
Abstract
Study design
Observational extended follow-up of a randomized controlled trial.
Objective
To compare mid-to long-term clinical and radiographic outcomes of allograft vs bioactive glass-ceramic (BG) cages for anterior cervical discectomy and fusion (ACDF) while preserving the original random allocation.
Methods
All patients randomized in the parent RCT underwent 1-2 level ACDF between August 2017–August 2022 (allograft n = 18; BG n = 22) were followed through August 2025. We compared patient-reported outcomes—neck disability index (NDI) and visual analogue scale (VAS)—cervical sagittal alignment, including C2-7 lordosis (CL), T1 slope, and T1 slope minus cervical lordosis (T1sCA), and CT–based subsidence using adjusted linear mixed-effects models (LMMs); fusion (Bridwell I–II) was compared between groups.
Results
Among 40 patients, 90% had follow-up longer than 24 months with mean follow-up 53.5 ± 25.2 months. Both groups showed significant within-group improvements in all patient reported outcomes. However, at the last visit, between-group differences were non-significant for the primary endpoints: NDI (BG–allograft −0.98, 95% CI −9.17 to 7.21; P = .814) and C2-7 lordosis (BG–allograft −0.19°; P = .917). Other endpoints (VAS, T1sCA, subsidence, fusion) were likewise similar. No cage breakage or migration occurred; adverse events were minor.
Conclusion
Over multi-year follow-up, bioactive glass-ceramic cages provided equivalent clinical improvement and radiographic stability to allograft cages after ACDF.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is widely used to treat cervical radiculopathy and myelopathy.1-3 Durable symptom relief and postoperative stability are both largely dependent on the material and design of interbody spacer or cage. 4 The cage’s mechanical profile—geometry, footprint, and elastic modulus—influences the magnitude of alignment correction and the distribution of endplate contact stresses, and its material properties—especially surface bioactivity and osteointegration potential—affect the likelihood of achieving solid fusion and the risks of implant-related complications, such as subsidence or migration.5,6 Because nonunion and implant-related complications are linked to poorer patient outcomes, need for re-operation, and higher medical cost, careful development and judicious selection of cage materials are critical to the durability of ACDF.7-9
Historically, iliac crest autograft has been regarded as the reference graft for cervical interbody fusion, but its advantages are offset by donor-site morbidity and longer operative time.10-12 Alternative options—including allograft, titanium, and polyetheretherketone (PEEK) cages—were developed to mitigate these drawbacks, yet each carries trade-offs. Titanium offers high strength and biocompatibility but, at the same time, is associated with subsidence. PEEK, while closer to bone in stiffness and less prone to subsidence, lacks intrinsic osteointegration and often requires supplemental bone grafting. Lastly, allograft may introduce concerns about immune reaction or disease transmission and variability in graft quality.11,13-16 To date, no single interbody spacer/cage has demonstrated unequivocal superiority across indications or settings; consequently, device utilization varies by era and region, and ongoing research and investment continue to explore new designs and optimize material selection.
Recent advances in biomaterials have led to bioactive glass-ceramic (BG) cages, such as CaO–SiO2–P2O5–B2O3–based devices, which combine mechanical robustness with surface bioactivity that promotes chemical bonding to bone and osteointegration.17-19 Early reports in lumbar and cervical fusion suggest clinical and radiographic outcomes broadly comparable to PEEK, titanium, or allograft—i.e, non-inferior performance within the observed follow-up windows.18,20-27 In our prior randomized controlled trial, BG and allograft demonstrated no significant differences in pain or spinal alignment at 12 months. 28 However, most published randomized controlled trials of BG cages—including our own—have been limited to approximately 1 year of follow-up, leaving long-term effectiveness and safety insufficiently characterized.20,24
Accordingly, we conducted an observational extended follow-up of the previous RCT cohort to evaluate mid-to long-term outcomes while preserving the original random treatment allocation. By preserving randomization and having longer follow-up, this study would offer a rare, internally valid view of how BG cages perform against allograft cages in ACDF.
Methods
Study Design and Ethics
We conducted an observational, single-center extended follow-up of the cohort originally randomized in a prospective RCT comparing allograft vs bioactive glass-ceramic cages for one- or two-level ACDF. Participants were enrolled in the parent trial between August 2017 and August 2022, and extended follow-up continued through August 2025. Long-term data were obtained from scheduled outpatient visits, structured chart review, and telephone contact. The study was approved by the Institutional Review Board (IRB No. KC25RISI0718), conducted in accordance with the Declaration of Helsinki and Good Clinical Practice; all participants provided written informed consent in the parent RCT.
Participants and Cohorts
All 40 randomized patients from the parent trial (allograft n = 18, BG n = 22) were eligible for this follow-up, preserving original treatment allocation. Parent-trial eligibility included adults (18-75 years) with cervical radiculopathy or myelopathy due to subaxial degenerative disc disease (soft disc herniation or spondylosis) confirmed by MRI/CT, after ≥ 3-6 months of unsuccessful conservative treatment. Key exclusions were prior surgery at the index level or posterior cervical surgery, severe osteoporosis (T-score < −3.5), indications exceeding two operated levels, active infection, deformity, fracture, malignancy, and known hypersensitivity to implant materials. Detailed inclusion/exclusion criteria and peri-operative protocols are described in the parent RCT publication. 28
Randomization
In the parent RCT, allocation to allograft (Cornerstone-SR™, Medtronic) or BG cage (Novomax, CGBio Inc.) was based on a computer-generated random sequence with sequentially numbered, sealed, opaque envelopes managed by a research coordinator independent of clinical care and outcome assessment. Group assignment was disclosed to the operating surgeon on the day before surgery. While complete blinding was not feasible due to cage appearance on imaging, outcome assessors and data analysts were independent of peri-operative care, minimizing assessment bias.
Surgical Procedure
All procedures were performed by a single experienced spine neurosurgeon using a standard Smith–Robinson anterior approach under general anesthesia with intraoperative neuromonitoring. After thorough discectomy and decompression, the assigned interbody device (allograft or BG cage) was implanted and secured with an anterior cervical plate and screws. Postoperative management followed a uniform protocol, including short-term cervical collar immobilization. Peri-operative techniques and care otherwise adhered to the parent protocol.
Outcomes and Assessments
Data on demographics and clinical context—age, sex, body mass index, American Society of Anesthesiologists (ASA) class, number of operated levels, smoking and alcohol history, and comorbid conditions—were abstracted from the medical record and summarized in the baseline table. Follow-up was organized prospectively: clinical visits at baseline, 1, 3, 6, 12, and 24 months and a last available visit; lateral radiographs at baseline, 1, 6, 12, and 24 months and last. The last follow-up timepoint was defined a priori as the latest available visit >24 months after the index surgery; when multiple visits were available beyond 24 months, the farthest visit was used.
The predefined primary outcome was the inter-group difference in Neck Disability Index (NDI) at the final follow-up. Secondary outcomes included other PROMs and radiographic parameters assessed at each follow-up time point. PROMs comprised the NDI and visual analogue scale (VAS) scores for neck and arm pain at scheduled clinical visits. At the last visit, satisfaction and subjective recovery rate were recorded as percentages, and recommendation was recorded as a binary response. Safety surveillance captured complications, reoperations, and additional cervical procedures over follow-up.
Radiographic evaluation targeted cervical sagittal alignment—C2-7 lordosis (cervical lordosis), T1 slope, and T1 slope minus cervical lordosis (T1sCA; T1 slope − C2-7 lordosis; also referred to as the cervical sagittal angle)—on standing lateral images, as well as segment-level metrics, including interspinous motion (ISM) on dynamic flexion–extension views and cage subsidence on CT scans. 29 The T1sCA reflects cervical sagittal balance by quantifying the additional angle, after accounting for the T1 slope, required for the cervical spine to achieve horizontal alignment; values ≤20° indicate balance, whereas values >20° indicate imbalance. 30 We parameterized inter-group contrasts such that positive estimates indicate higher values with bioactive glass-ceramic (BG) relative to allograft (BG–allograft). Between-group differences in improvement were defined as the difference in change from baseline between groups, ie, (ΔBG – Δallograft) at each time point. ISM was assessed at 6, 12, and 24 months and at last dynamic radiograph, and subsidence at 6 and 12 months and at last CT scan. 31 Fusion was graded using the Bridwell interbody fusion system (grades 1-2 treated as fused) by two reviewers independent of direct clinical care. 25 Per protocol, outcomes were analyzed through the last available visit; for patient-reported outcomes and cervical sagittal alignment, follow-up was censored at the last visit before any additional cervical surgery.
Statistical Analysis
Baseline characteristics were summarized as mean ± SD for continuous variables and as counts with percentages for categorical variables. Normality and homoscedasticity were checked with the Shapiro–Wilk and Levene tests. Between-group comparisons used Student or Welch t tests; when assumptions were not met, the Mann–Whitney U test was applied. Categorical variables were compared with the χ2 test or Fisher’s exact test as appropriate.
For longitudinal outcomes—including neck disability index (NDI), visual analogue scale (VAS) for neck and arm pain, C2-7 lordosis, T1 slope, T1sCA, and the segment-level measures of subsidence and interspinous motion—linear mixed models were applied as the primary approach. Fixed effects were group, time (modeled as a categorical factor), and their interaction. Models adjusted for the outcome’s baseline value and the prespecified covariates age, sex, BMI, ASA status, and the number of operated levels. A patient-level random intercept was included; a random slope for time was attempted and retained only when numerically stable. For outcomes analyzed with linear mixed models, results are reported as model-adjusted estimated marginal means (EMMs) with 95% confidence intervals at each time point by group; EMMs are the predicted means from the adjusted model and therefore differ from raw means. We also report between-group contrasts (BG–allograft differences in EMMs) with 95% CIs and two-sided P values, and within-group changes from baseline as model coefficients with P values. Primary analyses used linear mixed models and an available-case approach, whereby all randomized participants contributed their observed repeated measurements; missing data were addressed under the mixed-model missing-at-random (MAR) assumption without single-value imputation. Models were fitted by restricted maximum likelihood, and missing observations were handled under the missing-at-random assumption inherent to mixed models, which accommodates unbalanced follow-up. As sensitivity analyses, we repeated the models using generalized estimating equations and performed an intention-to-treat–oriented baseline-observation-carried-forward analysis for PROMs to assess robustness. At the last visit, patient satisfaction, recovery rate and recommendation were compared between groups. All analyses were conducted in Python using pandas, NumPy, SciPy, and statsmodels (MixedLM and GEE) with patsy. Package versions and reproducible scripts are available upon request. Two-sided P values are reported with a significance level of 0.05, without multiplicity adjustment.
Results
Baseline Characteristics
Baseline Characteristics of Allograft Group and Bioactive Glass-Ceramic cage
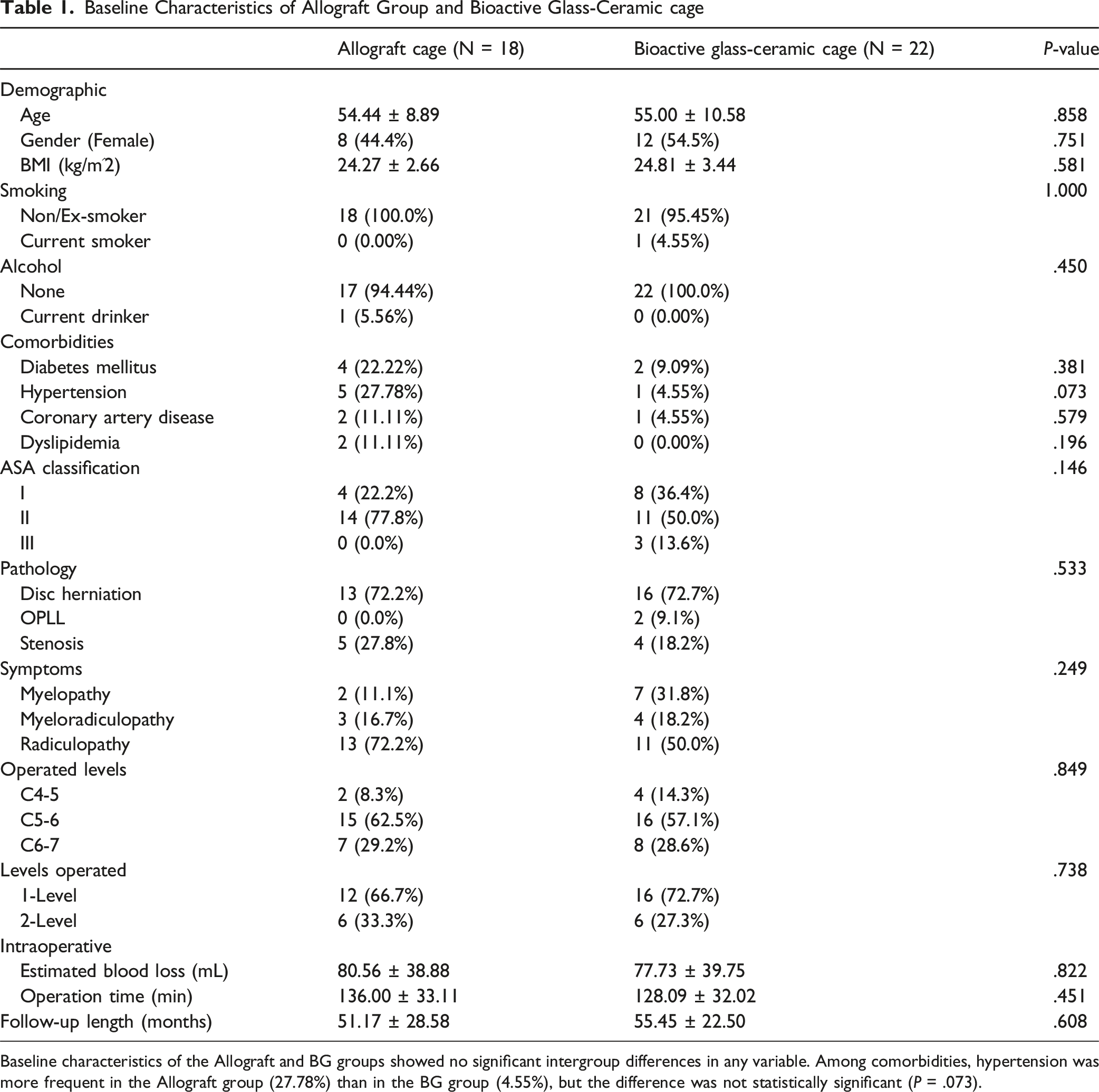
Baseline characteristics of the Allograft and BG groups showed no significant intergroup differences in any variable. Among comorbidities, hypertension was more frequent in the Allograft group (27.78%) than in the BG group (4.55%), but the difference was not statistically significant (P = .073).
A total of three patients (BG n = 2, allograft n = 1) underwent additional cervical surgery and therefore contributed outcomes only up to the visit immediately preceding surgery, not through the last follow-up. Including two of these who had surgery after the 6-month and 12-month visits, respectively, four patients in total (BG n = 1, allograft n = 3) were not available beyond 24 months; thus, 36/40 (90%) contributed outcomes at ≥24 months. The mean follow-up was 53.5 ± 25.16 months (excluding the four early discontinuations: 58.6 ± 20.88 months). Two-level ACDF was permitted per the parent RCT; in this cohort, 12 patients underwent two-level surgery (BG, n = 6; allograft, n = 6), and the remainder were single-level.
Patient-Reported Outcomes (PROMs)
Patient-Reported Outcome With Intra- and Inter-group Analysis of Allograft and Bioactive Glass-Ceramic Cage Groups
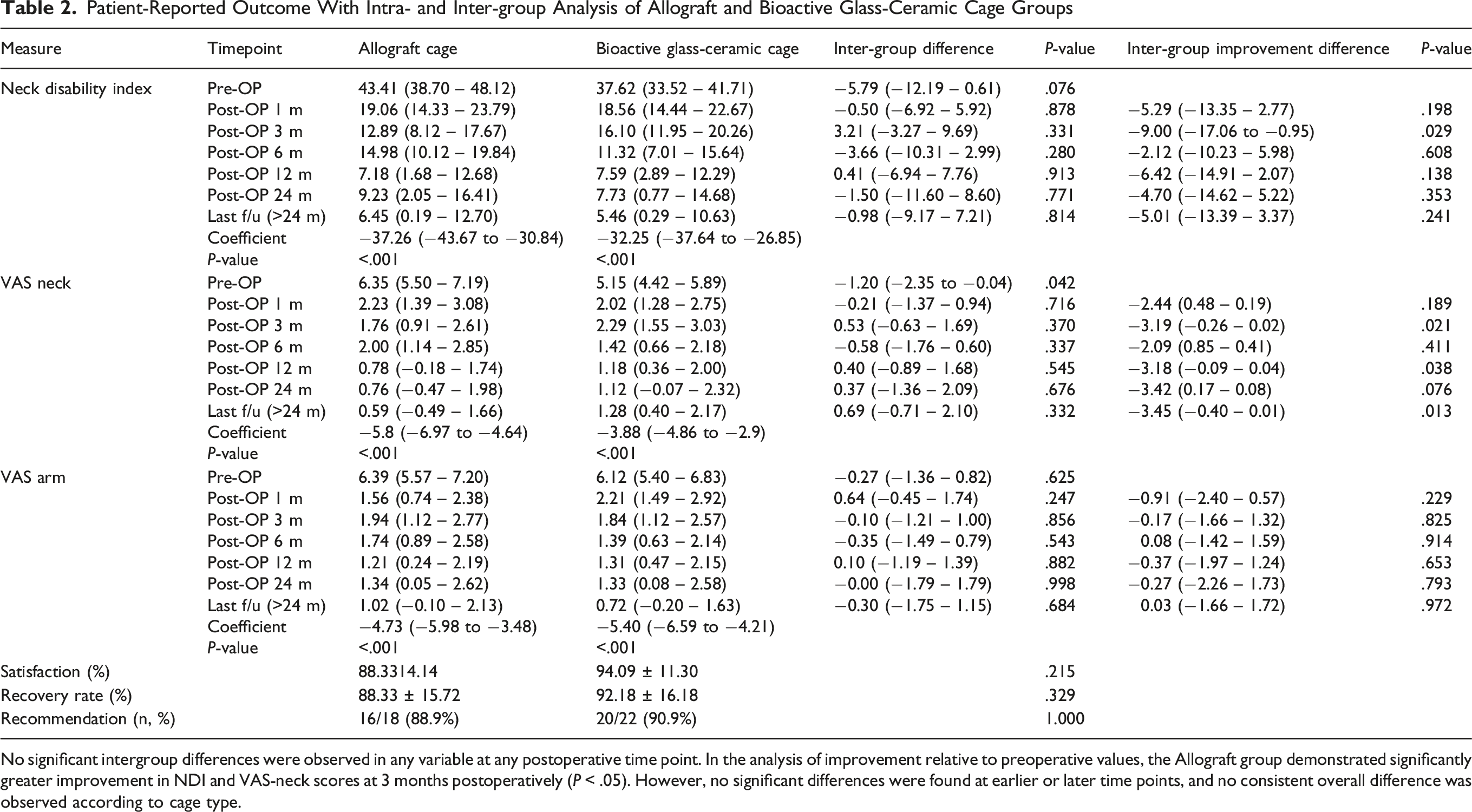
No significant intergroup differences were observed in any variable at any postoperative time point. In the analysis of improvement relative to preoperative values, the Allograft group demonstrated significantly greater improvement in NDI and VAS-neck scores at 3 months postoperatively (P < .05). However, no significant differences were found at earlier or later time points, and no consistent overall difference was observed according to cage type.
Radiologic Cervical Alignment Metrics With Intra- and Inter-group Analysis of Allograft and Bioactive Glass-Ceramic Cage Groups
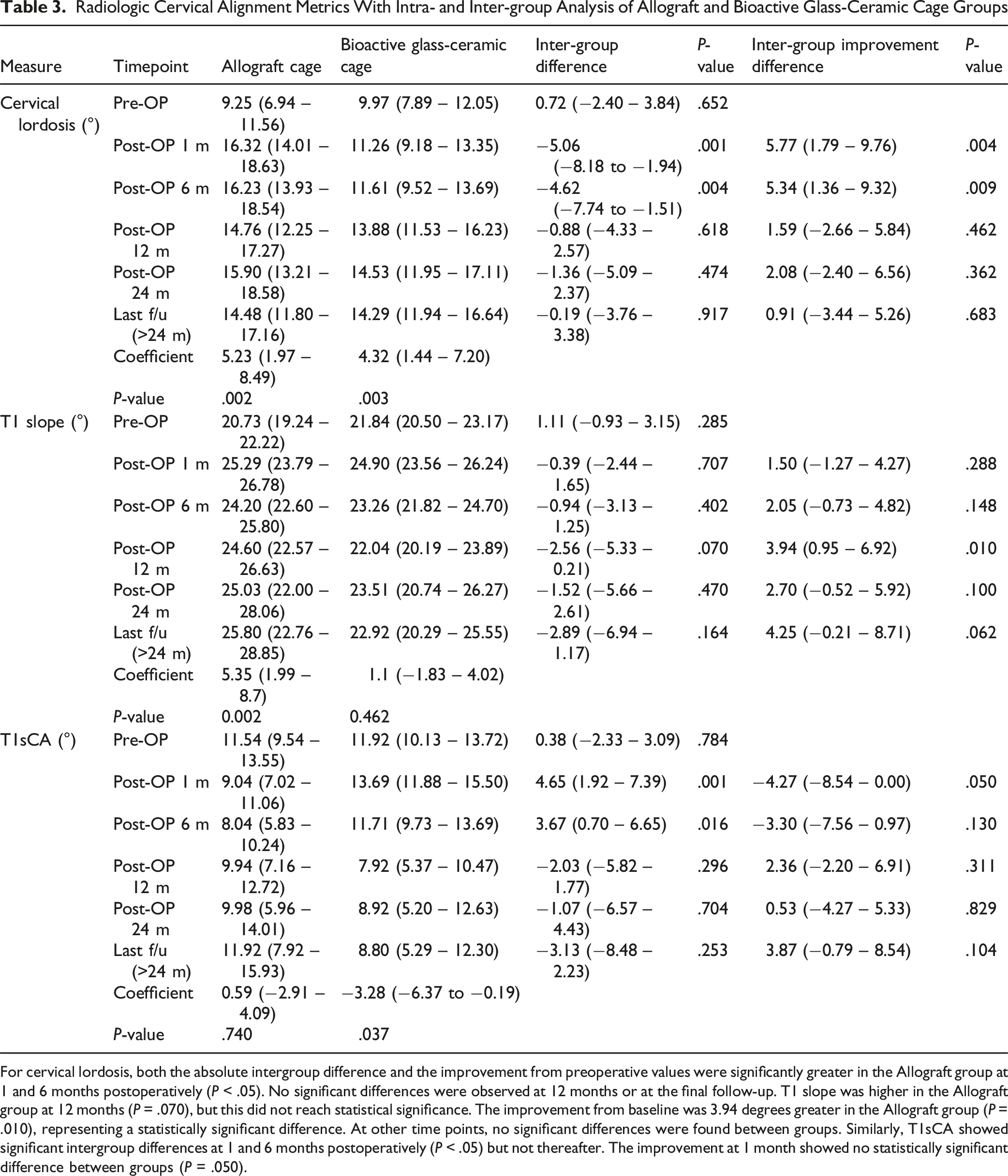
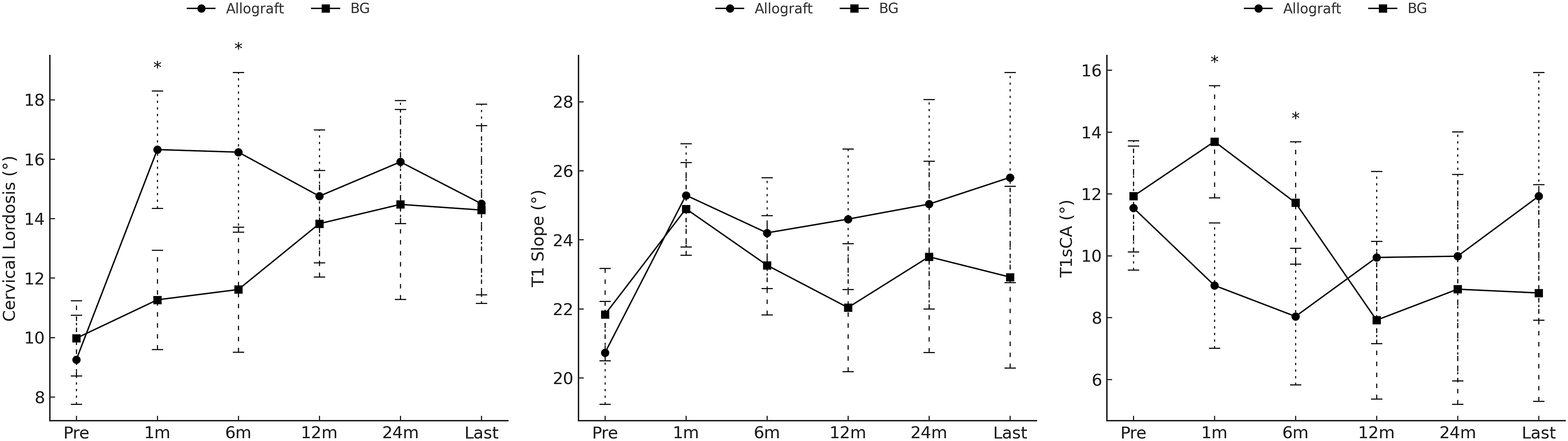
For cervical lordosis, both the absolute intergroup difference and the improvement from preoperative values were significantly greater in the Allograft group at 1 and 6 months postoperatively (P < .05). No significant differences were observed at 12 months or at the final follow-up. T1 slope was higher in the Allograft group at 12 months (P = .070), but this did not reach statistical significance. The improvement from baseline was 3.94 degrees greater in the Allograft group (P = .010), representing a statistically significant difference. At other time points, no significant differences were found between groups. Similarly, T1sCA showed significant intergroup differences at 1 and 6 months postoperatively (P < .05) but not thereafter. The improvement at 1 month showed no statistically significant difference between groups (P = .050).
Subsidence, Interspinous Motion, and Fusion Rate With Inter-group Analysis of Allograft and Bioactive Glass-Ceramic Cage Groups
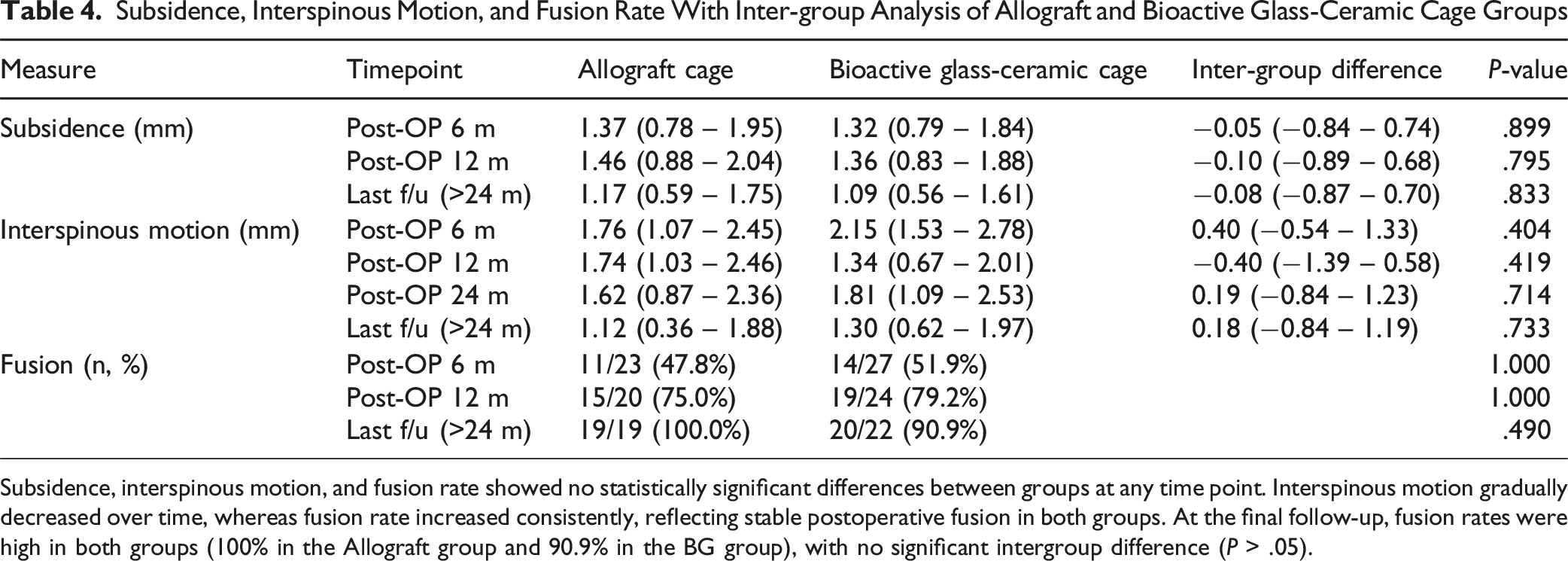
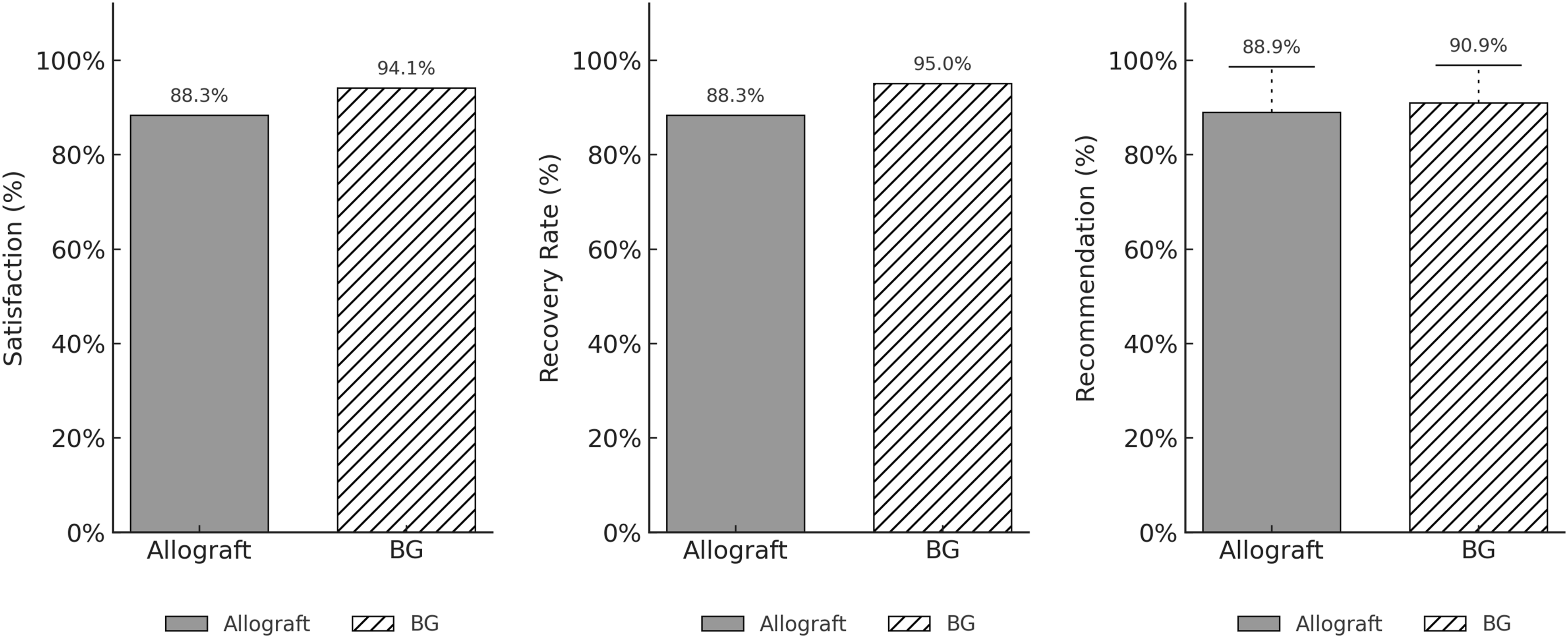
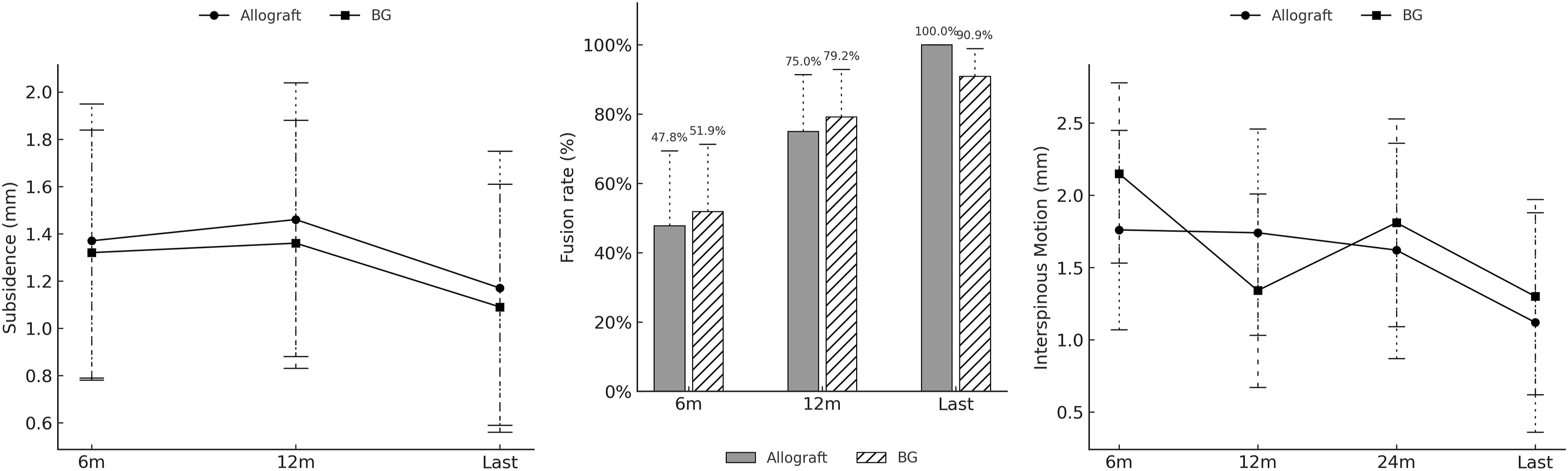
Subsidence, interspinous motion, and fusion rate showed no statistically significant differences between groups at any time point. Interspinous motion gradually decreased over time, whereas fusion rate increased consistently, reflecting stable postoperative fusion in both groups. At the final follow-up, fusion rates were high in both groups (100% in the Allograft group and 90.9% in the BG group), with no significant intergroup difference (P > .05).
At the last available visit, patient-reported global ratings of surgical intervention were similarly favorable. Satisfaction averaged 88.33 ± 14.14% in allograft and 94.09 ± 11.30% in BG (Mann–Whitney U test, P = 0.215). Subjective recovery rate averaged 88.33 ± 15.72% vs 92.18 ± 16.18% (Mann–Whitney U test, P = .329). Recommendation rates were likewise high and comparable (allograft 16/18, 88.9% vs BG 20/22, 90.9%, Fisher’s exact test, P = 1.000). Sensitivity analyses (GEE; ITT-BOCF) yielded no material differences from the primary LMM findings; the overall interpretation was unchanged.
Radiologic Parameters
Using linear mixed models (LMMs) to contrast groups at each visit (BG–allograft), cervical lordosis favored allograft at 1 month (estimate −5.06°, 95% CI −8.18 to −1.94; P = .001) and 6 months (−4.62°, −7.74 to −1.51; P = .004), but did not differ at 12 months (−0.88°; P = .618) or last follow-up (−0.19°; P = .917). T1 slope contrasts were small and not significant at any visit. T1sCA was higher with BG early—1 month (+4.65°, 1.92 to 7.39; P < .001) and 6 months (+3.67°, 0.70 to 6.65; P = .016)—with no between-group differences at 12 months (−2.03°; P = .296) or last follow-up (−3.13°; P = .253).
When comparing between-group differences in improvement (change from baseline; BG–allograft), allograft showed greater gains in cervical lordosis at 1 month (Δ −5.77°, 95% CI −9.76 to −1.79; P = .004) and 6 months (Δ −5.34°, −9.32 to −1.36; P = .009), and greater increases in T1 slope at 12 months (Δ −3.94°, −6.92 to −0.95; P = .010). These improvement differences attenuated thereafter and were not significant at 24 months or last follow-up (Figures 1–5). Chronological changes in patient-reported outcome in each group. In both the BG and Allograft groups, the NDI and VAS-arm scores showed no significant differences between groups at any time point before or after surgery. Both groups demonstrated significant postoperative improvement, and the improved status was maintained through the final follow-up. Although the preoperative VAS-neck score was higher in the Allograft group, no significant intergroup difference was observed after surgery. Similar to other measures, postoperative improvement in VAS-neck was sustained until the final follow-up Comparison of patient satisfaction, subjective recovery rate, and recommendation between allograft and bioactive glass-ceramic cage groups. The satisfaction, recovery rate, and recommendation scores were higher in the BG group compared with the Allograft group; however, none of these differences were statistically significant (P > .05). Both groups demonstrated high satisfaction levels exceeding 80% Radiologic cervical alignment measures with intra- and inter-group analysis of allograft and bioactive glass-ceramic cage groups. Preoperative values of cervical lordosis, T1 slope, and T1sCA showed no significant differences between groups. Cervical lordosis improved more rapidly in the Allograft group at 1 and 6 months postoperatively, showing statistically significant differences at these time points (P < .05). However, no significant intergroup differences were observed at 12 months or at the final follow-up, as the BG group demonstrated continuous improvement in cervical lordosis over time. T1 slope values were lower in the BG group from 6 months postoperatively to the final follow-up, but the differences were not statistically significant (P > .05). The T1sCA, calculated as the difference between T1 slope and cervical lordosis, reflected the trends of both variables—being greater in the BG group at 1 and 6 months postoperatively (P < .05), but showing no significant difference thereafter until the final follow-up Chronological changes in subsidence, fusion rate, and interspinous motion in each group. Subsidence showed no significant difference between the two groups at any time point (P > .05). Although the BG group exhibited a higher fusion rate at 6 and 12 months postoperatively and the Allograft group showed a higher rate at the final follow-up, none of these differences were statistically significant (P > .05). At the final follow-up, fusion rates were high in both groups (90.9% in the BG group and 100.0% in the Allograft group). Interspinous motion also showed no significant intergroup differences and demonstrated a decreasing trend over time, consistent with the high fusion rates observed Representative cases from each group. (A, B) Preoperative and 24-month follow-up standing lateral cervical radiographs of a patient who underwent C5–6 ACDF with an allograft cage demonstrate improved sagittal alignment with solid fusion. (C, D) Twenty-four-month follow-up CT (coronal and sagittal planes) shows bony bridging across the interspace, consistent with Bridwell grade 1 fusion. (E, F) Preoperative and 24-month follow-up standing lateral cervical radiographs of a patient who underwent two-level ACDF at C4–5 and C5–6 with bioactive glass-ceramic cages demonstrate improved cervical lordosis. (G, H) Twenty-four-month follow-up CT images show solid interbody fusion (Bridwell grade 1) at both segments

Although inter-group contrasts were null at later visits, within-group trajectories differed: in the BG group, cervical lordosis remained increased and T1sCA remained decreased relative to baseline at the last follow-up, whereas the allograft group did not show a comparable sustained pattern.
Fusion and Subsidence
Across postoperative assessments—defining the last visit as the latest visit >24 months—the two groups remained comparable; the timing of the last visit averaged 46.2 ± 19.10 months. Observed bony fusion (Bridwell grade 1 or 2) did not differ at any time point: 6 months 47.8% vs 51.9% (Fisher’s exact, P = 1.000), 12 months 75.0% vs 79.2% (P = 1.000), and last 100.0% vs 90.9% (P = .490). Subsidence increased from 6 to 12 months and then modestly declined; between-group contrasts were not significant at any visit: 6 months BG–allograft −0.05 mm (95% CI −0.84 to 0.74; P = .899), 12 months −0.10 mm (−0.89 to 0.68; P = .795), last −0.08 mm (−0.87 to 0.70; P = .833). Interspinous motion (ISM) decreased over time in both cohorts with no intergroup separation: 6 months + 0.40 mm (−0.54 to 1.33; P = .404), 12 months −0.40 mm (−1.39 to 0.58; P = .419), 24 months + 0.19 mm (−0.84 to 1.23; P = .714), last +0.18 mm (−0.84 to 1.19; P = 0.733).
Adverse Events
Operative time and length of hospital stay were comparable between groups. No major acute complications occurred; specifically, there were no postoperative deep infections, clinically significant hemorrhage, or events requiring urgent reoperation or other invasive intervention. Minor adverse events—small hematomas, incisional or graft‐site discomfort, and localized pain—occurred in a few patients and resolved with conservative management without surgical intervention. No implant-related complications were observed other than subsidence; specifically, there were no cases of cage breakage or migration.
In the allograft group, one patient who underwent C5-6 fusion had pseudoarthrosis with graft resorption at 12 months, persisting as non-fusion on 6-year CT. However, despite the radiographic nonunion, the patient exhibited no pain, functional limitation, or mechanical instability attributable to it. Another allograft patient had mild dysphagia through 12 months, which improved after otolaryngology care and was nearly absent by 5 years.
During follow-up, three patients underwent additional cervical operations (allograft n = 1, BG n = 2): laminotomy decompression at the index level at 12 months (allograft), unilateral laminotomy for bilateral decompression at C4-5 at 18 months for herniated nucleus pulposus (BG), and tumor resection for a caudal-level spinal meningioma approximately 3 years after ACDF (BG). Per protocol, patient-reported outcomes and cervical alignment were censored at the last visit before these procedures. Overall, serious complications were uncommon and similar between groups.
Discussion
This extended observational follow-up of a randomized ACDF cohort, with a mean follow-up of 53.5 months, may extend prior evidence into the mid-to long-term by tracking both clinical and radiographic endpoints beyond 24 months in patients treated with bioactive glass-ceramic (BG) cages vs structural allograft.
Compared with the 12-month follow-up results of the parent RCT, the present study—with a mean follow-up of 53.5 months—suggests that the postoperative improvements in PROMs observed at 12 months were generally maintained through the final visit in both groups. Patient satisfaction likewise remained favorable at long-term follow-up. Radiologically, early between-group differences in cervical alignment appeared to attenuate over time, with no clear divergence at later follow-up. Fusion-related and implant-associated measures showed gradual progression over time, following the expected postoperative course after ACDF. Finally, serious adverse events and additional cervical procedures were uncommon and did not indicate late safety differences between graft materials.
After adjusting for baseline differences, between-group differences in the magnitude of improvement remained non-significant at the final assessment. Beyond pain, perioperative experience metrics—satisfaction, recovery rate, and willingness to recommend—tended to favor BG numerically but did not reach statistical significance. These clinical patterns are directionally consistent with the parent randomized controlled trial from our institute and with prior reports of non-inferior short-term performance of BG relative to established materials.23-28,30,32
Unlike most prior ACDF reports on BG cages, our study and its parent randomized controlled trial report longitudinal changes in radiographic cervical sagittal alignment parameters. Early contrasts in cervical lordosis (1-6 months) favored allograft but attenuated by 12 months and were absent at the last visit, suggesting short-term postoperative settling followed by fusion-related stabilization rather than a sustained biomechanical disparity. T1 slope remained near baseline in the BG group but increased and then persisted in the allograft group; accordingly, while overall changes in T1sCA were small, the BG group showed a significant decrease in T1sCA. Importantly, both groups remained within a sagittally balanced range throughout, yet the BG group exhibited a measurable improvement in sagittal balance in this study. Given that lower cervical ACDF contributes substantially to lordosis formation, this alignment signal is potentially meaningful and warrants further study.
At the segment level, fusion rates at the last follow-up were high and similar (allograft 100.0%; BG 90.9%), cage subsidence was comparable between groups, and interspinous motion declined over time without intergroup separation, consistent with progressive consolidation. From a biomaterials standpoint, autograft efficacy is offset by donor-site morbidity and longer operative time; allograft avoids harvest but carries variability and theoretical risks; titanium may concentrate endplate stress and promote subsidence in some constructs; and PEEK provides modulus matching and radiolucency but lacks intrinsic osteointegration, often necessitating supplemental graft.11,14,16 By contrast, bioactive glass-ceramic systems (CaO–SiO2–P2O5–B2O3) exhibit surface bioactivity, form an apatite-like layer, and promote bone bonding/osteointegration—mechanisms that plausibly explain the convergence of outcomes once early postoperative effects abate.15,17,19
Two studies with finite-element analyses comparing BG with structural allograft further report lower peak von Mises stress within vertebral bone and the spacer and lower bone–implant contact pressure with BG, implying a lower theoretical risk of endplate collapse, subsidence, or implant yield.27,32 In our cohort, those modeled advantages did not directly translate into a statistically significant between-group difference in clinical subsidence, possible due to small cohort population.
Collectively, these data support BG as an alternative that preserves fusion, alignment maintenance, and patient-reported recovery over several years. Consistent with the broader literature, a prospective observational comparison reported similar or higher CT-based fusion rates for BG at 12 and more than 60 months and parallel improvements in NDI and VAS, and other 12-month series likewise found no meaningful differences in fusion between BG and allograft. 32
Limitations include the single-center setting with modest sample size, variation in imaging modalities over time, incomplete blinding of imaging assessors due to visible implant characteristics, and protocol-driven censoring prior to later operations. Also, given the number of outcomes and time points examined, the possibility of type I error cannot be excluded. Nonetheless, a key strength of our study is that this extended follow-up preserves the original randomized allocation, enabling mid-to long-term comparisons with reduced confounding and stronger internal validity than de novo observational cohorts, with sensitivity analyses support the robustness of the conclusions. Taken together, growing data already delineate the advantages of bioactive glass-ceramic; with confirmatory long-term biomechanical and clinical studies, these benefits are poised to translate into broader, evidence-based adoption across cervical fusion indications.
Conclusion
In this single-center cohort originally randomized to allograft or BG cages and followed for a mean of 53.5 months, both allograft cage and bioactive glass-ceramic cage groups achieved sustained improvements in pain and disability with no clinically meaningful between-group differences at final follow-up. Early alignment differences dissipated by 12 months, and fusion, subsidence, and ISM were similar, with no device failures. These findings support longer term safety of BG cages as an effective alternative to structural allograft for 1-2-level ACDF.
Footnotes
Author Note
I confirm that the abstract submitted is original and has not been submitted elsewhere, either in part or in whole.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure Statement
Dr Jin-Sung Kim is presently a consultant for RIWOspine (Knittlingen, Germany), Nexon Medical AG, Switzerland, Simulatory AG, Switzerland, and Elliquence, LLC (Baldwin, NY, USA). Except for that, the authors have nothing to disclose.