
Abstract
Background
Metacarpal (MC) epiphyses are normally found proximally for the first and distally for the second to fifth metacarpal bones. Pseudoepiphyses are infrequently found at the non-epiphyseal ends of metacarpal bones during the normal pediatric growth process. This is the first study aiming to investigate the radiological prevalence and features of metacarpal pseudoepiphyses in the Hong Kong Chinese population.
Methods
Standard bone age radiographs of children (chronological age 5 to 10) taken in two regional hospitals from Jan 2016 to Dec 2020 were analyzed. Exclusion criteria include: advanced bone age older than 11 years old, non-Chinese ethnic origin, history of hand trauma and skeletal dysplasia. Partial pseudoepiphyses can involve either or both the radial or ulnar cortices with no continuation in between. Complete pseudoepiphyses are those that extended across the full width of the metacarpal bone. The prevalence of metacarpal pseudoepiphysis was documented. The effect of Gender and Age differences on the prevalence of pseudoepiphysis was analyzed with chi-squared test using SPSS 26.
Results
A total of 421 radiographs (94 males; 327 females) were reviewed. The prevalence of pseudoepiphysis of 1st, 2nd, 3rd, 4th and 5th metacarpal bones was 25.7%, 21.1%, 0%, 0% and 23.5%, respectively. Complete pseudoepiphysis was most commonly seen in the 1st metacarpal bone (3.3%). Occurrence of pseudoepiphysis in single bone (36.1%) is more common than occurrence in multiple bones (15.4%). Combined 2nd and 5th metacarpal pseudoepiphysis is the most common pattern (38.5%). Gender (1st MC p = 0.19; 2nd MC p = 0.592; 5th MC p = 0.159) and Age (1st MC p = 0.103; 2nd MC p = 0.093; 5th MC p = 0.211) showed no differences on the prevalence of pseudoepiphysis.
Conclusion
There is a high prevalence of metacarpal pseudoepiphysis in the Hong Kong Chinese population. Understanding the radiological prevalence and features of metacarpal pseudoepiphyses is important to avoid misinterpretation as fractures in pediatric patients.
Introduction
Pseudo-epiphyses refer to an anatomical variant characterized by the presence of a structure that resembles a physeal growth plate at the opposite end of a normal epiphysis. Radiologically, this pseudo-physeal plate appears as areas of radiolucency, indicating a cartilage-like structure visible on radiographs. This condition can manifest as either a complete formation, where the pseudo-epiphyses fully mimic the appearance of a typical epiphysis, or as a partial formation, exhibiting a cleft, or notch-like appearance.
Pseudoepiphyses are infrequently found at the non-epiphyseal ends of metacarpal bones during the normal pediatric growth process. Notably, metacarpal epiphyses are typically located proximally for the first metacarpal and distally for the second to fifth metacarpal bones. In 1736, Nesbitt first reported a pseudoepiphysis on the distal first metacarpal bone. 1 Over the years, the incidence of pseudoepiphyses has been documented in several reported series in different populations, but the results vary widely.2–8
The mechanism of pseudoepiphysis formation was not fully understood. It has been suggested that pseudoepiphysis may be part of the normal developmental process of metacarpal bones and has no clinical significance. 4 However, the condition has been associated with a number of congenital anomalies, endocrine disorders and other systemic diseases that affect skeletal growth.4,9,10
A better understanding of the radiological prevalence and features of metacarpal pseudoepiphyses is important to avoid misinterpretation as fractures in paediatric patients. This retrospective review is the first study aiming to investigate the radiological prevalence and features of metacarpal pseudoepiphyses in the Hong Kong Chinese population.
Methods
Standard bone age radiographs of children of chronological age of 5 to 10 years old taken in two regional hospitals in Hong Kong were analyzed. The study period was from January 2016 to December 2020. The data were retrieved from the Clinical Data and Reporting System and Clinical Management System. Ethical approval for this study was granted by the Research Ethics Committee.
Standard bone age radiographs were used in this study as these are the most commonly obtained radiographs in our target population. In addition, the view of radiographs can be standardized, and the presence of previous injuries can be minimized. The bone age can also be evaluated by radiologist using the Greulich-Pyle or Tanner-Whitehouse method.
Exclusion criteria included (1) advanced bone age of 11 years old or above, (2) non-Chinese ethnic origin, (3) history of hand trauma, and (4) background of skeletal dysplasia. For patients with serial radiographs taken, only the earliest radiograph will be included.
In evaluating the radiographs, there is currently no universally agreed or validated radiological criteria found in the literature to define pseudoepiphysis. The authors performed a pilot screening of 20 radiographs. Two scatter plots Figure 1 were plotted and a radiological criterion was developed that best differentiated between pseudoepiphysis and non-pseudoepiphysis notches in metacarpal bones. Figure 2 was one of the examples to illustrate the evaluation of a notch-like or cleft-like metacarpal indentation. We would measure the depth (a) and width (b), and then calculate the (a) to (b) ratio and the angle of the notch. In this study, we defined a pseudoepiphysis when the (a) to (b) ratio is greater than 0.3 and the angle is less than 100°. In Figure 3, this notch was excluded and not considered a pseudoepiphysis because it did not fulfil our radiological criterion. We therefore defined a partial pseudoepiphysis as a cortical notch or cleft that met our radiological criterion. A partial pseudoepiphysis may involve either the radial or ulnar cortex, or sometimes both cortices with no continuation in between. Complete pseudoepiphyses, on the other hand, are those that extend across the entire width of the metacarpal bone as shown in Figure 4.
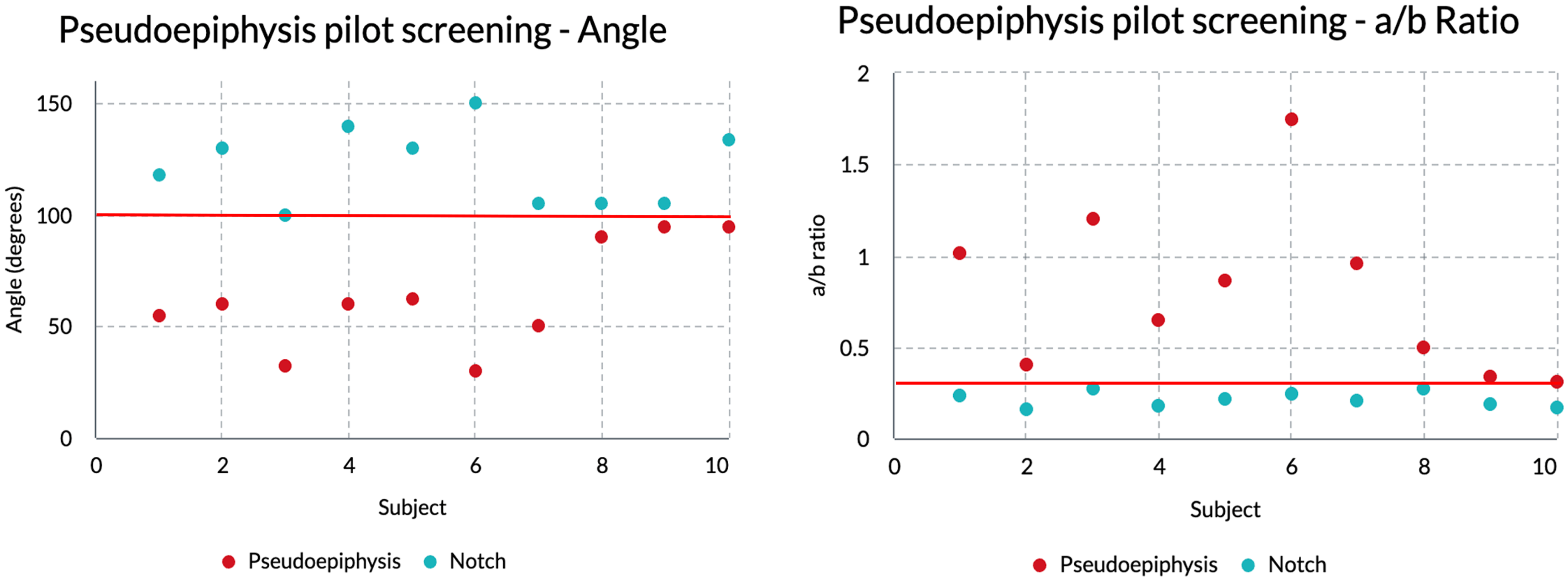
Scatter plots for the pseudoepiphysis pilot screening.
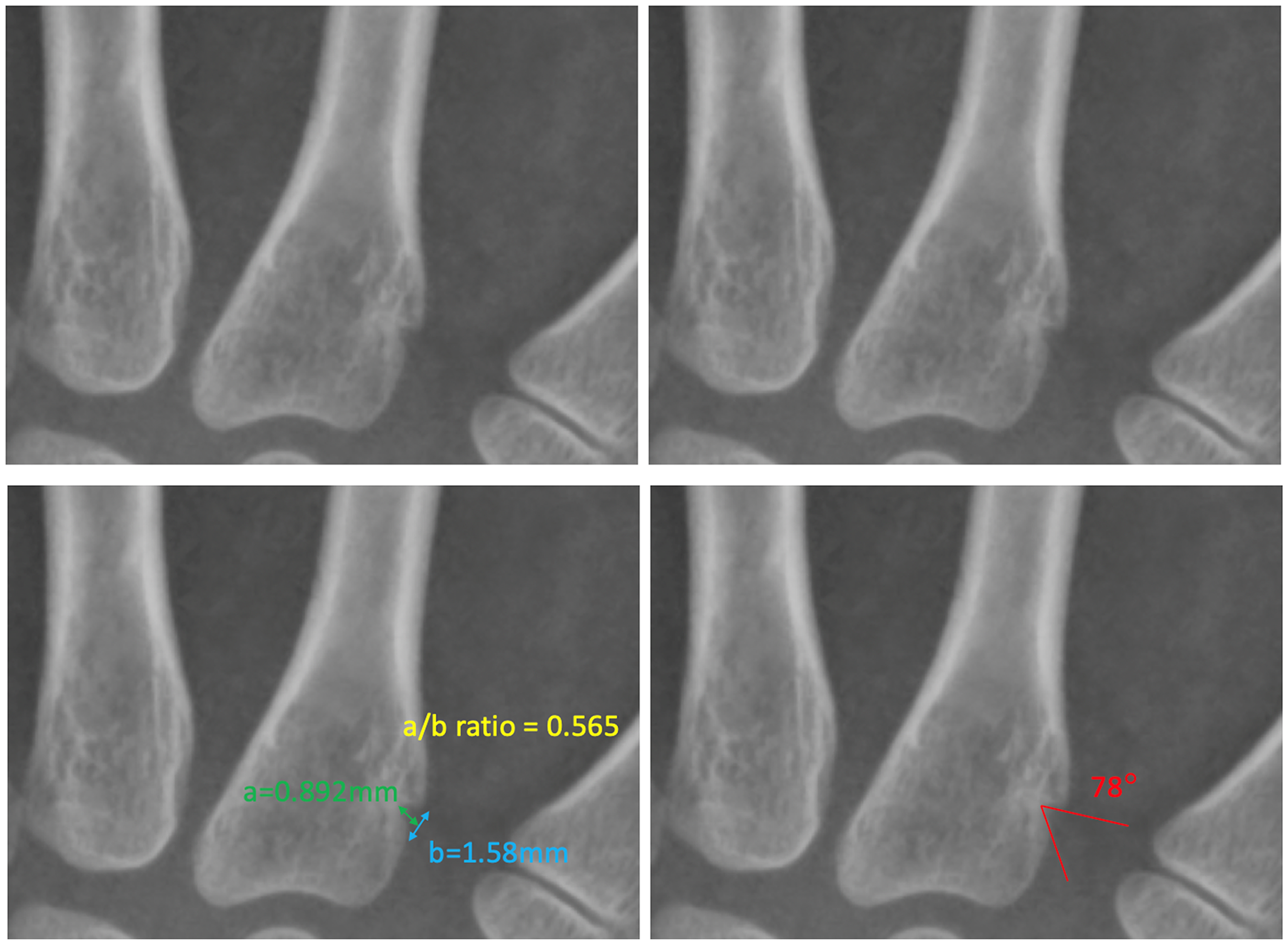
Example of a notch of the 2nd metacarpal bone that is included as a pseudoepiphysis (a/b ratio is greater than 0.3 and the angle is less than 100°).
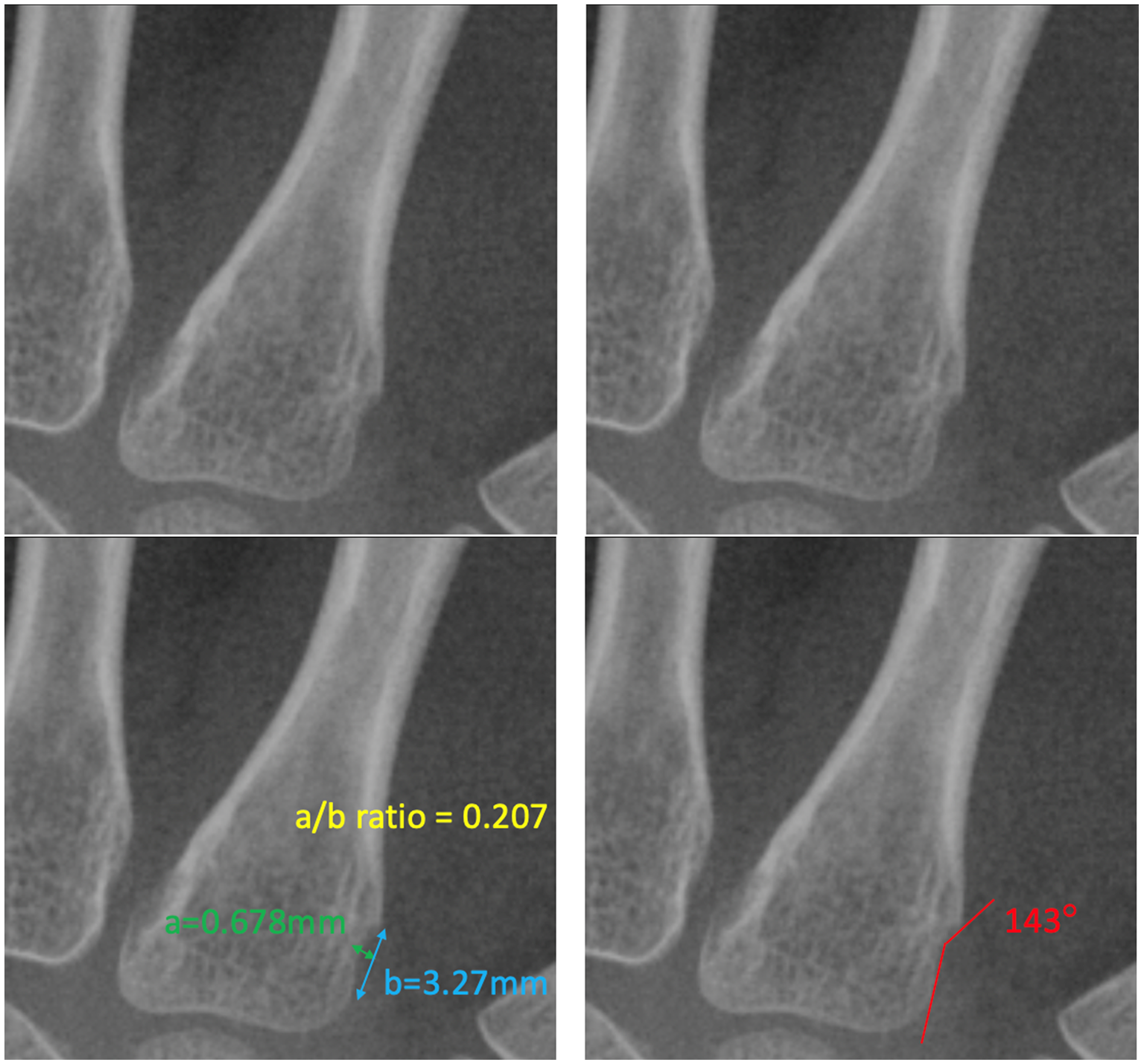
Example of a notch of the 2nd metacarpal bone excluded as a pseudoepiphysis (a/b ratio is less than 0.3 and angle is greater than 100°).
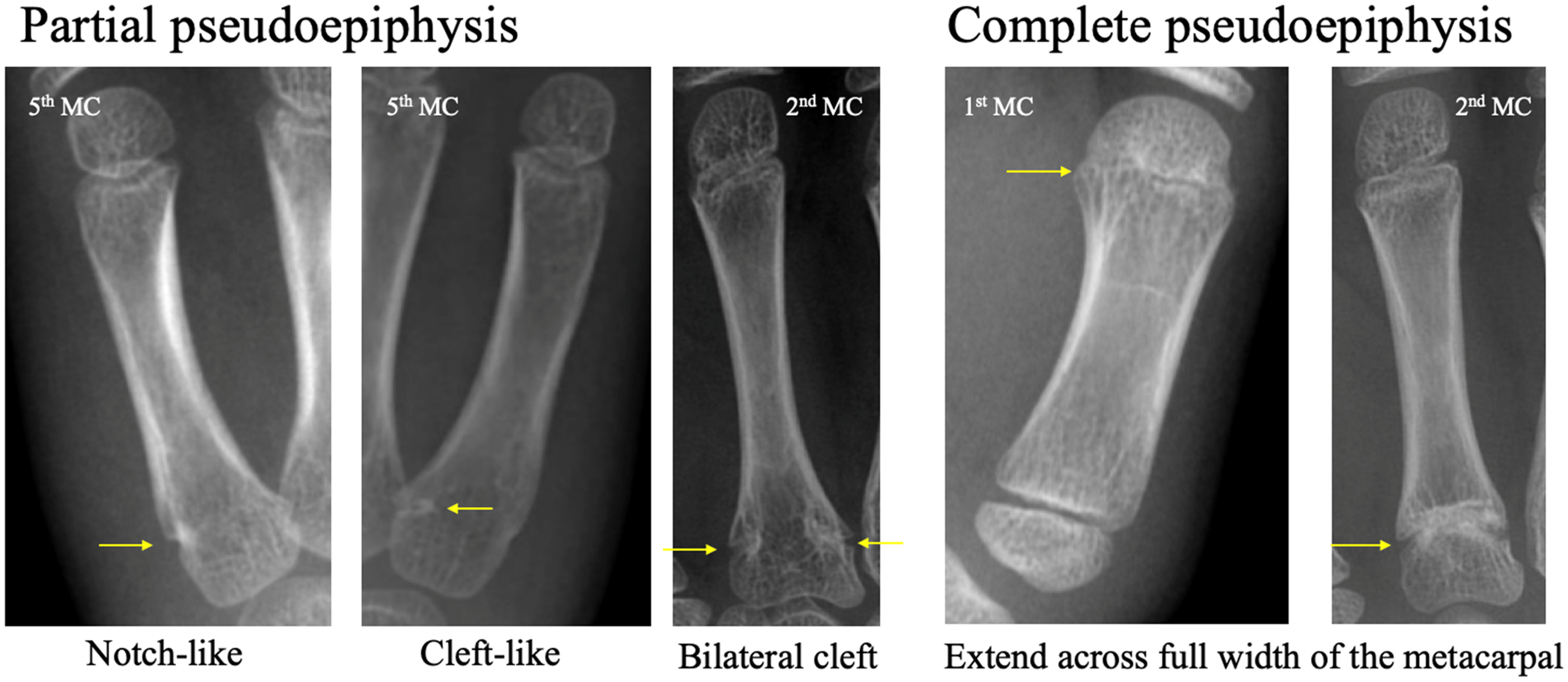
Examples of partial and complete pseudoepiphysis.
The presence of pseudoepiphyses in the five metacarpal bones and their distribution were independently recorded and evaluated by two orthopedic trainees, a Radiology trainee and an Orthopaedic specialist. We also documented the prevalence of partial and complete pseudoepiphyses as well as single and multiple pseudoepiphyses. Any discrepancy was discussed with a senior Hand specialist and a Radiology specialist to reach a consensus.
Subgroup statistical analysis was performed to evaluate the effects of gender and bone age on the prevalence of pseudoepiphysis. Statistical analysis was performed using chi-squared test by SPSS 26, and a p-value of <0.05 was considered statistically significant.
Results
A total of 421 standard bone age radiographs were analyzed with 94 being male patients (22.3%) and 327 being female patients (77.7%). Their mean age was 7.6 ± 1.4 years (range, 5–10 years). In our cohort, the overall prevalence of metacarpal pseudoepiphyses is 50.8%, with 214 cases identified out of a total of 421 cases.
After adding up all the pseudoepiphyses identified, we found most pseudoepiphyses in the 1st metacarpal bone and no pseudoepiphysis in the 3rd and 4th metacarpal bone. The prevalence of pseudoepiphyses of the 1st, 2nd, 3rd, 4th and 5th metacarpal bones was 25.7%, 21.1%, 0%, 0% and 23.5%, respectively. The percentage incidence of pseudoepiphyses on each metacarpal bone is shown in Figure 5.
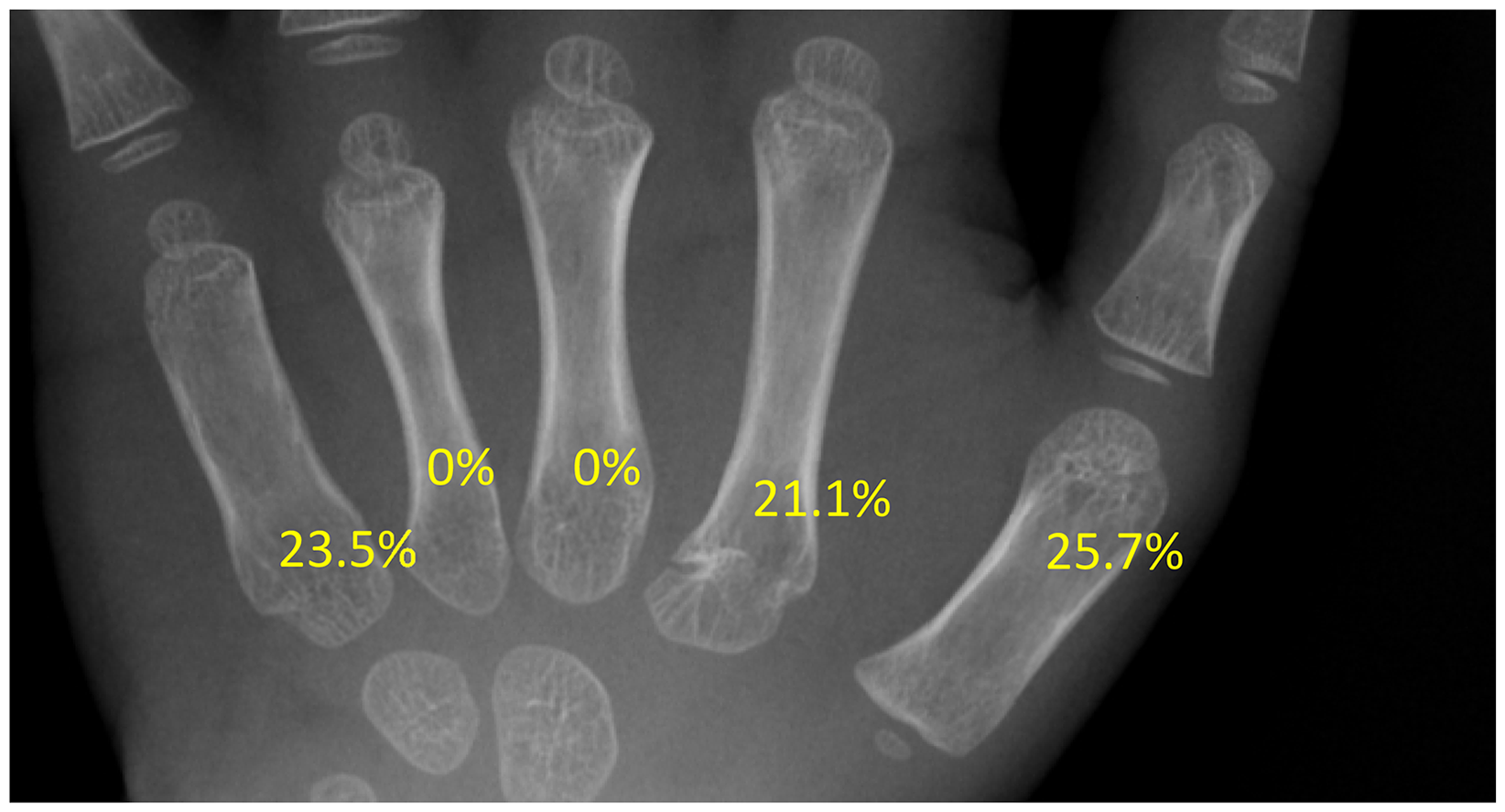
Percentage incidence of pseudoepiphysis on each metacarpal bones.
In patients with metacarpal pseudoepiphyses, the occurrence of pseudoepiphyses in a single bone (n = 149, 35.4%) is more common than the occurrence in multiple bones (n = 65, 15.4%). In patients with a single pseudoepiphysis, it is most commonly found in the 1st metacarpal bone alone (n = 68, 16.2%). In patients with multiple pseudoepiphyses, four different patterns of pseudoepiphysis distribution were identified. Combined 2nd and 5th metacarpal pseudoepiphyses is the most common pattern (n = 25, 5.9%). All identifiable patterns of metacarpal pseudoepiphysis are summarized in Table 1.
All identifiable patterns of metacarpal pseudoepiphysis.
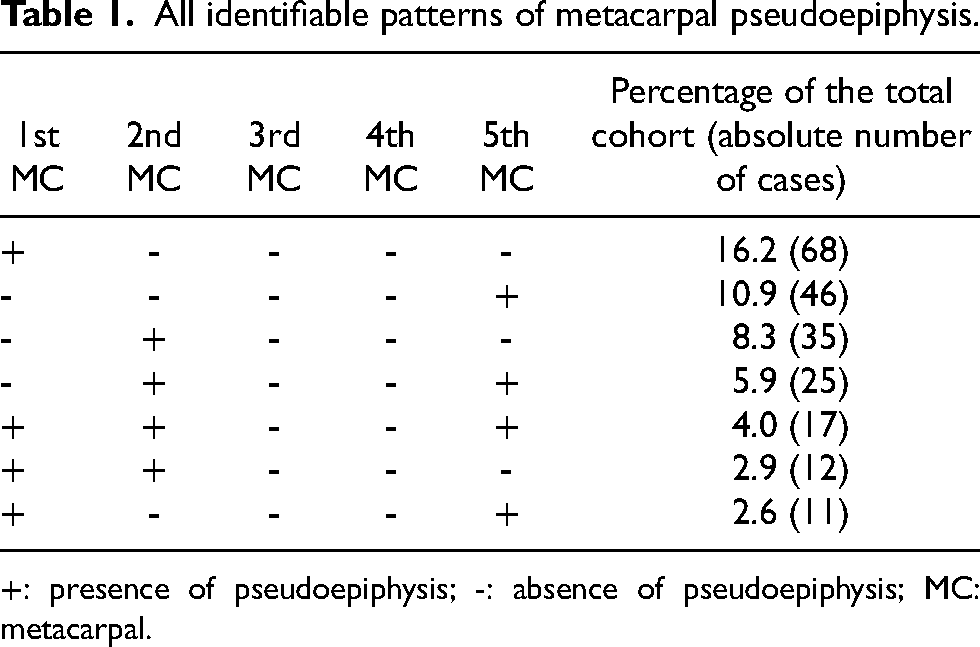
+: presence of pseudoepiphysis; -: absence of pseudoepiphysis; MC: metacarpal.
Looking at the frequency of partial and complete pseudoepiphyses in each metacarpal bone, similar frequencies of partial pseudoepiphysis were found across 1st, 2nd and 5th metacarpal bone from 19.5 to 22.8%. A complete pseudoepiphysis was most commonly seen in the 1st metacarpal bone with a prevalence of 3.3%. The distribution of partial and complete pseudoepiphyses is summarized in Table 2.
Distribution of partial and complete pseudoepiphysis in percentage (number).
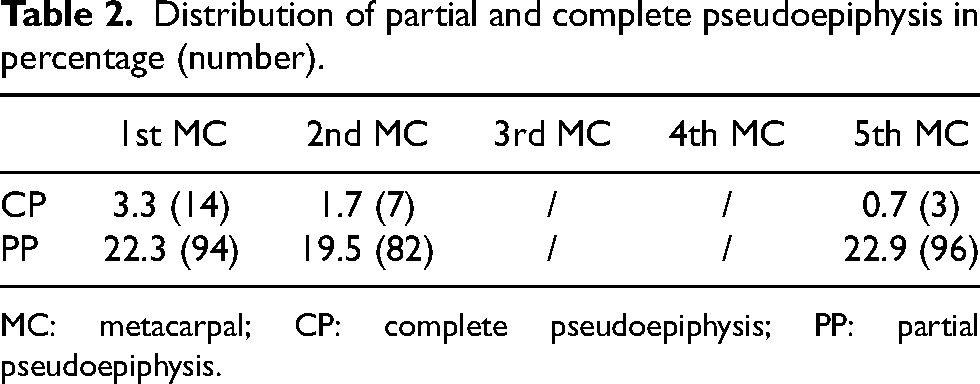
MC: metacarpal; CP: complete pseudoepiphysis; PP: partial pseudoepiphysis.
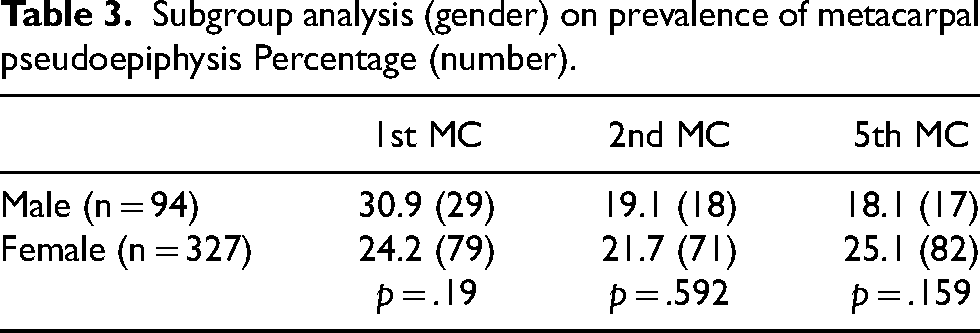
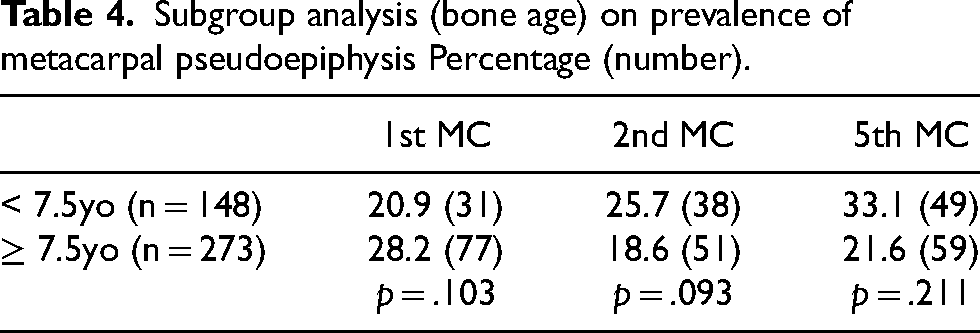
Two subgroup analyses were performed, which are summarized in Tables 3 and 4. In the gender group, comparing male versus female, the differences in the prevalence of metacarpal pseudoepiphyses were found to be statistically insignificant (1st MC p = 0.19; 2nd MC p = 0.592; 5th MC p = 0.159). In the bone age group, we divided the patient population into patients above (n = 273, 64.8%) and below (n = 148, 35.2%) a bone age of 7.5 years old. Again, no statistical difference was found in the prevalence of pseudoepiphysis (1st MC p = 0.103; 2nd MC p = 0.093; 5th MC p = 0.211).
Subgroup analysis (gender) on prevalence of metacarpal pseudoepiphysis Percentage (number).
Subgroup analysis (bone age) on prevalence of metacarpal pseudoepiphysis Percentage (number).
Discussion
Pseudoepiphysis was considered as a normal developmental variation, but the exact mechanism of formation was not yet fully understood. Haines, Ogden et al. and Laor et al. illustrated the development and histological formation of pseudoepiphysis.11–13 At the bones of the hands and feet, the epiphyseal end was known to grow by endochondral ossification from the transverse physis or secondary ossification centre. On the contrary, the non-epiphyseal end was recognized to undergo direct ossification from the metaphysis towards the articular surface. The authors further reported three basic patterns of ossification formation. Most commonly, a central osseous bridge extends outward from the metaphysis towards the periphery and the articular surface in a “mushroom-like” fashion. This physeal variant often has a circular notch proximal to this osseous bridge, which gives the bone the appearance of an epiphysis. Occasionally, this notch is eccentrically displaced and results in a cleft or partial pseudoepiphysis. Another pattern of non-epiphyseal ossification is when the horizontal cartilage remnants are much longer, isolating a region of developing bone such that there is a resemblance to a secondary ossification centre of an epiphyseal end, which may be the origin of a complete pseudoepiphysis. The least frequent pattern is when there is multiple stalks or osseous expansions with protrusions of varying lengths into the cartilage. Limb et al. however, proposed that complete pseudoepiphyses are likely to have formed as de novo ossification centres within a cartilaginous epiphysis. 7 In either situation, the physeal cells at the non-epiphyseal ends ultimately lose their columnar architecture and are incapable to contribute to bone length. It was observed that all transverse physes persisted later in skeletal development than the non-epiphyseal end physes.
After being first reported by Nesbitt in 1736, the incidence of pseudoepiphyses was documented in several reported series in different populations but the results vary widely. In one of the earliest studies by Posener et al. in 1939, 100 normal school children in London aged 4 to 8 years old were studied, and they found metacarpal pseudoepiphysis in 96% of the children's hands. 2 In 1967, Lee and Garn investigated a longitudinal series of hand radiographs of healthy white children (116 boys and 118 girls) and found a pseudoepiphysis in either the first, second or fifth metacarpal bones in 100% of the cases studied. 4 Levine, in 1972 examined 2250 children in four ethnic populations in South Africa and the prevalence of metacarpal and phalangeal pseudoepiphyses ranged from 77.1% to 88.9%. 5
Wood et al. were the first to document the incidence of different types of pseudoepiphyses. 6 They reviewed 399 radiographs with open epiphyses and 65 cases (16.3%) were found to have one or more abnormal epiphyses. They identified three types of abnormal epiphyses. Similar to the “complete pseudoepiphysis” in our study, they defined a “double epiphysis” as a bone with two complete epiphyses, one at each end, with complete separation of the bone. Double epiphyses were most common in the first metacarpal bone (29 cases, 7.3%) and the second metacarpal bone (22 cases, 5.5%). In contrast to our definition of “partial pseudoepiphysis”, they defined “pseudoepiphysis” separately as lucency on both the radial and ulnar sides of the abnormal epiphyseal plate without crossing the bone entirely, and “notching” as lucency only involving either radial or ulnar side of the bone. “Pseudoepiphysis” was also most commonly seen in first metacarpal bone (20 cases, 5.0%). A review of 610 radiographs of asymptomatic children by Limb et al. adopted a similar definition of complete and partial pseudoepiphysis as in our study. 7 Complete pseudoepiphyses were identified in the first metacarpal bone (1.97%) and second metacarpal bone (1.31%). Partial pseudoepiphyses were most commonly found in second metacarpal bone (15.25%), followed by the fifth metacarpal bone (7.21%) and the third metacarpal bone (0.49%). Lee et al. studied the radiological prevalence of metacarpal pseudoepiphysis in 2320 healthy Korean children. 8 The prevalence of pseudoepiphysis was 13.1%. The first metacarpal bone was most commonly involved (9.6%) followed by the second metacarpal bone (5.2%) and the fifth metacarpal bone (3.7%). 9.4% of children had a single pseudoepiphysis and 3.7% of children had multiple pseudoepiphyses. The overall prevalence of each incomplete or partial pseudoepiphysis was 5.0%, 4.0%, and 2.4% in the first, second, and fifth metacarpal bone, respectively, and prevalence of each complete pseudoepiphysis was 4.7%, 1.2%, and 0.1%, respectively. Our study confirmed that the first, second and fifth metacarpal bones were the most common sites. The third and fourth metacarpal pseudoepiphysis was not found in our study but was occasionally seen in some of the studies.2,5–7 We support that there are more children with a single pseudoepiphysis than children with multiple pseudoepiphyses. We also concur that partial pseudoepiphyses are more common than complete pseudoepiphyses.
Dreizen et al. were the first to report a significantly higher prevalence of metacarpal notching in boys than in girls. 3 Lee and Garn found that the incidence was very similar in both sexes. 4 Levine and Lee et al. also found significantly more metacarpal pseudoepiphyses in males than in females in different ethnic populations.5,8 This difference in incidence with gender could be due to the fact that during normal bone maturation, the epiphyseal union is completed on average 2 years earlier in girls than in boys, and also pseudoepiphyses were observed to fuse earlier than the normal physeal end. However, in the subgroup analysis performed in our study, comparing male versus female, the difference in the prevalence of metacarpal pseudoepiphyses was found to be statistically insignificant.
In our subgroup analysis, we also divided the patients into those above and below a bone age of 7.5 years old as the middle cut-off age of our sample population. Again, no statistical difference was found regarding the prevalence of pseudoepiphysis. Lee and Garn proposed that pseudoepiphysis is part of the normal developmental process at the non-epiphyseal end of the metacarpal bones and has no clinical significance. 4 However, Dreizen et al. observed that pseudoepiphysis was more common in children with delayed skeletal maturation. 3 This physeal variant has been associated with a number of congenital anomalies e.g., syndactyly, polydactyly, cleft hand etc., 6 endocrine disorders e.g., hypothyroidism, systemic diseases e.g., achondroplasia, Down's syndrome, 4 Laurence-Moon-Biedl-Bardet syndrome, 9 Silver Russell syndrome 10 and other diseases that affect skeletal growth. In this study, we excluded patients with background of skeletal dysplasia.
The definition of partial pseudoepiphysis has been inconsistent in the literature to date, and it is only described on the basis of morphology. Dreizen et al. used the terms “parasagittal”, “acute-angled”, “obtuse-angled”, “rectanguloid” and “crescent-shaped” notches to describe partial pseudoepiphysis. 3 Lee and Garn used similar terms: obtuse-angle stage, acute-angle stage, cleft stage, and fusion stage to outline the sequence of developmental stages of partial pseudoepiphysis. 4 They also attempted to grade the intensity of partial pseudoepiphysis: slight (+), moderate (++) or marked (+++) degrees of notching. These descriptions or grading of partial pseudoepiphyses were rather subjective. Therefore, we developed the radiological criterion to objectively define a partial pseudoepiphysis as mentioned above. Further studies are warranted to validate the current criterion in different patient groups and populations.
Metacarpal fractures and pseudoepiphyses exhibit distinct radiological features. Metacarpal pseudoepiphyses are found at the non-epiphyseal end of the 1st, 2nd and 5th metacarpal bones. It is not uncommon to have pseudoepiphysis in multiple bones, and from our study, the combined 2nd and 5th metacarpal pseudoepiphyses is the most common pattern. They typically present as notch-like or cleft-like indentations with smooth and well-defined edges. These indentations are usually narrow in width, involving either a partial or the entire diameter of the metacarpal bone. They are generally perpendicular to the diaphysis, resembling a normal epiphysis, with normal metacarpal alignment and preserved joint space. In contrast, metacarpal fractures appear as radiolucent lines with irregular, jagged edges which can be located at any point along any of the metacarpal bones. Depending on the fracture pattern, metacarpal fractures can exhibit variations in the width, shape and orientation. They may also lead to metacarpal misalignment and intra-articular involvement. The comparison between the radiological features of metacarpal pseudoephysis and metacarpal fracture is summarized in Table 5.
Comparison between the radiological features of metacarpal pseudoepiphysis and metacarpal fracture.
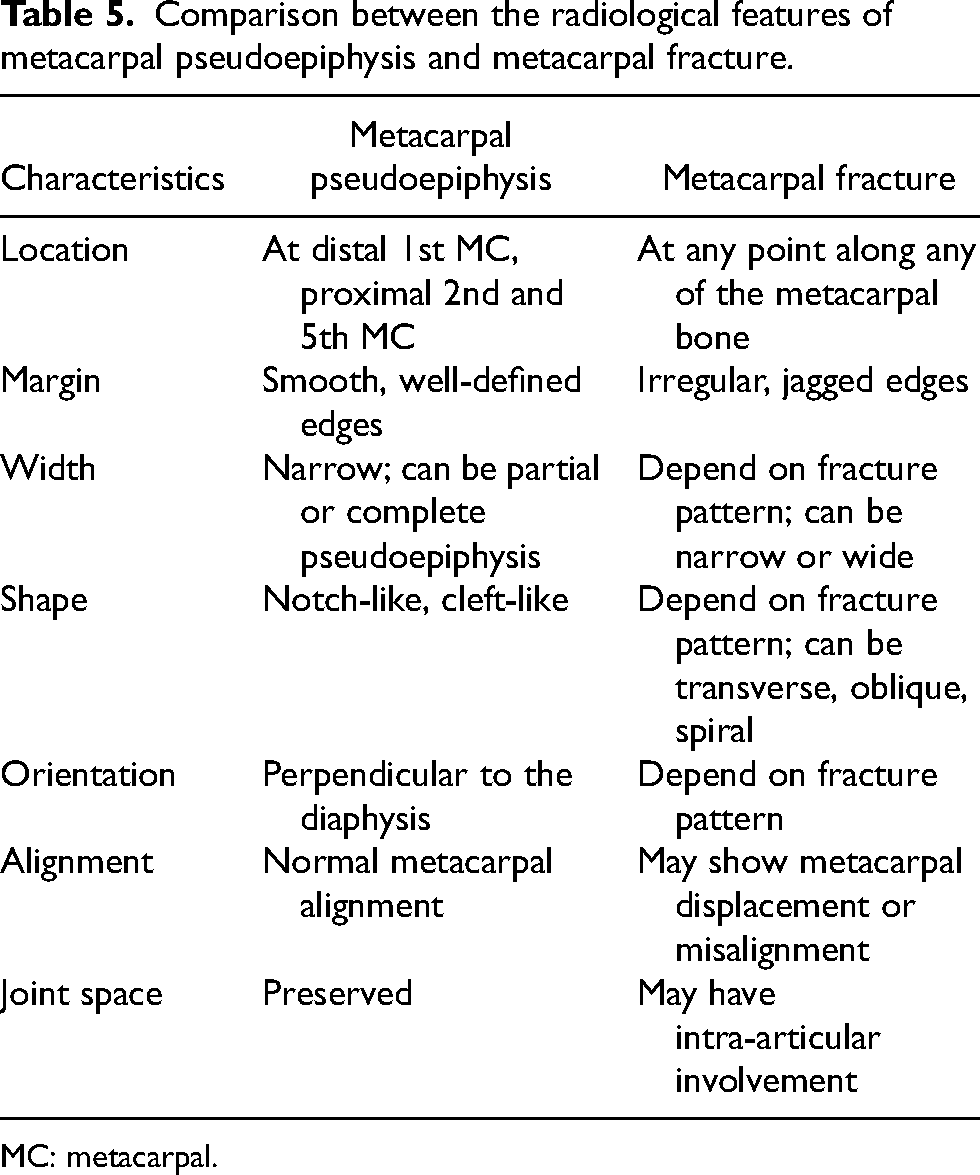
MC: metacarpal.
This study has strengths and limitations. This is the first study to investigate the radiological prevalence and features of metacarpal pseudoepiphyses in the Hong Kong Chinese population. All radiographs were analyzed in their digital form, which allowed adjustment of contrast for clearer visualization. However, there were several limitations. In our sample population, there are more females than males, as most patients requiring bone age radiographs are girls suspected of having precocious puberty. This may affect the accuracy of our results. The use of bone age radiographs can provide a standardized investigation, and can exclude cases of trauma and infection. However, the laterality of the metacarpal pseudoepiphysis cannot be evaluated. Furthermore, this is not a longitudinal study, so the change in morphology with age cannot be recognized and analysed. We also cannot determine the age of appearance and fusion of the pseudoepiphysis. This limitation of this study can be addressed by a subsequent longitudinal study. The observation of the presence of pseudoepiphysis was subject to an observational error, which could be improved by computed tomography or magnetic resonance imaging scans.
Conclusion
Metacarpal pseudoepiphyses are considered a normal variant of physeal development. There is a high prevalence of metacarpal pseudoepiphysis in the Hong Kong Chinese population. 50.8% of our patient population has pseudoepiphysis identified in one or more metacarpal bones, with a similar incidence found across 1st, 2nd and 5th metacarpal bone. The occurrence of pseudoepiphysis in a single bone is more common than in multiple bones. Complete pseudoepiphysis is most common in the 1st metacarpal bone. It was found that gender and bone age have no effect on the prevalence of metacarpal pseudoepiphysis. We have developed a radiological criterion to objectively define a pseudoepiphysis. Understanding the radiological prevalence and features of metacarpal pseudoepiphyses is important to avoid misinterpretation as fractures in pediatric patients. Future studies could further investigate the correlation between metacarpal pseudoepiphyses and metabolic and endocrine disorders.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.