
Abstract
Study Design
Retrospective cohort study.
Objective
To evaluate the predictive value of intraoperative bulbocavernosus reflex (BCR) monitoring for postoperative bowel dysfunction (PBD) following conus medullaris and cauda equina tumor (CMCET) resection.
Methods
A total of 118 patients were analyzed. Neurogenic Bowel Dysfunction Scores >6 at 1 month and 6 months postoperatively defined short- and long-term PBD. The amplitude reduction ratio (ARR) was calculated from bilateral BCR waveforms using the worst-side ARR for analysis. Multivariate logistic regression and ROC curve analysis determined independent predictors and optimal thresholds. Stratified 10-fold cross-validation confirmed threshold stability.
Results
Patients with short-term or long-term PBD had significantly higher ARRs than those without (P < 0.001 for both comparisons, Mann-Whitney U test). Furthermore, ARR emerged as the only independent predictor for either short-term (OR 1.287, 95% CI 1.018-1.627, P = 0.035) or long-term PBD (OR 1.153, 95% CI 1.055-1.261, P = 0.002). The threshold values of ARR for predicting short-term and long-term PBD were 59.6% (AUC = 0.991, 95% CI 0.974-1.000, P < 0.001) and 63.6% (AUC = 0.988, 95% CI 0.971-1.000, P < 0.001), respectively. Cross-validation confirmed these thresholds, with mean AUC values of 0.992 and 0.993 for short-term and long-term PBD, respectively.
Conclusions
The ARR of the intraoperative BCR waveform showed a high predictive value for PBD in patients with CMCET. We propose a 60% ARR reduction on either side of the BCR waveforms as an exploratory, hypothesis-generating early warning criterion for BCR monitoring during CMCET surgery, pending external validation in independent prospective cohorts before clinical implementation.
Keywords
Introduction
Conus medullaris and cauda equina tumors (CMCETs) represent a distinct entity within spinal cord tumors, characterized by their location at the transition between the central and peripheral nervous systems.1,2 CMCETs are primarily benign tumors, such as ependymomas, schwannomas, lipomas, and dermoid cysts, and surgical resection is typically the recommended therapeutic option.3–5 However, total resection of CMCETs is generally difficult and carries a significant risk of various complications.
New or worsening voiding and defecation dysfunction is one of the most common postoperative complications for CMCET patients. It may manifest as constipation, incontinence, urinary frequency, and urgency, all of which have a substantial impact on the patients’ quality of life. Preserving bladder and bowel function during CMCET resection requires more than surgical technique alone; intraoperative neurophysiological monitoring (IONM) is a crucial adjunct. The application of intraoperative neurophysiological monitoring (IONM) should be both feasible and effective in clinical settings to enhance surgical outcomes. IONM has been utilized in spine and spinal cord surgery since the 1970s. It can provide real-time feedback on the functional integrity of the spinal cord and nerve roots, allowing neurosurgeons to tailor surgical strategies to avoid iatrogenic spinal cord injury.6–8 Several IONM modalities have been developed so far for spine and spinal cord surgery, and the bulbocavernosus reflex (BCR) is the most appropriate one for assessing bladder and bowel function during CMCET resection.
The BCR is the contraction response of the bulbocavernosus muscle under stimulation of the penis or clitoris. It is mediated by the pudendal nerve and can reflect the functional integrity of the sacral reflex arcs at the S2-S4 levels. BCR has been used as an electromyography test to assess sphincter function since the 1950s. In 1997, Deletis and Vodusek first reported in detail intraoperative BCR recording in patients who underwent surgery with a risk of sacral cord injury. 9 To date, only a limited number of studies have investigated intraoperative BCR monitoring, indicating a gap in the research that this study aims to address. Recent studies have clarified the predictive value of BCR monitoring for postoperative bladder function.10–13 In our most recent study, we also verified the correlation between intraoperative BCR alterations and postoperative bladder function and proposed a more precise early warning criterion for BCR monitoring in CMCET surgery. 14 However, few studies have focused on the association between intraoperative BCR alterations and postoperative bowel function. Furthermore, in clinical practice, patients with voiding dysfunction do not necessarily develop bowel dysfunction postoperatively, and vice versa. Accordingly, the investigation of the application value of BCR monitoring for predicting bowel function after CMCET surgery remains significant. In this study, we conducted the aforementioned exploration and proposed a tailored warning criterion for BCR monitoring to preserve bowel function during CMCET surgery.
Methods
Patient Population
This study was conducted in accordance with the STROCSS guidelines. 15 Data of 131 patients who underwent CMCET resection at our hospital between October 2020 and August 2022 were retrospectively reviewed. The same surgical team operated on all patients, and IONM was utilized during every surgery. The inclusion criteria were as follows: (1) being confirmed as CMCETs according to pathological findings; (2) with a preoperative Neurogenic Bowel Dysfunction Score (NBDS) of zero to 6 points 16 ; and (3) undergoing surgery through a posterior median approach. The exclusion criteria were as follows: (1) failure to elicit BCR during surgery; and (2) with insufficient demographic, clinical, or follow-up data. Demographic and clinical data were extracted from the medical record, while the IONM data were sourced from our institutional database. Ethical approval for this study was provided by the Ethics Committee of our hospital. And written informed consent was obtained from all study participants prior to surgery.
Anesthesia
Intravenous-inhalation compound anesthesia was employed for all surgeries. The anesthesia induction was achieved using propofol and sufentanil at a dosage of 1.5-2.0 mg/kg and 0.3 μg/kg, respectively. To maintain anesthesia, a combination of propofol (4.0-6.0 mg/kg/h), remifentanil (0.05-0.20 μg/kg/min), and sevoflurane (at less than 0.5 minimum alveolar concentration) was applied. Muscle relaxants such as rocuronium (0.6-0.9 mg/kg) or atracurium (0.2 mg/kg) were administered for tracheal intubation during the induction phase. The vital signs, including heart rate, blood pressure, oxygen saturation, and end-tidal carbon dioxide levels, were continuously monitored throughout the surgery to ensure patient safety.
BCR Monitoring
BCR monitoring was performed as previously described. 14 The selection and placement of the stimulation electrodes for BCR monitoring varied according to sex. In male patients, the surface electrodes were placed on the proximal (cathode) and distal (anode) sides of the penis’s dorsal surface of the penis. In female patients, the needle electrodes were placed bilaterally on either side of the clitoris. The stimulation parameters were as follows: constant current stimulation delivered in 4 trains, with a pulse width of 600 μs, a stimulus intensity of 30-50 mA, and an inter-stimulus interval of 2 ms. For recording, 2 pairs of needle electrodes were inserted bilaterally into the external anal sphincter muscle at the mucocutaneous junction. The recording parameters included a band-pass filter set between 30 and 1500 Hz and a notch filter at 50 Hz.
The baseline BCR was obtained before the dura was opened. Throughout the surgery, BCR was typically elicited at three-minute intervals, with the frequency increasing every minute or more during the critical phases. An early warning was proposed when a decrease of over 50% in the BCR amplitude on either side was observed. The amplitudes of bilateral BCR waveforms were recorded before the end of surgery, and the side showing higher amplitude reduction (hereafter referred to as “worst-side ARR or maximal ARR”) was used to calculate the amplitude reduction ratio (ARR) using the following formula: ARR=(baseline amplitude-amplitude recorded before the end of the surgery)/(baseline amplitude) *100%. The side showing greater amplitude reduction was used to calculate ARR because it represents the worst-case scenario for sacral pathway integrity, providing the most conservative and clinically safest warning threshold. Potential anesthetic or physiological confounders were minimized by the standardized anesthesia protocol and continuous monitoring of vital signs.
Clinical Assessment and Follow-Up
Bowel function was evaluated using the NBDS at 3 scoring times: preoperatively, 1 month postoperatively, and 6 months postoperatively. Since an NBDS of 0-6 points indicates minimal neurogenic bowel dysfunction, 16 only patients meeting this preoperative criterion were enrolled to ensure that any postoperative bowel dysfunction was iatrogenic in origin. One patient was considered to have new onset postoperative bowel dysfunction (PBD) when he/she had an NBDS of over 6 points one month after surgery. If the NBDS obtained 6 months after surgery was still above 6 points, the patient was defined as having a long-term PBD. Otherwise, it is defined as a short-term PBD.
Comprehensive tumor assessment was performed according to the preoperative imaging data and operative notes. Tumor location, cystic or solid nature, tumor size (maximum diameter), presence or absence of a capsule, and degree of tumor adhesion to neural structures were all thoroughly analyzed as part of the evaluation. Furthermore, the extent of resection was meticulously documented and classified as either total or sub-total.
Statistical Analysis
Statistical analyses were performed using R (version 4.3.2, R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism (version 9.5.1, GraphPad Software Inc., San Diego, California, USA). Categorical variables are presented as frequencies and percentages, while continuous variables are presented as means and standard deviations or medians with interquartile ranges, as appropriate based on distribution. Group comparisons were performed using the Chi-square test, Fisher’s exact test, Student's t-test, or appropriate non-parametric tests. Subsequently, multivariate binary logistic regression analysis was applied to further explore the predictive value of ARR for short-term and long-term PBD. Clinical variables with a P-value less than 0.2 identified through the prior group comparisons were also included in the logistic regression model. The effect size was estimated using the odds ratio (OR) with a corresponding 95% confidence interval (CI). Furthermore, the predictive thresholds of ARR for predicting short-term and long-term PBD were determined by the Receiver Operating Characteristic (ROC) curve analysis, and the predictive efficiency was evaluated by the area under the curve (AUC). 95% CI for AUC values were calculated using the DeLong method. To reduce overfitting risk, stratified 10-fold cross-validation was performed using the predetermined ARR thresholds. Multicollinearity among predictors in the logistic regression models was assessed using variance inflation factors (VIF), with VIF >10 considered indicative of severe collinearity. Model calibration was evaluated using the Hosmer–Lemeshow goodness-of-fit test. The events-per-variable (EPV) ratio was also calculated to contextualize model stability. The level of statistical significance was set at P < 0.05.
Results
Patient Characteristics
A total of 118 patients with CMCET were finally enrolled in this study. A flowchart of the process is shown in Figure 1. A total of 24 patients (20.3%) had new-onset PBD at 1 month postoperatively, of whom 19 (16.1%) met the criteria for long-term PBD at 6 months. Demographics and clinical characteristics of the enrolled patients are presented in Table 1. The cohort had a mean age of 41.5 ± 13.9 years, with 69 males (58.5%) and 49 females (41.5%). The predominant tumor pathology was schwannomas, accounting for 58 cases (49.2%), followed by epidermoid cysts (20 cases, 16.9%), ependymomas (13 cases, 11.0%), teratomas (13 cases, 11.0%), and lipomas (8 cases, 6.7%). The flowchart of the current study Demographic and Clinical Characteristics of 118 Enrolled Patients and Group Comparisons Between Those With and Without Postoperative Bowel Dysfunction Note. PBD, Postoperative bowel dysfunction; aResults of Student t test bResults of Chi-square test cResults of Mann-Whitney U test.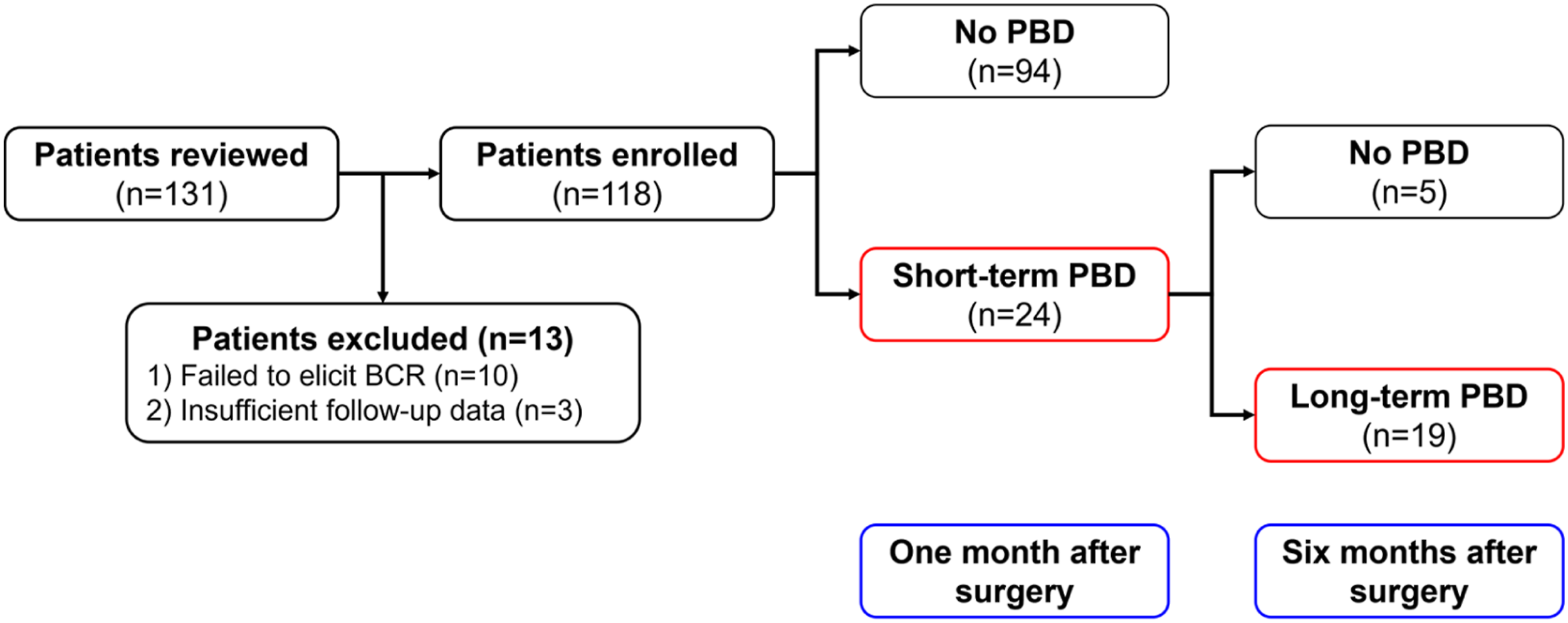
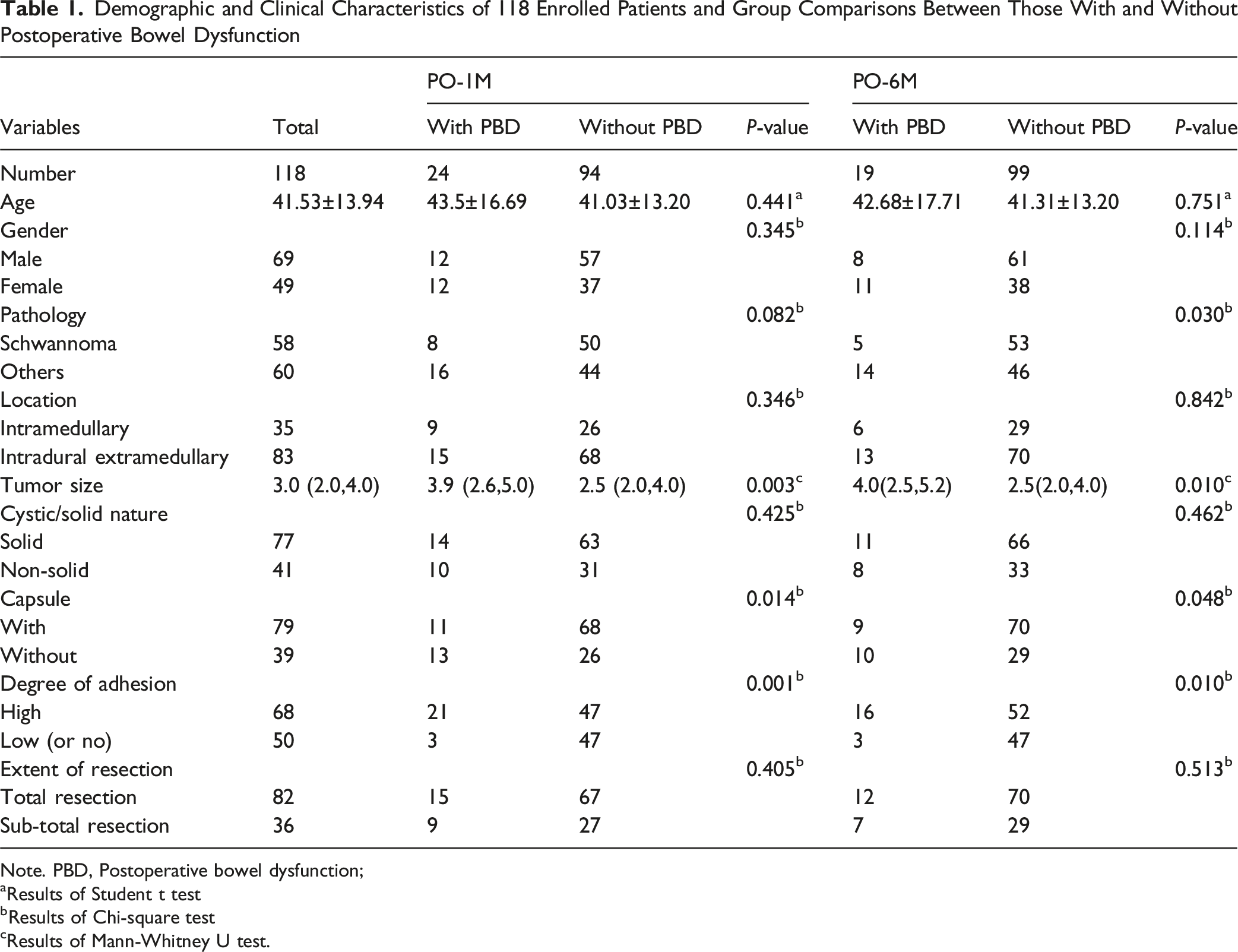
Subsequently, a group comparison was performed between patients with short-term and long-term PBD and those without to identify potential risk factors for PBD. Table 1 presents the results. Patients with larger tumor size (P = 0.003 and 0.010, for short-term and long-term PBD, respectively; Mann-Whitney U test), absence of a capsule (P = 0.014 and 0.048, chi-square test), or high degree of tumor adhesion to neural structures (P = 0.001 and 0.010, chi-square test) were more prone to suffer PBD. Moreover, patients with schwannomas showed a lower chance of suffering long-term PBD (P = 0.030, chi-square test).
The Predictive Value of BCR Monitoring and Other Factors for PBD
The values of ARR were compared between patients with and without short- and long-term PBD. Both patients with short- and long-term PBD exhibited significantly higher ARRs (Figures 2A,B, P < 0.001 for both, Mann-Whitney U test). Multivariate binary logistic regression analysis was conducted as described in the Methods. As shown in Figure 3A,B, ARR emerged as the only independent predictor for both short-(OR 1.287, 95% CI 1.018-1.627, P = 0.035) and long-term PBD (OR 1.153, 95% CI 1.055-1.261, P = 0.002). Comparison of worst-side amplitude reduction ratios (ARR, %) between patients with and without PBD. A: At 1 month postoperatively, patients with short-term PBD exhibited significantly higher worst-side ARRs than those without PBD (P < 0.001, Mann-Whitney U test). B: At 6 months postoperatively, patients with long-term PBD exhibited significantly higher worst-side ARRs than those without PBD (P < 0.001, Mann-Whitney U test) Multivariate binary logistic regression analysis identifying independent predictors of short-term and long-term PBD. Clinical variables with univariate P < 0.2 from group comparisons, together with age and gender, were entered into each multivariable model. Only worst-side ARR achieved independent significance in both models. Points represent odds ratios (OR) with 95% confidence intervals (CI). A: Short-term PBD model; B: Long-term PBD model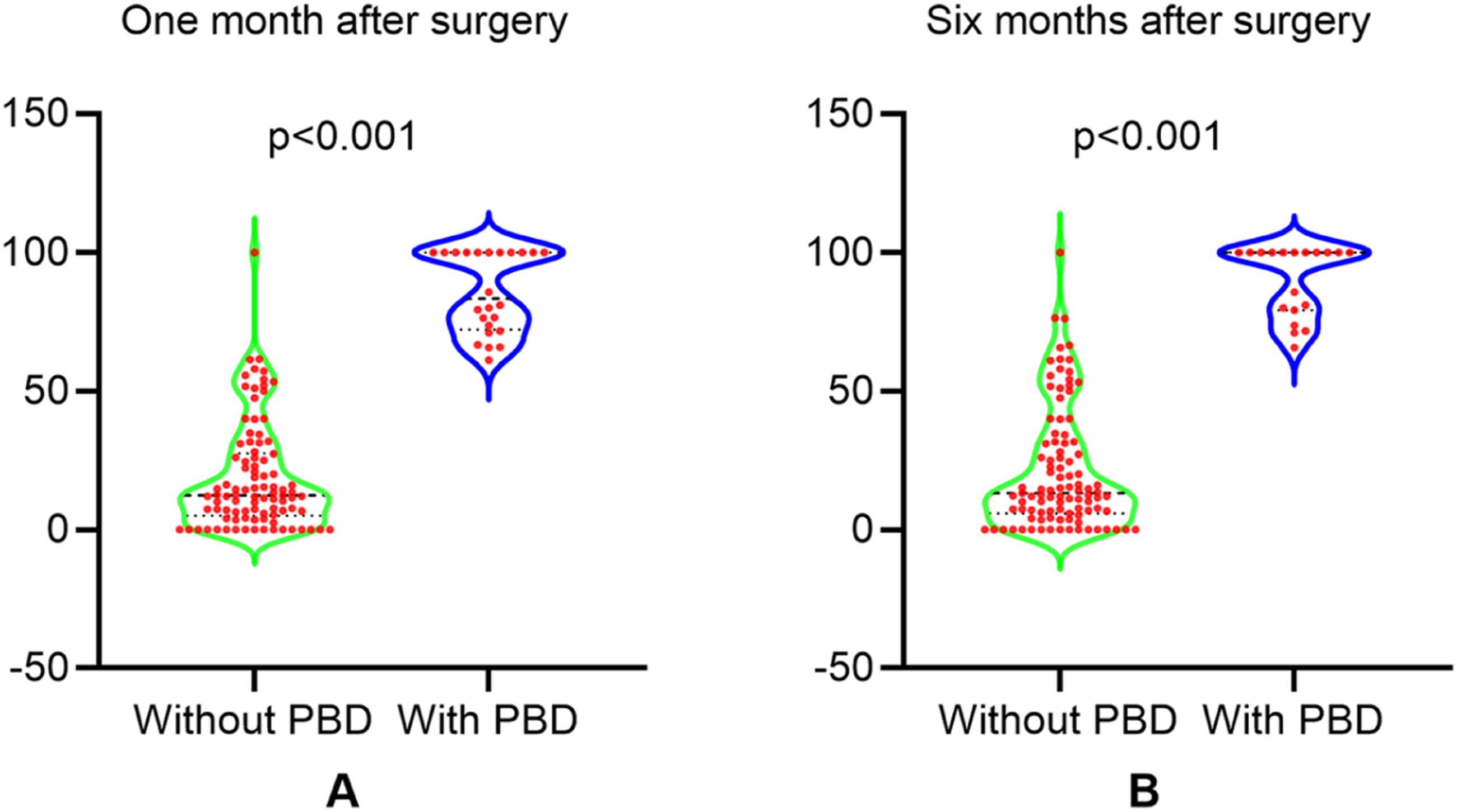

Although tumor size, absence of a capsule, and higher degree of tumor adhesion demonstrated univariate significance, none retained independent significance in multivariate modeling. Collinearity assessment showed VIF values well below the threshold of 10 for both models (1-month model: VIF_max = 5.75; 6-month model: VIF_max = 1.73). Model calibration demonstrated adequate fit (Hosmer-Lemeshow test: 1-month PBD P = 1.000; 6-month PBD P = 0.863). The limited number of outcome events (short-term PBD: 24 events, EPV = 3.43; long-term PBD: 19 events, EPV = 2.71) should be noted in the context of model stability.
A Refined Warning Criterion for BCR Monitoring During CMCET Surgery
To better utilize BCR monitoring in CMCET surgery, ROC curve analysis was applied to identify the critical threshold value of the ARR for predicting PBD. The results are shown in Figure 4. The optimal threshold value for ARR to predict short-term PBD was 59.6%, with a sensitivity of 100% and a specificity of 96.8% (Figure 4A, AUC = 0.991, 95% CI 0.974-1.000, P < 0.001). For predicting long-term PBD, the optimal ARR threshold value was 63.6%, with a sensitivity of 100% and a specificity of 94.9% (Figure 4B, AUC = 0.988, 95% CI 0.971-1.000, P < 0.001). Receiver operating characteristic (ROC) curves for worst-side ARR in predicting short-term and long-term postoperative bowel dysfunction (PBD). AUC, area under the curve. A: Short-term PBD (1 month). B: Long-term PBD (6 months)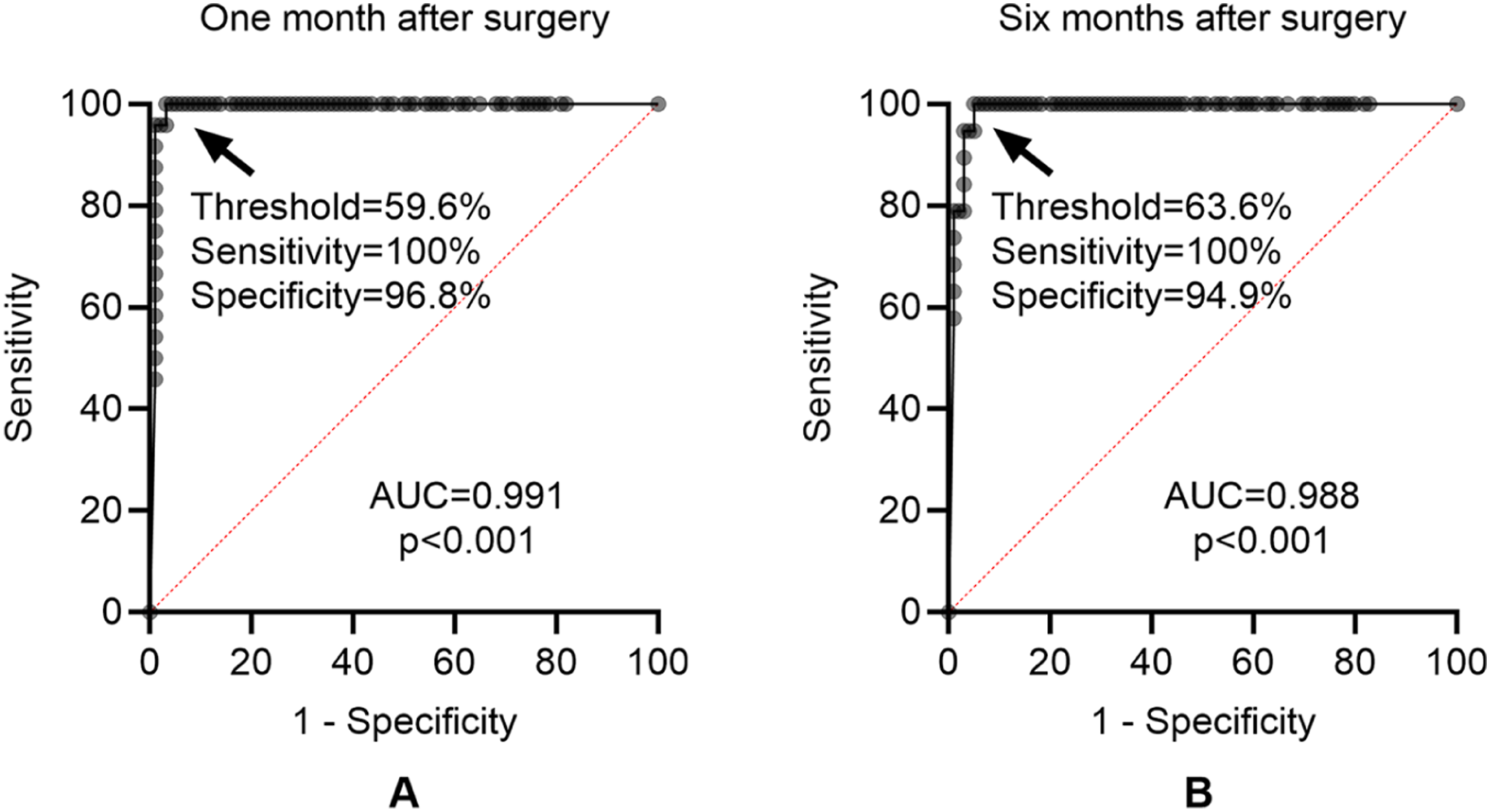
Internal Validation Results Using 10-Fold Cross-Validation at Fixed ARR Cutoffs
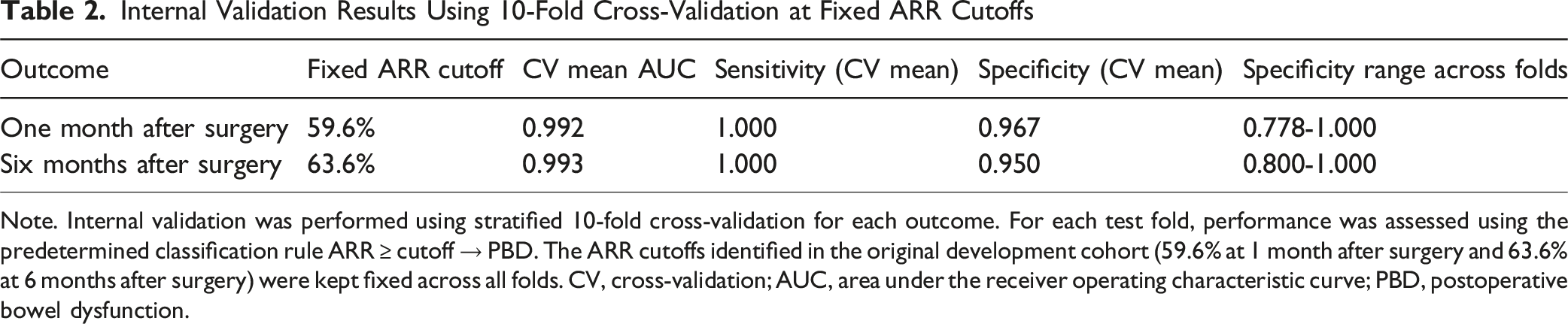
Note. Internal validation was performed using stratified 10-fold cross-validation for each outcome. For each test fold, performance was assessed using the predetermined classification rule ARR ≥ cutoff → PBD. The ARR cutoffs identified in the original development cohort (59.6% at 1 month after surgery and 63.6% at 6 months after surgery) were kept fixed across all folds. CV, cross-validation; AUC, area under the receiver operating characteristic curve; PBD, postoperative bowel dysfunction.
Discussion
The Application of BCR Monitoring in Spine and Spinal Cord Surgery
Spine and spinal cord surgery is one of the earliest applications of IONM. By the late 1970s, somatosensory evoked potential monitoring was already in use for patients with cervical or upper thoracic lesions. In the next few decades, somatosensory and motor evoked potential monitoring, evoked electromyography, and sensory and motor fiber mapping of the cauda equina have been successively applied to assess the function of the sacral nervous structures. Compared to the above modalities, BCR can directly and comprehensively reflect the functional integrity of sensory and motor sacral nerve fibers and is more suitable for the intraoperative monitoring of lumbosacral spinal surgeries. 17 Additionally, the high sensitivity and specificity of BCR monitoring for predicting postoperative voiding dysfunction in patients who undergo lumbosacral spinal cord tumor resection and posterior lumbar fusion have been confirmed.12,13 At our center, we have applied BCR monitoring to spinal cord surgeries since the late 2010s, and the eliciting rate and warning capability were both satisfied.
Although intraoperative BCR monitoring has been applied in clinical practice for over 2 decades, relevant research is still scarce and scattered. This may be mainly due to the low incidence rate of lumbosacral diseases, which makes it challenging to carry out corresponding cohort studies. Even now, BCR is considered an IONM modality that requires further verification for its clinical significance. 18 Overall, clinical evidence regarding the predictive utility of intraoperative BCR monitoring is always required.
The Predictive Value of Intraoperative BCR Monitoring for PBD
Compared to postoperative bladder dysfunction, PBD is clearly a rare topic related to intraoperative BCR monitoring in previous studies. A study performed on 22 infants and children who underwent untethering surgery suggested that BCR monitoring is feasible for preventing postoperative bladder and bowel dysfunction. 19 Additionally, some case reports have focused on the correlation between intraoperative BCR monitoring and postoperative bladder and bowel dysfunction.20,21 To the best of our knowledge, no research has been conducted specifically on the predictive efficacy of intraoperative BCR monitoring for PBD. In addition to the low incidence of relevant lesions, the limited follow-up of bowel function is also a critical reason. One supporting evidence is that studies describing the predictive value of BCR monitoring for sexual function are even rarer.
In the current study, we presented the first large-sample analysis of the effectiveness of intraoperative BCR monitoring in predicting PBD after CMCET surgery. Patients with a more significant ARR of the BCR waveform intraoperatively had a higher probability of suffering short- and long-term PBD. Moreover, the ARR was identified as the sole independent predictor of both short- and long-term PBD. ROC curve analysis further confirmed the high predictive performance of ARR for both short- and long-term PBD, with sensitivity maintained at 100% across both outcomes. In addition, the critical threshold values of ARR for predicting PBD were also obtained through the ROC curve analysis, which could help us improve the early warning criteria of intraoperative BCR monitoring.
A Refined Early Warning Criterion for BCR Monitoring During CMCET Surgery
Our previous study analyzed the correlation between bilateral BCR changes and postoperative voiding dysfunction. Bilateral ARRs both showed excellent predictive performance, with satisfactory sensitivities and specificities. From the neurophysiological perspective, the side of the sacral reflex pathway demonstrating greater amplitude reduction during surgery represents the more severely affected neural pathway. To ensure optimal intraoperative safety, threshold determination should therefore prioritize this more vulnerable side, providing the most conservative warning signal. 14
ROC curve analysis showed that the warning thresholds of ARR for predicting short-term and long-term PBD were 59.6% and 63.6%, respectively. Considering the requirements of clinicians and patients, we propose a 60% amplitude reduction on either side of the BCR waveform as an exploratory early warning criterion for PBD after CMCET surgery. This is inconsistent with the corresponding recommendation we proposed in our previous study (a two-thirds amplitude reduction). This is not contradictory. On the contrary, this proves the inconsistency between postoperative bladder and bowel function. From a scientific research perspective, the correlations of intraoperative BCR changes with postoperative bladder, bowel, and sexual functions should be distinguished. From a clinical practice perspective, we do not want patients to experience any dysfunctions. Consequently, the correlations between intraoperative BCR changes and different functions should be considered together, and a more conservative early warning criterion should be the priority recommendation. From this point of view, the current study further refined the early warning criteria proposed in the previous study.
While BCR was prioritized for its direct reflection of sacral reflex arcs, comparison with other IONM modalities (eg, Somatosensory evoked potential, Motor evoked potential, pudendal somatosensory evoked potential and sphincter EMG) was beyond the scope of this study, which focused specifically on bowel function.
The 60% ARR threshold, although slightly more conservative than the ROC-derived values, was chosen with clinical safety in mind. Although statistically significant predictors do not always translate directly into intraoperative decision-making, the exceptionally high sensitivity (100%) in this cohort supports its use as a practical early-warning criterion until external validation is available. We acknowledge that the very high AUC values may reflect model overfitting given the small number of outcome events. However, stratified 10-fold cross-validation yielded mean AUC values consistent with development cohort values, suggesting the thresholds are not merely artifacts of the training data. Importantly, the present study evaluated the predictive rather than preventive value of BCR monitoring. Whether acting upon ARR warnings can improve bowel outcomes requires future interventional studies. As single-center retrospective findings, external validation in independent prospective cohorts is essential before clinical implementation.
Other Factors Affecting Postoperative Bowel Function
While tumor-related factors such as larger size, absence of a capsule, and higher degree of adhesion were identified as risk factors for PBD in univariate analysis, none achieved independent predictor status in multivariate modeling. One possible explanation is that these anatomical and operative features may influence postoperative bowel function primarily through their mechanical impact on sacral neural pathways—an effect that is likely captured in real time by intraoperative BCR amplitude changes. Once ARR is included in the model, the incremental contribution of these variables may diminish substantially. Additionally, the limited number of outcome events further reduced statistical power, and VIF analysis confirmed no severe multicollinearity in either model. Model calibration was satisfactory in both models; notably, the Hosmer–Lemeshow P-value of 1.000 in the 1-month model likely reflects near-perfect separation by ARR rather than miscalibration. Clinically, these tumor characteristics nonetheless remain important surgical considerations warranting heightened vigilance and meticulous neurophysiological monitoring.
Limitations
The current study has several potential limitations. First, as a retrospective single-center study, selection and information bias are inherent; external validation in independent, preferably multicenter prospective cohorts is essential to confirm generalizability. Second, the number of outcome events was relatively small (24 short-term and 19 long-term PBD), which may affect the stability of logistic regression estimates and ROC thresholds; the extremely high AUC values should be interpreted with this in mind, notwithstanding the reassuring cross-validation results. Third, this study evaluated predictive rather than preventive efficacy; whether acting upon ARR warnings can improve bowel outcomes requires future interventional studies. Fourth, bowel function was assessed solely using NBDS; quality-of-life impact and sexual function were not evaluated. Fifth, the selection of worst-side ARR was guided by neurophysiological rationale and prior published work, but a formal empirical comparison with alternative bilateral ARR definitions was not performed within the current cohort, warranting future investigation.
Conclusions
The current study evaluated the application value of intraoperative BCR monitoring in predicting PBD after CMCET surgery. The ARR of the BCR waveform with more significant intraoperative changes emerged as the sole independent predictor for short-term and long-term PBD, with critical threshold values of 59.6% and 63.6%, respectively. Given these clinical considerations, we propose an exploratory 60% amplitude reduction on either side of the BCR waveforms as an early warning criterion pending external validation in independent prospective cohorts before any clinical implementation can be considered.
Footnotes
Author Note
Ke Li is the first author. He is the member of AO Spine, and his AO Membership ID is pp500129865.
Ethical Considerations
This study was approved by the Ethics Committee of Beijing Tiantan Hospital (KY2022-080-01).
Consent to Participate
And written informed consent was obtained from all study participants prior to surgery.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Capital’s Funds for Health Improvement and Research (2022-2-1073).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
Disclosures
The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this article.