
Abstract
Non-infectious subcutaneous emphysema of the hand has previously been mentioned in literature. In most cases, it presents in a benign and self-resolving form, which may be managed conservatively. However, in cases of subcutaneous emphysema involving insufflation with nitrogen gas, clinical vigilance is advised as acute compartment syndrome may be a potential complication due to the non-permeative nature of the gas. This would necessitate a complete change in the dynamics of management, warranting urgent surgical intervention. Current literature on acute compartment syndrome of the hand complicating subcutaneous emphysema is scarce. This report aims to highlight this unique case and add to the current literature on this rare condition.
Introduction
Non-infectious subcutaneous emphysema of the hand has previously been described in literature. In most cases, it presents in a benign and self-resolving form, which may be managed conservatively. 1 –4 However, in cases of subcutaneous emphysema involving insufflation with nitrogen gas, clinical vigilance is advised as acute compartment syndrome may potentially complicate it due to the non-permeative nature of the gas. This would necessitate a complete change in the dynamics of management, warranting urgent surgical intervention. Current literature on acute compartment syndrome of the hand complicating subcutaneous emphysema is scarce. This report aims to highlight this unique case and add to the current literature on this rare condition.
Case report
A healthy 27-year-old, right-hand dominant gentleman presented to the Emergency Department complaining of pain and swelling of the right hand after an alleged industrial injury. The patient, who worked in a tyre shop, had accidentally punctured and inflated the first web space of his right hand with a high-pressure pneumatic pump while attempting to ‘purge and fill’ a tyre with nitrogen gas. He presented to us a few hours after the injury had occurred. Clinically, there was a puncture wound situated at the dorsal aspect of the first web space of the right hand with evident swelling (Figure 1a, 1b and 1c). Crepitus was felt on palpation over the dorsal surface of the right hand. Range of motion of all finger joints was limited due to pain, but full range of motion was maintained at the right wrist and elbow. Sensation remained intact in all fingers and capillary refill time was less than 2 s. Radiographs of the right hand revealed the presence of gas shadows between the first and second web spaces tracking to the radial border of the wrist (Figure 2a and 2b). He was diagnosed as a case of subcutaneous emphysema of the right hand by the Emergency Department Medical Officer and subsequently referred to the Orthopaedic team for further management. Unfortunately, his condition took a turn for the worse while waiting to be assessed by the Orthopaedic team. He started complaining of increasing pain and numbness over the radial (dorsal and radial) aspect of his right hand (corresponding to the puncture wound area). Worsening of the swelling and increasing tenderness was also noted. Active and passive movement of all fingers accentuated the pain. Despite these findings, the capillary refill time remained less than 2 s. He was assessed and diagnosed with acute compartment syndrome of the right hand complicating subcutaneous emphysema due to accidental insufflation with nitrogen gas. The patient subsequently underwent fasciotomy of the right hand. As all compartments of the right hand were clinically involved, a fasciotomy procedure involving two dorsal longitudinal incisions over the second and fourth metacarpals, a longitudinal incision over the radial side of the first metacarpal and a longitudinal incision over the ulnar side of the fifth metacarpal was done. A carpal tunnel release was also performed in addition to this. The wounds were left open to heal by secondary intention. He progressed well post-operatively and was discharged 48 h later with an uneventful recovery. At his last review at a month post-operatively, his surgical wounds were well healed and rehabilitative progress was noted to be good.
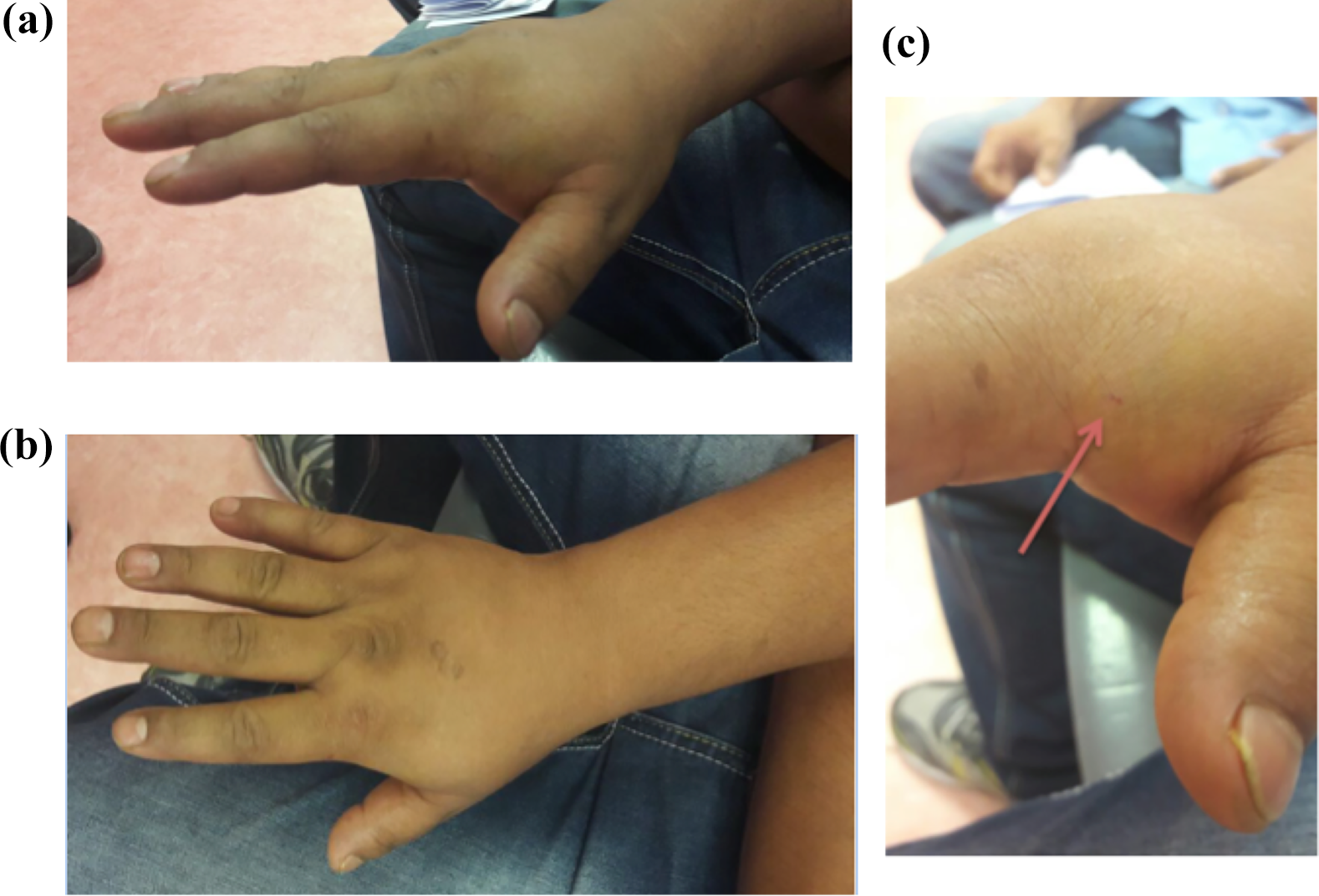
(a, b) Swollen dorsum of right hand and (c) close-up image of the puncture wound (pointed arrow) sustained at the dorsal surface of the first web space.
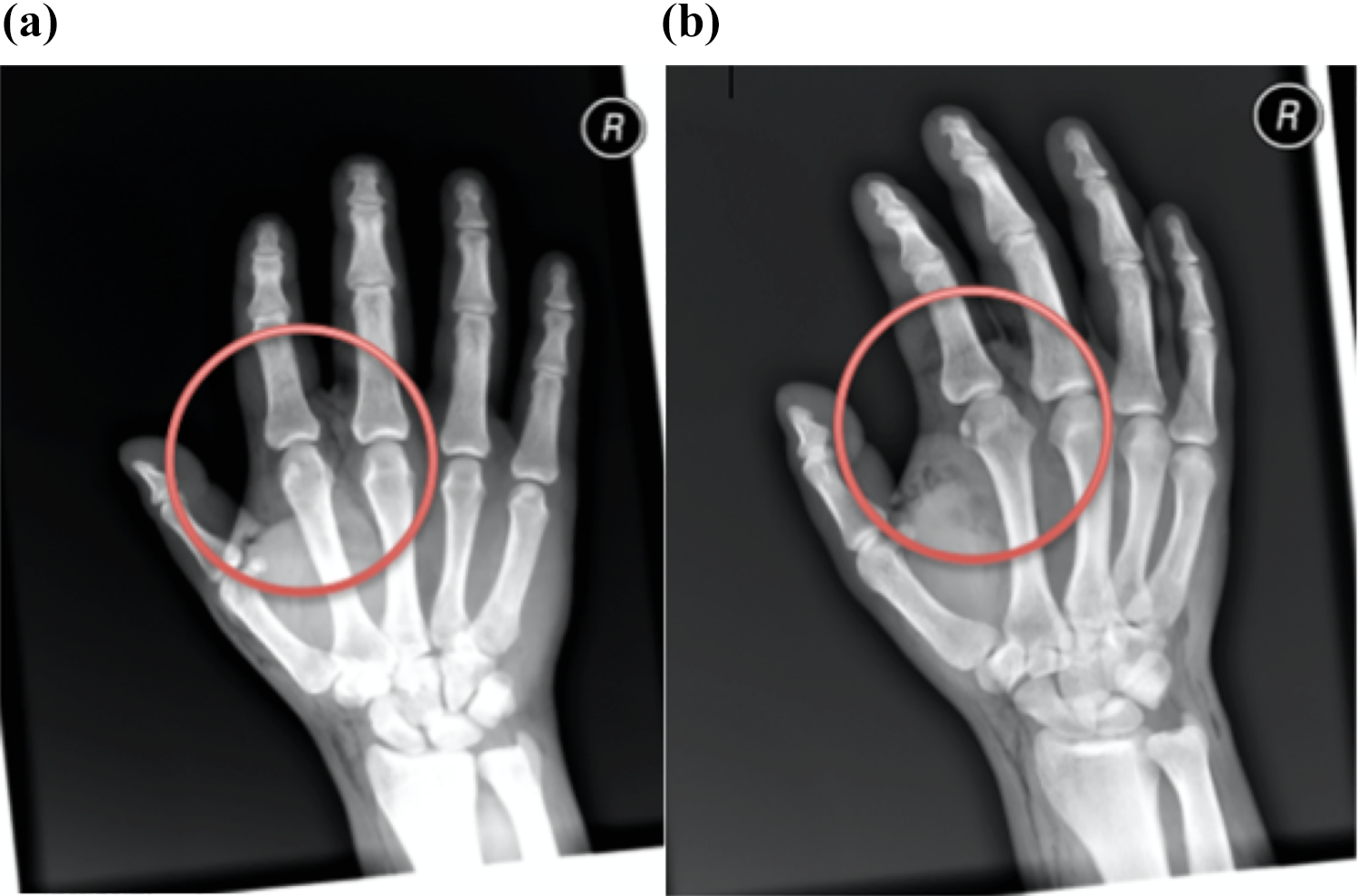
(a, b) Radiographs of anterior-posterior and oblique views of the right hand showing gas shadows (circled within the soft tissues of the first and second web space) tracking up to the radial aspect of the wrist.
Discussion
Subcutaneous emphysema of an isolated limb is rare. It has previously been described but none resulting with acute compartment syndrome of the involved limb. 2,5 –8 The condition may be caused by both infectious and non-infectious causes. 9 Clinically, both entities present with swelling and palpable crepitus of the affected limb. However, malaise, fever and leucocytosis are usually present in cases of infectious origin, which is caused by gas-forming organisms such as clostridia, anaerobic streptococci and coliform bacteria. 9 Proper diagnosis at presentation is crucial as management and prognosis differ greatly in both these conditions. A comprehensive history and detailing of the timeline of onset is key to aiding the diagnostic process in addition to a thorough physical examination with relevant investigations. Butt and Hird and Filler et al. mention that infection from gas-forming organisms usually takes between 12 h and 18 h to develop. They also describe that gas in the subcutaneous space, which develops within 6–10 h of trauma, is suggestive of a benign process. 1,2
The index patient sustained a condition, which was of non-infectious origin, caused by a puncture wound from a high-pressure pneumatic device. Puncture wounds due to these devices may result in one-way valve mechanisms, which trap air and cause subcutaneous emphysema. The composition of air pumped through these devices usually consists of air with approximately 78% of nitrogen, 21% of oxygen and 1% of miscellaneous gases. 4 In theory, this composition of mixed gases may escape from the area of insufflation with time via a process known as permeation. This may explain the self-resolving nature of subcutaneous emphysema in previously described cases. 3,5 However, in our patient, accidental insufflation with nitrogen gas from a high-pressure pneumatic pump had occurred while he was in the process of ‘purging and filling’ a tyre. This is a process commonly done when attempting to fill a tyre with pure nitrogen in order to strain the oxygen out of the tyre. Tyres filled with pure nitrogen are said to have pressures that remain more constant, as they are less likely to permeate from the tyre, which explains its application in high-performance race cars and heavy-duty vehicles. Despite the benefits gained on the road, nitrogen in this case most likely exerted a deleterious effect as it only dissolves slowly within a confined soft tissue space. This property has been demonstrated in a study assessing insufflation gas for laparoscopic surgery. 10 With a relatively high and constant volume of nitrogen gas trapped within the subcutaneous tissue for a prolonged period of time, venous collapse, reduced arteriovenous pressure gradient and increasing interstitial pressure could have led to compartment syndrome.
Acute compartment syndrome is defined as a symptom complex due to raised pressure within a closed osseo-fascial space that leads to circulatory compromise and dysfunction of contents of the space. 11,12 This may complicate subcutaneous emphysema as gas such as nitrogen can track into deeper soft tissues and musculature via fascial planes. This condition develops when either volume of a compartment reduces or volume of its contents increases. It eventually leads to circulatory compromise due to the pathophysiological cascade described above making it an orthopaedic emergency. Patients will usually present with a swollen, tense and tender limb, complaining of pain that is out of proportion to the injury, which is further magnified with passive stretching of the fingers. This may progress to paraesthesia and subsequent paralysis if left untreated. Diagnosis is primarily clinical, however, in children or patients who are obtunded or sedated, the diagnosis may be aided by various intra-compartmental measurement techniques. These include invasive techniques such as the infusion technique, slit catheter technique, continuous infusion and monitoring technique or intra-compartmental pressure monitoring systems. Non-invasive techniques mentioned in literature include ultrasonic devices, near-infrared spectroscopy and laser Doppler flowmetry. 11
Indications for fasciotomy include clinical signs and symptoms consistent with compartment syndrome such as pain out of proportion to the injury, swelling and progressive numbness, compartment pressures within 30 mmHg of diastolic pressure and intra-compartmental pressures between 30 mmHg and 45 mmHg. 11 In the patient reported above, he presented with features consistent with acute compartment syndrome of the right hand, which necessitated an urgent fasciotomy.
The authors aim to highlight the possibility of subcutaneous emphysema of the hand progressing to acute compartment syndrome especially in cases involving high-pressure pneumatic devices insufflating nitrogen gas. Clinical vigilance is advised despite literature generally suggesting conservative management for non-infectious subcutaneous emphysema cases of the upper limb.
Supplemental material
Supplemental Material, supplementary_material - A case of acute compartment syndrome of the hand complicating subcutaneous emphysema due to accidental nitrogen gas insufflation
Supplemental Material, supplementary_material for A case of acute compartment syndrome of the hand complicating subcutaneous emphysema due to accidental nitrogen gas insufflation by Collin SK Looi and Manohar Arumugam in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.