
Abstract
The injury mechanism of a case of hybrid Bado type I/III Monteggia fracture had been recorded live by the parent of a gymnast in a competition. This live recording was generously offered by the parent to the treating surgeon to study the injury mechanism. The video captured was segmented by slow motion frames to study the whole process of the injury mechanism. The injury mechanism was analyzed by the authors jointly to verify the interpretation of the loading mechanism and the resultant injury. The patient had been treated with conventional method with satisfactory result.
Keywords
Introduction
Giovanni Battista Monteggia first described this fracture pattern in 1814, 1 followed by many other authors publishing articles that theorized the mechanisms of the various types of Monteggia fractures. 2,3 Monteggia fractures are one of the most challenging ones to treat in children’s upper limb fractures. Bado termed the injuries as “lesions.” This is a more accurate term as these injuries are a combination of a fracture and dislocation. We will continue to use the term “lesion” in our discussion in this report. Bado had described the comprehensive injury types and the relationship between the ulnar angulation and the direction of the radial head dislocation. 4 Even with good history of fall from height in specific situation, the mechanism could not be appreciated as it occurred in a split second. 5 –7 Ethical approval was obtained from the ethics review board of the Joint NTEC/CUHK ethics committee. Written informed consent was obtained prior to collecting the video clip.
Case report
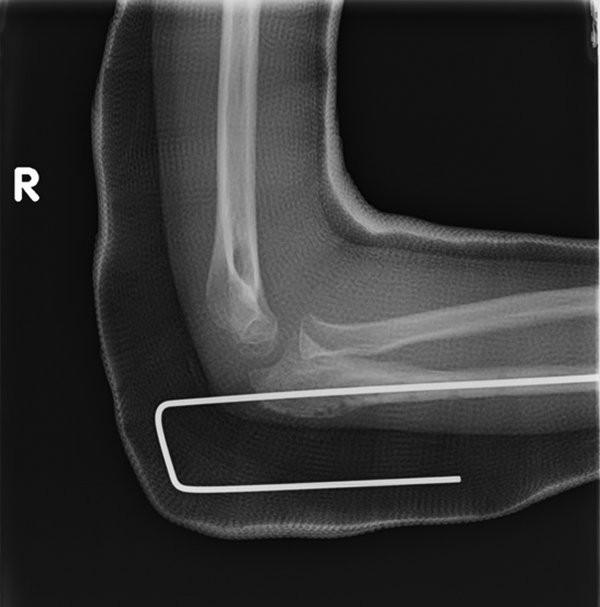
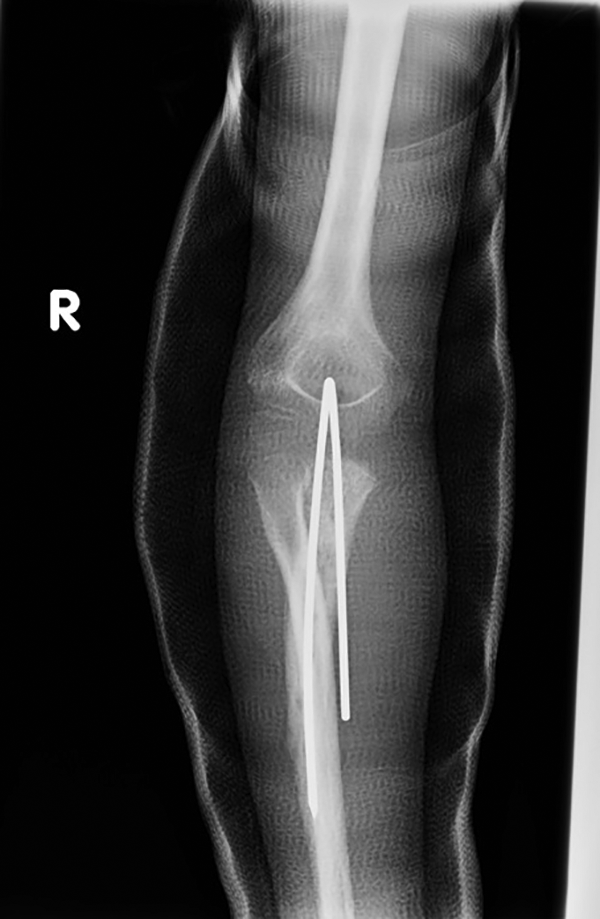
This is the first report describing the cause of Monteggia lesion in detail, through a sequence of action photos. A 15-year-old girl was participating in a gymnastic competition in a country away from her home city. Her parent accompanied her on that trip. The father of the patient had taken a video recording of his daughter during her performance. She was performing on a higher uneven bar coming to the end of the set exercise where she would swing high for a closing landing. She slipped off the uneven bar and fell forward landing on her back and arms. As a result, she injured her right elbow during the fall. She attended the accident and emergency department and was diagnosed to have a Monteggia fracture (Figures 1 and 2). The anterior and lateral dislocation of the proximal radius and the apex radial (varus) and anterior angulation of the proximal ulna confirmed that this was a type I/III Monteggia lesion. 8 –16 The patient also had a posterior interosseous nerve (PIN) palsy resulting in drop fingers and thumb. This was further confirmation that this was a hybrid type I/III lesion. Closed reduction was attempted at the attending hospital overseas and failed. The patient subsequently returned home and presented to a nearby hospital to continue with the definitive treatment. The patient was treated with attempted closed reduction again under general anesthesia which failed as well (Figure 3). Therefore, she underwent an open reduction and plating of the ulnar fracture which resulted in the restoration of the proximal radioulnar joint (PRUJ) alignment. Postoperatively the patient was treated with a dynamic splint for the PIN palsy and physical therapy. The PIN had recovered completely with the thumb extension having recovered by 5 months. With this history, the father was requested to provide the authors a copy of the video footage for the study of the injury mechanism. The important frames were selected to describe the injury mechanism.
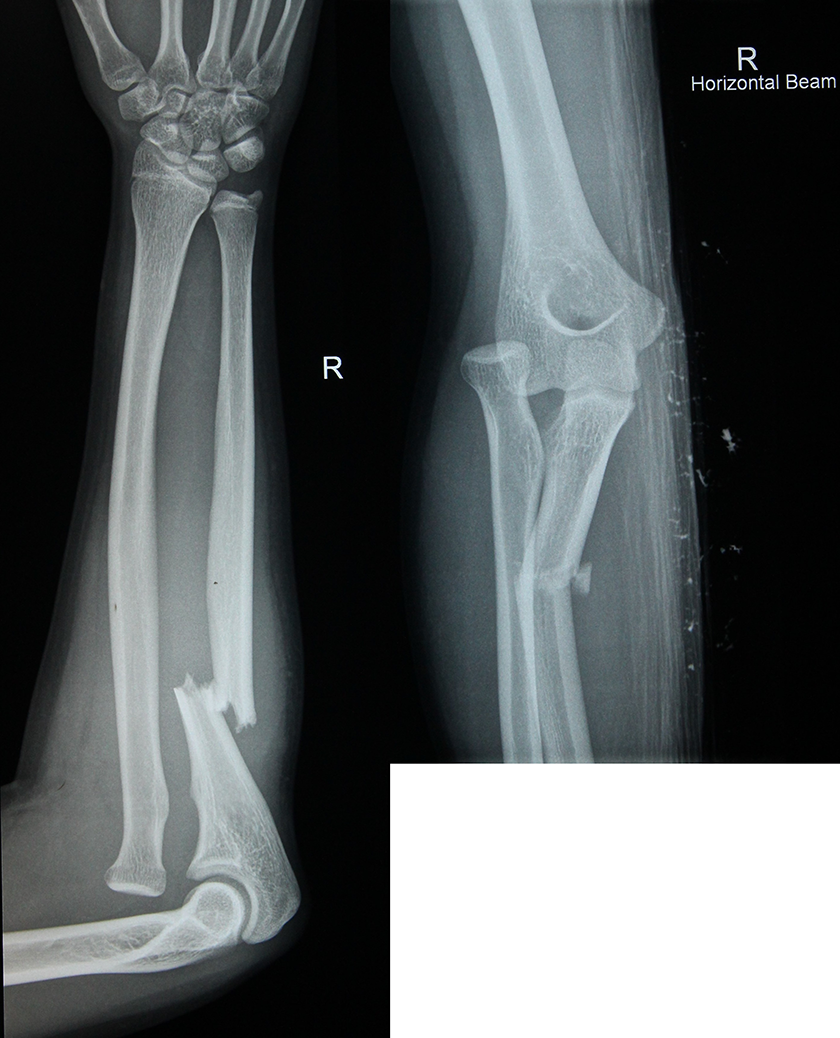
Anterioposterior (AP) and lateral X-rays of injured elbow.
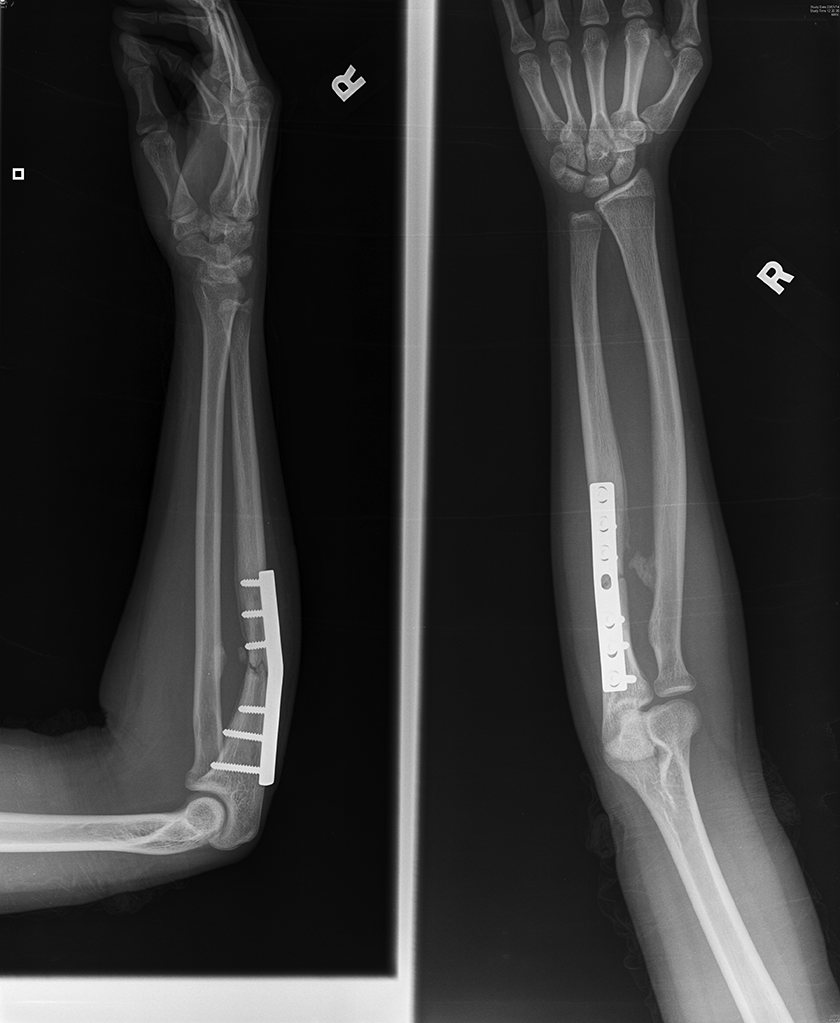
AP and lateral X-rays of elbow after open reduction and internal fixation of the ulnar fracture.
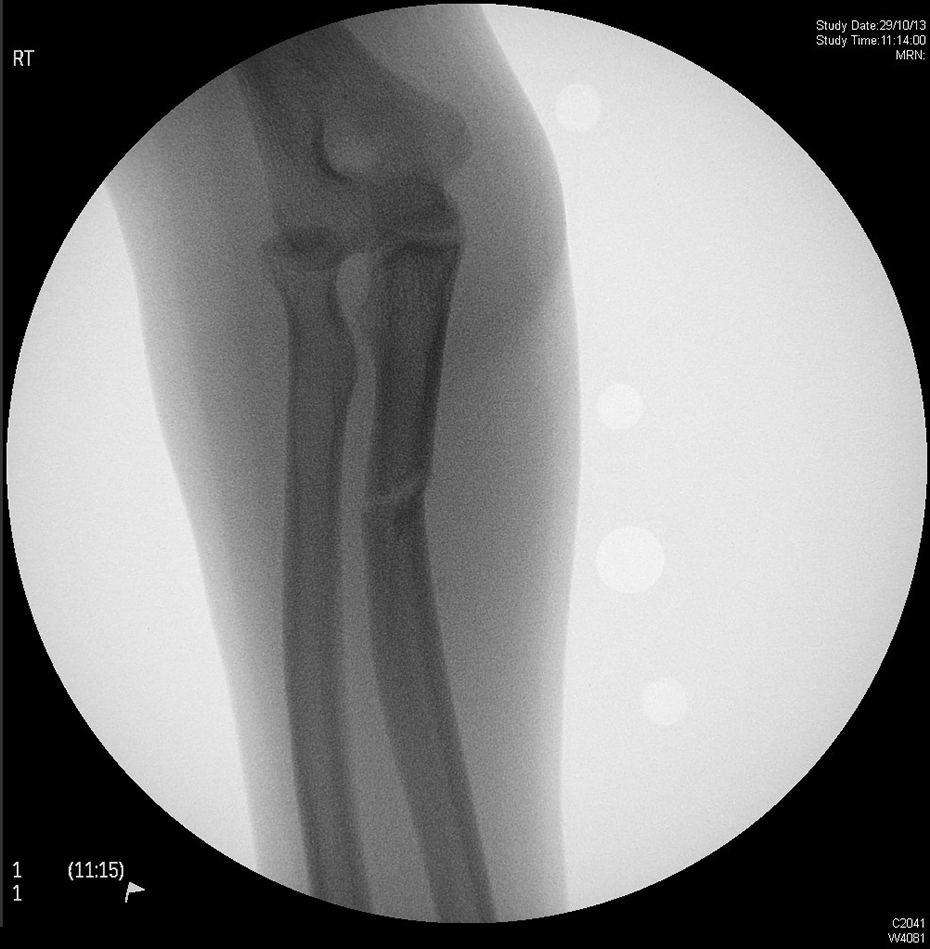
Intraoperative Fluoroscan.
Injury mechanism of a hybrid type I/III Monteggia lesion resulting from a fall from uneven bars
1. The falling position (Figure 4)

The falling position.
Patient was falling and forward in supine position, her arms were extended at shoulder 70° with elbow forward, hand pointing laterally indicating forearm in pronation. 17
2. First contact injured hand landing (Figure 5)

First contact injured hand landing.
The injured arm first contacted the mat with her hand and the elbow was in extension, the shoulder extension was reduced to 45° as the body continued to travel forward and descend. The elbow remained extended, the fingers were pointed lateral and forearm remained in a pronated position. The direction of the patient’s hair lashing back indicated the descending phase of the body.
3. Falling body loading to the pitching arm (Figure 6)

Falling body loading to the pitching arm.
The force of the loading of the falling body caused shoulder extension to become reduced to 20°. The elbow began to be hyperextended to 30°. The elbow appeared facing forward deforming the arm just below the elbow.
4. Just before body loading (Figure 7)

Just before body loading.
There was now further body loading with shoulder extension at 20° and elbow hyperextension to 70°. There was some external rotation of the arm.
5. Moment of sacral landing, maximal loading to arm, and first rebound (Figure 8)

Moment of sacral landing, maximal loading to arm, and first rebound.
The body had landed on sacrum. The shoulder extension was now reduced to 10°. The elbow hyperextension had now increased to 90° and there was a prominence on the lateral aspect of the pronated or changing position of the forearm. This was because now the body had reached ground which relieved the hand from loading. The hair had now lashed back.
6. Body and legs landing and second rebound (Figure 9)

Body and legs landing and second rebound.
The body continued to fall back and legs began to flex at the knees increasing the hip flexion to 135°. The shoulder extension remained at 20°. Elbow hyperextension deformity increased and forearm became flat on the ground and the legs continued to fall. The arm appeared to be rotated internally as indicated by the thumb position. The hand had now been released from the ground but was still in pronated position.
7. Patient righting reaction 1 (Figure 10)

Patient righting reaction part 1.
The patient began to lift her body up and the legs began to extend at the hip reducing the flexion. The shoulder was extended to 40°, the elbow hyperextension deformity had now been reduced to 90 and elbow became elevated from the ground. The arm appeared to be rotated internally. The hand remained released from the ground in pronated position.
8. Patient righting reaction 2 (Figure 11)

Patient righting reaction part 2.
The head extension was now reduced, as the patient was lifting her body. She was at the same time lifting and extending her legs more. The shoulder extension increased to 50°. The elbow hyperextension deformity was now reduced to 60 and elbow had become elevated from the ground. The arm appeared rotated internally. The hand was pitching the ground in pronated position again.
9. Patient righting reaction 3 (Figure 12)

Patient righting reaction part 3.
There was more body lifting and the legs began to be more extended, increased to 80°–90°. The shoulder extension increased at 70°, elbow hyperextension deformity reduced to 30, the arm appeared rotated internally presenting olecranon laterally with a distal deformity. The hand was pitching the ground in pronated position. It was at this point that the “varus” force was being applied to the proximal forearm.
10. Patient righting reaction 4 (Figure 13)

Patient righting reaction part 4.
There was further body lifting and legs were extended more at hips to 70° of flexion. The shoulder extension remained at 70°. The elbow hyperextension deformity was now reduced to 30°. The arm appeared rotated internally producing a prominence of the olecranon below the elbow. It appeared that there was more of a varus force applied at this point of her injury. It was at this point at which the elastic limit of the proximal ulna was breached and the cortices fail, to produce a varus angulated fracture pattern. The hand was pitching the ground in pronated position.
11. Patient righting reaction 5 (Figure 14)

Patient righting reaction part 5.
The body was lifting forward and the legs were further extended to 70° of flexion. The shoulder extension was increased to 70°–80°. The elbow hyperextension deformity had been reduced to 10°. The arm appeared rotated internally presenting olecranon and prominence below the elbow. Again the varus posturing of the proximal forearm was demonstrated. Hands were pitching the ground in pronated position.
12. Patient righting reaction 6 (Figure 15)

Patient righting reaction part 6.
The patient had lifted her body upright and her legs continued to extend to 50° of flexion. Her shoulder extension had been reduced from 80° to 70° and the elbow changed from a hyperextension deformity to a flexion position. The arm became rotated internally resulting in a prominence of the olecranon distal to the elbow. The hand was now lifted off the ground in a pronated position.
13. Complete landing (Figures 16 and 17)

Complete landing part 1.

Complete landing part 2.
Patient was now sitting upright and the legs extended at knee. The shoulder was now flexed to 30°. The elbow had now changed to a flexion position with the fracture extension deformity demonstrated below the elbow. The forearm was now held in neutral rotation. The fracture distal to the elbow was seen in extension and with varus deformity.
Discussion
The injury mechanisms of Monteggia lesions have been described in the literature based on historical accounts. With the increasing availability and high quality of audio–video equipment, more injuries are being recorded and their injury mechanisms can now be studied better with a frame by frame analysis which is far superior than a verbal account from patient or written descriptive account of an event by a witness. The verbal description or snapshot photo alone is difficult to comprehend. This case has demonstrated that the injury occurred in a very short space of time and with normal speed; therefore, it is very difficult to appreciate the interaction between the patient and the injuring force mechanism. The energy of the fall can be estimated from the body weight, height of the fall, and the speed at which patient has generated from the uneven bars. The force vector can be calculated at the point of loading which changes due to the motion of the shoulder and elbow joint through the range of maximal limits before the fracture occurs. The kinematics and the kinetic energy can both be estimated, although individuals react differently due to variations of muscular strength flexibility and muscle reaction characteristics. The clinical pattern will be similar as soon after this case the author had another younger male patient giving similar history of falling from a swing and sustaining a similar injury with more comminution. This younger patient also had a PIN injury. He was initially treated with open reduction with residual subluxation of the proximal radioulnar joint reduction. This could be due to insufficient correction of the ulnar deformity or from more disruption of the soft tissue that developed around the proximal radius. This was revised by reconstruction of the bone fragment followed by percutaneous K-wire fixation and careful repair of the ruptured periosteum which led to complete reduction of the PRUJ (Figures 18 to 20). The important information from determining the injury mechanism is that it can help understand what soft tissue will potentially be injured. This understanding of the mechanism of the injury can alert the surgeon to stay alert to those potential difficulties in fracture reduction. Although restoration of anatomy will be largely worked out by radiography with X-rays and MRI, the anticipation of the damaged tissue alerts us on the effect of the damaged soft tissue and their effects on the PRUJ alignment. Both patients had an uneventful healing of their fractures with a full recovery of the nerve palsy. The limitation in this analysis is that the video was taken of mainly the lateral view. Thus, only the vertical and lateral plane vectors could be analyzed. The coronal view could not be assessed and detail of how the hand twisted the forearm into varus position could not be determined.
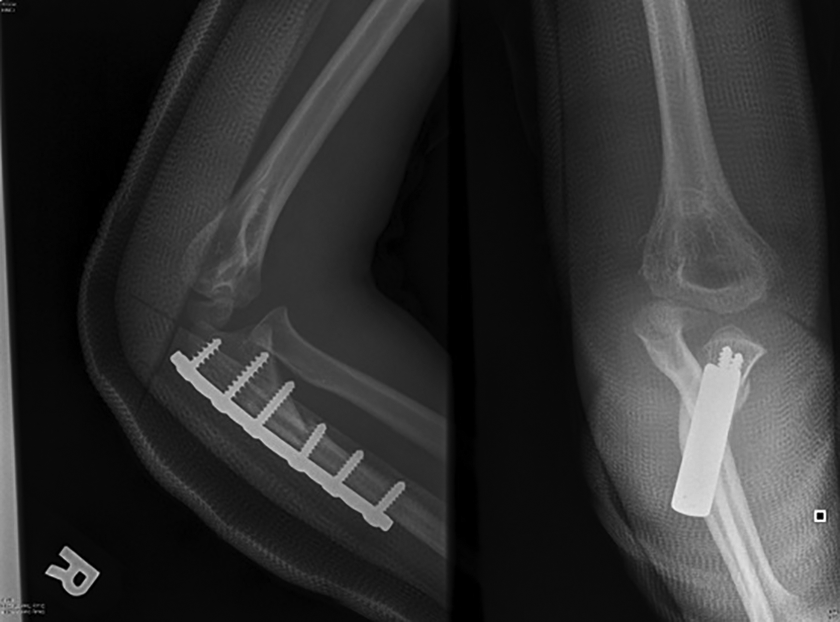
Post-op AP and lateral X-rays of young patient elbow showing proximal radioulnar joint still dislocated after open reduction and plating.
Postoperative lateral X-rays after revision of fracture reduction and fixation with intramedullary Kirschner wire.
Postoperative AP X-rays after revision of fracture reduction and fixation with intramedullary Kirschner wire.
Conclusion
This is the first report describing the cause of Monteggia lesion in detail through a sequence of action photos. Reporting this case has, we feel, illustrated that the hybrid Bado type I/III Monteggia fracture occurs because of patient falling forward from height landing in supine position on outstretched hands with arms extended at shoulders and elbow. The pitching outstretched hand of the injured elbow caused an extreme hyperextension of the arm and an asymmetric loading on the injured side most likely producing a varus stress resulting in such injury associated with PIN palsy. Developing an understanding of the soft tissue injury can be an aid to treatment ultimately which should lead to a better restoration of the PRUJ alignment.
We feel that the case confirms the original mechanism of Wright in 1963 that the ulna fails first with a hyperextension and varus force followed by a subsequent lateral dislocation of the proximal radius. 18,19 The author would like to thank the generous offering of the video material from the patient and her father’s high-quality editing of the original video into frame on frame pictures and detailed study of such injury.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.