
Abstract
Background/Purpose:
Laminotomy is an established procedure to relieve symptoms of lumbar spinal stenosis. However, there is a group of patients with symptomatic recurrence. Re-decompression and fusion could be an effective salvage procedure but the results are seldom found in the literature. In this study, we focused on investigating the clinical outcomes and complication rates of revision decompression with fusion in this patient group.
Methods:
A retrospective study including patients who had undergone revision decompression with fusion for recurrent symptoms due to same level restenosis after primary laminotomy for lumbar spinal stenosis was performed. Patients with recurrent symptoms due to prolapsed intervertebral disc, trauma, infection, and neoplasm were excluded. Demographics, clinical outcomes, and complications were retrieved.
Results:
Twenty-eight patients with a total number of 42 levels of revision decompression and fusion were included. With a mean follow-up time of 27 months after revision surgery, there were statistically significant improvement of 63, 49, and 13% in Japanese Orthopaedic Association score, visual analog scale for leg pain, and Roland-Morris disability questionnaire score, respectively. There were 6(21%), 2(7%), 0(0%), and 2(7%) cases of dural tear, infection requiring reoperation, new neurological deficit, and other complications, respectively, in these revision cases.
Conclusion:
Bearing potential complications in mind, re-decompression with fusion is a viable option with reasonable clinical outcomes for patients with recurrent symptoms after laminotomy for lumbar spinal stenosis. As a treatment option for symptomatic lumbar spinal stenosis, primary laminotomy could have the potential benefit of lower complication rates in revision surgery.
Introduction
Lumbar spinal stenosis is a condition of lumbar spinal canal narrowing resulted from various possible causes. Patients suffering from lumbar spinal stenosis could have symptoms of back pain, leg pain, claudication, and impaired daily function. Surgical decompression is an effective procedure to relieve these symptoms. 1 However, there is a group of patients who did not have sustained relief of these symptoms after decompression surgery. 2 The success rate of revision surgery for this group of patients has been highly variable, ranging from 22% to 82% in different reports. 3 –8 A consensus has not yet been reached regarding the management of this group of patients with recurrence of symptoms.
Previous reports 3 –13 of clinical outcomes after revision lumbar spinal surgery included patients with different types of primary surgery performed, different causes of recurrent symptoms, and different types of revision surgery performed. The clinical outcomes of revision decompression with fusion for same level restenosis after laminotomy for lumbar spinal stenosis were poorly studied.
In this study, we focused on investigating the clinical outcomes in this patient population. This study also analyzes the complication rates of revision decompression with fusion in this patient group. Complication rates in primary decompression with fusion for symptomatic lumbar spinal stenosis, without prior lumbar spinal surgery, were also analyzed. Complication rates of revision surgery group and primary surgery group were compared.
Method
Patient selection
Of the 429 patients underwent primary laminotomy for symptomatic lumbar spinal stenosis in our institution from 1999 to 2016, 28 (6.25%) patients who had undergone revision decompression with fusion for recurrent symptoms after primary laminotomy were included in this study.
The inclusion criteria were (1) prior laminotomy for lumbar spinal stenosis, (2) recurrent back pain or claudication symptoms, (3) same level restenosis confirmed with radiological studies (X-ray, computed tomography, and magnetic resonance imaging). Patients were excluded if the recurrent symptoms were due to causes, such as prolapsed intervertebral disc, trauma, infection, neoplasm, and adjacent level disease. All patients had conservative treatment for the recurrent symptoms for more than 6 months. All patients underwent revision decompression with fusion for the recurrent symptoms.
Patient-reported outcome measures, as well as objective outcome measures, were collected in the outpatient clinic during patient follow-up. Patient demographics, clinical condition before reoperation, and operative variables were retrospectively reviewed. Intraoperative variables and postoperative complications were also reviewed.
One hundred and seventy-six patients who had undergone primary decompression with fusion for lumbar spinal stenosis during the same time period in our institution were included in this study as the control cohort. The inclusion criteria were (1) decompression and fusion for lumbar spinal stenosis, (2) back pain or claudication symptoms present, and (3) no prior lumbar spinal surgery. Patients were excluded for causes, such as infection, trauma, neoplasm, and prolapsed intervertebral disc. Intraoperative variables and postoperative complications were reviewed. Indications for spinal fusion in this patient group included the presence of symptoms arising from elements, such as degenerative disc disease, spondylolisthesis, and preoperative or intraoperative spinal instability.
Clinical outcome measure
Prerevision surgery and postrevision surgery outcome measures were collected at clinic follow-ups before and after revision surgery. After 2004, all data including complications and clinical outcome measures were collected prospectively.
Patient-reported outcome measures such as subjective overall improvement, regret of undergoing revision surgery, Roland-Morris disability questionnaire score (RMDQ), 9 Oswestry disability index score (ODI), 10,14 visual analog scale for back pain (VAS-back), 15 and VAS for leg pain(VAS-leg) 16 were collected. Objective outcome measure, such as Japanese Orthopaedic Association (JOA) score, 17,18 was also collected. These scores were retrieved from respective patients’ medical records for analysis retrospectively.
Intraoperative variables and postoperative complications in revision decompression with fusion group and primary decompression with fusion group were analyzed. Intraoperative variables and complications such as dural tear, blood loss, and operation time were collected during the perioperative period during hospitalization. Postoperative complications rates such as infection requiring reoperation, new neurological deficit, and others (including pedicle fracture, implant failure, wound infection, wrong level, delirium) were collected during perioperative hospitalization period and postoperative follow-ups in the clinic. These data were retrieved from respective patients’ medical record for analysis retrospectively.
Statistical analysis
Statistical analysis was performed with commercially available software (SPSS). Statistical significance was set at p < 0.05. Parametric data were presented with mean ± standard deviation (SD) and were compared with paired or unpaired t-test. Nonparametric data were presented with median and compared with Wilcoxon rank sum test or Mann–Whitney U-test. Nominal data were compared with the chi-square test.
Results
Twenty-eight patients with recurrent symptoms of lumbar spinal stenosis after laminotomy were included in this study. All of them had radiographic evidence of same level restenosis and had conservative treatment for more than 6 months. Mean ± SD (range) age of patients was 62 ± 8 (49–74) years (Table 1). There were 18 males (64%) and 10 females (36%). L4/5 (64%) was the most frequently involved level. The mean ± SD (range) JOA score, VAS-back, VAS-leg, ODI score, and RMDQ score immediately before revision surgery were 14.0 ± 4.6 (6–23), 4.8 ± 3.2 (0–10), 6.7 ± 3.2 (0–10), 48.9 ± 17.8 (10–74), and 15.8 ± 4.6 (6–21), respectively.
Demographics and clinical condition of 28 patients immediately before revision surgery.
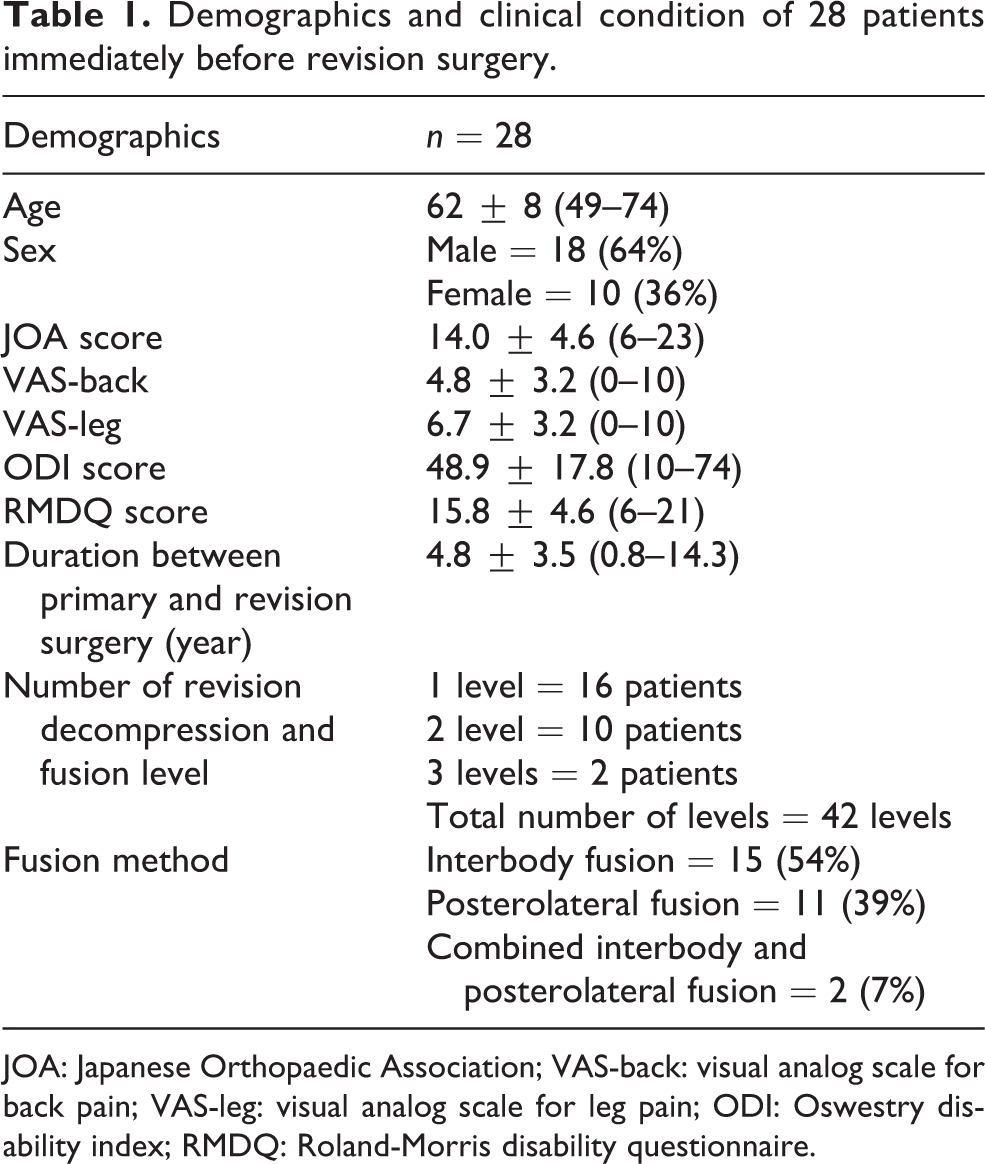
JOA: Japanese Orthopaedic Association; VAS-back: visual analog scale for back pain; VAS-leg: visual analog scale for leg pain; ODI: Oswestry disability index; RMDQ: Roland-Morris disability questionnaire.
All patients underwent revision decompression with fusion. The mean duration between primary surgery and revision surgery was 4.8 ± 3.5 (0.8–14.3) years. Pedicle screw system was used in all cases. Fifteen (54%) patients underwent interbody fusion of the involved segments with polyetheretherketone cage and bone autograft, while 11 (39%) underwent posterolateral fusion with bone autograft and 2 (7%) underwent combined posterolateral and interbody fusion. Transforaminal interbody fusion was performed in patients to relieve back pain from degenerative discs, decompress foraminal stenosis, restore sagittal alignment, or provide more rigid construct with intraoperative spinal destabilization during posterior decompression.
Clinical outcomes
The mean follow-up time for 28 patients was 27 ± 26 (2.4–67.1) months. At latest follow-up, significant improvement in mean JOA score, VAS-leg pain, and RMDQ scores was observed when compared with pre-reoperation level. The mean improvement (Table 2) in JOA score, VAS-leg pain, and RMDQ score was 6.4 (63%) ± 5.0 (p < 0.05), 3.3 (49%) ± 3.3 (p = 0.001), and 2.4 (13%) ± 4.0 (p = 0.024). The mean improvement in VAS-back and ODI score was 1.7 (26%) (p = 0.078) ± 4.1 and 8.8 (3%) (p = 0.71) ± 21.7. The mean subjective overall improvement was 56% and none of the patients expressed regrets for having revision surgery (Table 3).
Difference in prerevision and postrevision scores with a mean follow-up of 27 months.
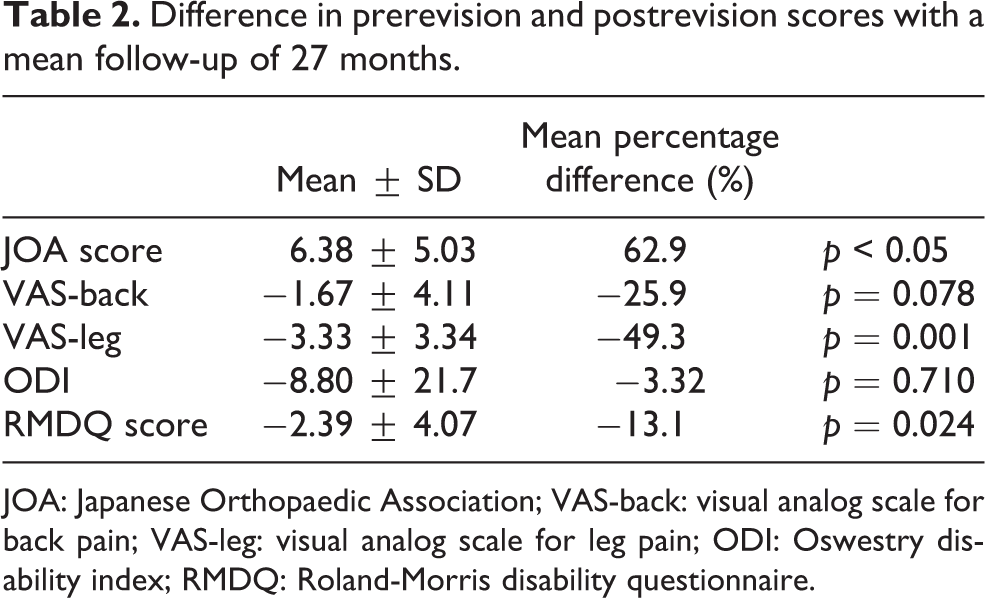
JOA: Japanese Orthopaedic Association; VAS-back: visual analog scale for back pain; VAS-leg: visual analog scale for leg pain; ODI: Oswestry disability index; RMDQ: Roland-Morris disability questionnaire.
Demographics and clinical condition of patients underwent revision and primary decompression with fusion for symptomatic lumbar spinal stenosis.a
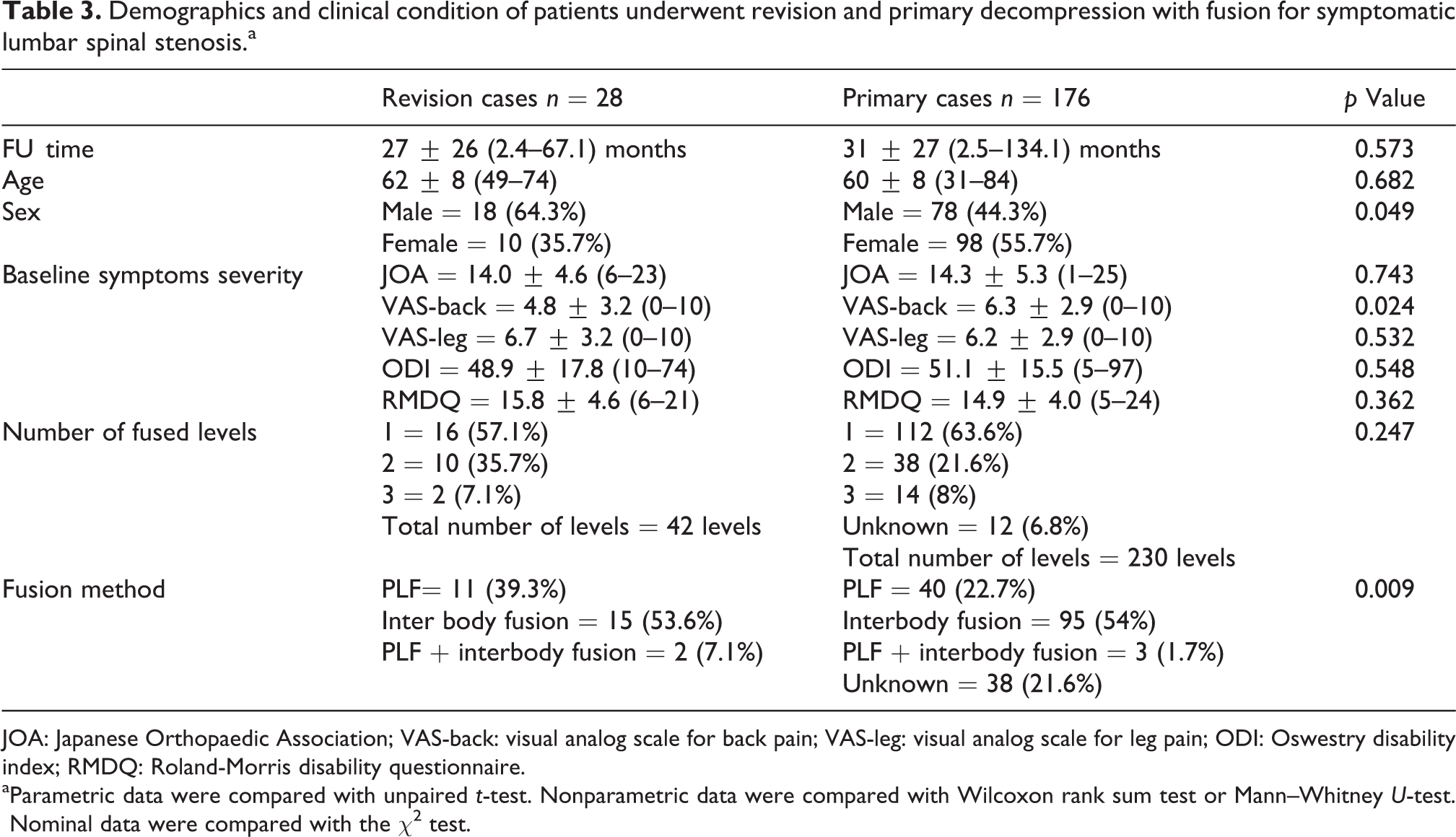
JOA: Japanese Orthopaedic Association; VAS-back: visual analog scale for back pain; VAS-leg: visual analog scale for leg pain; ODI: Oswestry disability index; RMDQ: Roland-Morris disability questionnaire.
aParametric data were compared with unpaired t-test. Nonparametric data were compared with Wilcoxon rank sum test or Mann–Whitney U-test. Nominal data were compared with the χ2 test.
The mean scores at 6, 12, 18, and 24 months were shown in Figure 1.
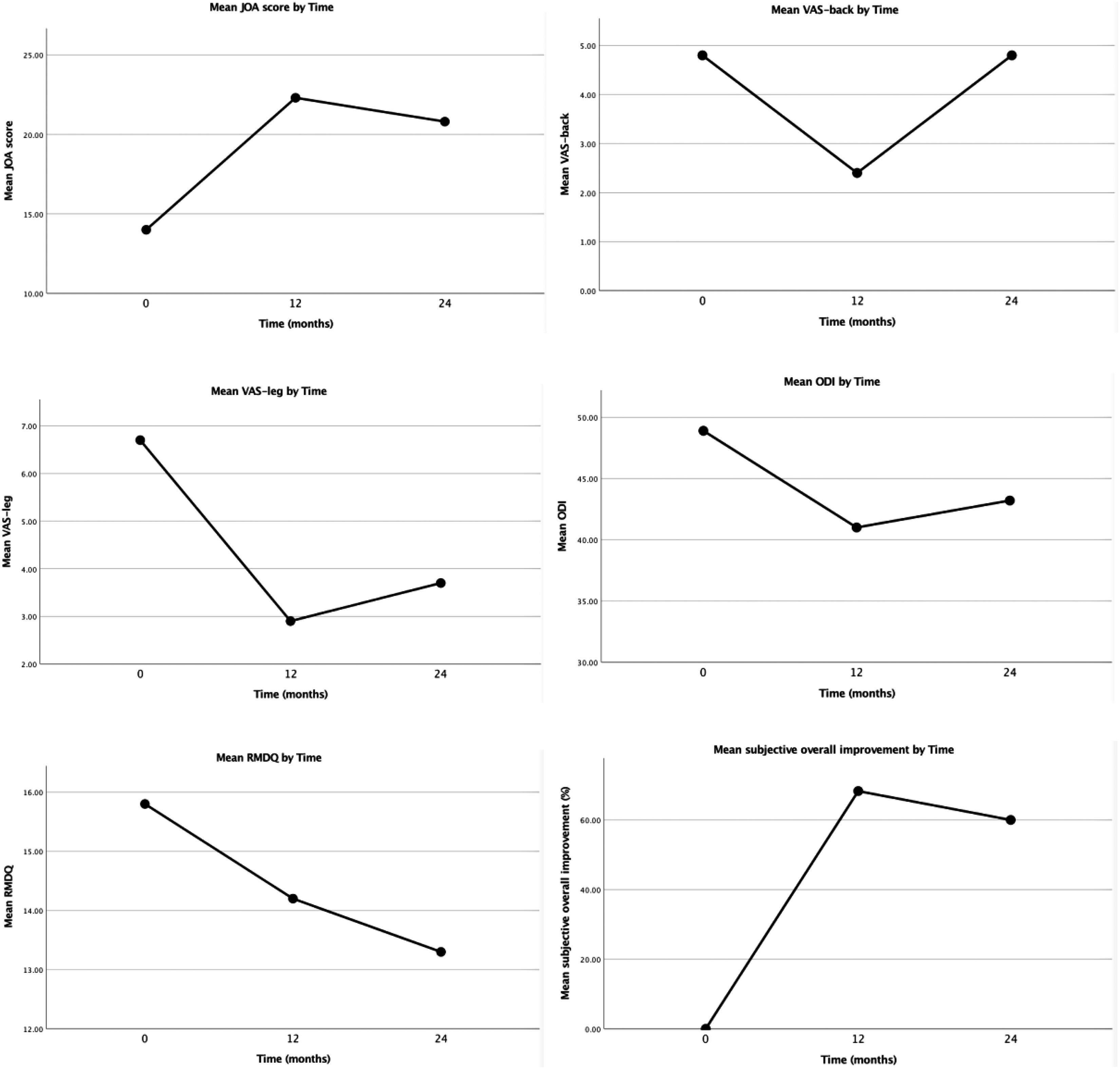
Graphs showing mean JOA score, VAS-back, VAS-leg, ODI, RMDQ, and subjective overall improvement at 12-month and 24-month postrevision surgery. JOA: Japanese Orthopaedic Association; VAS-back: visual analog scale for back pain; VAS-leg: visual analog scale for leg pain; ODI: Oswestry disability index; RMDQ: Roland-Morris disability questionnaire.
Complications (Table 4)
Complication rates of revision and primary decompression with fusion for symptomatic lumbar spinal stenosis.a
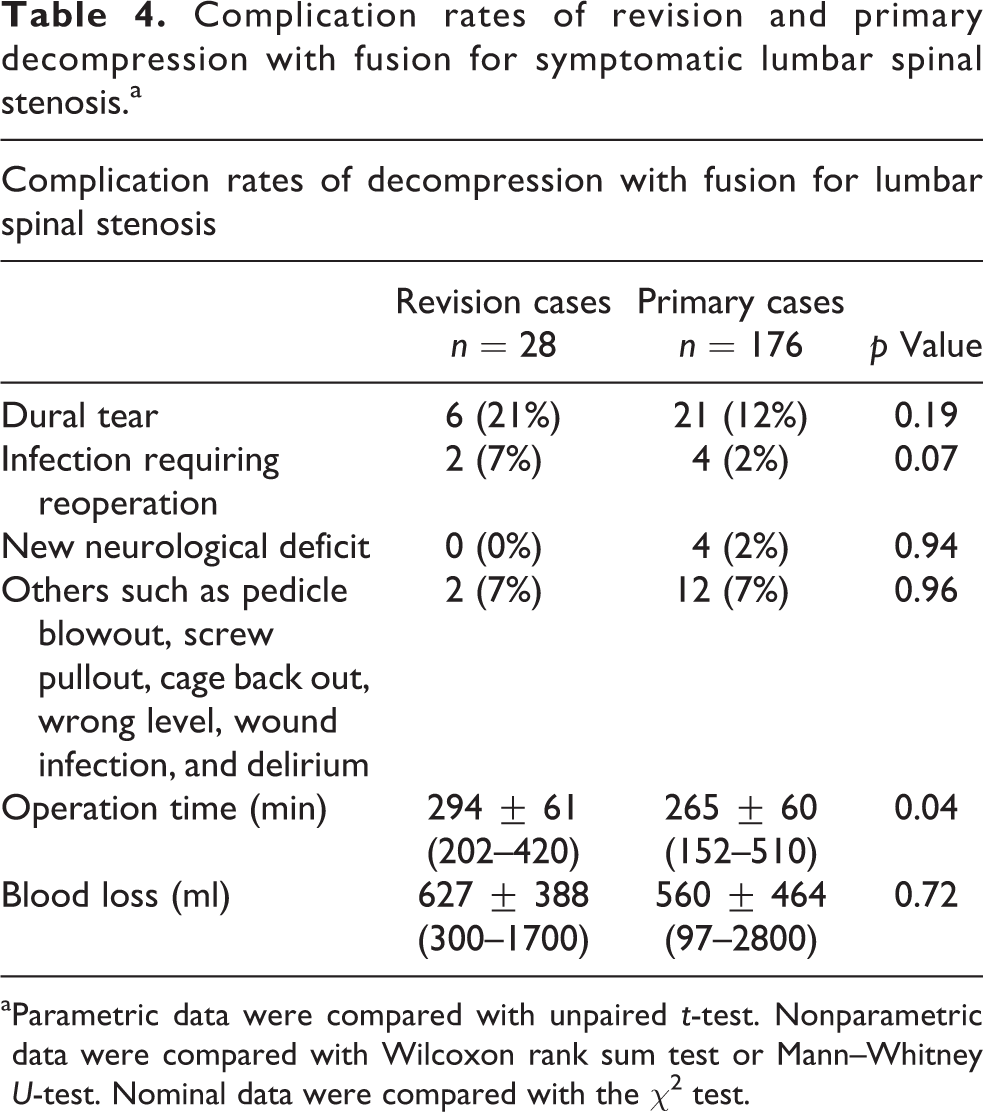
aParametric data were compared with unpaired t-test. Nonparametric data were compared with Wilcoxon rank sum test or Mann–Whitney U-test. Nominal data were compared with the χ2 test.
Eighteen (64%) patients, who had undergone revision decompression and fusion, had no intraoperative or postoperatively complications. There were six (21%) cases of dural tear intraoperatively. There were two (7%) cases of infection requiring reoperation. There were one (3.5%) case of pedicle blowout and one (3.5%) case of screw pullout. There were no salvage operations deemed necessary, except the aforementioned two cases of infection, for these complications. The mean ± SD operation time taken was 294 ± 61 min. The mean ± SD intraoperative blood loss was 627 ± 388 ml.
In the control group of 176 patients who had undergone primary decompression with fusion for lumbar spinal stenosis in our institution during the same time period as the revision cases, 132 (75%) of them had no intraoperative or postoperative complications. There were 21 (12%) cases of dural tear and 4 (2%) cases of infection requiring reoperation. There were three (2%) cases of postoperative new neurological deficit. There were 12 (7%) cases of other complications, including wrong level, wound infection, pedicle blowout, cage back out, and delirium. The mean ± SD intraoperative blood loss was 590 ± 464 ml. The mean ± SD operation time taken was 265 ± 60 min.
Discussion
This study shows that revision decompression with fusion is an effective treatment for recurrent symptoms after laminotomy for lumbar spinal stenosis. With a mean follow-up of 29 months, there was a significant improvement in leg pain measured by VAS-leg for 49%, in symptoms and functions measured by JOA score for 63%, and in disability measured by RMDQ score for 13%. None of the patients expressed regrets for having the revision surgery and the mean subjective overall improvement is 56%. Furthermore, there was no statistically significant difference in the amount of blood loss and intraoperative or postoperative complication rates when compared with primary surgery cases, except that it required significantly longer operation time.
Clinical outcomes of revision lumbar spinal surgery have been reported in previous studies. 3 –8 However, the majorities of these reports included heterogeneous group of patients with different primary surgery performed, different revision surgery undergone, and different causes for reoperation. And the success rates in these reports range from 22% to 82%. One of the logical reasons for the variability of success rate could be the heterogeneity of patient groups and revision surgery. It is difficult to ascertain the effectiveness of a specific type of revision surgery for specific patient groups and guide clinical management. Further research of revision spinal surgery in different patient groups is needed to formulate a reasonable approach of managing recurrent symptoms in different patient populations. Mendenhall et al. 11 reported favorable outcomes in patients who had undergone revision decompression and fusion for recurrent symptoms due to same-level restenosis with prior laminectomy. They reported significant improvement in back and leg pain, disability, and mental health symptoms in these patients after 2 years of follow-up. For patients with prior laminotomy done for symptomatic lumbar spinal stenosis and recurrence of symptoms, there is a paucity of studies reporting outcomes of revision surgery in this patient group. Our study showed that revision decompression with fusion is an effective option for them.
Higher risk of complications in revision spinal surgery had been reported in previous studies. 19 –26 This could be explained by the distortion of anatomy and soft tissue from primary surgery. Devascularization of soft tissue is often present in the previous surgical wound, which could affect wound healing and predispose to wound infection after revision lumbar surgery. Patients with higher comorbidities are also at a higher risk of postoperative superficial and deep infections. 19 Epidural fibrosis and scarring is also an important contributing factor to postrevision surgery complications. The scarring and adhesions require meticulous surgical techniques to detach them from neural tissue in order to obtain adequate decompression. In our study, there is no statistically significant difference in complication rates, in terms of complication rates of dural tear, infection requiring reoperation, and new neurological deficit. This could be a result of reduced distortion of anatomy and soft tissue in the primary laminotomy surgery when compared with primary laminectomy as in other studies. Revision decompression and fusion required longer operation time than primary cases in this study, though the amount of blood loss is similar.
Proper patient selection, identification of the underlying cause of recurrent symptoms, and adequate preoperative clinical and radiological assessment are crucial for the success of revision spinal surgery. 11,26 As revision spinal surgery carries a significant risk of complication, adequate conservative treatments including medications and physiotherapy should be offered before proceeding to surgical intervention. In our study, the mean duration between primary and revision surgery is 4.8 years. It lies well within ranges in other reported series, 5,11,13,27,28 which suggests that the experience in our institution may be representative of others’.
There are several limitations in this study. The first one is that this is a retrospective study. Data including clinical outcomes and perioperative variables were retrospectively retrieved from patient’s medical records, although they were collected at the time of revision surgery and during postoperative follow-up in the clinic. Secondly, there is a lack of control group for comparison of clinical outcomes with other treatments. Thirdly, the clinical outcome measures were collected in the spine clinic mainly by spine surgeons, who may or may not be the one performing the revision surgery. And the sample size of this study is relatively small and this could also well explain the lack of statistically significant increase in complication rates compared to primary surgery. Further prospective, controlled, large-scale studies are warranted for evaluating the effectiveness of revision decompression with fusion in this patient group. Despite all these limitations, our study adds valuable series to the limited amount of data regarding the results of revision surgery in this patient group.
Conclusions
Bearing potential complications in mind, re-decompression with fusion is a viable option with reasonable clinical outcomes for patients with recurrent symptoms after laminotomy for lumbar spinal stenosis. As a treatment option for symptomatic lumbar spinal stenosis, primary laminotomy could have the potential benefit of lower complication rates than primary decompression with fusion due to the less extensive nature of surgery. And it carries a potential benefit that effective salvage surgery (e.g. re-decompression with fusion) was available for recurrent symptoms.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.