
Abstract
Study design
Retrospective cohort study.
Objective
To perform a retrospective study comparing 2 level hybrid surgery (1 level ACDF and 1 level CDR) with 2 level ACDF and 2 level CDR.
Methods
Patients undergoing first-instance two-level cervical spine surgery were identified using CPT codes and grouped into ACDF, CDR, or hybrid (single-level ACDF + single-level CDR) cohorts, with exclusions for posterior fusion, trauma, infection, malignancy, prior revision, and overlapping procedures. Revision surgery was defined as any cervical operation within two years of the index procedure, and baseline variables included demographics, comorbidities (Elixhauser Comorbidity Index), cervical pathology, insurance type, tobacco history and osteoporosis. Comparisons were performed using t-tests and chi-square tests, and adjusted Cox proportional hazards models and Kaplan–Meier analysis were used to evaluate two-year revision risk and revision-free survival among cohorts.
Result
Among 122,164 patients, ACDF patients were older and had greater comorbidity burden and higher rates of myelopathy and osteoporosis, with overall secondary cervical procedures most frequent after two-level ACDF. On multivariable analysis, myelopathy, tobacco history and osteoporosis were independently associated with increased revision risk, while insurance status was not. Surgical approach (ACDF, CDR, or hybrid) was not independently associated with two-year revision risk, and Kaplan–Meier analysis showed no significant differences in revision-free survival among cohorts.
Conclusion
Surgical approach (ACDF, CDR, or hybrid) was not independently associated with differences in two-year revision risk.
Introduction
Degenerative cervical spine disease is a common disorder characterized by neck pain, radiculopathy, and myelopathy. 1 Early surgical management relied on laminectomy and posterior foraminotomy, but because these approaches were limited in treating centrally or paracentrally located discs, anterior cervical discectomy and fusion (ACDF) became the preferred technique by the mid-20th century. 2 ACDF may be linked to long-term complications, including reduced neck mobility, adjacent segment disease, and pseudoarthrosis.3–5 Although debated, many researchers suggest that adjacent segment disease following ACDF results from reduced mobility at fused levels, which increases mechanical stress and leads to greater motion in neighboring segments.6,7
To overcome the limitations of ACDF; especially reduced spinal mobility and adjacent segment disease; cervical disc replacement (CDR) was introduced as a motion-preserving option. CDR serves as an alternative surgical approach, particularly for younger, more active patients with cervical spine pathology. 4 CDR eliminates the need for fusion and maintains movement at the treated segment, thereby reducing stress on adjacent levels.4,7 Since its commercial introduction in 2007, 8 the use of CDR has increased substantially but is not suitable for all patients, such as those with poor bone and endplate quality.4,9–11 To address this issue, some surgeons perform hybrid ACDF and CDR operations to capitalize on the stability and motion preservation respectively of these two methodologies, Hybrid ACDF/CDR procedures typically involve performing ACDF at a more spondylotic level, with CDR at a less degenerated adjacent segment, either above or below.6,12,13
Limited data exist that compares Hybrid surgery with ACDF and CDR control groups. We therefore aim to perform a retrospective study comparing 2 level hybrid surgery (1 level ACDF and 1 level CDR) with 2 level ACDF and 2 level CDR using PearlDiver national database.
Methods
Data Source
This retrospective cohort study was conducted using the PearlDiver All-Payer Claims Database (Mariner), accessed through the Bellwether research interface. PearlDiver contains de-identified, longitudinal administrative claims data including inpatient and outpatient encounters, procedural codes, diagnoses, and demographic information. All cohort construction and analyses were performed using PearlDiver’s proprietary query language and statistical modules.
Study Design and Cohort Identification
Patients undergoing cervical spine surgery were identified using Current Procedural Terminology (CPT) codes. Three treatment cohorts were created: two-level anterior cervical discectomy and fusion (ACDF), two-level cervical disc replacement (CDR), and hybrid constructs consisting of single-level ACDF combined with single-level CDR. Only first-instance cervical procedures were included to capture index operations.
Two-level ACDF patients were identified using CPT-22551 as the index procedure with exactly one additional CPT-22552 code recorded on the same operative date. Two-level CDR patients were identified using CPT-22856 with exactly one CPT-22858 code on the same date. To ensure inclusion of isolated two-level procedures, patients were required to have only one additional-level code. Individuals undergoing posterior cervical fusion (CPT-22600) within one month of the index procedure were excluded. Patients with diagnoses related to trauma, infection, or malignancy were excluded. Additionally, patients with any prior cervical revision surgery before the index procedure were excluded. To create mutually exclusive cohorts, patients appearing in both the ACDF and CDR groups on the same date were removed.
The hybrid cohort was defined as patients undergoing single-level ACDF (CPT-22551 without CPT-22552) and single-level CDR (CPT-22856 without CPT-22858) on the same operative date. Patients with posterior cervical fusion within one month, trauma, infection or malignancy diagnoses, or prior cervical revision surgery were excluded. Only first-instance hybrid procedures were included.
Revision surgery was defined as any instance of cervical surgery (anterior fusion, posterior fusion, instrument removal, CDR revision or cervical decompression) after the primary two-level surgery and within two years [Supplemental Table 1].
Baseline demographic and clinical characteristics included age, sex, and Elixhauser Comorbidity Index (ECI). Additional variables included cervical myelopathy, cervical radiculopathy, insurance plan type, tobacco history and osteoporosis status.
Statistical Analysis
The Student’s t-test and Pearson chi-squared test of independence were used to compare continuous and categorical variables, respectively. Cox proportional hazards regression models were constructed to evaluate the association between surgical approach and risk of cervical revision surgery within two years. Models were adjusted for age, gender, ECI, cervical radiculopathy, cervical myelopathy, insurance plan type, tobacco history and osteoporosis. Kaplan–Meier survival analysis was performed to evaluate time to cervical revision surgery over a two-year follow-up period. Revision-free survival was compared among the ACDF, CDR, and hybrid cohorts.
Results
Study Population
A total of 122,164 patients met inclusion criteria and were included in the final analysis. This included 115,778 patients who underwent two-level ACDF, 4883 patients who underwent two-level CDR, and 1503 patients who underwent hybrid surgery.
Baseline Demographics and Clinical Characteristics
Demographics of 2 level ACDF, CDR and Hybrid Surgery
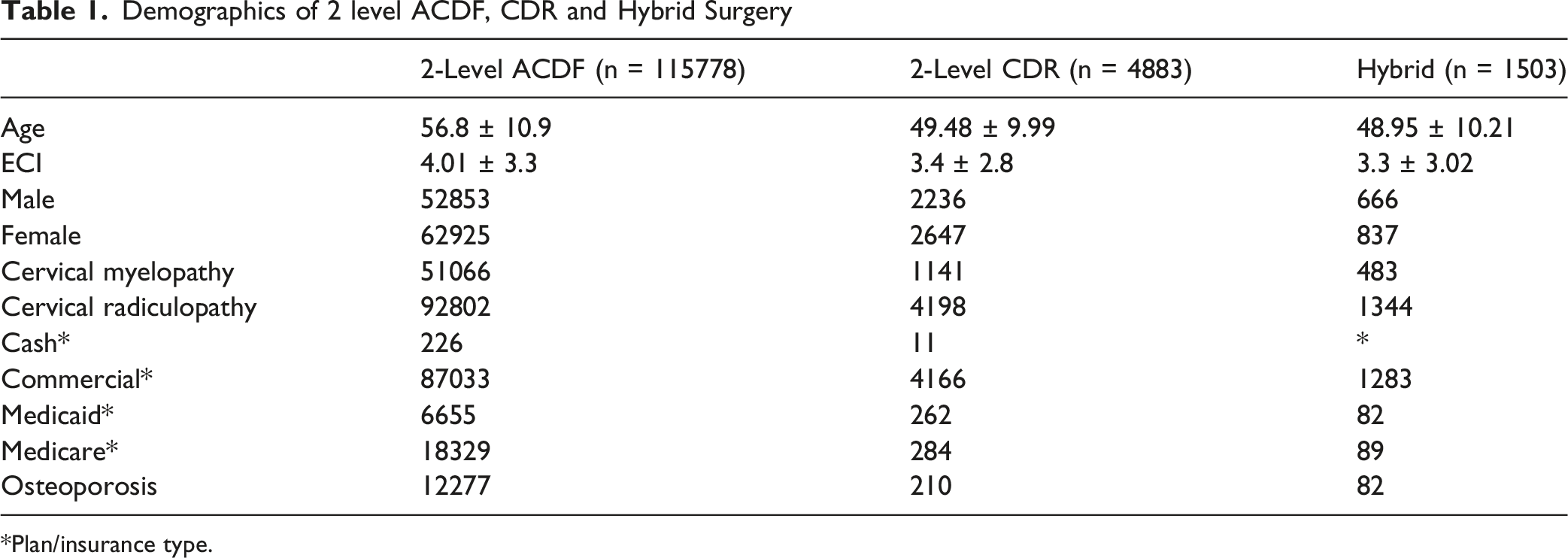
*Plan/insurance type.
Male patients comprised 45.7% of the ACDF cohort, 45.8% of the CDR cohort, and 44.3% of the hybrid cohort. Cervical myelopathy was most prevalent in the ACDF group (44.1%), followed by the hybrid (32.1%) and CDR (23.4%) groups. Cervical radiculopathy was present in the majority of patients across all cohorts, with the highest prevalence in the ACDF group (80.2%).
Commercial insurance was the most common payer across all cohorts. Tobacco history and osteoporosis was more prevalent among ACDF patients (34% and 10.6%) compared with CDR (32.6% and 4.3%) and hybrid (31% and 5.5%) patients.
Postoperative Revision and Reoperation Patterns
Cervical revision surgery pattern after 2 level ACDF, CDR and Hybrid Surgery

Instrument removal was performed in 1083 (0.9%) ACDF patients and 20 (0.4%) CDR patients, with no cases in the hybrid cohort. CDR revision procedures were observed exclusively in the CDR cohort (n = 35 [0.7%]). Cervical decompression was performed in 1422 (1.2%) ACDF patients, 47 (0.96%) CDR patients, and 18 (1.2%) hybrid patients.
Overall, secondary cervical procedures were most frequent among patients undergoing two-level ACDF.
Multivariable Cox Regression Analysis
Hazard of Cervical revision surgery after 2-level ACDF, CDR or hybrid surgery
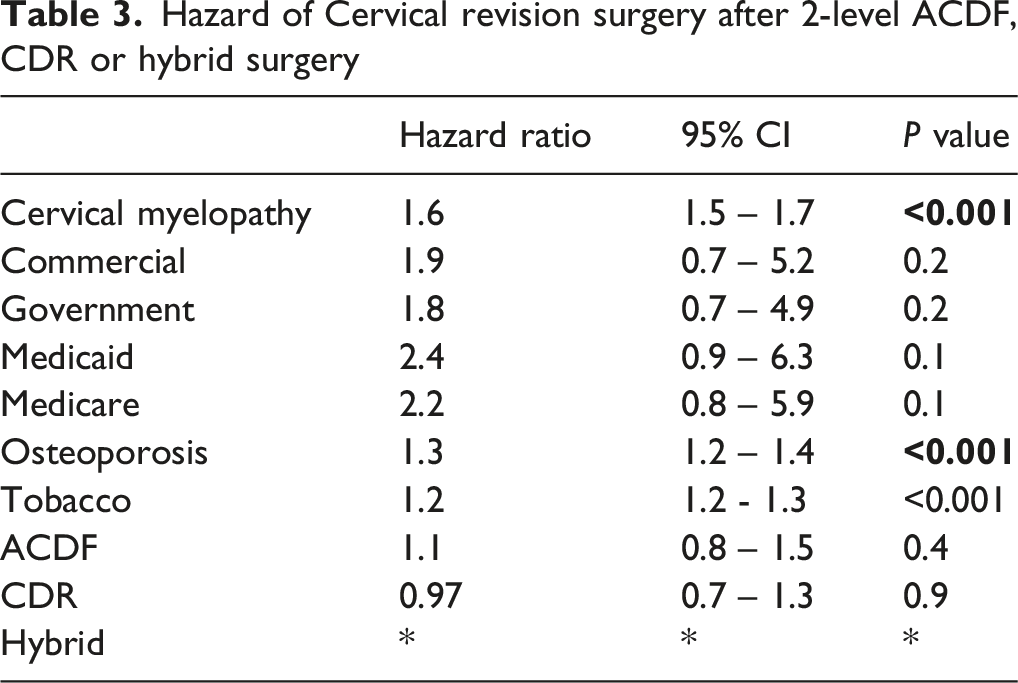
After adjustment, surgical approach was not independently associated with revision risk. Two-level ACDF was not associated with significantly increased risk compared with other cohorts (HR 1.2, 95% CI 0.9-1.6, P = .10), and CDR was not associated with reduced risk (HR 0.99, 95% CI 0.7-1.4, P = .96). The hybrid cohort was used as the reference group.
The initial cox proportional hazards model included 122,164 patients with 4675 revision events. The model included age, sex, Elixhauser Comorbidity Index (ECI), cervical myelopathy, cervical radiculopathy, insurance plan, osteoporosis, tobacco use, and surgical procedure–ACDF, CDR, and Hybrid. The overall model demonstrated neither ACDF or CDR revision risk significantly differed from Hybrid constructs (ACDF HR: 1.24, P = .138, CDR HR: 0.99, P = .963). However, the assumption of proportional hazards was violated in this model with Schoenberg residual global P value <.001. Age, sex, ECI and radiculopathy each violated the proportional hazards assumption. Due to limitations of the integrated bellwether statistical modeling software within PearlDiver, controlling for varying age, sex, ECI and radiculopathy across time was not possible. Instead, a sensitivity analysis was conducted by creating a model excluding these variables. Sensitivity analysis similarly found no statistically significant differences compared to hybrid constructs (ACDF: HR 1.12, P = .444, CDR: HR 0.97, P = .867). In the revised model Schoenfeld residual test demonstrated the proportional hazards assumption was not violated. (global test: χ2 = 11.43, df = 10, P = .325). Model concordance was modest, 0.605 for the full model and 0.581 for the sensitivity analysis.
Survival Analysis
Kaplan–Meier survival analysis demonstrated substantial overlap among the two-level ACDF, two-level CDR, and hybrid cohorts over the two-year follow-up period. Kaplan Meier analysis demonstrated high revision-free survival for all three cohorts. Revision-free survival at 1 year was 97.2% for ACDF (95% CI, 97.1%–97.3%), 97.7% for CDR (95% CI, 97.2%–98.1%), and 97.8% for hybrid procedures (95% CI, 97.1%–98.6%). At 2 years, revision-free survival was 95.8% for ACDF (95% CI, 95.6%–95.9%), 96.8% for CDR (95% CI, 96.2%–97.3%), and 96.5% for hybrid procedures (95% CI, 95.5%–97.5%).
Log-rank testing showed a statistically significant difference between groups (χ2 = 11.7, df = 2, P = .003). However, these differences were not maintained after multivariable adjustment.
Discussion
In this large retrospective cohort study utilizing a national all-payer claims database, we compared two-year revision rates following two-level anterior cervical discectomy and fusion (ACDF), two-level cervical disc replacement (CDR), and hybrid ACDF/CDR constructs. After adjustment for demographic and clinical factors, surgical approach was not independently associated with revision risk, with substantial overlap in revision-free survival between hybrid and comparison cohorts. These findings suggest that two-level ACDF, CDR, and hybrid surgery provide comparable mid-term durability.
There was a moderate difference in point estimates between ACDF and hybrid surgery, with a trend towards reduced revision rates in hybrid surgery at 2 years compared to ACDF. However, due to a substantially smaller sample size in the hybrid cohort, 95% confidence intervals were wide, and this finding was not found to be different from random chance. These findings instead suggest continued research is warranted as more patients are treated with hybrid constructs and the sample size of this cohort increases. As more data becomes available, propensity matched analyses may also be useful, since variations in baseline characteristics and indication bias likely play a role in patient selection and outcomes.
Our results are consistent with those recently reported by Durand et al., 14 who analyzed a large commercial insurance database and found no significant differences in revision rates among two-level ACDF, CDR, and hybrid constructs in patients under 65 years old at five years of follow-up. Similar to their study, our analysis employed strict CPT-based cohort definitions and excluded patients with trauma, malignancy, infection, prior revision surgery, and staged posterior fusion, enhancing cohort specificity. While Durand et al. 14 investigated exclusively commercial insurance and patients 65 and under, our data includes alternative payer types and older ages, potentially improving generalizability. Futhermore, we identified increased revision risks for patients with indication of radiculopathy or myelopathy, and a small but significant effect of ECI.
While Durand et al. 14 observed higher revision rates in plated hybrid constructs, our dataset did not include stratification by implant type or fixation method, which may partly explain minor differences in reported hazard ratios. Nevertheless, both studies demonstrate that, when controlling for confounders, surgical strategy alone does not appear to be a dominant predictor of early to mid-term revision.
Several systematic reviews and meta-analyses have emphasized the biomechanical advantages of hybrid surgery and CDR over multilevel fusion. Yang et al reported superior preservation of cervical range of motion and reduced adjacent segment motion with hybrid constructs compared to two-level ACDF, while noting similar complication rates and clinical outcomes. 15 Likewise, Lu et al. 16 and Hollyer et al. 17 found improved radiographic parameters with hybrid surgery but no consistent differences in short-term complications or functional scores.
Our findings complement this literature by demonstrating that while these reported biomechanical benefits may improve quality of life, they do not necessarily translate into reduced revision rates within two years. This suggests that drivers of revision are multifactorial. Radiographic preservation of motion may not be sufficient, in isolation, to prevent early reoperation, particularly in a heterogeneous, real-world population.
Consistent with prior studies, patients undergoing ACDF in our cohort were older and had higher comorbidity burdens than those undergoing CDR or hybrid surgery. Similar patterns were reported by Michalopoulos et al, who noted that hybrid and CDA patients were generally younger and healthier than ACDF patients in the ACS-NSQIP database. 18
Our multivariable analysis demonstrated that surgical approach was not independently associated with revision risk after adjustment. Instead, cervical myelopathy, tabacco use and osteoporosis were stronger predictors of revision. Myelopathy often reflects advanced spinal cord compression and multilevel disease, 19 which may not be fully addressed with index surgery or may progress despite intervention. Tobacco use is a well established cause of reoperation after cervical vertebrae intervention, 20 while osteoporosis likely contributes through impaired bone quality, increasing the risk of subsidence, pseudoarthrosis, or hardware failure. These findings underscore the importance of patient-level factors in determining postoperative durability.
We observed that anterior and posterior cervical fusion procedures were the most common secondary interventions across all cohorts. CDR-specific revisions were rare, consistent with prior reports indicating low failure rates of cervical arthroplasty.
Durand et al. 14 and Raso et al. 21 have suggested that reoperations following hybrid surgery and CDR are more commonly related to adjacent segment pathology, stenosis, or progression of degenerative disease rather than implant failure. Because claims data lack granular clinical and radiographic detail, we were unable to determine the specific indications for revision. However, the predominance of fusion-based revisions in our cohort suggests that progressive degeneration and biomechanical changes remain key drivers of reoperation, regardless of index procedure.
Compared with prior institutional series and meta-analyses, our study benefits from a substantially larger sample size and broad payer representation, enhancing generalizability. Whereas most meta-analyses include fewer than 700 patients, our cohort included over 120,000 individuals. This allowed for robust multivariable modeling and subgroup adjustment. Additionally, our use of first-instance procedures and strict CPT coding minimized misclassification.
Limitations
Several limitations should be acknowledged. First, the retrospective nature of claims-based analyses introduces potential residual confounding, despite multivariable adjustment. Important variables such as sagittal alignment, bone mineral density, implant design, and surgeon experience were unavailable (Figure 1). Kaplan Meier Curve showing revision free survival stratified by cohort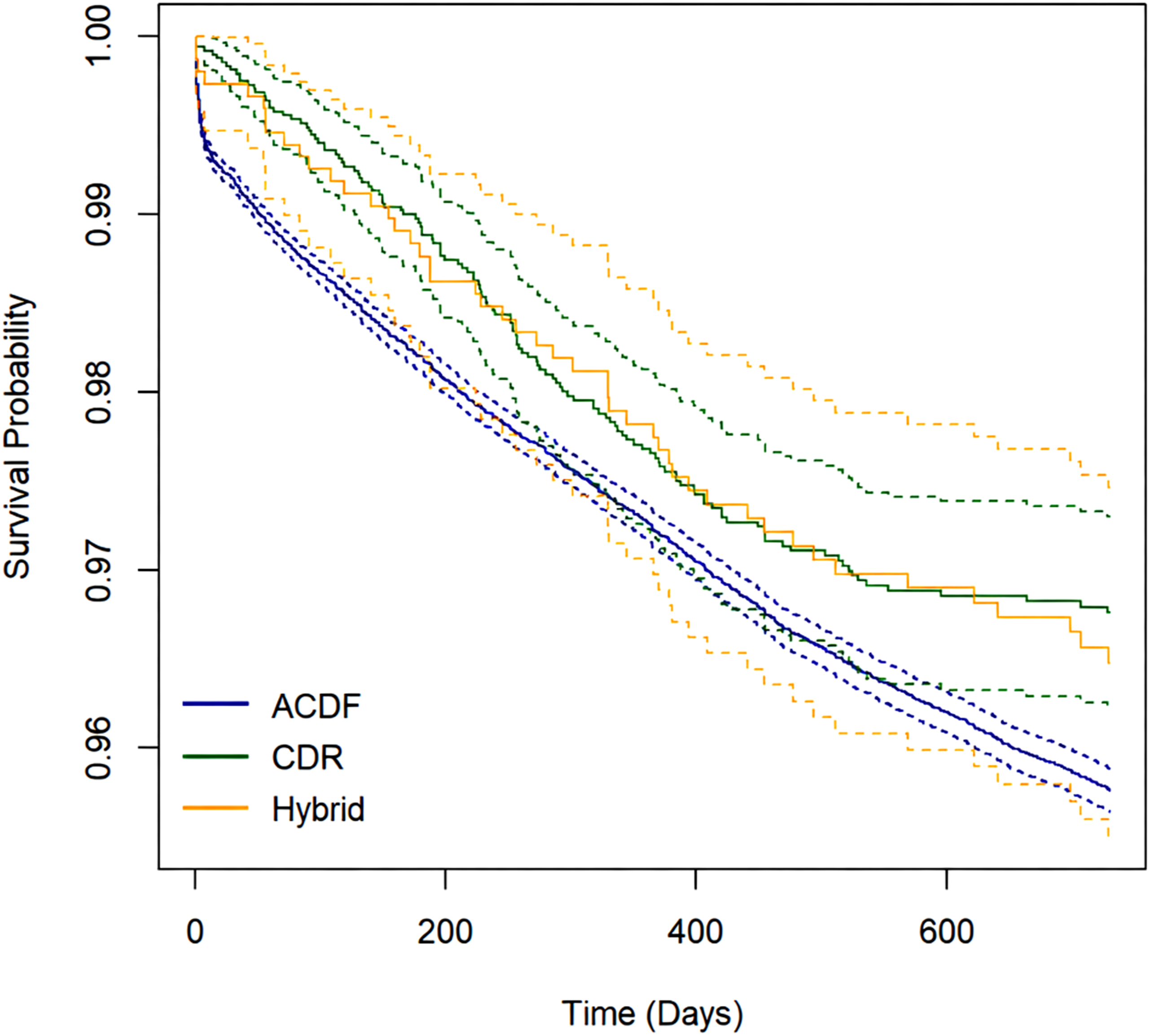
Second, revision surgery was identified through procedural codes, which may underestimate minor reoperations or nonoperative management, and do not control for level so were unable to determine if revisions were at an index level or adjacent level, limiting interpretability. Third, we were unable to stratify patients by implant type, plating technique, or specific hybrid configurations, which have been shown to influence outcomes in prior studies.
Finally, our follow-up period was limited to two years due to small cohort size, particularly of the hybrid procedure and data availability. Longer-term studies suggest that differences in adjacent segment disease may become more apparent after five to ten years. The two-year follow-up period is insufficient to capture differences in long-term outcomes between surgery types, such as comparison of adjacent segment disease. With time, more hybrid surgeries are likely to be performed, and longer-term follow up for previously implanted constructs will become available.
Supplemental Material
Supplemental Material - Nationwide Comparison of 2 year Revision Surgery Risk After Hybrid Cervical Surgery with 2-Level ACDF and 2-Level CDR Surgical Technique
Supplemental Material for Nationwide Comparison of 2 year Revision Surgery Risk After Hybrid Cervical Surgery with 2-Level ACDF and 2-Level CDR Surgical Technique by Ali Issani, Aidan Lindgren, Daniel Rusu, Raymond J. Hah, Ram Kian Alluri, Jeffrey Wang in Global Spine Journal
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
No funding was received for this study. Ali Issani, Aidan Lindgren and Daniel Rusu have nothing to disclose. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes, and stock options from Bone Biologics, Electrocore, PearlDiver, and Surgitech. Raymond J. Hah has received grant funding from SI bone, consulting fees from NuVasive, and support from the North American Spine Society to attend meetings. Ram K. Alluri has received grant funding from NIH, consulting fees and stock options from HIA Technologies, and payment from Eccential Robotics for lectures and presentations. Informed consent and institutional review board approval were not required as this review did not include patient information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.