
Abstract
Objective:
To explore the prevalence and variations of toe symphalangism in the Hong Kong Chinese population.
Methods:
A retrospective review of foot radiographs taken in Chinese adult patients admitted to United Christian Hospital from 1 January, 2016 to 31 December, 2016. Exclusion criteria include (1) previous toe amputation, (2) skeletal immaturity, (3) severe deformity, and (4) repeated attendance. The frequencies were compared by χ 2 test.
Result:
A total of 1364 foot radiographs were reviewed. Six-hundred sixty radiographs were excluded. A total of 704 radiographs were included in this study. There were total 849 feet reviewed (left: 290, right: 269, bilateral: 145). Their mean age (± standard deviation) was 59.5 ± 14.2 years. The prevalence of 2nd, 3rd, 4th, and 5th toe symphalangism was 0.2%, 0.8%, 9.9%, and 76.7%, respectively. The prevalence resembles Asian population. There was no significant difference in the prevalence associated with the following factors: (1) gender and (2) left versus right foot. There was no 4th toe symphalangism without 5th toe involvement. In the 145 bilateral feet radiographs, asymmetrical distribution of toe symphalangism was found in 8.2%. Second toe symphalangism is rare (0.24%).
Conclusion:
This is the first study in Hong Kong to report prevalence of toe symphalangism in Chinese population. There is a high prevalence rate of 5th toe symphalangism in the Hong Kong Chinese Population. This implies less flexible lesser toes in the Chinese population with higher risks of development of deformities. The clinical implication of such findings needs further research.
Keywords
Introduction
Toe symphalangism refers to end-to-end synarthrosis of intermediate and distal phalanges of lesser toes (Figure 1). It is also referred as “two-phalanged toes” or “biphalangia.” Pedal symphalangism was first described by Leonardo da Vinci in 1492. There are two proposed theories: (1) incomplete segmentation with failure of development of distal interphalangeal joint and (2) fusion of middle and distal phalanxes. 1 This phenomenon receives limited attention as it does not cause dysfunction. Symphalangism is believed to be genetically determined. Its incidence was observed from 35% to 80%, being less common in Caucasian and more common in Asian. It is most commonly found in 5th toe. However, it may also be found in more medial digits up to and including 2nd toe. From previous observations, it is not present in a medial digit unless its immediate lateral digit is also involved. 2 It can be found as isolated condition or with other congenital malformation including fusion of tarsal bones or interphalangeal joint of fingers. 3 To best of our knowledge, there is no study on its prevalence in Hong Kong Chinese population. The objective of this study would be to explore the prevalence and variations of toe symphalangism in the Hong Kong Chinese population.

(Left) Biphalangeal toe (Right) Triphalangeal toe.
Methods
A retrospective review of foot radiographs taken in Chinese adult patients for all possible indications admitted to United Christian Hospital from 1 January, 2016 to 31 December, 2016. Exclusion criteria include (1) previous toe amputation, (2) skeletal immaturity, (3) severe deformity that precluded accurate interpretation, and (4) repeated attendance (Figure 2(a) to (c)). The data were retrieved from Clinical Data and Reporting System and Clinical Management System. The presence of toe symphalangism and its distribution were recorded and analyzed by three independent investigators. Any discrepancy was discussed to achieve consensus prior to the calculation of prevalence. Radiologists were not included in the analysis because the identification of toe symphalangism in this study encountered minimal difficulty.
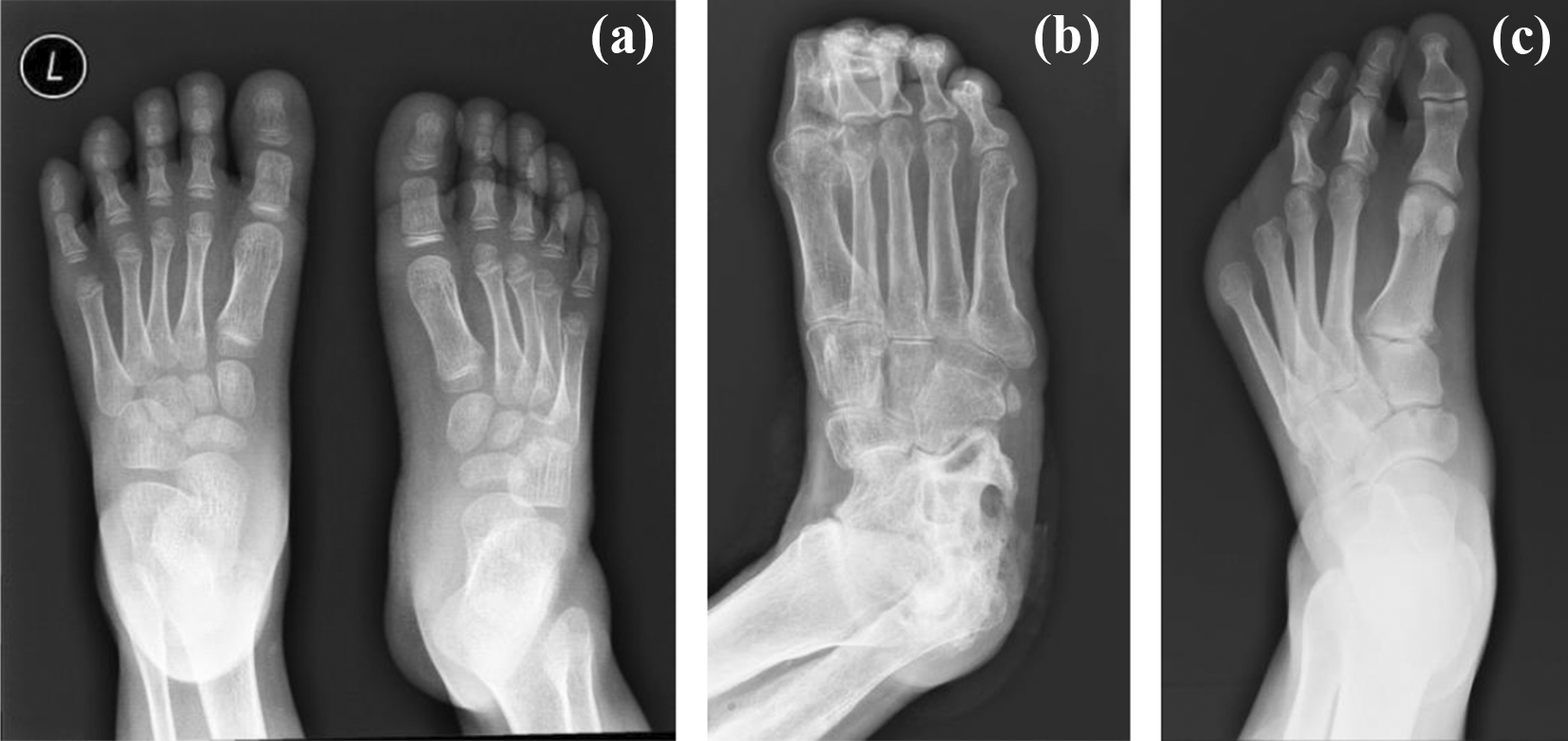
Examples of radiographs being excluded: (a) Pediatrics, (b) severe deformity that affects interpretation, and (c) previous amputation.
A total of 1364 foot radiographs were reviewed. Six-hundred sixty radiographs were excluded and a total of 704 radiographs were included in this study. Radiographs were available in dorsoplantar and dorsoplantar oblique view. Statistical analysis was performed using χ 2 test, and a p value <0.05 was considered statistically significant.
Results
A total of 704 subjects were included with 366 (51.9%) being male patients and 338 (48.1%) being female patients. Their mean age (± standard deviation) was 59.5 ± 14.2 years. There were total 849 feet reviewed (left: 290, right: 269, bilateral: 145). The overall prevalence of 2nd, 3rd, 4th, and 5th toe symphalangism was 0.2%, 0.8%, 9.9%, and 76.7%, respectively. The percentage incidence pedal symphalangism on each side is shown in Figure 3.

Distribution of biphalangeal toes in each foot.
The frequency of pedal symphalangism of each digit in both male and female is shown in Table 1. There was no significant difference in the prevalence associated with the following factors: (1) gender and (2) right versus left foot.
aPrevalence and distribution of pedal symphalangism of each digit with respect to gender.
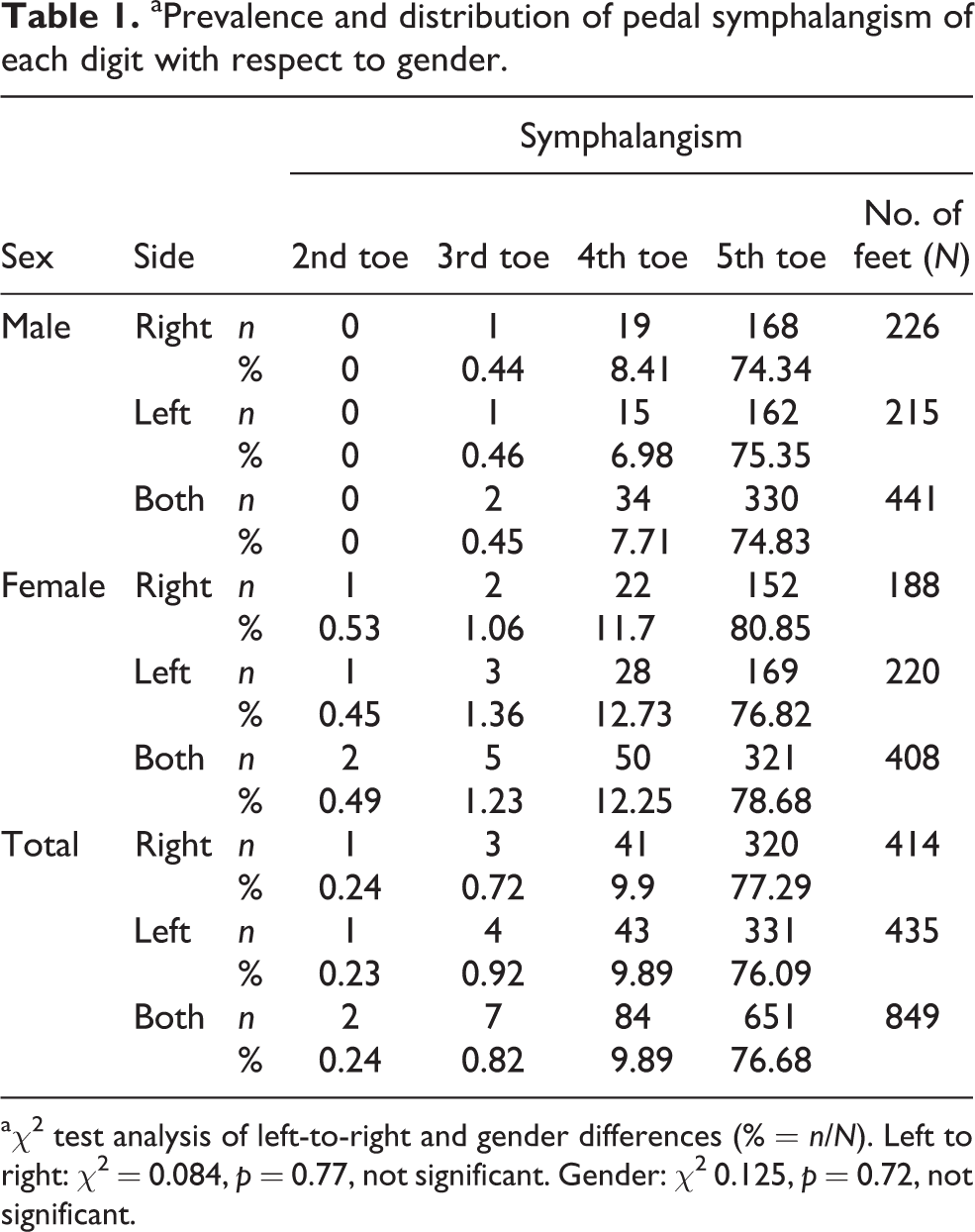
a χ 2 test analysis of left-to-right and gender differences (% = n/N). Left to right: χ 2 = 0.084, p = 0.77, not significant. Gender: χ 2 0.125, p = 0.72, not significant.
Pedal symphalangism is not observed in a medial digit unless its immediate lateral digit is also involved, that is, there was no 4th toe symphalangism without 5th toe involvement.
In the 145 bilateral foot radiographs available, 35 (24%) showed no toe symphalangism, 85 (58.6%) showed bilateral 5th toe symphalangism, 11 (7.6%) showed bilateral 4th + 5th toe symphalangism, 1 (0.69%) showed bilateral 3rd + 4th + 5th toe symphalangism, 1 (0.69%) showed bilateral 2nd + 3rd + 4th + 5th toe symphalangism, and 12 (8.2%) showed asymmetrical involvement.
Discussion
This is the first and only study to report the prevalence and pattern of toe symphalangism in Hong Kong Chinese population. China is a big country and Hong Kong is located in the southeast area of China. The population in Hong Kong could be different from that in the northern part of China. For example, population in northern part of China are taller than those in the southern part. From our study, the samples are taken from Hong Kong. It is an extremely common anatomical variation among this population with overall prevalence of symphalangism in 5th toe being 76.68%, 4th toe being 9.89%, 3rd toe being 0.82%, and 2nd toe being 0.24%. Symmetrical involvement is more frequent than asymmetrical distribution.
Concerning laterality in toe symphalangism, no significant left-to-right difference in the percentage was observed in previous studies. 3,4 Current study is line with this result (left-to-right difference, p = 0.77).
Differences in toe symphalangism with respect to gender difference have been reported in former studies. Some studies revealed no sex difference in incidence 2,3 while some concluded that biphalangeal toes were more frequently found in women. 5,6,7 In present study, there is no significant difference in prevalence observed associated with gender (gender difference, p = 0.72).
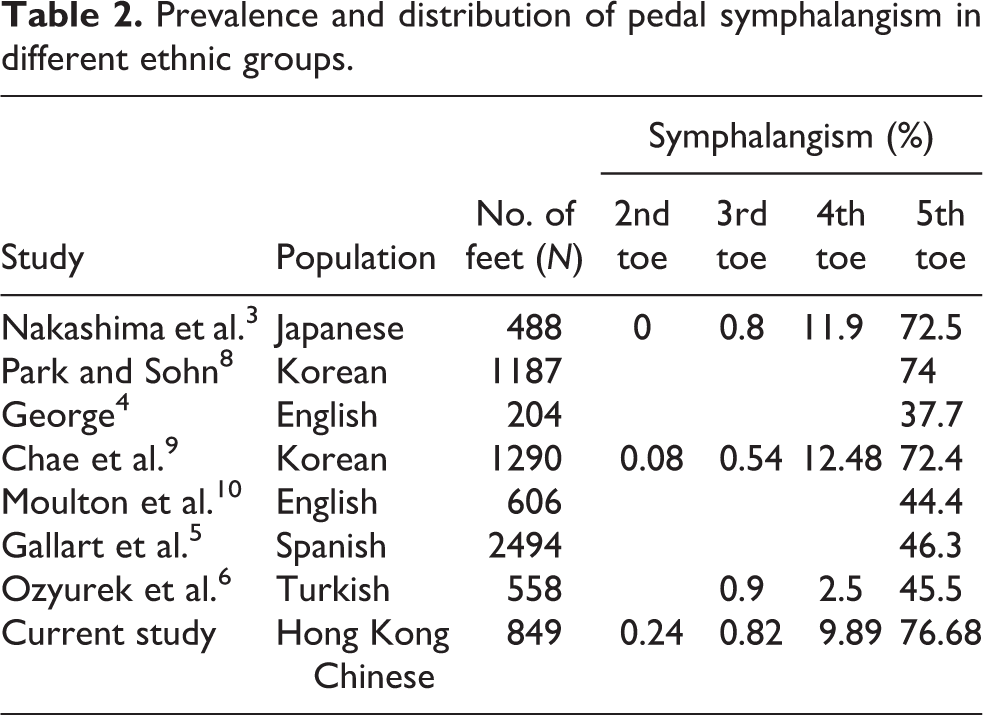
Previous radiographic and cadaveric studies have reported the prevalence and distribution of toe symphalangism in different ethnic groups. Their results are summarized in Table 2. The overall prevalence of 5th symphalangism in Asian population has been reported to be around 70% while that in Caucasian population was around 40%. In our findings, the prevalence of toe symphalangism in Hong Kong Chinese population resembles the findings in Asian populations. 3,8,9
Prevalence and distribution of pedal symphalangism in different ethnic groups.
Conflicting results on symmetrical involvement of pedal symphalangism were described. While George 4 reported symmetrical involvement in all subjects, Moulton et al. 10 stated 4.8% and Ozyurek et al. 6 stated 10.5% asymmetrical distribution. In the current study, 12 (8.2%) in 145 films showing bilateral feet had different numbers of phalanges in either foot (Figure 4).

Asymmetrical involvement of pedal symphalangism.
Second toe symphalangism (Figure 5) is known to be a rare phenomenon. Its prevalence ranges from 0% to 0.1% as stated in previous papers. 3,11 In the present study, its frequency is 0.24%, which is slightly higher comparing to former studies.

Second toe symphalangism.
With loss of flexibility created by this synostosis, Banks stated that it is often more difficult for the digit to accommodate irritation from shoes and it therefore predisposes the 5th toe to the development of painful pressure keratosis or nail dystrophy. 12 Besides, Dereymaeker concluded that the prevalence of biphalangeal 5th toe in patients with hammer or claw toes was significantly higher than that in the control group. 13 This was not observed in patients with bunionettes or overriding 5th toe. The stiffness and rigidity of the biphalangeal 5th toe may predispose it for symptomatic hammer or claw toe.
The current study provided an overview on the prevalence and pattern on pedal symphalangism in Hong Kong Chinese population, which might aid clinical judgment. Figure 6(a) showed a case of missed fracture through the biphalangeal 5th toe with the radiolucent fracture line being mistaken as distal interphalangeal joint. Figure 6(b) and (c) was radiograph taken 12 weeks post-injury, showing healed fracture. Rozen et al. reported similar cases of missing fracture. 14 Therefore, recognition of biphalangeal toes would be clinically important as it would potentially affect our diagnosis and subsequent management especially in injury cases.

Fracture biphalangeal left 5th toe being misdiagnosed as normal.
This study has strengths and limitations. It was the first study on prevalence of toe symphalangism and variation on laterality and gender in Hong Kong Chinese population. The sample size was large comparing with current literatures using foot radiographs in adult. Substantial amount of X-rays bilateral feet were also included. Bilateral feet radiographs were available in this study for analysing the symmetry of pedal symphalangism, which was seldom performed in previous studies. All radiographs reviewed were in digital forms, which allowed adjustment of contrast and opacity for clearer visualization. However, there are limitations concerning projection of radiographs. The foot radiographs were taken in different views namely dorsoplantar, medial oblique, lateral, standing, and so on.
Conclusion
There is a high prevalence rate of 5th toe symphalangism in the Hong Kong Chinese Population. No significant difference in prevalence observed associated with gender or laterality. The less flexible lesser toes in the Chinese population have higher risks of development of deformities. The clinical implication of such findings needs further research.
Footnotes
Authors’ note
Patient’s rights and confidentiality have been well protected in all aspects.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.