmental knee arthroplasty (UKA) over total knee arthroplasty (TKA), particularly in terms of clinical outcomes such as function and pain relief, the specific impact on health-related quality of life (HRQOL) remains unclear. This systematic review and meta-analysis aim to address this gap by comparing HRQOL outcomes between UKA and TKA, providing valuable insights for clinical decision-making.
Methods
We conducted a literature search in the PubMed, Embase, Cochrane Controlled Register of Trials (CENTRAL), and Web of Science databases up to July 15, 2023. Eligible studies assessed HRQOL using EQ-5D, SF-36, or SF-12 and were assessed for methodological quality using the Newcastle-Ottawa Scale (NOS).
Results
Seven eligible studies were included, comprising a total of 64,585 patients with 35,809 undergoing TKA and 28,776 undergoing UKA. Patient age ranged from 52.0 to 67.7 years with an average BMI ranging from 27.2 to 31.0 kg/m2. Follow-up periods ranged from 6 months to 10 years. Five studies (63,829 patients) that evaluated HRQOL using EQ-5D showed significantly better outcomes for UKA compared to TKA (MD -0.04, 95% CI -0.05 to −0.02). Two studies (756 patients) that evaluated HRQOL using SF-36 showed no significant difference between TKA and UKA. Five studies (63,286 patients) that evaluated functional outcomes using Oxford Knee Score (OKS) showed significantly better functional scores for UKA compared to TKA (MD -1.29, 95% CI -1.86 to −0.72). Four studies (24,570 patients) that reported patient satisfaction showed no statistically significant difference between TKA and UKA (MD 0.97, 95% CI 0.90 to 1.05). Further subgroup analysis did not affect the conclusions.
Conclusions
Our meta-analysis suggests that UKA is associated with better HRQOL and knee function, as well as similar patient satisfaction, compared to TKA for patients with unicompartmental osteoarthritis.
Keywords
Introduction
Unicompartmental knee arthroplasty (UKA) and total knee arthroplasty (TKA) are both effective treatments for unicompartmental osteoarthritis (OA), with proven reliability and success. However, there remains a lack of consensus regarding the preferred surgery. 1 Traditionally, the efficacy of knee arthroplasty has been evaluated based on objective clinical data such as revision rates, implant survival rates, complication rates, and relevant radiological parameters, as assessed by physicians.2,3 While these metrics are vital for assessing surgical outcomes, they may not capture the full extent of the surgery’s efficacy for the patient. Research has found that despite favorable objective efficacy evaluations, a substantial number of patients remain dissatisfied with the results of knee arthroplasty surgery.4–9 This highlights the need to explore additional factors that contribute to patient satisfaction and overall quality of life following surgery.
As society progresses and living standards rise, people are increasingly seeking higher levels of quality of life following knee arthroplasty procedures. Consequently, evaluating patients' subjective experiences, such as health-related quality of life (HRQOL), is becoming essential in assessing the efficacy of knee arthroplasty surgery.
HRQOL can be defined as the extent to which perceived health affects an individual’s ability to lead a fulfilling life. 10 As a multifactorial construct, HRQOL encompasses measures of social, physical, psychological and emotional factors, while also taking into account the individual’s goals, values, and life priorities.11–13 Generic methods such as EuroQol5-Dimension scores (EQ-5D), Short Form-36 (SF-36), and Short Form-12 (SF-12) are widely used to measure HRQOL, providing insights into patients' overall well-being and functional status. Despite the availability of these measurement tools, there remains a need for further research to address several gaps in the current understanding of HRQOL among patients undergoing TKA and UKA. This study aims to fill this gap by conducting a systematic review and meta-analysis to comprehensively evaluate HRQOL outcomes in adults with unicompartmental osteoarthritis following TKA and UKA. By comparing the HRQOL outcomes associated with each surgical intervention, we seek to identify which approach offers superior benefits in terms of patient-reported outcomes. The findings of this study will be useful for surgeons and patients alike in making well-informed decisions regarding the choice of implant for the treatment of unicompartmental osteoarthritis.
Materials and methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 14 A research protocol was agreed upon by all co-authors prior to initiating the literature searches. The study protocol was registered on the PROSPERO International prospective register of systematic reviews (https://www.crd.york.ac.uk/PROSPERO/) with registration number: CRD42023408908.
Literature search and selection of studies
We conducted a systematic search of the PubMed, Embase, Cochrane Controlled Register of Trials (CENTRAL) and Web of Science databases to identify all relevant studies published up to July 15, 2023. Conference abstracts and case reports were excluded from the search. The search terms included but were not limited to “total knee arthroplasty”, “total knee replacement”, “TKA,” “TKR,” “unicondylar knee arthroplasty”, “partial knee replacement”, “unicondylar knee replacement”, “unicompartmental knee arthroplasty”, “UKA”, “UKR”, “PKR”, “health-related quality of life”, “HRQOL”, “SF-36”, “SF-12,” and “EQ-5D”. In PubMed, we attempted to use Medical Subject Headings (Mesh) whenever possible, otherwise, we searched for the terms in the title and/or abstract. In addition, we manually searched the reference lists of previous systematic reviews for additional studies. Two independent authors (KS and LPQ) initially screened studies based on title and abstract. In cases of disagreement or uncertainty, the full text was retrieved and reviewed, and any discrepancies were resolved through discussion with a third author (ZYM).
Inclusion criteria
The inclusion criteria for this systematic review were as follows: (1) The study should have included patients aged 18 years or older with unicompartmental osteoarthritis and reported on HRQOL outcomes following TKA and UKA; (2) HRQOL was measured with EQ-5D, SF-36 or SF-12 assessment tools before and after surgery, the follow-up period was at least 6 months (3) Studies were matched cohort analysis with similar baseline scores. Studies were excluded if they met any of the following criteria: (1) Patients with late patellofemoral joint (PFJ) arthritis; (2) Patients with anterior cruciate ligament (ACL) reconstruction in combination with UKA or UKA without an ACL; (3) Studies that considered revision arthroplasty, Periprosthetic joint infection, inflammatory arthritis, neurological disorders, or simultaneous TKA or UKA.
Outcomes
The primary outcome of this study is HRQOL, which was evaluated by EQ-5D, SF-36 or SF-12 at the 6-month follow-up after TKA or UKA. Secondary outcome included the assessment of patient satisfaction, as well as the Oxford Knee Score (OKS), a widely recognized measure of knee joint function.
Data extraction
The data were independently extracted from all included studies by two authors (LPQ, ZYM). The extracted information encompassed: (1) Study details such as authorship, year, and country; (2) Study design and follow-up; (3) Population characteristics such as cohort, sample size, gender, age, and body mass index (BMI); (4) Primary and secondary outcome measures. For studies with incomplete data, we attempted to contact the corresponding authors.
Risk of bias assessment
Two authors, KS and LPQ, independently evaluated the methodological quality and risk of bias of the included studies using the Newcastle-Ottawa Scale (NOS). 15 Any disagreements were resolved through discussion between the two authors, and in cases where consensus could not be reached, the opinion of a third author, ZYM, was sought.
Statistical analysis
Continuous variables were presented as mean ± standard deviation, while categorical variables were reported as absolute and relative frequencies. In cases where standard deviation was not reported, it was estimated from the standard error of the mean, 95% confidence interval, p value, or other methods recommended in the Cochrane Handbook. A random effects model was employed to account for heterogeneity, which was assessed using Cochrane’s Q test (χ2 p < .10) and quantified using I2. Significant heterogeneity was considered to be present when I2 was greater than 50%.
16
To further explain the heterogeneity among studies, subgroup analysis was conducted. Forest plots were used to visually display the effect size of each study and the pooled estimates. A p value
Results
Literature search
A total of 293 relevant articles were retrieved from our search. After removing duplicates and screening titles and abstracts, 23 full-text articles were reviewed for evaluation. Of these, 16 studies were excluded for various reasons. Ultimately, 7 eligible studies were included 17–23 (Figure 1). PRISMA flowchart of search strategy.
Study characteristics and risk-of-bias assessment
Important characteristics of patients enrolled in the included studies.

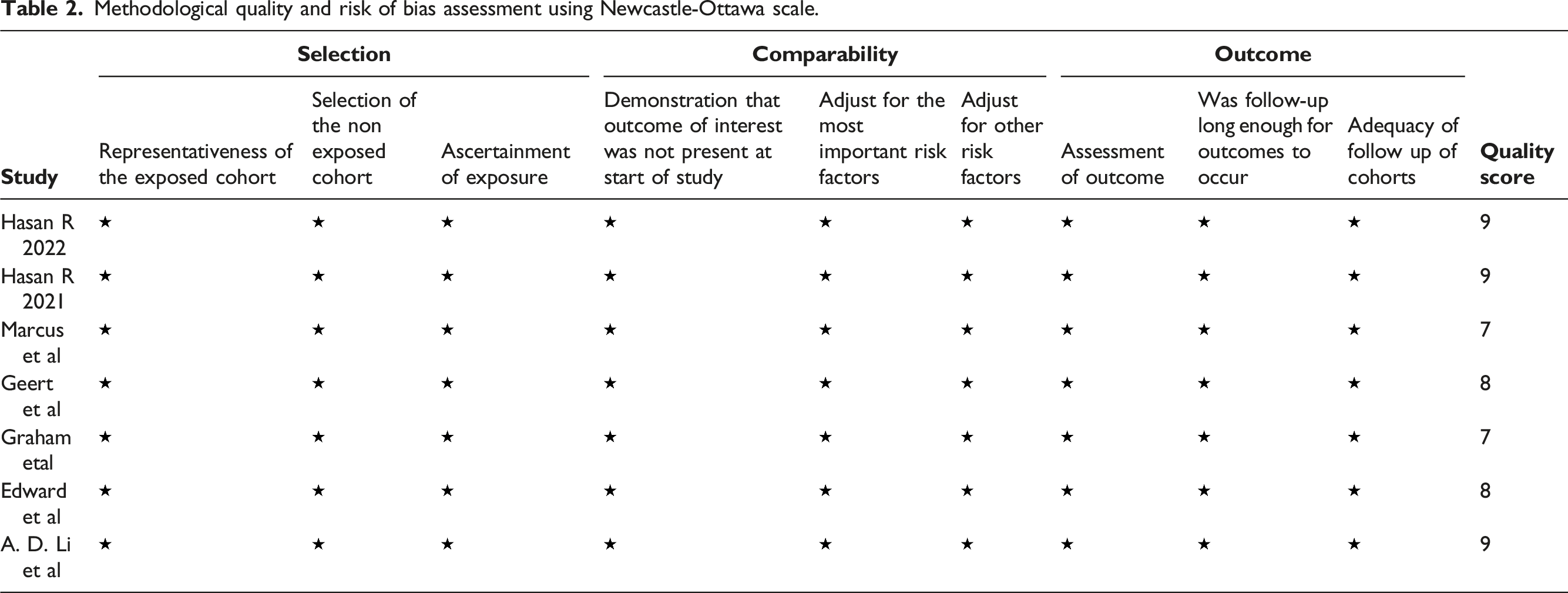
Methodological quality and risk of bias assessment using Newcastle-Ottawa scale.
Primary outcomes
Five studies17–20,23 (n = 63,829) evaluated HRQOL using the EQ-5D scale at 6 months follow-up. Forest plot analysis showed a statistically significant difference between the two groups (MD −0.04, 95% CI −0.05 to −0.02, p༜.0001, I2 = 85%) (Figure 2). Two studies21,22 (n = 756) assessed HRQOL using the SF-36 scale, and forest plot analysis revealed no significant difference between the TKA and UKA groups in both the SF-36 PCS (MD −1.01, 95% CI −2.43 to 0.41, p = .50, I2 = 0%; Figure 3) and SF-36 MCS scores (MD 0.29, 95% CI −1.18 to 1.76, p = .85, I2 = 0%; Figure 4). Forest plot analysis of health-related quality of life using EQ-5D in total knee arthroplasty and unicompartmental knee arthroplasty patients at 6 months post-surgery. CI confidence interval. Forest plot analysis of health-related quality of life using SF-36 PCS in total knee arthroplasty and unicompartmental knee arthroplasty patients at 6 months post-surgery. CI confidence interval. Forest plot analysis of health-related quality of life using SF-36 MCS in total knee arthroplasty and unicompartmental knee arthroplasty patients at 6 months post-surgery. CI confidence interval.


Secondary outcomes
Oxford knee score
Five studies17,19–22 (n = 63,286) reported pain and function outcomes at 6 months follow-up using the OKS. The UKA group had significantly better pain and function outcomes compared to the TKA group at 6 months (MD -1.29, 95% CI, −1.86 to −0.72, p < .00,001; I2 = 90%) (Figure 5). Forest plot analysis of oxford knee score in total knee arthroplasty and unicompartmental knee arthroplasty patients at 6 months post-surgery. CI confidence interval.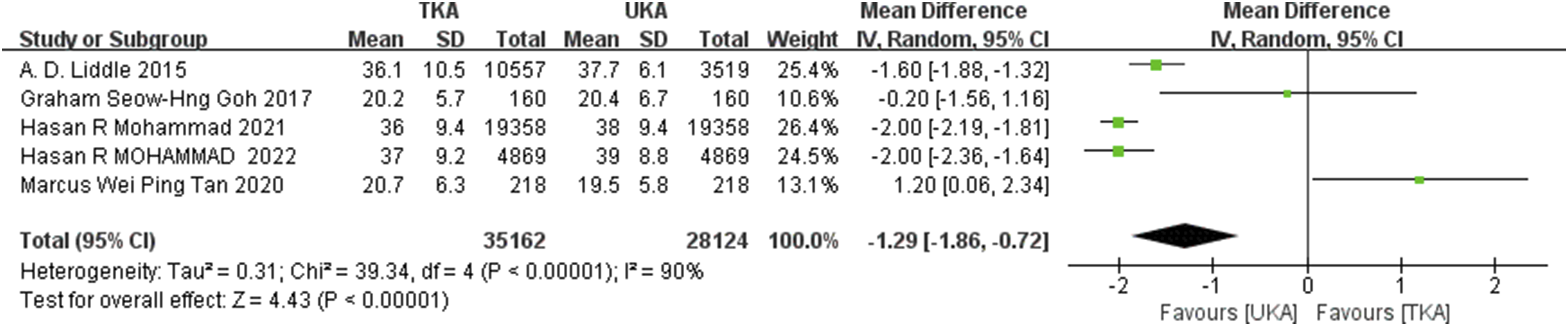
Patients’ satisfaction
Four studies19–22 (n = 24,570) reported patient satisfaction after surgery. Patients satisfaction showed no statistically significant difference between the two groups (MD 0.97, 95% CI, 0.90 to 1.05, p < .00,001; I2 = 95%) (Figure 6). Table 3 presents a summary of the outcomes from all the included studies. Forest plot analysis of patients’ satisfaction in total knee arthroplasty and unicompartmental knee arthroplasty patients. CI confidence interval. Summary of outcomes in both TKA and UKA groups.

Subgroup analysis
To address the high heterogeneity observed in the meta-analysis of HRQOL studies that utilized the EQ-5D instrument, we conducted a subgroup analysis based on the study design. The forest plot analysis revealed that 2 prospective studies18,23 and 3 retrospective studies17,19,20 showed similar results, with a mean difference (MD) of −0.10 (95% CI, −0.15 to −0.04; p = .18; I2 = 45%) and −0.03 (95% CI, −0.03 to −0.02; p = .22; I2 = 34%), respectively (Figure 7). Forest plot compares health-related quality of life between subgroups based on study design, utilizing the EQ-5D instrument. CI confidence interval.
Discussion
Previous studies comparing UKA and TKA outcomes have mainly focused on objective functional outcome scores, often overlooking the subjective experience of patients. In this meta-analysis, we aim to comprehensively investigate HRQOL after TKA and UKA to provide evidence supporting informed and shared decision-making in the care of patients with unicompartmental osteoarthritis. To the best of our knowledge, this is the first study of its kind to focus specifically on HRQOL in patients undergoing TKA and UKA.
The results showed that the UKA group had a significantly better HRQOL compared to the TKA group when using EQ-5D, while the difference was not statistically significant when using SF-36. However, considering the limited number of studies and patients that used SF-36 (only two studies21,22 with 756 patients), the former tool was deemed to be more reliable due to the larger number of studies and patients that used it (5 studies17–20,23 with 63,829 patients). Moreover, studies utilizing EQ-5D have higher literature quality and less risk of bias than those utilizing SF-36, with 3 out of 5 studies rated as NOS 917,19,20 and the remaining 218,23 scored as NOS 8, whereas studies utilizing SF-36 are rated as NOS 7.21,22 Further subgroup analysis suggest that the observed heterogeneity may be attributed to differences in the study design. Additionally, our findings demonstrate that UKA leads to superior knee function and equivalent patient satisfaction compared to TKA.
The superior HRQOL and knee function observed in the UKA group may be attributed to its ability to restore the ligament-driven kinematics of the native knee by retaining cruciate ligaments and quadriceps. 24 Additionally, UKA involves smaller incisions, minimal bone cuts, and soft tissue dissections, leading to shorter hospital stays, faster recovery times, lower rates of infection, morbidity, and mortality.25–27 However, studies have reported that the revision rate for UKA is significantly higher than that for TKA,28–31 making surgeons reluctant to select UKA and instead opting for TKA. Nonetheless, in high-volume centers, the long-term revision rates of UKA are very low.31,32 Factors contributing to differences in revision rates include the lower threshold for UKA revision,33,34 the proficiency of the surgeon, and the younger and more active patient population undergoing UKA.
OA is a common condition that can cause joint pain and impaired function. 35 However, OA not only affects the physical well-being of patients, but also their psychological health. Individuals with OA often experience severe psychological distress, such as depression, anxiety, and sleep disturbance.36,37 These symptoms have a significant impact on HRQOL of patients.38,39 Therefore, assessing HRQOL is crucial for evaluating the extensive health implications of OA and its treatment. Our study’s 6-month follow-up period aligns with previous research indicating substantial HRQOL improvements within the first 6 months post-surgery, with relatively stable outcomes thereafter.40,41
Patient-reported outcomes measures (PROMs) for UKA and TKA encompass pain relief, functional improvement, satisfaction, activity level, joint perception, psychological well-being, and health-related quality of life. While no previous meta-analyses have focused specifically on HRQOL after TKA and UKA, other systematic reviews have examined related PROMs for comparison purposes. Arirachakaran et al 42 analyzed data exclusively from randomized controlled trials (RCTs) and found that patients who underwent UKA had better PROMs scores for function and range of motion than those who underwent TKA. Wilson et al 43 conducted a meta-analysis that included RCTs, cohort studies, and national joint registries, and found that UKA had better combined PROMs scores than TKA. Tripathy et al 44 found that UKA patients were less aware of their artificial joint in daily life compared to TKA patients, as assessed by the Forgotten Joint Score (FJS-12). Other studies45–47 have also reported superior range of motion and cost-effectiveness for UKA. Our study is consistent with these results.
Our review had several limitations. Firstly, the meta-analysis was limited by the relatively small number of studies available on the topic, especially high-quality studies including RCTs, which hindered our ability to conduct graphical or statistical assessments of publication bias. 48 Secondly, the differences in patient selection, implant selection, surgical techniques, and rehabilitation protocol may have resulted in diverse outcomes, leading to high heterogeneity among the studies. Thirdly, the analysis for the change in the PROMS was not discussed in our article, which is a valuable research direction in the future. Despite these limitations, our review also had specific strengths. The use of standardized methods for study selection, data extraction, and quality assessment enhanced the validity and reliability of our findings. Meanwhile, the outcomes of this meta-analysis had certain clinical significance.
Conclusions
Our systematic review and meta-analysis indicate that for individuals with unicompartmental osteoarthritis, UKA appears to result in superior HRQOL, improved knee function, and comparable levels of patient satisfaction when compared to TKA. Despite the substantial advantages associated with UKA, it must call out that not all TKA candidates are UKA candidates. Care must be taken to avoid erroneous application of this data.
Footnotes
Authors’ Contributions
KS Designed the study, conducted the literature search, and draft the manuscript. LPQ and ZYM Independently reviewed the selected studies and extracted relevant data. HYS participated in the design of the study and performed the statistical analysis. SHZ Interpreted the findings and contributed to the discussion section. DHL, SHL, and YGL Provided supervision and guidance throughout the research process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
No repositories were used for data.