
Abstract
Study Design
Retrospective cohort study.
Objectives
To compare all-cause revision rates after lumbar fusion among asthmatic patients receiving maintenance inhaled corticosteroid (ICS) therapy, asthmatic patients without maintenance ICS, and asthma-free controls without ICS exposure.
Methods
Three cohorts of patients undergoing lumbar fusion were identified from a real-world health records database: (1) asthmatic patients with maintenance ICS therapy, (2) asthmatic patients without ICS therapy, and (3) asthma-free controls. Pairwise 1:1 propensity-score matching was performed to control for baseline differences in comorbidities, including known osteoporosis and systemic steroid exposure. All-cause revision rates were compared between cohorts at two- and five-years post-fusion using Chi-square tests and Kaplan-Meier analyses.
Results
Asthmatic patients on maintenance ICS were significantly more likely than asthmatic patients without ICS to undergo revision at 2 (P < 0.001, OR = 3.11, 95%CI = 2.25-4.31) and 5 (P < 0.001, OR = 3.16, 95%CI = 2.34-4.19) years following fusion. Asthmatic patients receiving maintenance ICS were also more likely than asthma-free controls to undergo revision at 2 (P < 0.001, OR = 3.48, 95%CI = 2.47-4.90) and 5 (P < 0.001, OR = 3.98, 95%CI = 2.92-5.42) years. Asthmatic patients without maintenance ICS had similar hazard of revision over 5 years of follow-up compared to asthma-free controls (P = 0.082, HR = 1.07; 95%CI = 0.99-1.15).
Conclusions
Maintenance ICS therapy is associated with increased risk of revision following lumbar fusion in asthmatic patients. ICS use, traditionally considered low-risk, may have clinically relevant effects on lumbar fusion outcomes. Future studies are warranted to further elucidate the biological mechanisms driving revision in these patients.
Keywords
Introduction
Lumbar spine fusion for degenerative spinal conditions such as dynamic spondylolisthesis with spinal stenosis is a commonly performed procedure globally. Certain modifiable prognostic factors have been identified for increased risk of complications following lumbar fusion, including number of levels fused, American Society of Anesthesiologists status, and poor bone quality.1–3
Inhaled corticosteroids (ICS) are a first-line intervention for managing asthma, with some patients with refractory disease requiring daily maintenance treatment with ICS. 4 However, long-term use of steroids is not without adverse effects. Chronic systemic steroid use has been shown to decrease bone mineral density (BMD) in patients with asthma, particularly at the spine and femur.5–7 Kebaish et al found that patients on long-term corticosteroid therapy who underwent posterior lumbar spine surgery had significantly higher risk for adverse events postoperatively, including infection, reoperation, and readmission 8 .
While systemic corticosteroid use is known to be associated with increased complication rates following lumbar fusion, the association between ICS use and outcomes of lumbar fusion has not been previously explored. Unlike systemic corticosteroids, ICS act locally in the lungs, reducing the need for high dosages and lowering the risk of systemic side effects. 9 Despite this, evidence exists of a dose-dependent effect of ICS use on decreased lumbar spine BMD. 5 These results suggest that maintenance ICS use may impact bone quality and subsequently fusion outcomes following lumbar surgery. This study aimed to elucidate the association between maintenance ICS use and all-cause revision rates following lumbar fusion surgery. Given the potentially adverse effects of prolonged ICS use on bone health, we hypothesized that asthmatic patients receiving maintenance ICS therapy would have elevated rates of revision compared to both asthmatic patients without maintenance ICS therapy and asthma-free controls.
Methods
Data Source
The data used in this retrospective cohort analysis was collected from the TriNetX Research Network, which provided curated access to electronic medical records (diagnoses, procedures, medications, laboratory values, and genomic information) from approximately 149 million patients from 108 healthcare organizations. The data reviewed is a secondary analysis of existing data, does not involve intervention or interaction with human subjects, and is de-identified, and thus exempt from Institutional Review Board approval.
Patient Selection
Patients undergoing primary lumbar fusion from March 2006 to March 2026 were identified using current procedural terminology (CPT) codes 22 533, 22 558, 22 612, 22 630, and 22 633. Patients undergoing fusion for indications of malignancy or infection were excluded. Remaining patients were stratified into 3 cohorts: (1) asthmatic patients receiving maintenance ICS therapy (“ICS Asthma” cohort), (2) asthmatic patients not receiving ICS therapy (“Non-ICS Asthma” cohort), and (3) asthma-free controls without ICS exposure in the 6 months prior to fusion (“Asthma-Free Controls” cohort). Maintenance ICS therapy was defined as filling 3 or more prescriptions of inhaled fluticasone, mometasone, budesonide, beclomethasone, or ciclesonide in the 6 months prior to fusion, reflecting regular use consistent with asthma management. Patients with chronic obstructive pulmonary disease (COPD) were excluded to isolate the impact of asthma-specific ICS use and to minimize confounding from COPD-related disease progression.
Statistical Analyses
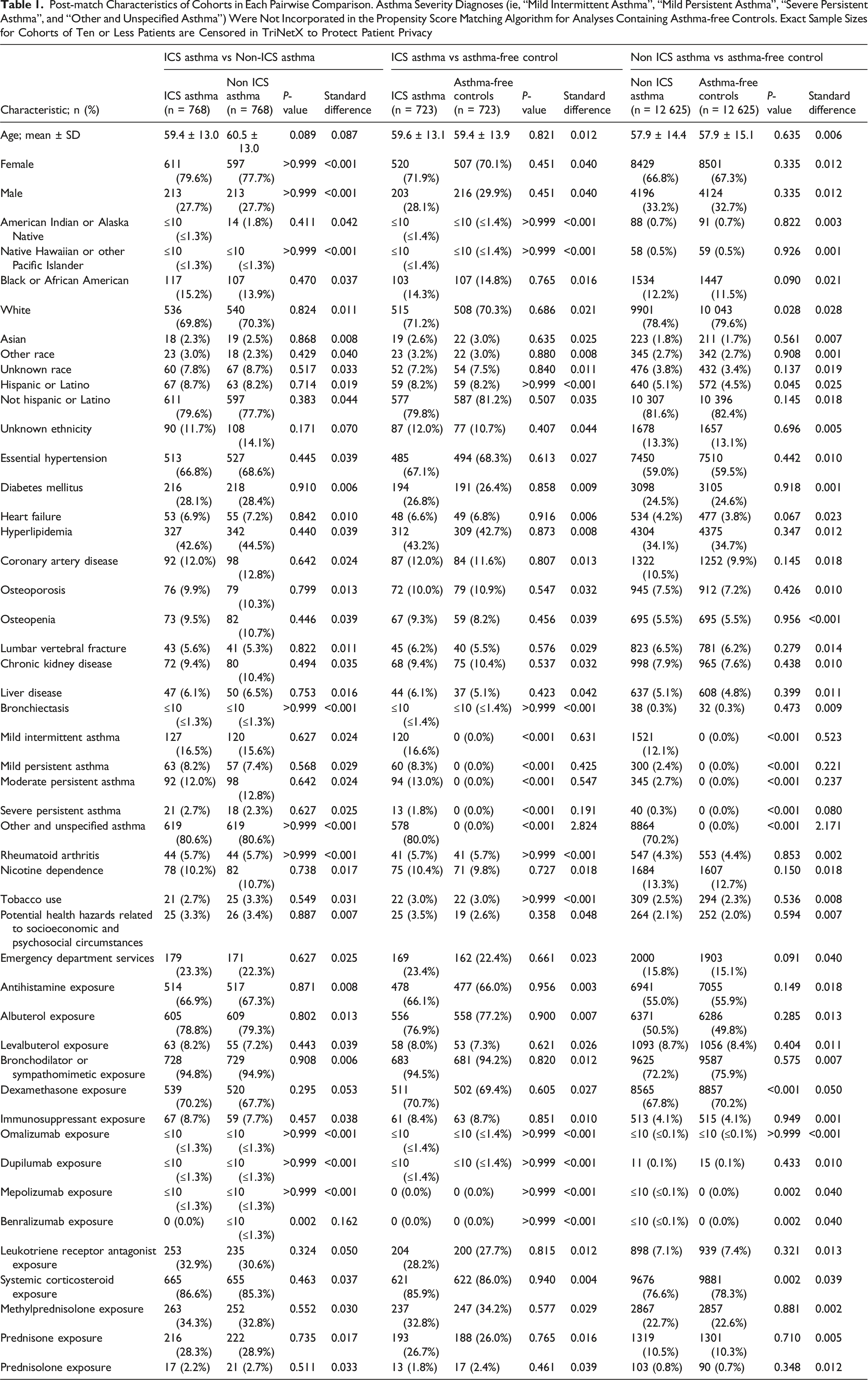
Post-match Characteristics of Cohorts in Each Pairwise Comparison. Asthma Severity Diagnoses (ie, “Mild Intermittent Asthma”, “Mild Persistent Asthma”, “Severe Persistent Asthma”, and “Other and Unspecified Asthma”) Were Not Incorporated in the Propensity Score Matching Algorithm for Analyses Containing Asthma-free Controls. Exact Sample Sizes for Cohorts of Ten or Less Patients are Censored in TriNetX to Protect Patient Privacy
The primary outcome of interest was the rate of all-cause revision following fusion. Revision was defined as either repeat lumbar fusion (CPT 22533, 22558, 22612, 22630, 22633), instrumentation removal (CPT 22850, 22852, 22855), or reinsertion of spinal instrumentation (CPT 22849). As TriNetX does not include operative level as a variable, revision encompassed both re-operations at the index level as well as procedures at adjacent levels. To explore potential indications for revision, secondary outcomes included rates of surgical site infection (SSI, inclusive of both deep and superficial SSI), pseudoarthrosis, and implant mechanical failure. Rates of each outcome were compared at two- and five-years following fusion using Chi-square tests, with results reported using odds ratios (OR) and absolute risk differences (ARD). Time to revision surgery was further evaluated using Kaplan–Meier survival analysis and compared between groups with the log-rank test. Cox proportional hazards models were used to estimate hazard ratios (HR) and 95% confidence intervals (CI) for up to 5 years following fusion. Statistical significance was set at P < 0.05 for all outcomes analyses. A full table of clinical codes and time windows used to create cohorts and conduct analyses can be found in Supplemental File 2.
Sensitivity Analyses
Sensitivity analyses were performed to better characterize the relationship between ICS exposure intensity and revision risk. Dose-equivalent information is not reliably captured in the TriNetX database. As such, ICS exposure intensity was approximated using prescription fill frequency as a proxy. Patients receiving ICS prescriptions in the 6 months prior to fusion were identified and stratified into the following cohorts based upon the number of prescriptions filled during this period: 1 ICS prescription, 2 prescriptions, 3 prescriptions, 4-5 prescriptions, or 6+ prescriptions. Pairwise 1:1 propensity score matching between cohorts was performed in a similar fashion to the main analysis. Revision rates were compared between fill-count strata at 2 and 5 years following fusion using chi-square tests.
A second sensitivity analysis was performed using an alternative ICS exposure definition to assess the robustness of our results to different ICS exposure windows. Maintenance ICS use was redefined as 6 or more prescription fills within the 12 months prior to lumbar fusion to re-approximate chronic use. Comparison cohorts were correspondingly redefined. Asthmatic patients with less than 6 prescription fills in the 12-months prior to fusion comprised the “Non ICS Asthma” cohort, and asthma-free patients with no ICS exposure served as the controls. 1:1 propensity score matching was again performed in a pairwise fashion, and revision rates were compared between cohorts at 2 and 5 years following fusion using chi-square tests.
Results
Asthmatic Patients Receiving Maintenance ICS vs Asthmatic Patients Without ICS
We initially identified 13 974 asthmatic patients who underwent lumbar fusion. Of this population, 5.6% of patients received maintenance ICS therapy. Pre-match characteristics of all cohorts in the primary analysis are available in Supplemental File 1. Following 1:1 propensity score matching, there were 768 patients in each cohort (Table 1). Cohorts were generally well matched, with all StD less than 0.10 other than for recent benralizumab exposure.
Complication Rates by Cohort

Bold indicates statistical significance at P < 0.05.
At 5 years after fusion, asthmatic patients receiving maintenance ICS remained more likely than asthmatic patients without maintenance ICS to undergo revision (P < 0.001, OR = 3.16, 95%CI = 2.34-4.19, ARD = 16.1%) and experience pseudoarthrosis (P = 0.013, OR = 1.43, 95%CI = 1.08-1.89, ARD = 4.6%). Asthmatic patients receiving maintenance ICS also were more likely to experience implant mechanical failure (P = 0.044, OR = 1.81, 95%CI = 1.01-3.26, ARD = 1.8%) at this time point. There was no significant association between maintenance ICS use and the rate of SSI (P = 0.110, OR = 1.38, 95%CI = 0.93-2.05, ARD = 2.1%). Kaplan-Meier analyses revealed that asthmatic patients receiving maintenance ICS had significantly higher hazard of revision over 5 years of follow-up (P < 0.001, HR = 2.69, 95%CI = 2.07-3.49; Figure 1). Kaplan-Meier curves demonstrating five year revision-free survival probability in asthmatic patients receiving maintenance ICS and asthmatic patients without maintenance ICS. Shaded areas represent 95% confidence intervals for survival probability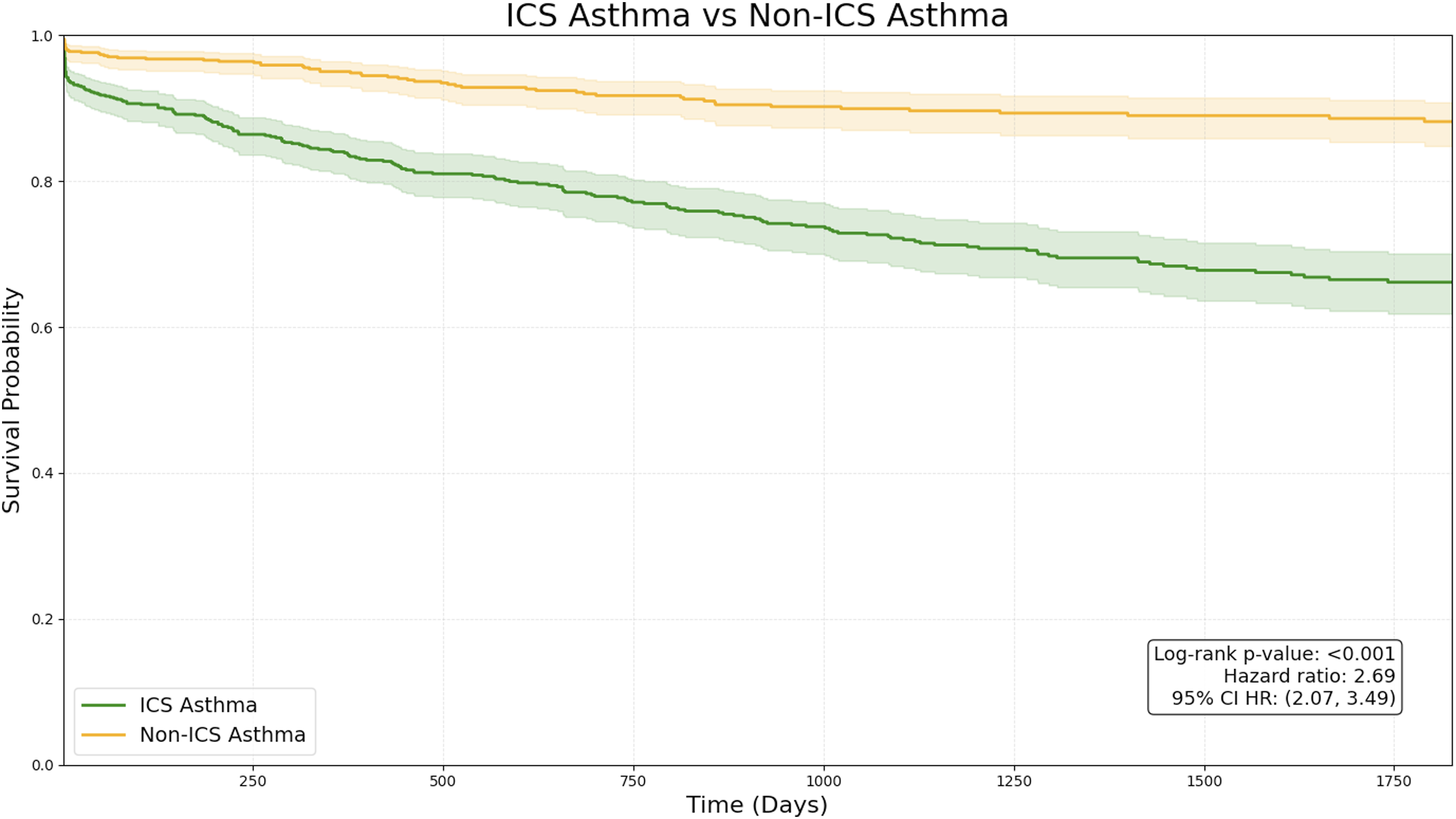
Asthmatic Patients Receiving Maintenance ICS vs Asthma-free Controls
A total of 95 789 asthma-free patients were identified who underwent lumbar fusion. Following propensity score matching, 723 patients remained in the ICS Asthma and Asthma-Free Control cohorts (Table 1). At 2 years following fusion, asthmatic patients receiving maintenance ICS were significantly more likely than asthma-free controls to undergo revision (P < 0.001, OR = 3.48, 95%CI = 2.47-4.90, ARD = 13.4%) and experience pseudoarthrosis (P < 0.001, OR = 1.99, 95%CI = 1.44-2.75, ARD = 7.3%). There were no significant differences in rates of SSI (P = 0.0501, OR = 1.54, 95%CI = 1.00-2.38, ARD = 2.5%) or mechanical failure (P = 0.117, OR = 1.65, 95%CI = 0.88-3.10, ARD = 1.4%).
At 5 years following fusion, asthmatic patients on maintenance ICS remained significantly more likely to undergo revision (P < 0.001, OR = 3.98, 95%CI = 2.92-5.42, ARD = 18.4%) than asthma-free controls. Asthmatic patients on maintenance ICS were similarly more likely to experience SSI (P = 0.019, OR = 1.63, 95%CI = 1.08-2.46, ARD = 3.2%), pseudoarthrosis (P < 0.001, OR = 2.04, 95%CI = 1.50-2.77, ARD = 8.4%), and implant mechanical failure (P = 0.033, OR = 1.87, 95%CI = 1.05-3.36, ARD = 2.1%) than controls. Asthmatic patients on maintenance ICS had significantly higher hazard of revision when compared to controls over 5 years follow-up (P < 0.001, HR = 3.21; 95%CI = 2.41-4.28) Figure 2. Kaplan-Meier curves demonstrating five year revision-free survival probability in asthmatic patients receiving maintenance ICS and asthma-free controls. Shaded areas represent 95% confidence intervals for survival probability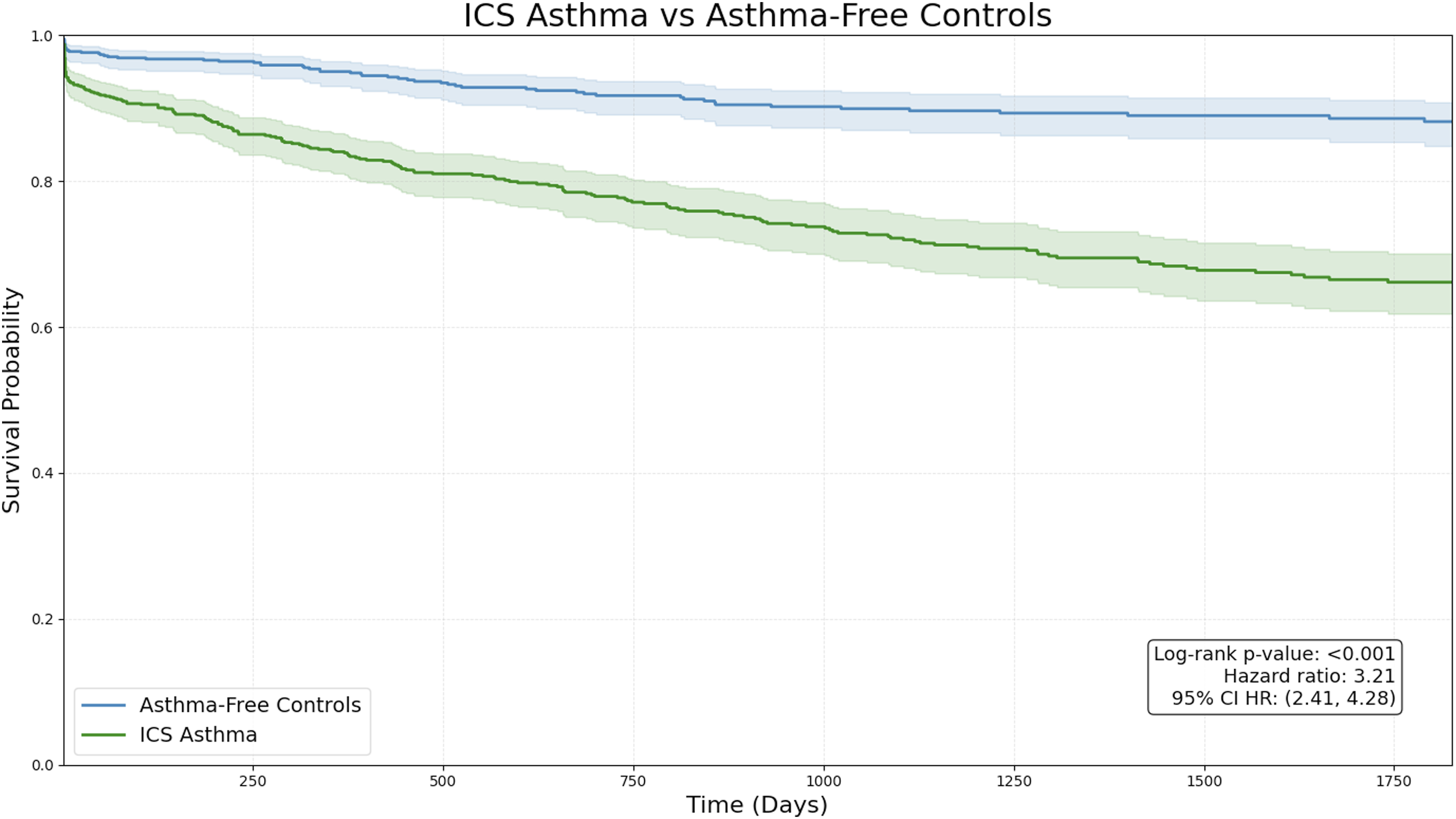
Asthmatic Patients Without Maintenance ICS vs Asthma-free Controls
Following propensity-score matching, there were 12 625 patients in each cohort (Table 1). At 2 years following fusion, there were no significant differences in the rate of revision (P = 0.279, OR = 1.05, 95%CI = 0.96-1.15, ARD = 0.4%), SSI (P = 0.110, OR = 1.10, 95%CI = 0.98-1.24, ARD = 0.4%), or implant mechanical failure (P = 0.664, OR = 1.04, 95%CI = 0.88-1.23, ARD = 0.1%) between asthmatic patients without maintenance ICS and asthma-free controls. However, asthmatic patients without maintenance ICS were significantly more likely than controls to experience pseudoarthrosis (P = 0.002, OR = 1.12, 95%CI = 1.04-1.21, ARD = 1.3%).
At 5 years, asthmatic patients without maintenance ICS were more likely than asthma-free controls to experience revision (P = 0.006, OR = 1.12, 95%CI = 1.03-1.21, ARD = 1.1%), SSI (P = 0.027, OR = 1.14, 95%CI = 1.02-1.27, ARD = 0.6%), and pseudoarthrosis (P < 0.001, OR = 1.15, 95%CI = 1.07-1.24, ARD = 1.8%). There was no significant difference in rates of mechanical failure (P = 0.767, OR = 1.02, 95%CI = 0.88-1.18, ARD = 0.1%). Asthma-free controls had similar hazard of revision compared to asthmatic patients without maintenance ICS over 5 years of follow-up (P = 0.082, HR = 1.07; 95%CI = 0.99-1.15) Figure 3. Kaplan-Meier curves demonstrating five year revision-free survival probability in asthmatic patients without maintenance ICS and asthma-free controls. Shaded areas represent 95% confidence intervals for survival probability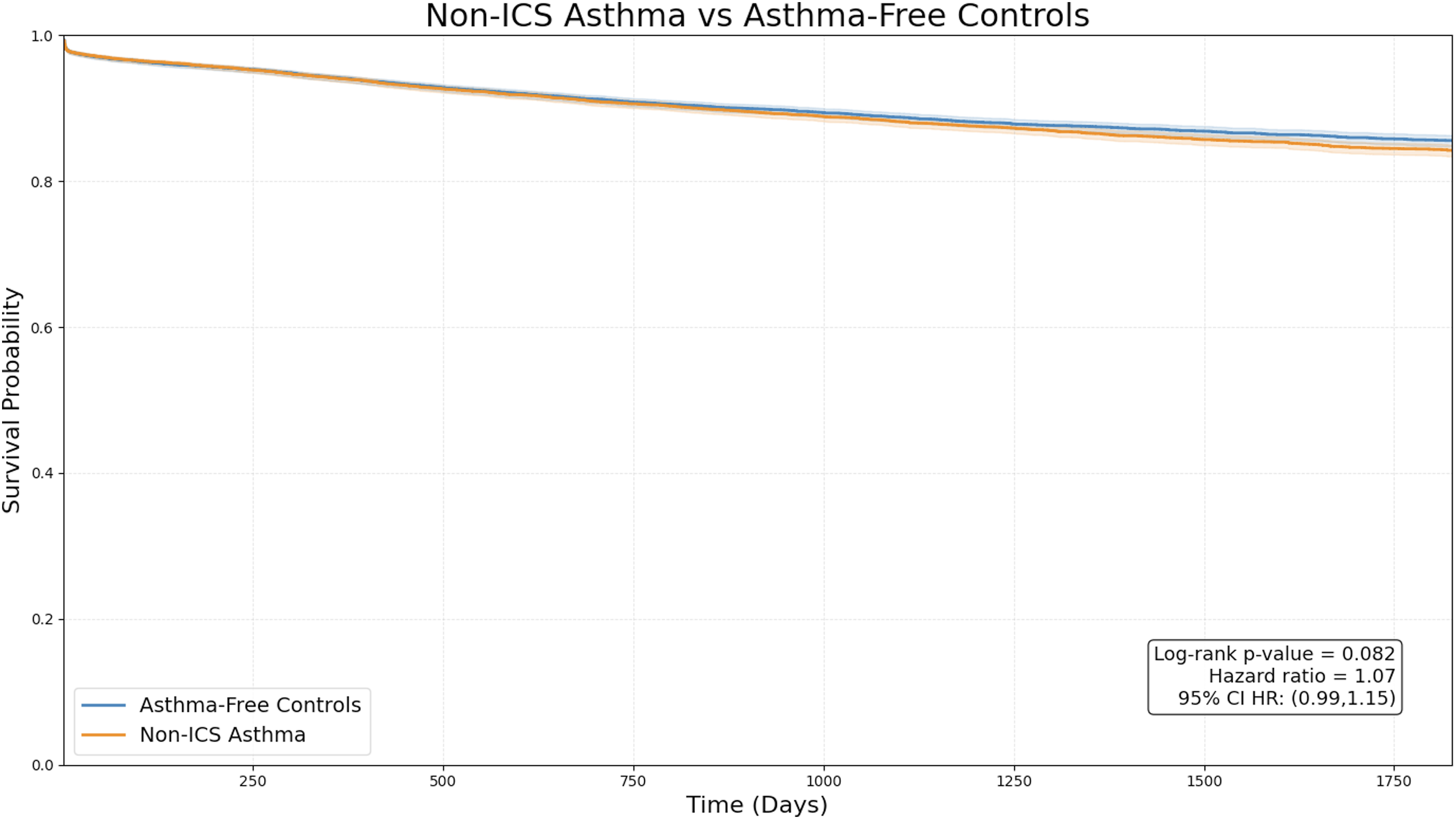
Fill Count Strata Sensitivity Analyses
Revision Rates by Fill-Count Strata Cohort
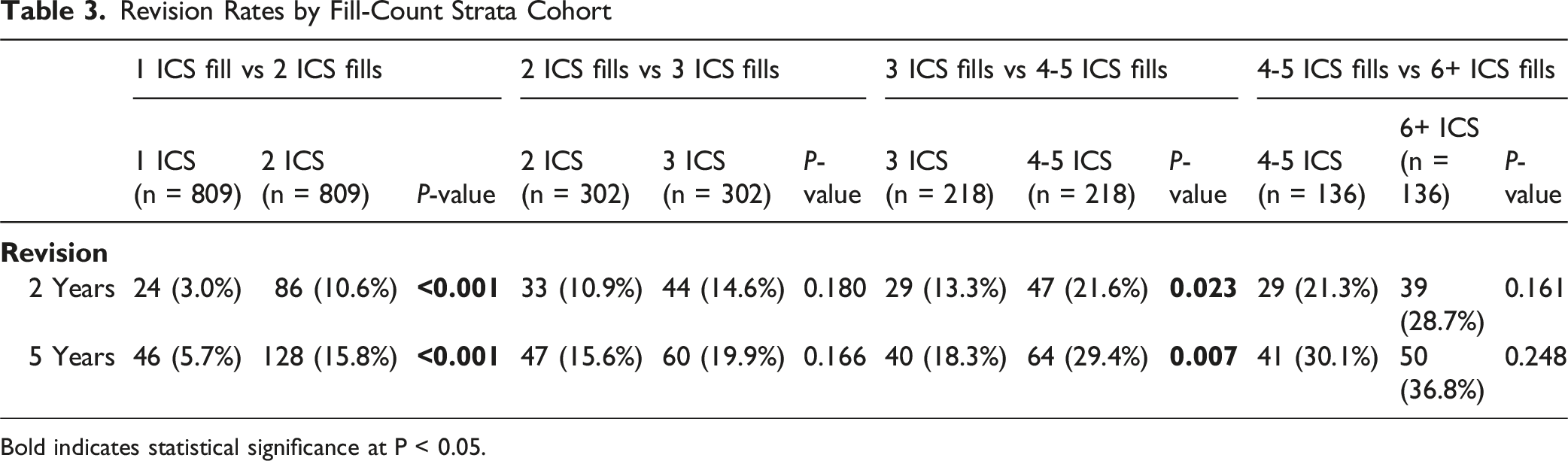
Bold indicates statistical significance at P < 0.05.
Alternative Exposure Window Sensitivity Analysis
Revision Rates by Cohort in Sensitivity Analysis Redefining Maintenance ICS Use as Six or More ICS Fills Within the 12 months Prior to Fusion
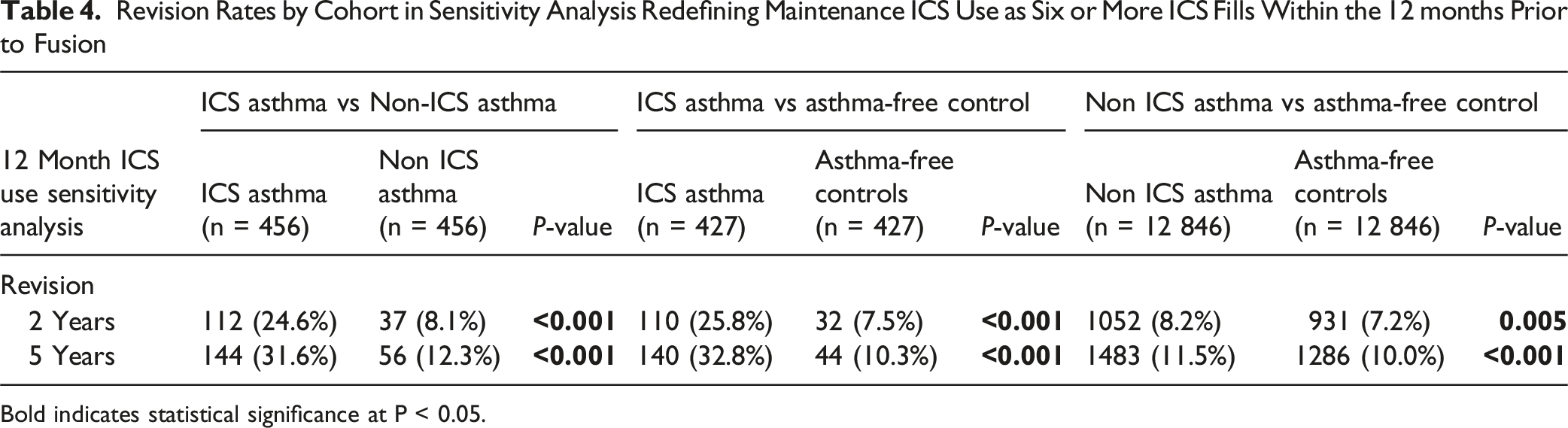
Bold indicates statistical significance at P < 0.05.
Discussion
Although the adverse effects of systemic corticosteroid use on outcomes of lumbar fusion have been well reported, the effects of long-term inhaled steroid use are not well characterized. In this retrospective matched cohort study of lumbar fusion patients with up to 5-year follow-up, asthmatic patients receiving maintenance ICS therapy had a higher risk of all-cause revision compared to both asthmatic patients not on ICS and asthma-free controls. These findings may hold important implications for the perioperative management of asthmatic patients undergoing lumbar fusion.
Our findings were consistent when evaluated using an alternative ICS exposure window. In addition, the fill-count sensitivity analysis demonstrated a pattern of higher revision risk with increasing prescription frequency, suggesting a possible dose-dependent relationship. The consistent findings across sensitivity analyses suggest that the observed association between maintenance ICS use and elevated revision rates following lumbar fusion is not dependent on a single exposure definition. Because this study was observational and retrospective in nature, we were unable to establish causality or determine the mechanisms underlying the observed relationships. However, we hypothesize that maintenance ICS use may increase revision risk through an osteoporosis-mediated mechanism similar to that caused by systemic corticosteroid use. 6 While ICS are primarily localized to the lungs, previous studies have shown that ICS use decreases serum osteocalcin levels, a marker of systemic bone formation, in a manner consistent with steroid induced bone loss.10–12 Moreover, several studies have reported significant associations between long-term ICS use in asthmatic patients and lower BMD.13–16 Future research incorporating direct assessments of bone health, including BMD, is needed to definitively clarify the mechanisms driving the observed associations. Nonetheless, our results demonstrate that even ICS use, traditionally considered lower risk than oral steroid use, may have clinically relevant effects on fusion integrity.
Importantly, asthmatic patients not receiving maintenance ICS therapy had similar revision rates to asthma-free controls at both two- and five-years post-fusion. Although a statistically significant increase in revision was observed at 5-year follow-up, the magnitude of this difference was small relative to that seen in other pairwise comparisons. Consistent with this, Cox proportional hazards modeling demonstrated no meaningful difference in 5-year revision risk between these groups. The association between asthma itself and outcomes following lumbar fusion has not been extensively explored in the literature. While one study identified asthma as a risk factor for increased postoperative pain following lumbar fusion, asthma has not been previously linked to increased revision rates after lumbar fusion. 17 Our results, demonstrating only a minor association between asthma and revision rates, suggest that the observed differences in revision rates between asthmatic patients receiving maintenance ICS therapy and asthma-free controls are likely more attributable to ICS use rather than asthma itself.
Our secondary analysis of complication rates may offer additional insight into the potential mechanisms underlying the observed association between ICS use and revision risk. In the first 5 years following fusion, asthmatic patients receiving maintenance ICS were significantly more likely than both asthmatic patients without maintenance ICS and asthma-free controls to experience implant mechanical failure and pseudoarthrosis. These complications reflect a pattern consistent with suboptimal fusion integrity secondary to poor bone quality.18,19 In contrast, SSI rates were similar between ICS-treated and non-ICS-treated asthmatic patients, suggesting that infection is less likely to explain the observed differences in revision rates. These findings support a plausible role for compromised bone quality in mediating the association between ICS exposure and revision. However, because revision indications cannot be directly determined within the TriNetX database, these mechanistic conclusions should be interpreted as indirect and preliminary.
The findings of this retrospective cohort study should be taken as hypothesis-generating rather than practice-changing until validated in datasets with more granular information, including BMD. Nonetheless, surgeons may consider incorporating routine Dual-Energy X-ray Absorptiometry (DEXA) scans into the preoperative work-up of asthmatic patients receiving maintenance ICS. In line with Enhanced Recovery After Surgery (ERAS) principles, such preoperative risk stratification and optimization of modifiable factors, including bone health, represent key components of perioperative care in spine surgery. 20 Osteoporosis is already under screened in individuals over the age of 50 undergoing lumbar fusion. 21 Diagnosing and medically managing osteoporosis in asthmatic patients receiving ICS, who may be at higher risk for osteoporosis, may help to mitigate risk of revision following surgery. 22
This study had several limitations. Firstly, our use of a research database prevented us from assessing functional outcomes and patient-reported outcome measures, as these measures are not recorded. Further, we were also unable to directly attribute revision procedures to specific indications and instead relied on a separate analysis of complication rates to infer potential mechanisms. Despite these drawbacks, the large sample size and the real-world nature of the data strengthen the robustness of our findings. Although we performed propensity score matching between cohorts, it is also possible that uncaptured variables may confound our results. For example, we matched for asthma severity diagnoses and exposure to systemic corticosteroids in the 6 months prior to fusion. However, we were unable to balance for the dosing of steroids and for how long patients received them. As asthmatic patients receiving maintenance ICS are likely sicker and may require more frequent systemic steroids for disease flare-ups, it is possible that greater systemic steroid burden contributed to the differences observed in our study. We were similarly unable to fully balance for rehabilitation compliance, socioeconomic status, or smoking intensity. Surgical complexity variables such as the number of fused levels, the use of interbody cages, the use of biologic adjuvants (eg, bone morphogenetic protein), and osteotomy procedures are not reliably captured in the TriNetX database and therefore could also not be controlled for. These may have confounded the observed relationships in this study. Sample size limitations further prevented us stratifying our cohorts by surgical approach (eg, anterior vs posterior fusion). Finally, the retrospective nature of this study prevented us from assigning causation to any observed relationships.
Conclusion
Maintenance inhaled corticosteroid therapy in asthmatic patients is associated with increased risk of revision after lumbar fusion. ICS use, traditionally considered lower risk than oral steroid use, may therefore have clinically relevant effects on fusion integrity. Future research is warranted to understand the drivers of revision in asthmatic patients receiving ICS and whether management of asthma with non-steroidal medications can reduce revision risk while still appropriately controlling asthma.
Supplemental Material
Supplemental material - Maintenance Inhaled Corticosteroid Use is Associated With Increased Revision Risk in Asthmatic Patients Undergoing Lumbar Fusion
Supplemental material for Maintenance Inhaled Corticosteroid Use is Associated With Increased Revision Risk in Asthmatic Patients Undergoing Lumbar Fusion by Eric Mao, BA, Sydney Thai, BS, Krystell E. Ceballos-Alvarez, BS, Andreas K. Demetriades, FRCSEd, Sarvdeep Dhatt, MD, Bhavuk Garg, MD, Gianluca Vadala, MD, PhD, Amit Jain, MD, MBA, AO Spine Knowledge Forum Degenerative in Global Spine Journal
Supplemental Material
Supplemental material - Maintenance Inhaled Corticosteroid Use is Associated With Increased Revision Risk in Asthmatic Patients Undergoing Lumbar Fusion
Supplemental material for Maintenance Inhaled Corticosteroid Use is Associated With Increased Revision Risk in Asthmatic Patients Undergoing Lumbar Fusion by Eric Mao, BA, Sydney Thai, BS, Krystell E. Ceballos-Alvarez, BS, Andreas K. Demetriades, FRCSEd, Sarvdeep Dhatt, MD, Bhavuk Garg, MD, Gianluca Vadala, MD, PhD, Amit Jain, MD, MBA, AO Spine Knowledge Forum Degenerative in Global Spine Journal
Supplemental Material
Supplemental material - Maintenance Inhaled Corticosteroid Use is Associated With Increased Revision Risk in Asthmatic Patients Undergoing Lumbar Fusion
Supplemental material for Maintenance Inhaled Corticosteroid Use is Associated With Increased Revision Risk in Asthmatic Patients Undergoing Lumbar Fusion by Eric Mao, BA, Sydney Thai, BS, Krystell E. Ceballos-Alvarez, BS, Andreas K. Demetriades, FRCSEd, Sarvdeep Dhatt, MD, Bhavuk Garg, MD, Gianluca Vadala, MD, PhD, Amit Jain, MD, MBA, AO Spine Knowledge Forum Degenerative in Global Spine Journal
Supplemental Material
Supplemental material - Maintenance Inhaled Corticosteroid Use is Associated With Increased Revision Risk in Asthmatic Patients Undergoing Lumbar Fusion
Supplemental material for Maintenance Inhaled Corticosteroid Use is Associated With Increased Revision Risk in Asthmatic Patients Undergoing Lumbar Fusion by Eric Mao, BA, Sydney Thai, BS, Krystell E. Ceballos-Alvarez, BS, Andreas K. Demetriades, FRCSEd, Sarvdeep Dhatt, MD, Bhavuk Garg, MD, Gianluca Vadala, MD, PhD, Amit Jain, MD, MBA, AO Spine Knowledge Forum Degenerative in Global Spine Journal
Footnotes
Ethical Considerations
The data reviewed is a secondary analysis of existing data, does not involve intervention or interaction with human subjects, and is de-identified, and thus exempt from Institutional Review Board approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.