
Abstract
Study Design
Retrospective cohort study.
Objective
There is a lack of contemporary evidence evaluating the influence of estrogen replacement therapy (ERT) on clinical outcomes following lumbar spine surgery. We hypothesized that ERT would be associated with lower rates of pseudoarthrosis following lumbar spine fusion.
Methods
A multi-institutional electronic medical record database was queried for female patients >50 years old undergoing single- and multi-level lumbar spine fusion surgeries. Propensity score matching (1:1) resulted in evenly distributed ERT and non-ERT cohorts. Exclusion criteria included history of previous lumbar spine surgery, spine neoplasms, trauma, inflammatory, or infectious bone conditions. Comparisons were made with independent sample t-tests.
Results
There were 2268 patients in the single-level and 2776 patients in the multi-level lumbar spine fusion cohorts. During the thirty-day post-operative period, patients in the ERT cohorts demonstrated significantly higher rates of emergency department utilization following single-level and multi-level lumbar spine fusion. Significantly lower rates of postoperative blood transfusion were observed in the non-ERT cohort following multi-level lumbar spine fusion. At 5 years, patients in the non-ERT cohort demonstrated significantly higher rates of pseudoarthrosis following single-level and multi-level lumbar spine fusion. However, at 5 years patients in the ERT cohort demonstrated similar rates of adjacent segment disease and lumbar spine reoperation following single-level and multi-level lumbar spine fusion.
Conclusions
Pre-operative ERT exposure was associated with lower rates of pseudoarthrosis following lumbar spine fusion with similar rates of lumbar spine reoperation. These findings can enhance pre-operative counseling and risk stratification prior to lumbar spine fusion.
Introduction
Lumbar spinal fusion is a commonly performed surgery for the management of degenerative spine disorders including spinal stenosis, spondylolisthesis, and degenerative disc disease.1,2 Previous research has documented the impact of multiple patient factors on clinical outcomes following lumbar spinal fusion surgery including age, bone quality, and multiple medical comorbidities.3,4 Recently, sex-based differences in musculoskeletal physiology and bone health have gained increasing attention due to its influence on post-operative outcomes following spine surgery.5-8
Estrogen plays a vital role in bone metabolism, collagen synthesis, and inflammatory modulation, which may influence fusion rates fusion following lumbar spine surgery.9-12 Postmenopausal estrogen deficiency has been associated with decreased bone mineral density and impaired rates of osteointegration, which may contribute to suboptimal outcomes following lumbar spine fusion surgery.13-15 Despite these associations, the impact of estrogen replacement therapy (ERT) on outcomes following lumbar spinal fusion remains inadequately characterized across large patient cohorts.16,17
Thus, the objective of this study was to assess the association between pre-operative ERT and clinical outcomes following lumbar spinal fusion. Based on prior evidence,13-15 we hypothesized that ERT use would be associated with reduced rates of pseudoarthrosis five years following lumbar spinal fusion compared with patients not receiving ERT.
Materials and Methods
This propensity score–matched, multi-institutional cohort study analyzed patients undergoing single- and multi-level posterior lumbar spinal fusion between January 1, 2004, and December 31, 2024. Data were obtained from the TriNetX Research Network (TriNetX LLC, Cambridge, MA), a federated electronic medical record platform that aggregates clinical data from over one-hundred participating healthcare organizations. The dataset includes inpatient, outpatient, emergency department, laboratory data, and medication histories. All data were extracted from the TriNetX Research Collaborative Network on November 2, 2025. TriNetX compiles real-time, patient-level information and does not rely on healthcare administrative claims or employment records. Historical records prior to the implementation of ICD-10 were mapped to their corresponding ICD-9 codes to maintain consistency. This study was exempt from Institutional Review Board (IRB) review due to the lack of identifiable patient information. This study also adhered to observational reporting standards for cohort studies from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).
Diagnosis and Procedure Codes Associated with the Study Design
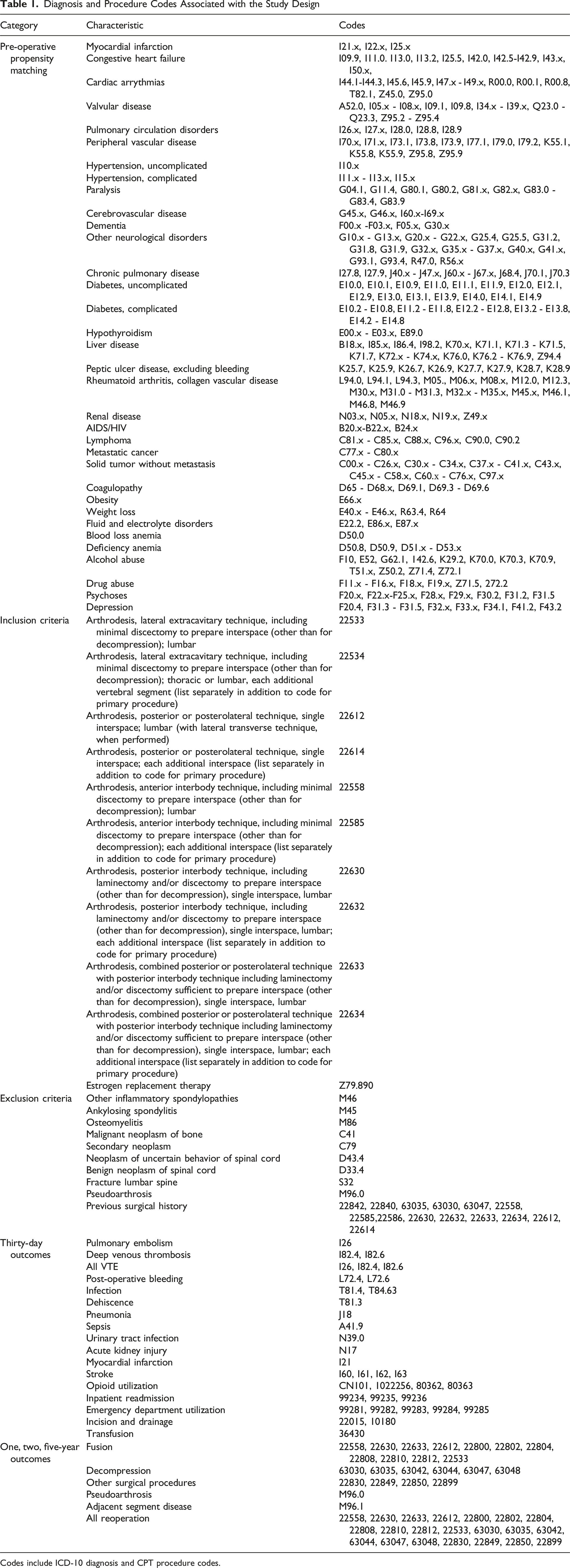
Codes include ICD-10 diagnosis and CPT procedure codes.
To reduce confounding between patients in the ERT and non-ERT cohorts, 1:1 propensity score matching was performed based on over 320 clinical variables including age, sex, race, body mass index, and other medical comorbidities (Table 1). Comorbidities were identified using ICD-10 codes derived from the Charlson and Elixhauser comorbidity indices including essential hypertension (ICD-10: I10), hyperlipidemia (ICD-10: E78.5), diabetes mellitus (ICD-10: E08-E13), ischemic heart disease (ICD-10: I20-I25), chronic obstructive pulmonary disease (ICD-10: J44.9), chronic kidney disease (ICD-10: N18), anemia (ICD-10: D64.9), long-term anticoagulant use (ICD-10: Z79.01), and tobacco use (ICD-10: Z72.0) (Table 1). Propensity scores were calculated using logistic regression and patients were matched using nearest-neighbor matching without replacement and application of a caliper width of 0.10. Post-match balancing was evaluated using standardized mean differences (SMDs) all of which were <0.10, indicating adequate covariate balance.
Perioperative and longitudinal outcomes were identified using ICD-10, SNOMED, and CPT codes, which were evaluated at 30 days, 1-, 2-, and 5-year intervals after the index surgery (Table 1). The primary outcomes of interest were pre-defined as rates of pseudoarthrosis (ICD-10: M96.0), adjacent segment disease (ICD-10: M96.1), and all lumbar spine reoperation (CPT codes (22558, 22630, 22633, 22612, 22800, 22802, 22804, 22808, 22810, 22812, 63030, 63035, 63042, 63044, 63047, 63048, 22830, 22849, 22850, 22899). Outcomes of interest were compared between patients in the ERT and non-ERT cohorts. In compliance with TriNetX privacy protocols, outcome counts <10 were rounded up to 10 to protect patient confidentiality. Binary outcomes were analyzed using the measure of association function, while time-to-event data were evaluated via Kaplan–Meier survival analysis with log-rank testing. Continuous variables were presented as means ± standard deviations and compared with independent-samples t-tests. Categorical variables were expressed as counts and percentages, which were compared using Chi-squared or Fisher’s exact tests, as appropriate. Odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were calculated. Patients with preexisting outcomes prior to the observation window were excluded from time-to-event analyses. A two-tailed P value <.05 was considered statistically significant.
Results
Study Cohorts
Demographic and Medical Co-morbidity Data Used for Propensity Matching
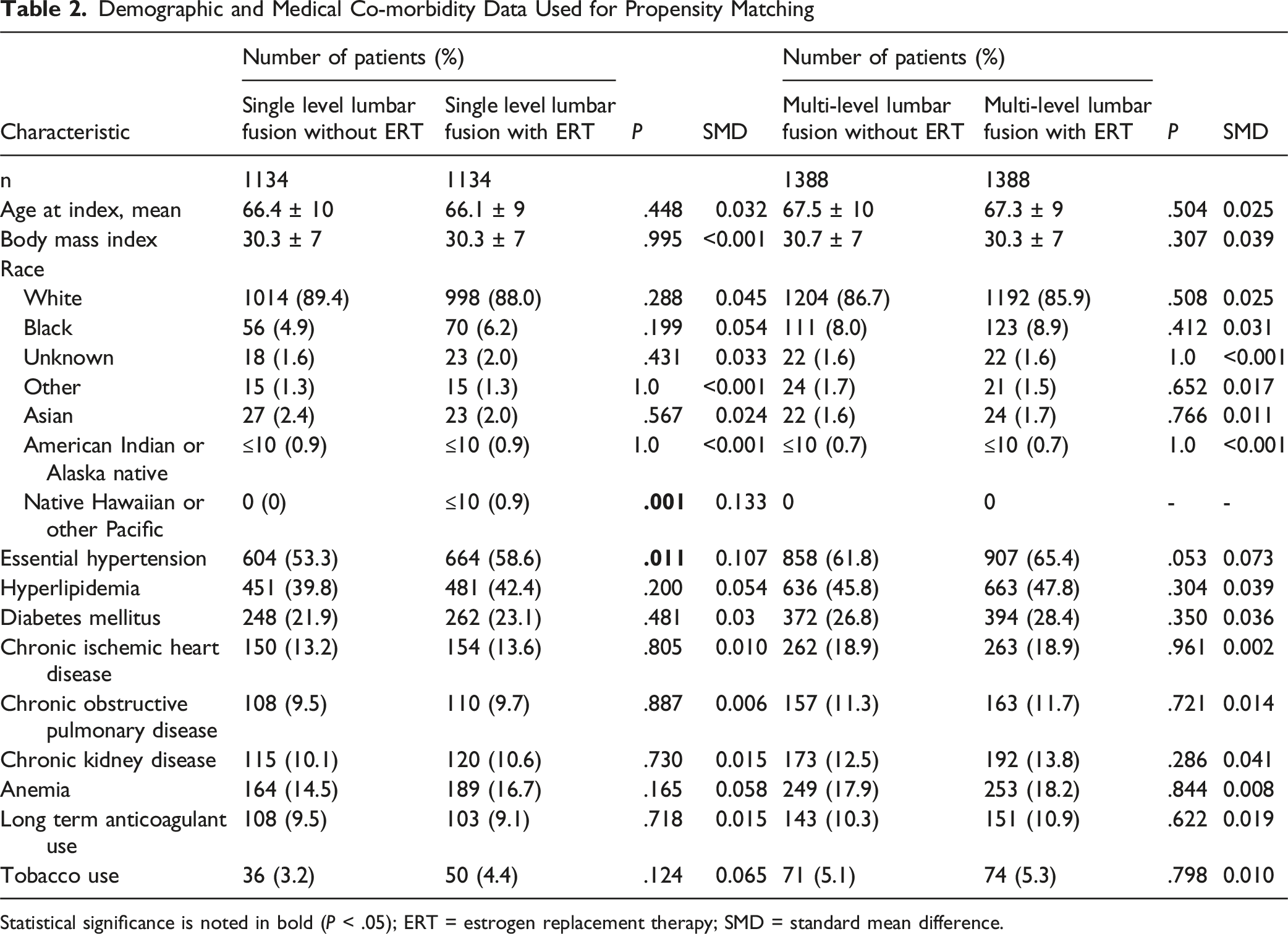
Statistical significance is noted in bold (P < .05); ERT = estrogen replacement therapy; SMD = standard mean difference.
Thirty-Day Outcomes
Comparison of Thirty-Day Complication Rates Following Lumbar Spine Fusion
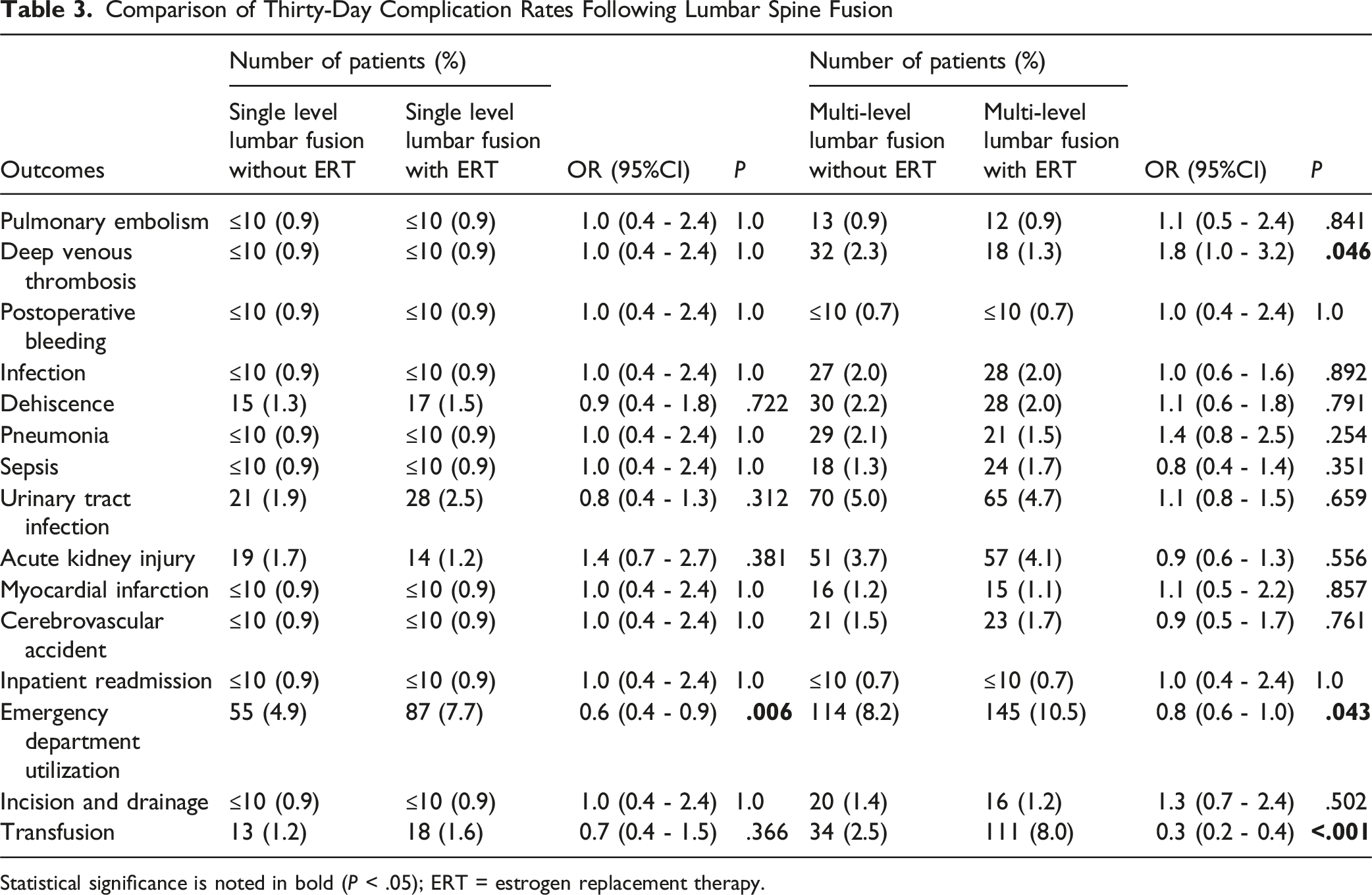
Statistical significance is noted in bold (P < .05); ERT = estrogen replacement therapy.
One-Year Outcomes
Comparison of One-Year Complication Rates Following Lumbar Spine Fusion
Statistical significance is noted in bold (P < .05); ERT = estrogen replacement therapy.
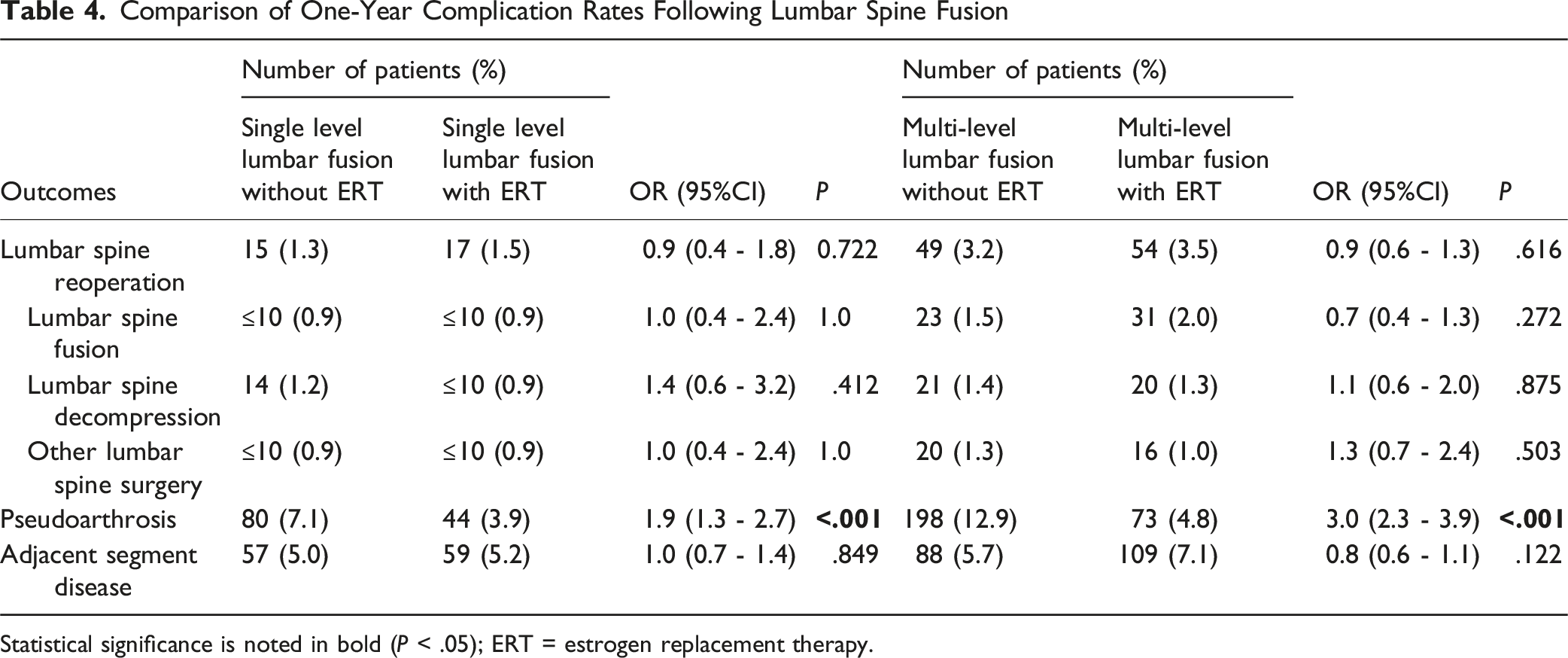
Among patients undergoing multi-level lumbar spine fusion, the non-ERT cohort demonstrated significantly higher rates of pseudoarthrosis (OR: 3.0, 95% CI: 2.3-3.9; P < .001) compared to the ERT cohort within the one-year postoperative period. There were no significant one-year differences in the rates of adjacent segment disease and lumbar spine reoperation including fusion, decompression, and other lumbar spine surgical procedures following multi-level lumbar fusion by ERT status (P > .05).
Two-Year Outcomes
Comparison of Two-Year Complication Rates Following Lumbar Spine Fusion
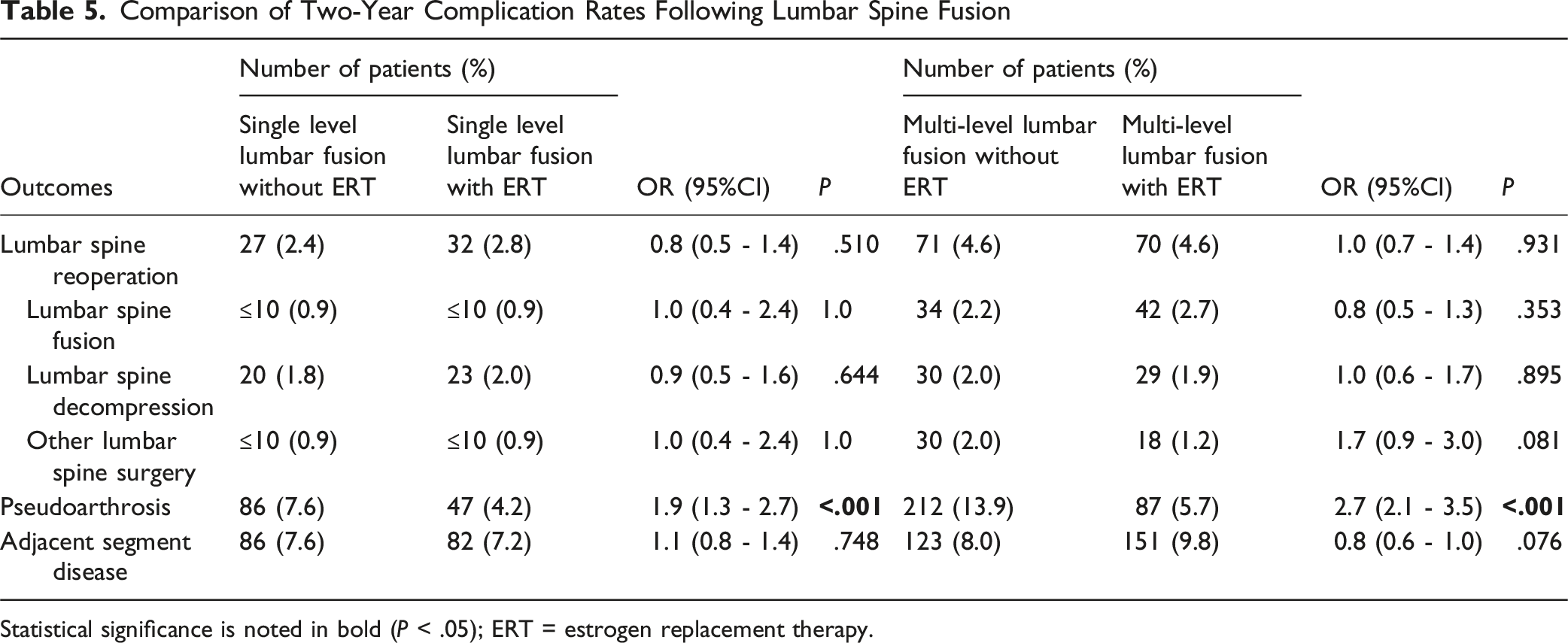
Statistical significance is noted in bold (P < .05); ERT = estrogen replacement therapy.
Among patients undergoing multi-level lumbar fusion, the non-ERT cohort demonstrated significantly higher rates of pseudoarthrosis (OR: 2.7, 95% CI: 2.1-3.5; P < .001) compared to the ERT cohort during the two-year postoperative period. There were no significant two-year differences in the rates of lumbar spine reoperation including fusion, decompression, and other lumbar spine surgical procedures following multi-level lumbar fusion by ERT status (P > .05).
Five-Year Outcomes
At five years, patients in the non-ERT cohort demonstrated significantly higher rates of pseudoarthrosis (OR: 2.0, 95% CI: 1.4-2.8; P < .001) following single-level lumbar spine fusion (Figure 1). There were no significant five-year differences in the rates of lumbar spine reoperation including fusion, decompression, and other lumbar spine surgical procedures following single-level lumbar fusion by ERT status (P > .05, Table 6). Survival analysis for pseudoarthrosis diagnosis following single-level lumbar spine fusion Y-axis demonstrates the percentage of patients without pseudoarthrosis and x-axis demonstrates the number of days since the index surgery; ERT = Estrogen replacement therapy Comparison of Five-Year Complication Rates Following Lumbar Spine Fusion Statistical significance is noted in bold (P < .05); ERT = estrogen replacement therapy.
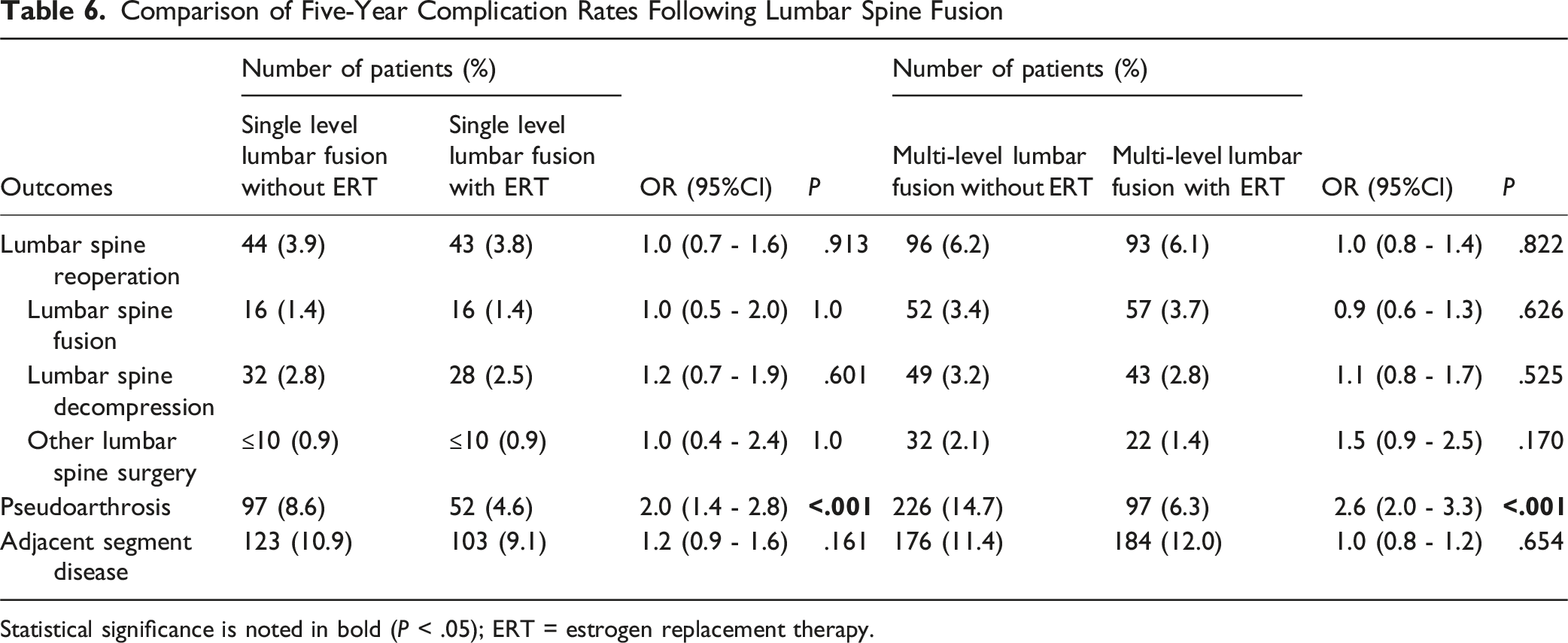
At 5 years, patients in the non-ERT cohort demonstrated significantly higher rates of pseudoarthrosis (OR: 2.6, 95% CI: 2.0-3.3; P < .001) following multi-level lumbar spine fusion (Figure 2). There were no significant five-year differences in the rates of lumbar spine reoperation including fusion, decompression, and other lumbar spine surgical procedures following multi-level lumbar fusion by ERT status (P > .05). Survival analysis for pseudoarthrosis diagnosis following multi-level lumbar spine fusion Y-axis demonstrates the percentage of patients without pseudoarthrosis and x-axis demonstrates the number of days since the index surgery; ERT = Estrogen replacement therapy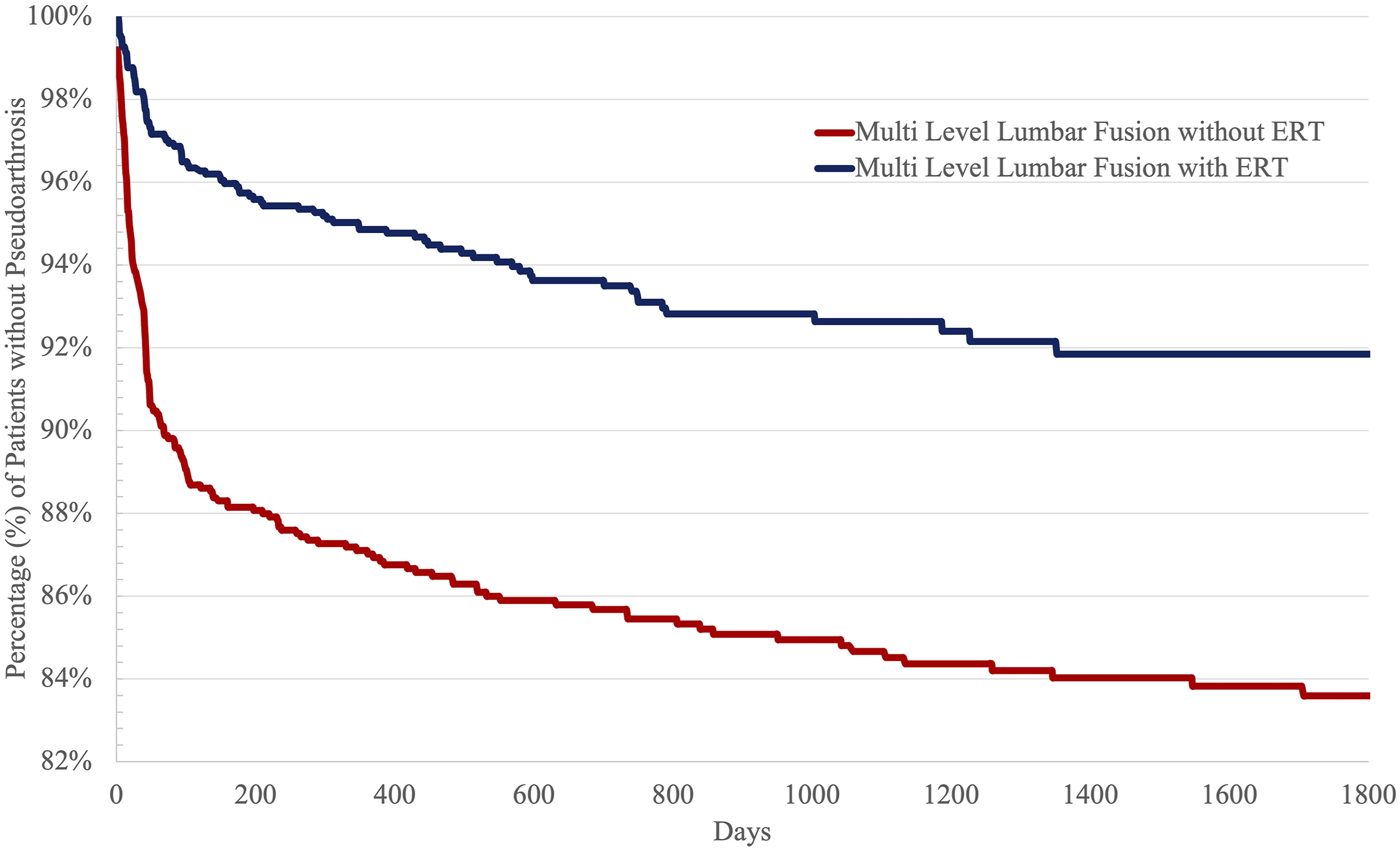
Discussion
Patients with pre-operative exposure to ERT demonstrated lower rates of pseudoarthrosis at five years following lumbar spinal fusion. However, there were similar rates of adjacent segment disease and lumbar spine reoperation between the two cohorts at 5 years. This study also demonstrated that pre-operative exposure to ERT was not associated with increased rates of thirty-day medical complications including cerebrovascular accident and venous thromboembolic events. However, pre-operative exposure to ERT was associated with higher rates of ED utilization, which may suggest the need for greater healthcare resource allocation during the early post-operative period. Collectively, these results confirmed our hypothesis that ERT use would be associated with lower rates of pseudoarthrosis following lumbar spinal fusion. Results from this study can be used to enhance patient counseling and risk stratification prior to lumbar spinal fusion.
The literature suggests that ERT has a biologically plausible and potentially beneficial influence on lumbar spinal fusion outcomes through its effect on inflammatory modulation and bone metabolism.18-20 Estrogen deficiency is associated with increased bone resorption, reduced osteoblastic activity, and poor bone quality, which may compromise fusion mass formation and increase the risk of pseudoarthrosis in postmenopausal patients. 21 By mitigating these processes, ERT may enhance fusion biology, increase bone mineral density, and support hardware stability.22,23 However, clinical evidence suggests that lumbar spine fusion rates can be influenced by patient age, baseline bone density, comorbidities, smoking status, and the use of adjunctive osteobiologics.24,25 Importantly, potential benefits of pre-operative ERT exposure must be weighed against the known systemic risks of ERT including thromboembolic and cardiovascular events, which limit its routine use in post-menopausal women undergoing spine fusion surgery. 26 While ERT may contribute to a favorable biological environment for lumbar spine fusion in estrogen-deficient patients, it should be considered as part of a broader, individualized strategy for bone health optimization. 27
Prior studies have also highlighted potential risks and medical complications associated with pre-operative ERT exposure following surgery due to the pro-thrombotic nature of estrogen. 28 Venous thromboembolic events are feared complications following elective spine surgery, which vary between 0.2% and 13.6% depending on several patient factors. 29 Spine surgeons must balance the increased risk of venous thromboembolic events following surgery with the increased risk of post-operative bleeding events associated with prophylactic anticoagulation following lumbar spine fusion. 30 There are currently no widely accepted guidelines to inform spine surgeons on the use of chemoprophylaxis for venous thromboembolic events following lumbar spine surgery.31,32 Prior studies have demonstrated that preoperative ERT is associated with increased risks of deep vein thrombosis and pulmonary embolism following spine surgery. 26 However, studies in the arthroplasty literature demonstrate lower rates of thromboembolic events among patients with ERT exposure after total joint arthroplasty, which highlights the risk dependency on the type of surgery. 33 In the present study, pre-operative ERT exposure was not associated with increased risks of deep vein thrombosis, pulmonary embolism, myocardial infarction, or cerebral vascular incidents following lumbar spinal fusion.
However, patients with pre-operative ERT exposure demonstrated higher rates of emergency department utilization following lumbar spine fusion, which may indicate a need for greater healthcare resource allocation during the early post-operative period for pain, anxiety, and other related factors. Spine surgeons should recognize this association and develop strategies to mitigate this risk following surgery including enhanced post-operative pain management protocols, earlier scheduled post-operative visits, and better-informed patient-specific counseling. The similar rates of medical complications observed between patients with and without pre-operative ERT exposure demonstrate the relative safety of ERT following lumbar spine fusion surgery.
Recent spine surgery literature has emphasized the importance of perioperative bone health optimization prior to lumbar spine fusion.5,6 There are over 54 million patients in the United States alone that have osteoporosis, which is defined as having a bone mineral density that is 2.5 standard deviations below the average for a sex and race-matched cohort. 7 In the future, with the ease of measuring Hounsfield units on routine computerized tomography scans, the prevalence of osteoporosis is expected to increase significantly. 20 Prior studies in the spine surgery literature have demonstrated the difficulty of instrumentation and fusion among patients with osteoporosis, which can contribute to higher rates of pseudoarthrosis and proximal junctional failure.4,6,8 Preoperative management of osteoporosis remains essential to mitigate the risk of these complications and enhance clinical outcomes after lumbar spine fusion.18,19 Patients undergoing lumbar spine fusion should receive routine mineral supplementation in the form of calcium and vitamin D. 20 Patients with low bone mineral density including post-menopausal female patients should also be considered for anti-resorptive therapies like bisphosphonate or anabolic agents including ERT or parathyroid hormone. 21 In our study, rates of lumbar spine reoperation were similar between the two cohorts following lumbar spinal fusion despite lower rates of pseudoarthrosis observed in the ERT cohort. This suggests the presence of other etiologies for reoperation following lumbar spine fusion including symptom recurrence. Collectively, the best available evidence suggests that post-menopausal women present unique perioperative risks during lumbar spine fusion, which should be addressed through appropriate medical management prior to surgery.22-25
There were several limitations to this study. While broad and inclusive across many healthcare organizations, electronic medical record data in TriNetX has coding limitations including a lack of certain clinical variables. For example, radiographic data, functional status, and patient reported outcome measures were not available. Rates of pseudoarthrosis were determined from recorded diagnostic codes as radiographic data were unavailable. Furthermore, biometric data including bone mineral density assessments were not unavailable in the electronic medical record. Inclusion of these data in future investigations can allow for an objective assessment of the impact of ERT on bone mineral density. Additionally, the reasons for increased emergency department utilization observed among patients on ERT could not be determined from the electronic medical record data due to a lack of associated diagnoses. The quality of electronic medical record data relies on the healthcare provider to input clinical endpoints accurately and consistently. Furthermore, the retrospective nature of this study limited the study findings to associations between variables. Future prospective studies are needed to validate these associations. The specific regimens for ERT exposure prior to lumbar spinal fusion were not detailed in TriNetX including dosing, administration, and duration. The magnitude and route of ERT administration may impact the bone metabolic profile and potential risk for medical complications following lumbar spine fusion. Underlying medical reasons for estrogen deficiency likely varied between study participants although all were post-menopausal women. While propensity score matching allowed for the creation of similar study cohorts with shared demographics and medical comorbidities, there was likely residual confounding from unaccounted variables. For example, additional institutional variables including surgeon experience, institutional volume, and surgical technique were unaccounted for in this study, which are known modulators of clinical outcomes following lumbar spine fusion. The purpose of this study, however, was to determine the association between pre-operative ERT exposure and rates of pseudoarthrosis, reoperation, and other medical complications following lumbar spine fusion.
In conclusion, pre-operative ERT exposure was associated with lower rates of pseudoarthrosis following lumbar spine fusion. Patients with pre-operative ERT exposure did not demonstrate higher rates of thirty-day medical complications after lumbar spine fusion. However, pre-operative ERT exposure was associated with higher rates of ED utilization following lumbar spine fusion. At 5 years, patients with pre-operative ERT exposure had similar rates of lumbar spine reoperation compared to patients without ERT exposure. Overall, results from this study highlight the relative safety of pre-operative ERT exposure prior to lumbar spine fusion surgery and a potential benefit with lower rates of pseudoarthrosis. Collectively, these findings suggest that pre-operative ERT exposure may enhance bone biology and fusion following lumbar spine fusion. Ultimately, insights from this study can enhance patient risk stratification and informed decision-making prior to lumbar spine fusion surgery.
Footnotes
Author Contributions
J.S.: Project conceptualization, data collection, data analysis, manuscript composition, manuscript revisions.
R.J.F.: data collection, data analysis, manuscript composition, manuscript revisions.
R.A.R.: project conceptualization, manuscript composition, manuscript revisions.
C.A.R.: Project conceptualization, data analysis, manuscript composition, manuscript revisions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
This study received review exemption based on the policies of the Institutional Review Board.