
Abstract
Study Design
Retrospective cohort study.
Objective
To elucidate the risk factors of intraoperative neurophysiological monitoring
Methods
We reviewed 1 024 patients with idiopathic scoliosis who underwent deformity correction and were followed-up for ≥1 year. The pre-and postoperative Cobb angle of the major structural curve, operative time, estimated blood loss (EBL), number of levels fused, event that caused the IONM alert, and intervention required for the recovery of the signal were recorded. Patients who received IONM alerts (alert group) and those who did not (non-alert group) during the operation were compared.
Results
Compared to the non-alert group, the alert group had a significantly greater preoperative Cobb angle of the major structural curve (P < .001), number of levels fused (P = .003), operative time (P < .001), and EBL (P < .001). The percentage of correction did not significantly differ between the 2 groups (P = .348). Eight patients (.8%) underwent a staged operation because the IONM signal alert hindered correction of the deformity. The percentage of correction of patients who underwent staged operation was 64.9 ± 15.1%, and no permanent neurologic deficits occurred.
Conclusion
A greater magnitude of preoperative deformity and surgical extent increases the risk of cord injury identified by IONM alerts during correction of deformities in patients with AIS. However, in patients in whom the IONM alert cannot be recovered or reproduced by proceeding with deformity correction, surgeons can minimize the risk by aborting the initial procedure and completing the correction using staged operations.
Keywords
Introduction
Although the incidence of spinal cord injury following deformity correction in patients with adolescent idiopathic scoliosis (AIS) remains low (.3-1.4%), it could cause severe sequelae, including paraplegia.1-3 The efficacy of intraoperative neurophysiological monitoring (IONM), which enables surgeons to appropriately deal with situations that could harm the spinal cord, has been proven in many previous studies.1,2,4,5 Among monitoring techniques, multimodal IONM, including somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs), has gained popularity owing to its high sensitivity and specificity in detecting cord injuries.6-9 It has been reported that the sensitivity, specificity, and positive predictive value of multimodal IONM could be up to 100%, 98.5%, and 85%, respectively, when used for the surgical treatment of AIS. 10
When an IONM signal alert is associated with a specific surgical procedure that is reversible, surgeons can correct the procedure that caused the alarm.2,4,11 Mispositioned screws can be replaced, or excessive curvature correction could be released.2,4 Furthermore, previous studies have demonstrated that simply increasing mean arterial pressure (MAP) could result in recovery of IONM signal abnormality in many cases. 12 However, IONM signal abnormality may not always be reversible, and correction of the AIS curvature itself may cause IONM signal alerts. 12 Previous reports have suggested that when the IONM signal does not recover despite reversible measures or correction of the curvature itself leads to repeated IONM alerts, surgical procedures should be aborted due to the risk of paraplegia.2,4,13 However, aborting the procedure without proceeding to deformity correction would mean failure of surgery. It is also unclear how surgeons could cope with such situation to achieve appropriate deformity correction while avoiding the risk of spinal cord injury. 2 Although performing staged procedure have been suggested, the outcomes or complications of staged operation due to IONM signal alert has not been reported.
Therefore, the current study was conducted to 1) elucidate the risk factors of IONM alert during deformity correction surgery for AIS and 2) describe the outcomes of patients who underwent staged correction surgery due to IONM alert during the initial procedure.
Materials and Methods
Study Design and Participants
This retrospective cohort study was approved by the Institutional Review Board of our institute (Asan Medical Center Institutional Review Board, S2022-2098-0001). The requirement for informed consent was waived owing to the retrospective nature of the study. A total of 1 347 patients who underwent deformity correction for AIS between July 2013 and March 2021 were retrospectively reviewed. The inclusion criteria were
1
age between 12 and 18 years at the time of the operation and
2
idiopathic scoliosis without associated syndromes. The exclusion criteria were
1
revision procedures
2
; patients who underwent surgery involving anterior or middle column osteotomy;
3
congenital or syndromic scoliosis; and
4
follow-up period of <1 year (Figure 1). All operations were performed by 2 surgeons at a single institute. Surgical techniques of instrumentation and reduction were similar between the 2 surgeons. The posteroanterior image-intensifier rotation technique was used for correct pedicle screw insertion.
14
Long rod was contoured according to the coronal shape of the curvature and was applied on the concave side of the main curve. This rod was derotated 90° counter-clockwise for deformity correction. The second rod contoured according to the desired sagittal plane shape and was inserted in the other side. An additional compression-distraction maneuver was performed to achieve further correction.15,16 Patient selection process.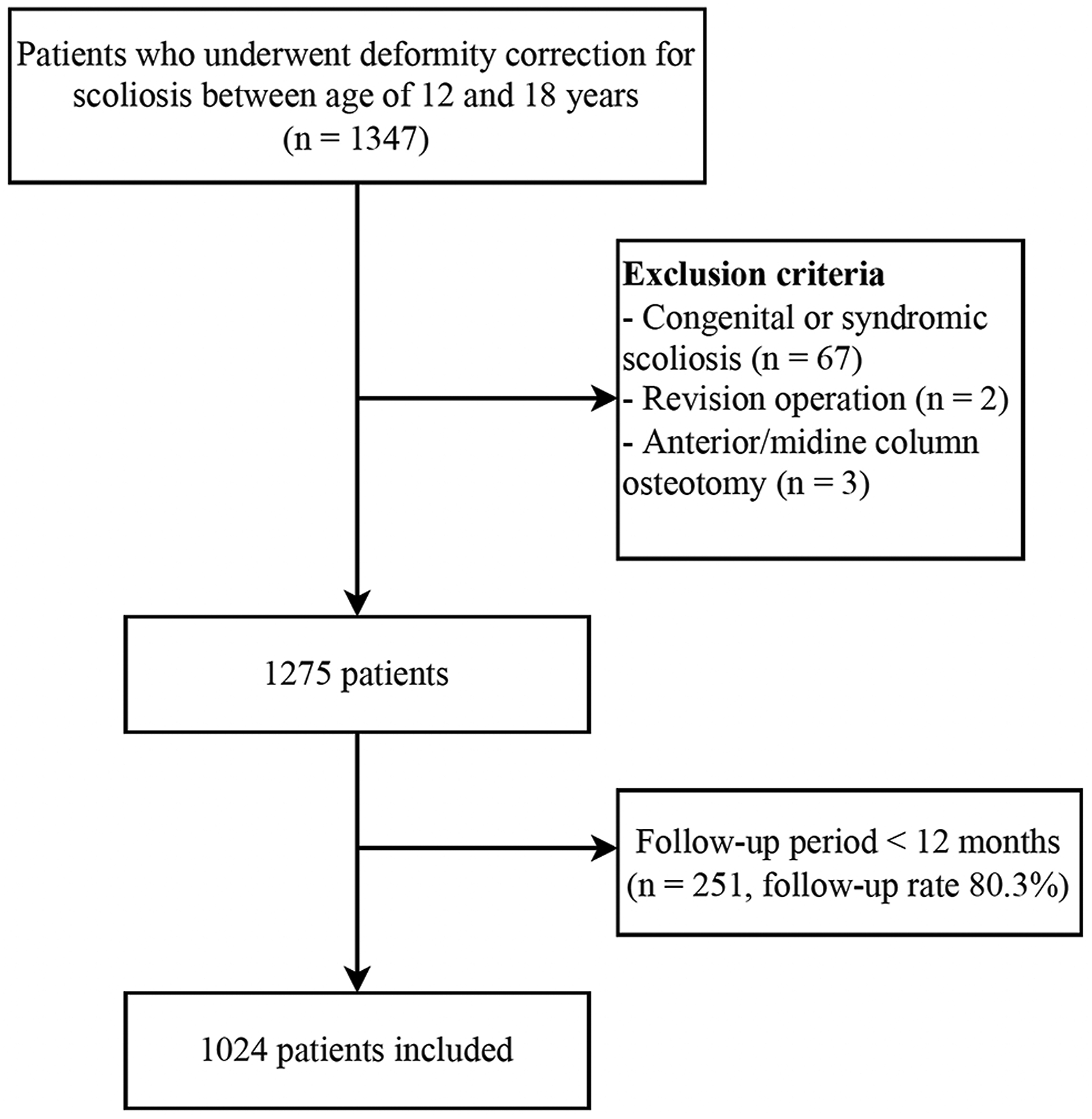
Multimodal IONM was performed in all operations. Total intravenous anesthesia was performed until the termination of IONM, as inhalational anesthetics could affect IONM signals.17-19 IONM signal level change showing a ≥50% reduction in SSEPs or MEPs was defined as an IONM signal alert.7,20 Furthermore, such signal level change needed to be unresponsive to an increased voltage from stimulation to be accepted as an alert. Signal latency change was not considered a criterion because it has been reported to have less diagnostic value in previous studies.2,7,21 Patients who experienced IONM signal alert during surgery were classified as the “alert group” while patients without IONM alert during operation were defined as the “non-alert group.”
Interventions in Cases of IONM Signal Alert
When an IONM signal alert occurred, the anesthesia team first reviewed the MAP and hemoglobin levels. The MAP was increased above 90 mmHg or 15% above the baseline pressure to restore perfusion to the spinal cord. 12 Transfusion was performed when necessary. If the IONM signal was not recovered despite the above measures, the surgeon reviewed the surgical procedure that seemed to be associated with the alert and attempted reverse the procedure, by removing the rod or releasing compressions/distractions. Removal of intraoperative halo traction was also considered if it was applied. However, when the IONM signal abnormality was not reversible or an alert was repeated by corrective maneuvers, the operation was aborted without completing deformity correction. For aborted cases, a second-stage operation was performed after a week. During the interval between the 2 operations, the patients were kept in bed while limiting the head elevation below 30° because the rod was not connected in most cases.
Variables
Data including age, sex, body mass index, Lenke curve type, number of fused levels, estimated blood loss (EBL), operation time, amount of transfusion, and application of intraoperative halo-traction were recorded. Radiographic measurements were performed preoperatively and 1 year postoperatively. Radiographic measurements and curve-type classifications were performed by the surgeon at the time of surgery and follow-up. The Cobb angle of the major structural curve in the standing and bending radiographs was measured. Thoracic kyphosis was measured as the Cobb angle between T5 and T12 on sagittal whole-spine radiographs. The flexibility of the major structural curve was calculated as follows: (Cobb angle of major structural curve in preoperative standing radiograph – Cobb angle of major structural curve in bending radiograph)/(Cobb angle of major structural curve in preoperative standing radiograph) × 100 (%). Furthermore, the percentage of correction of the major structural curve was calculated as follows: (Cobb angle of major structural curve in preoperative standing radiograph – Cobb angle of major structural curve in 1-year postoperative radiograph)/(Cobb angle of major structural curve in preoperative standing radiograph) × 100 (%). Trigger events that caused IONM signal alerts and interventions were also recorded for patients in the alert group.
Statistical Analysis
Comparisons were made between the alert and non-alert groups. All variables were tested for normality using the Shapiro-Wilk test. Continuous variables were analyzed using Student’s t-test, and categorical variables were analyzed using the chi-square test. Statistical analysis was performed using Statistical Package for the Social Sciences software (version 21.0; SPSS Inc, Chicago, IL, USA). Statistical significance was set at P < .05.
Results
Patient Clinical Characteristics
Patient and scoliosis curvature characteristics in both groups.
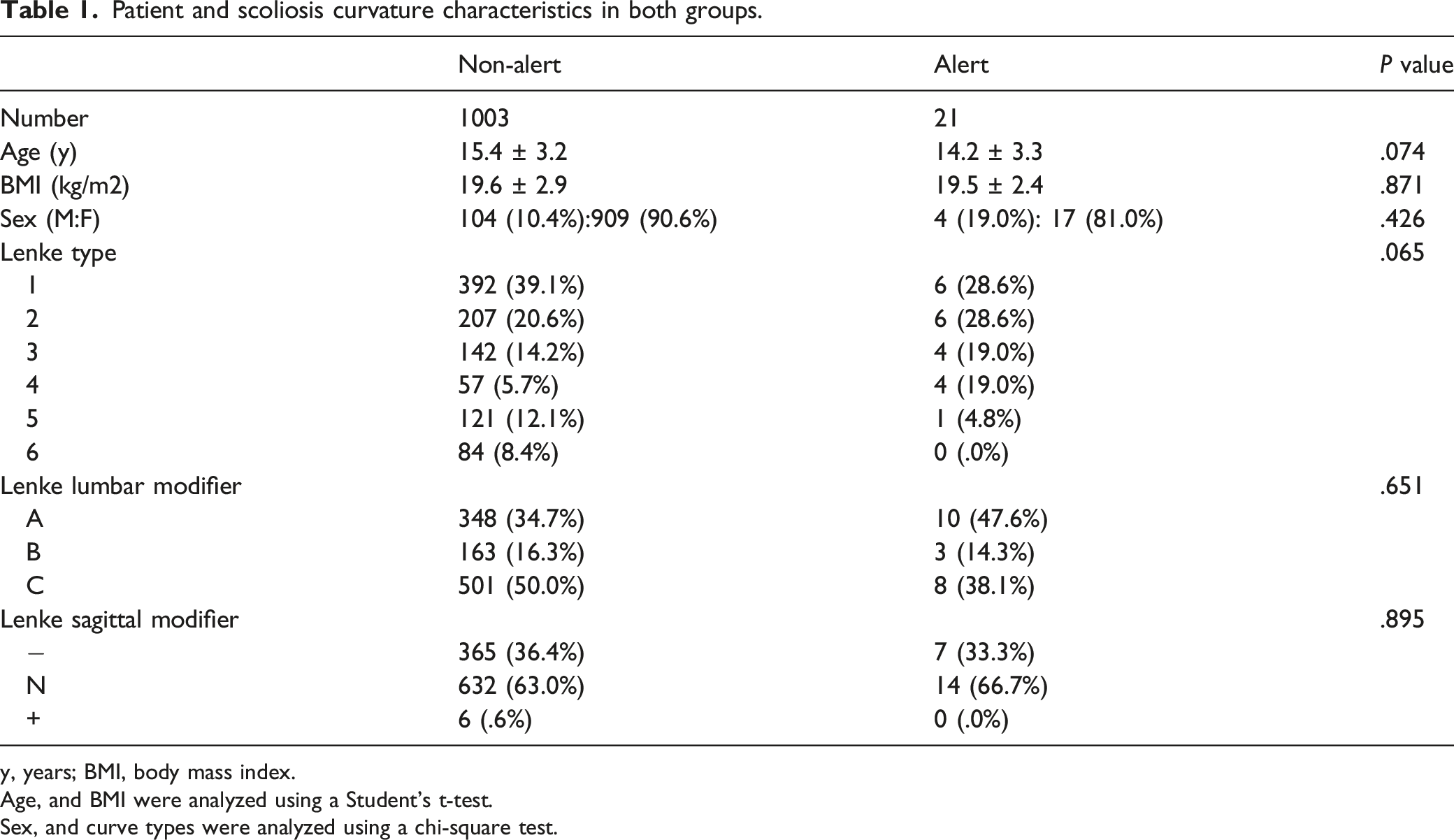
y, years; BMI, body mass index.
Age, and BMI were analyzed using a Student’s t-test.
Sex, and curve types were analyzed using a chi-square test.
Comparison of Perioperative Factors and Postoperative Results
Perioperative factors and postoperative results in both groups.
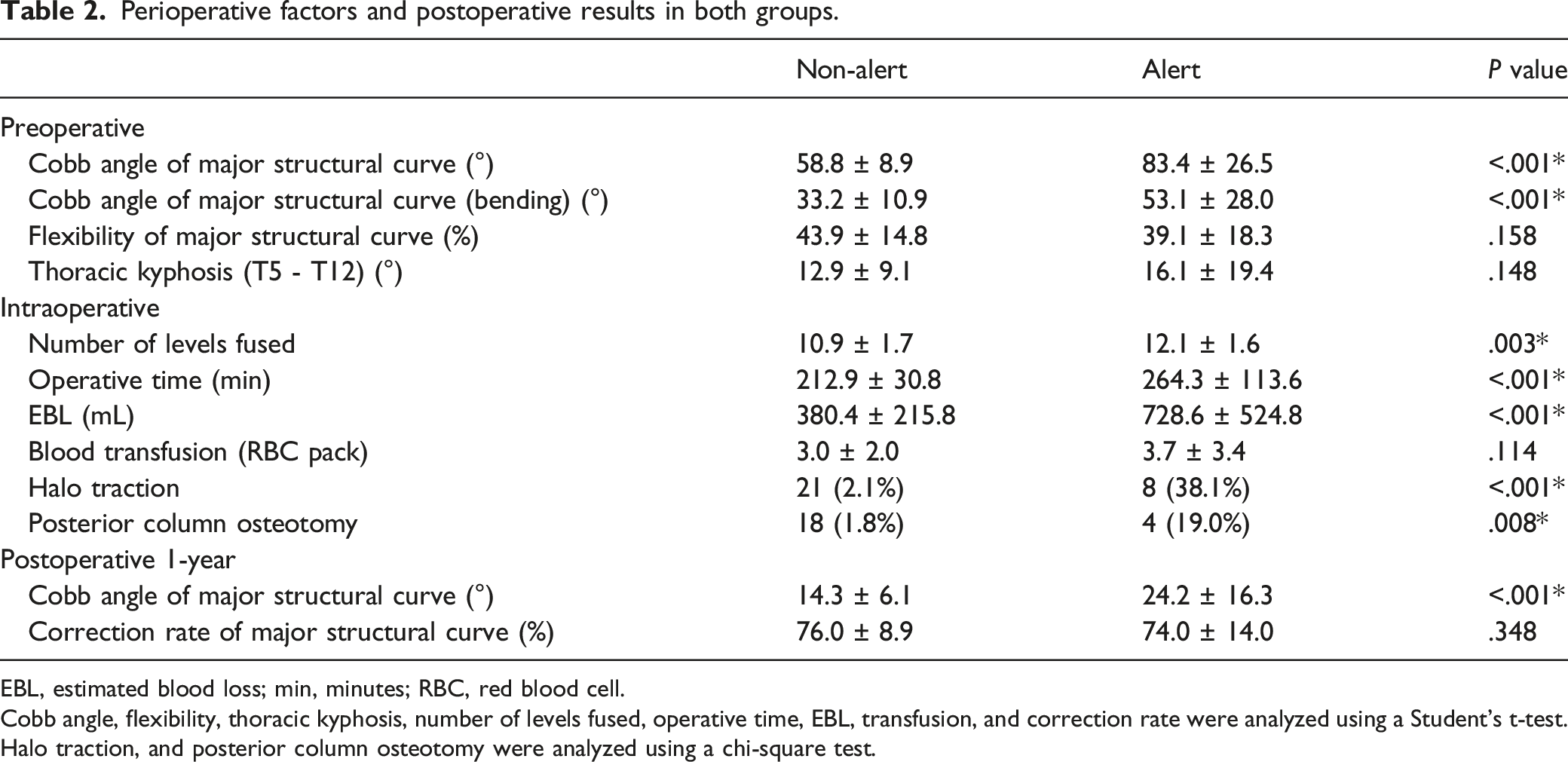
EBL, estimated blood loss; min, minutes; RBC, red blood cell.
Cobb angle, flexibility, thoracic kyphosis, number of levels fused, operative time, EBL, transfusion, and correction rate were analyzed using a Student’s t-test.
Halo traction, and posterior column osteotomy were analyzed using a chi-square test.
Triggering Event of IONM Alert and Interventions in Response
Triggering event that caused neuromonitoring signal alert.
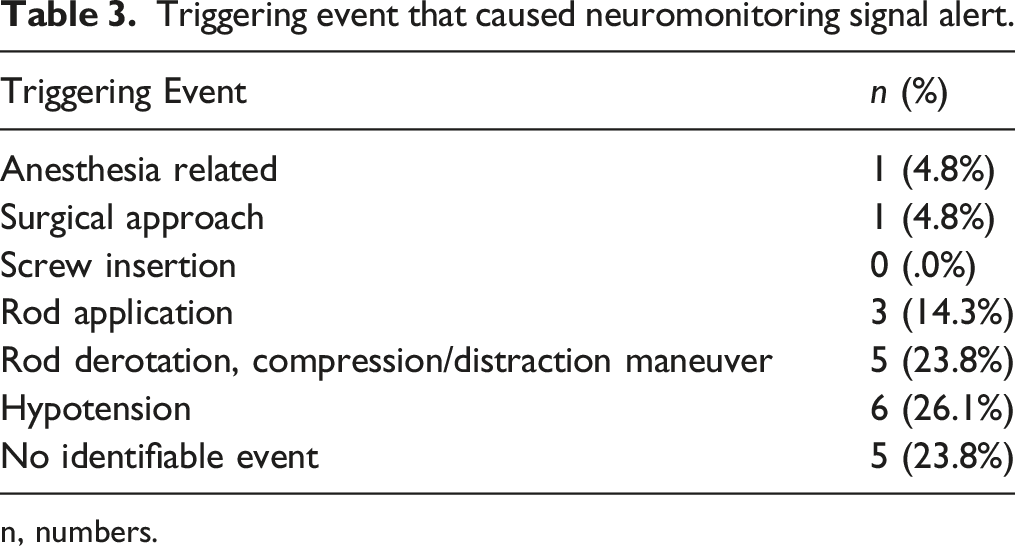
n, numbers.
Measures performed that resulted in neuromonitoring signal recovery.
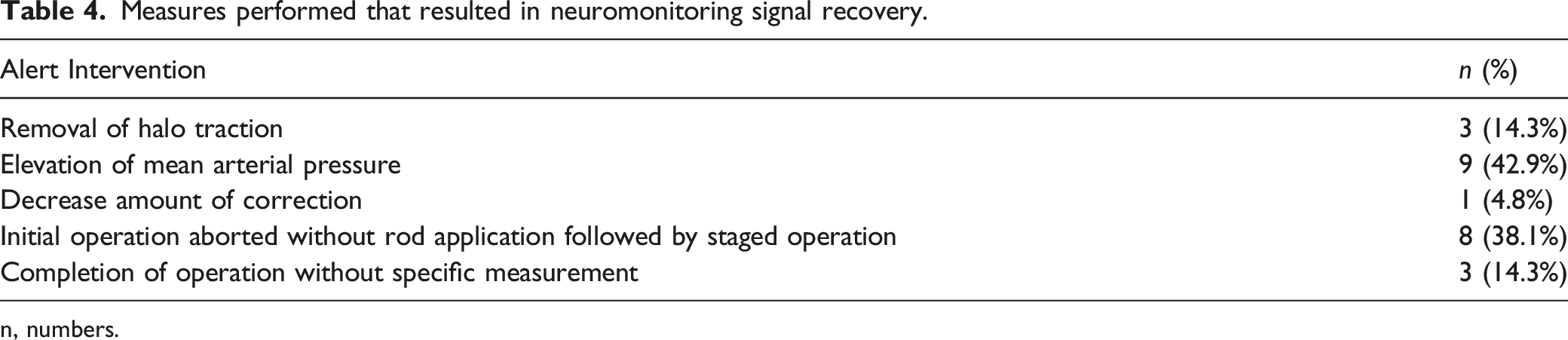
n, numbers.
Illustrative case 2 (Patient 8) (A) A 13-year-old female presented with back deformity. Preoperative radiograph showed the Cobb angle of the major structural curve was 116°. (B) While performing deformity correction MEP signal flattened during single rod application which did not respond to increasing mean arterial pressure. (C) MEP signal recovered after rod removal. The initial operation was aborted with deformity correction planned for second stage operation. Postoperatively, bilateral lower extremity motor grade was identified as grade 3. High-dose dexamethasone was administered, and lower extremity motor power was fully recovered at postoperative day 3. (D) Second stage operation was performed 5 days after the initial operation which was uneventful and resulted in successful deformity correction. (E) Degree of correction of 74.1% was identified at postoperative one-year radiograph, although coronal imbalance was also noted.
Staged Operation in Response to IONM Alert
Details of patients who underwent staged operation due to neuromonitoring signal alert.
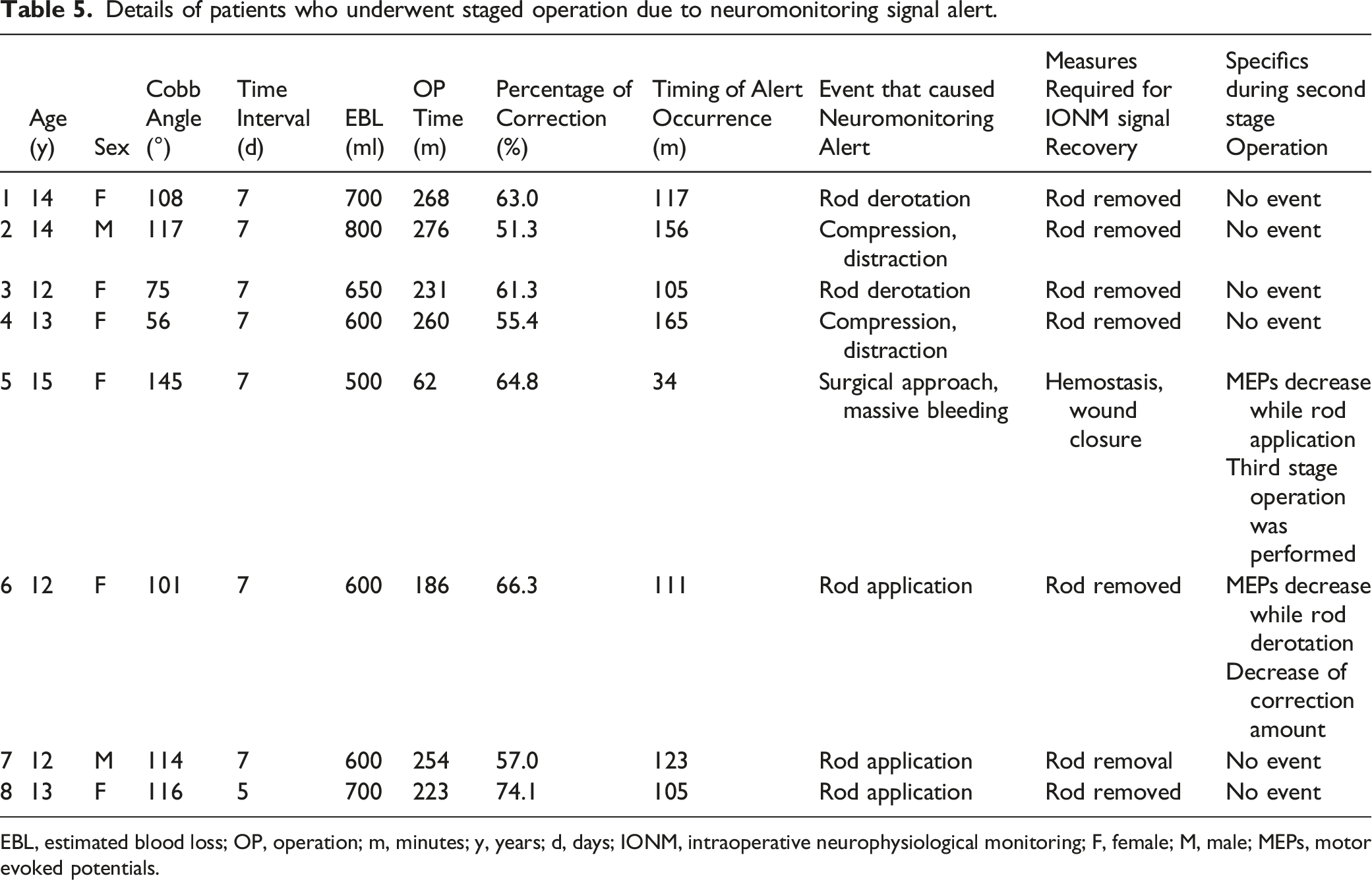
EBL, estimated blood loss; OP, operation; m, minutes; y, years; d, days; IONM, intraoperative neurophysiological monitoring; F, female; M, male; MEPs, motor evoked potentials.
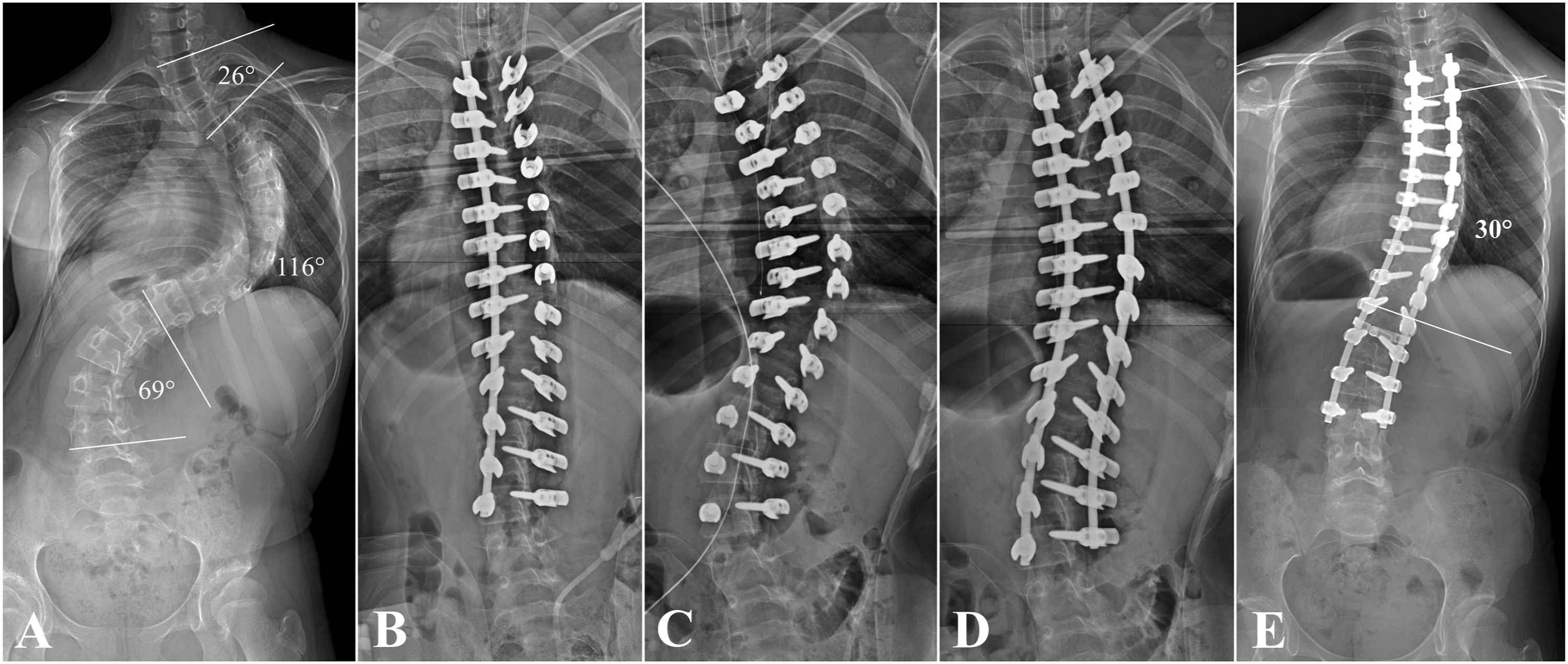
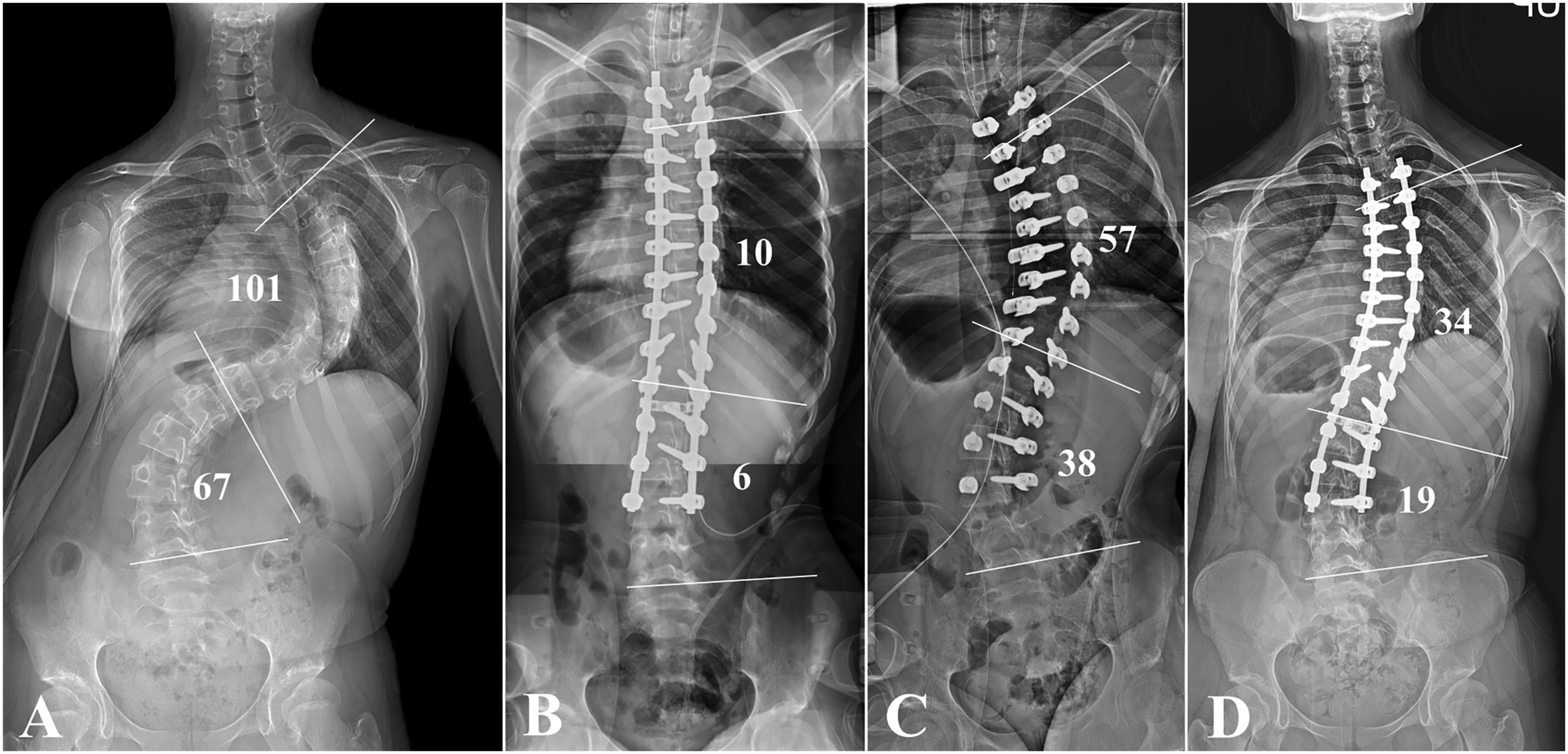
The staged operation was performed after 6.8 ± .7 days. For 6 patients (75.0%), no specific event or IONM signal alert occurred during the second-stage operation (Figure 3). However, IONM signal alert again occurred during rod derotation in 1 patient, which required a decrease in the amount of correction (Figure 4), and 1 patient required a third-stage operation since the MEP decrease recurred during rod application. When comparing patients who underwent staged operation with those who had single stage operation, patients with staged operation had significantly greater preoperative Cobb angle of major structural curve (104.0 ± 27.4 vs 59.2 ± 9.6, P < .001) and a more rigid curvature (flexibility, 27.9 ± 13.3% vs 44.0 ± 14.9%, P = .003). Furthermore, patients who required staged operation demonstrated a significantly greater postoperative 1-year Cobb angle of major structural curve (40.7 ± 12.0° vs 14.3 ± 6.2°, P < .001) with a lower percentage of correction (64.9 ± 15.1% vs 76.1 ± 9.0%, P = .001). Nevertheless, the percentage of correction of patients with staged operation still reached 64.9 ± 15.1%. Total SRS-22 score changed from 2.3 ± .2 preoperatively to 2.7 ± .1 at 1-year postoperative period (P = .161). Illustrative case 1 (Patient 1) (A) Deformity correction was planned for 14-years-old female patient who was diagnosed with AIS. Preoperative Cobb angle of the major structural curve is 108°. (B) Left lower extremity MEP amplitude decrease of >80% occurred while performing rod derotation. The operation was aborted without rod application since MEP signal alerts were repeated with attempting deformity correction. (C) Second stage operation was performed after a week. One-year postoperative radiograph demonstrates successful deformity correction with a percentage of correction of 63.0%. Illustrative case 3 (Patient 6) (A) A 12-year-old female patient presented with deformity of back. Preoperative radiograph demonstrates that the Cobb angle of the major structural curve is 101°. (B) Deformity correction was performed while applying intraoperative halo traction. Although correction of deformity was successful with percentage of correction rate >90%, MEP signal flattened after completing the correction. (C) Decreasing the amount of correction did not recover the MEP signal, and therefore, both rods were removed. (D) Second stage operation was performed after a week with lessened degree of correction. One-year postoperative radiograph demonstrates major structural curve Cobb angle of 34° with percentage of correction of 66.3%.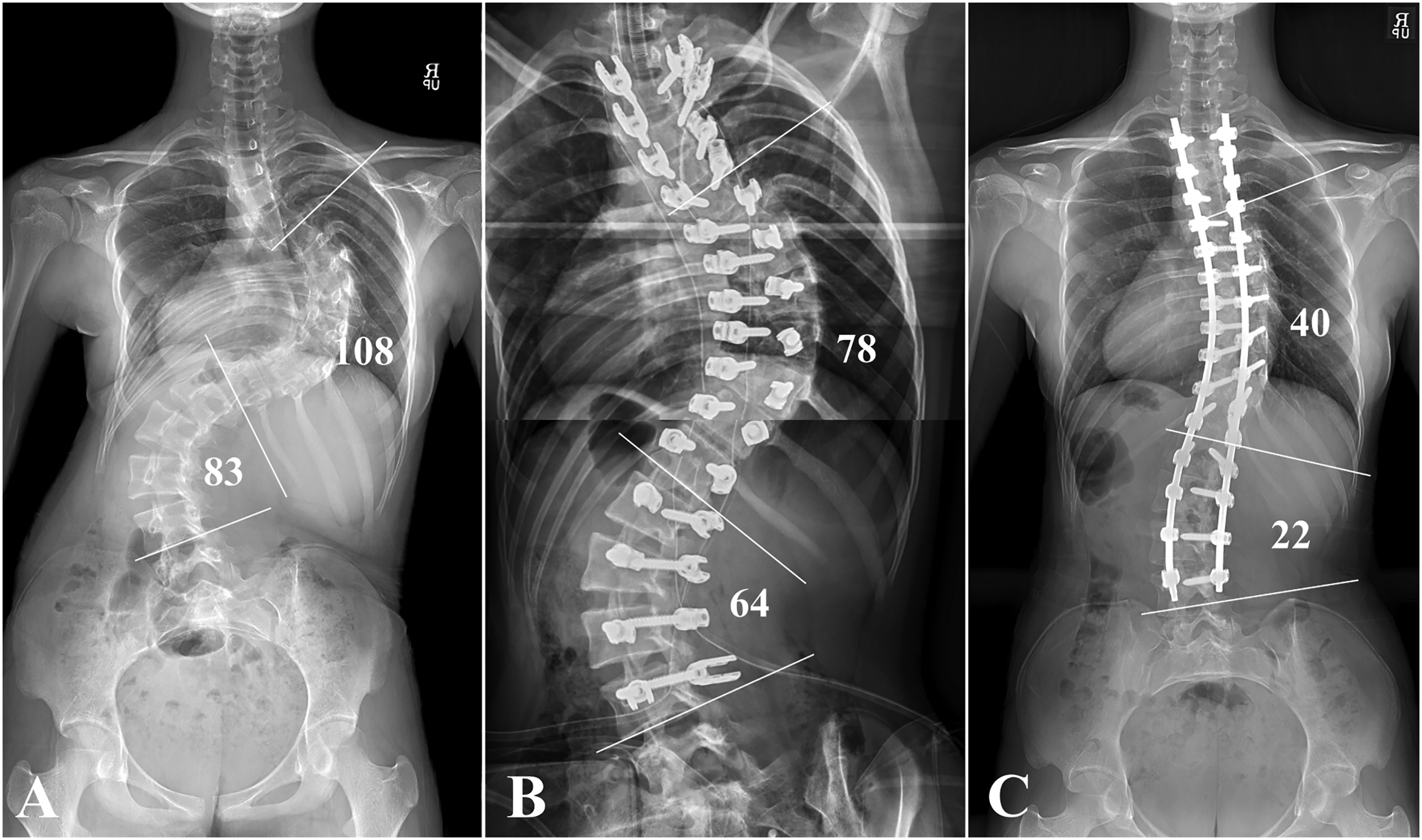
Discussion
Although previous studies have demonstrated the efficacy of multimodal IONM in detecting the possibility of spinal cord injury, measures for surgeons to manage alert situations are not always evident.17,22,23 The present study demonstrated that patients who had IONM signal alert had more severe deformities and more extensive operations characterized by increased number of levels fused, operative time, and EBL. Intraoperative halo traction and PCO were also performed more frequently in the alert group. Hypotension was the most frequent cause of IONM alerts, and elevation of MAP was also most frequently associated with IONM signal recovery. When IONM signal alert hindered proceeding with the deformity correction, staged operation was performed after aborting the initial procedure, resulting in a percentage of correction of 64.9 ± 15.1% while causing no neurologic deficit. No patients had permanent neurologic deficits in either the alert or non-alert group, and 1 patient (.1%) suffered temporary lower extremity weakness.
The current study suggests that greater deformity and increased surgical extent are associated with an increased risk of IONM alerts, which has also been demonstrated in previous studies.2,21,24 Longer operation and greater blood loss due to increased surgical extent might have caused hypoperfusion to the spinal cord, although not always demonstrated as a decrease in MAP.2,12,25,26 The results of the present study showed that hypotension was the most frequent event that caused IONM alerts, and an increase in MAP most often resulted in signal recovery and emphasizes the significance of maintaining cord perfusion during operation. Kobayashi et al suggested that early spinal cord impairment caused by cord ischemia due to excessive bleeding causes MEPs waveform deterioration, although blood pressure does not always differ significantly. 6 Yang et al reported that increasing MAP as a first response after the loss of IONM signals was successful in 20% of patients, and 60% of patients had a return of IONM signals after an increase in MAP in conjunction with other interventions. 12
Furthermore, patients with greater preoperative deformities would experience more rapid changes in spinal cord trajectory during deformity correction.22,27 Changes in the spinal cord trajectory in a spinal cord that is already prone to hypoperfusion due to extensive operation would have increased the risk of cord injury which caused IOMN alert.2,12 In the same context, surgical procedures that caused changes in the spinal cord trajectory, including rod application, derotation, and compression/distraction, most frequently caused IONM alert (38.1%) in the present study. Kobayashi et al reported that rod derotation was the most common procedure that led to IONM alert, and patients with greater preoperative deformity often experienced such alerts. 6
Patients in the alert group underwent PCO and intraoperative halo traction more frequently. Buckland et al reported that performing Ponte osteotomy during deformity correction for AIS increases the risk of IOMN alerts. 21 Feng et al identified osteotomy procedures and intraoperative traction as risk factors for IONM alert because they are associated with increased corrective force and the possibility of injury to the spinal cord. 28 Performing PCO increases the operative time and EBL. Intraoperative halo traction would have caused distractive stress to the spinal cord and 3 patients required halo traction removal as well as an increase in MAP for the recovery of IONM signal abnormality. 29 Therefore, surgeons should be aware of the increased risk of IONM alertness or cord injury when osteotomy or intraoperative halo traction is planned.2,21,22,28
Eight of the 21 patients who received IONM alert required staged operation after abortion of the initial procedure. Considering that hypotension and more extensive surgery are associated with the risk of IONM alert, these 8 patients who were not able to complete the initial procedure would have experienced increased stress to the spinal cord due to hypoperfusion and changes in spinal cord trajectory. 12 Furthermore, repeating the correction maneuver when the IONM alert is irreversible or repeated increases the risk of cord injury. 2 The interval between the initial procedure and the staged operation would provide time for the spinal cord to recover from the insult that occurred during the first surgery, and be more tolerant to injury during deformity correction during the second operation. With this strategy involving a staged operation, we experienced no permanent neurological deficit among the 1 024 patients included. Furthermore, although the percentage of correction of patients who underwent staged operation was lower than that of those who underwent single-stage operation, the percentage of correction still reached 64.9 ± 15.1%. Therefore, staged operation in cases of irreversible IONM alert could be considered a strategy that could successfully achieve deformity correction for AIS while enhancing safety regarding spinal cord injury. 30
While a pre-established checklist or algorithm in case of IONM alert during AIS deformity correction could be helpful, management of IONM signal change is complex and remains a topic of debates.4,12,17 When association between IONM alert and surgical or anesthesiology procedure is clear, those procedures could be fixed. 2 Other established measures, including increasing MAP, removing halo traction, decreasing the correction magnitude, and simply waiting for signal improvement, should also be attempted.2,4,12,21 Possible attempts should be performed to achieve successful deformity correction in the initial operation, since although staged operation would be an option, it still increases patient discomfort and hospital stay. However, considering that preventing serious neurological deficits is of utmost importance, surgeons should carefully consider proceeding to staged operation when proceeding with deformity correction during the initial operation increases the risk of cord injury.
The current study has several limitations. First, since the incidence of IONM alerts is low (2.1%), performing multivariate analysis was not possible. Only a univariate two-group comparison was performed in this study, as multivariate analysis is not recommended when the incidence of index cases is below 10%. 31 This limits the capacity of this study to identify the risk factors for IONM more clearly, and the relationship between multiple factors that demonstrated significant results in the current study should be further analyzed. Second, the frequency of performing PCO during surgery was relatively low compared to other studies, which limits the capacity to demonstrate osteotomy as a risk factor for IOMN alert.21,22 Third, while number of levels fused is significantly different between the non-alert (10.9 ± 1.7) and alert groups (12.1 ± 1.6, P = .003), the difference between the 2 groups is small which may lack clinical significance. However, the result would signify a trend that a more extensive operation is associated with risk of IONM alert. Finally, the inherent bias of being a retrospective analysis cannot be excluded.
In conclusion, patients with IONM alerts had a greater magnitude of preoperative deformity, EBL, operation time, and number of levels fused compared to patients without signal alerts. In patients in whom the IONM alert cannot be recovered or reproduced by proceeding with deformity correction, surgeons can minimize the risk by aborting the initial procedure and completing the correction with staged operation. Staged operation resulted in a percentage of correction of 64.9%, and no permanent neurological deficit occurred in the 1 024 patients included in the series.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.