
Abstract
Study Design
Retrospective matched case-control study.
Objectives
Pelvic fixation failure (PFF) is a rare, underrecognized mechanical complication from surgical management of adult spinal deformity (ASD). Studies show that residual postoperative malalignment may increase mechanical stress on pelvic instrumentation, but the role of global radiographic parameters in predicting PFF remains poorly defined. Our study aims to identify radiographic predictors of PFF and evaluate the time-dependent relationship between residual deformity and PFF rates.
Methods
This was a single-center, retrospective, matched case-control study of ASD patients who underwent pelvic fixation from 2016-2024 and had >1-year postoperative follow-up. PFF was defined as any reoperation for pelvic screw or rod failure, and patients were matched in a 1:4 ratio by age and sex. Global radiographic outcome measures were collected, and multivariable logistic regression and Cox proportional hazard models were used to assess PFF predictors and time-to-failure.
Results
31 (5.99%) of 517 eligible patients experienced PFF, and 94 patients were included in total after propensity matching with 63 eligible controls. Postoperative C2 Tilt (C2T) (OR: 1.15, P = 0.013) and ΔC7-Central Sacral Vertical Line (ΔC7-CSVL) (OR: 1.66, P = 0.007) were associated with increased PFF risk. T1-Pelvic Angle (T1PA) trended toward significance (P = 0.062). Time-to-event analysis confirmed these findings and identified a C2T cutoff for hazard ratio>1 of 6.9°.
Conclusions
Residual postoperative global spinal imbalance, specifically C2T, is a significant predictor of PFF and accelerated time-to-failure. This highlights the importance of achieving global alignment intraoperatively to improve long-term construct durability and prevent PFF complications in ASD surgery.
Keywords
Introduction
Adult spinal deformity (ASD) is a complex, often progressive spinal disorder that frequently requires long-segment thoracolumbar fusions to correct global sagittal and coronal malalignment.1,2 Stabilization of the distal construct using pelvic fixation methods has become a cornerstone of ASD surgery, as it increases construct rigidity and reduces the likelihood of construct-related complications such as distal instrument instability or sacral insufficiency fractures.3,4 That said, while pelvic fixation is widely utilized, pelvic fixation failure (PFF) remains a rare yet underrecognized mechanical complication. Prior studies report a 3-41% pelvic fixation failure rate. 5 This wide range underscores the heterogeneity of published PFF rates and highlights the need for matched control analyses to better understand PFF risk factors.
Prior literature has identified several potential contributors to PFF including more extensive preoperative deformity 6 (e.g. high T1-pelvic angle [T1PA]), residual coronal plane deformity 7 (e.g. C7-Central Sacral Vertical Line [C7-CSVL]), longer constructs, 8 and smaller-diameter pelvic screws. 6 However, the role of global residual sagittal plane deformity remains poorly characterized.6,9 Recent interest has focused on global parameters such as C2 Tilt (C2T), which may reflect persistent sagittal imbalance and contribute to increased biomechanical strain. Importantly, residual malalignment may promote the persistence of compensatory mechanisms to achieve global balance. When compensatory mechanisms are exhausted – imbalance ensues. We hypothesized that a persistent global state of imbalance increases construct stress across the lumbosacral junction. 10 Few studies have systematically evaluated this relationship, particularly in a time-dependent framework or using matched controls to account for confounders.
Accordingly, the goals of this study were to: (1) identify radiographic and clinical parameters associated with PFF using a matched control design, (2) evaluate whether residual malalignment or imbalance in the global sagittal and coronal planes increased the risk of PFF, and (3) determine whether residual malalignment or imbalance predicts PFF in a time-dependent manner.
Materials and Methods
Study Design and Outcome Measures
Pelvic Fixation Failure Mechanisms

Pelvic Fixation Failure mechanisms observed in a clinical cohort. The most common failure mode was Screw Loosening (35%), followed by Set Cap Loosening or Dislodgement (23%), Rod Fracture Across Lumbosacral Junction (13%), Pseudoarthrosis (13%), Sacral/Iliac Fracture, and Broken Pelvic Screw (6%).
Data Collection
Demographics
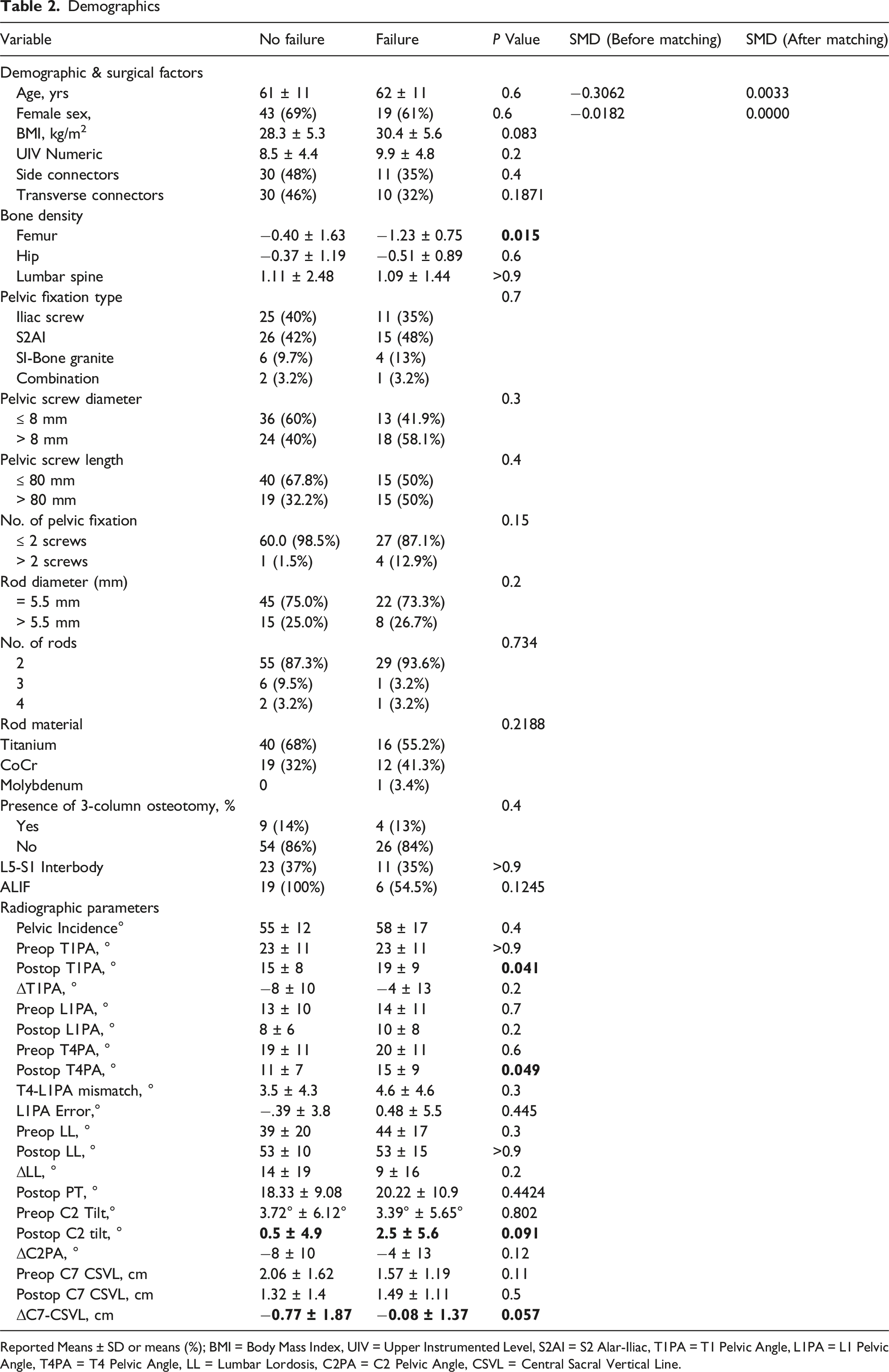
Reported Means ± SD or means (%); BMI = Body Mass Index, UIV = Upper Instrumented Level, S2AI = S2 Alar-Iliac, T1PA = T1 Pelvic Angle, L1PA = L1 Pelvic Angle, T4PA = T4 Pelvic Angle, LL = Lumbar Lordosis, C2PA = C2 Pelvic Angle, CSVL = Central Sacral Vertical Line.
Statistical Analyses
To control for confounding, PFF cases were matched to controls in a 1:4 ratio using nearest-neighbor propensity score matching based on age at surgery, along with exact matching of sex (Supplemental Figure 3). Matched controls were excluded if they had <1 year follow-up or did not have an accessible surgical record. Baseline equivalence between groups before and after matching was assessed to demonstrate standardized mean differences (SMD) of covariates between the PFF group and controls, with a threshold <|0.1| indicating an acceptable balance.
Standard t-tests were used to analyze continuous variables. Fisher’s or Chi-squared tests were used for categorical variables. Univariable analysis of demographic, radiographic, and surgical characteristics was conducted to compare PFF and control groups.
Following univariable analysis, results with a P ≤ 0.1 were included in multivariable logistic regression models to identify independent predictors of PFF.6,7 The final model included postoperative C2T, ΔC7-CSVL, and postoperative T1PA. Receiver operating characteristic (ROC) curves assessed accuracy of distinguishing PFF cases from controls. Cox proportional hazard models estimated hazard ratios (HR) with 95% confidence intervals (CI) for time-to-failure analysis. To identify a clinically meaningful cutoff of postoperative C2T associated with increased risk of PFF, we incorporated a natural spline transformation of C2 Tilt (3 degrees of freedom) to model its non-linear relationship with time-to failure. We then examined the spline curve and its corresponding 95% CI to determine the lowest value that HR and confidence bounds exceeded 1.0. Statistical analyses were performed in R Studio (v4.2 2024.02.29).
Results
851 patients who underwent ASD correction surgery were identified and 517 cases with >1-year radiographic follow-up were screened for PFF. Of these, 31 patients (5.99%) experienced PFF. In total, 94 patients were included in this study after propensity matching and inclusion of 63 eligible control patients (Supplemental Figure 1). Pelvic screw loosening was the most frequently observed mechanism of PFF (n = 11.35%). (Table 1).
Similar mean age was calculated between cases and controls (61.0 ± 11.0 vs 62.0 ± 11.0 years P = 0.6). All matched variables had acceptable balance with SMD <|0.1|, indicating adequate matching of patients with and without PFF. Univariable analyses demonstrated that PFF patients had higher postoperative C2 tilt (2.5° ± 5.6 vs 0.5° ± 4.9, P = 0.091), ΔC7-CSVL (−0.08 cm ± 1.37 vs −0.77 cm ± 1.87, P = 0.057), and 6-week T1PA (19° ± 9 vs 15° ± 8, P = 0.041) (Table 2).
Postoperative T4PA was deemed significantly different between failures & non failures (15° ± 9 vs 11° ± 7, P = 0.049). However, it was not implemented in multivariable analysis due to its high correlation with postoperative T1PA (R = 0.92). Moreover, postoperative T4PA in isolation is less clinically relevant than postoperative T4-L1 mismatch.12–14 L1PAE and HAE were not significantly different between groups (−0.39° ± 3.8° vs 0.48° ± 5.5°, P = 0.45, 3.5° ± 4.3° vs 4.6° ± 4.6, P = 0.30, respectively).
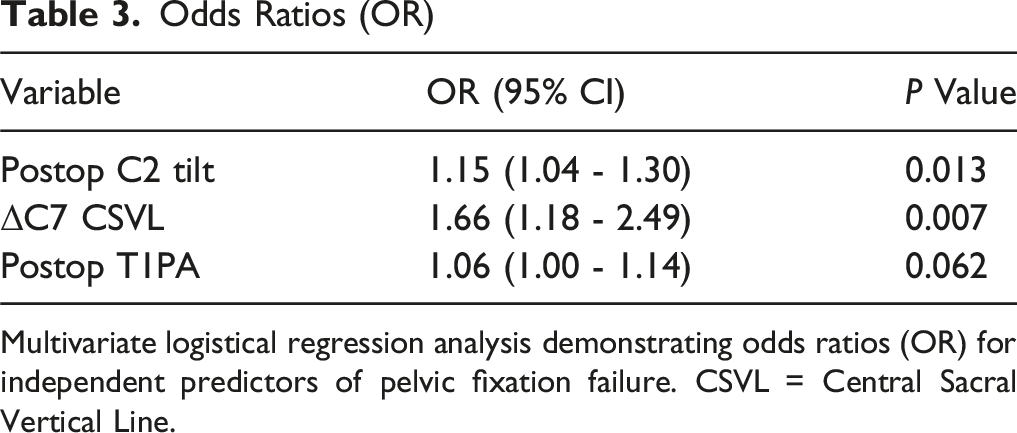
From the univariate analysis, postoperative C2T, ΔC7-CSVL, and postoperative T1PA were identified as potential predictors of PFF. A subsequent multivariable logistic regression model of 82 patients demonstrated good discrimination (AUC = 0.747) using these predictors (Figure 1). Specifically, C2T (OR 1.15, 95% CI 1.04 - 1.30, P = 0.013) and ΔC7-CSVL (OR = 1.66, 95% CI 1.18 - 2.49, P = 0.007) demonstrated significant predictive value for PFF, while only one 6-week postoperative measure of malalignment (T1PA) trended towards significance (OR = 1.06, 95% CI 1.00 - 1.14, P = 0.062) (Table 3). ROC curve for the multivariable logistic regression model predicting PFF. The model included postoperative C2T, postoperative T1PA, and ΔC7-CSVL. AUC was 0.747, indicating good discriminatory ability of the model in distinguishing failure and non-failure cases Odds Ratios (OR) Multivariate logistical regression analysis demonstrating odds ratios (OR) for independent predictors of pelvic fixation failure. CSVL = Central Sacral Vertical Line.
Hazard Ratios, (HR)
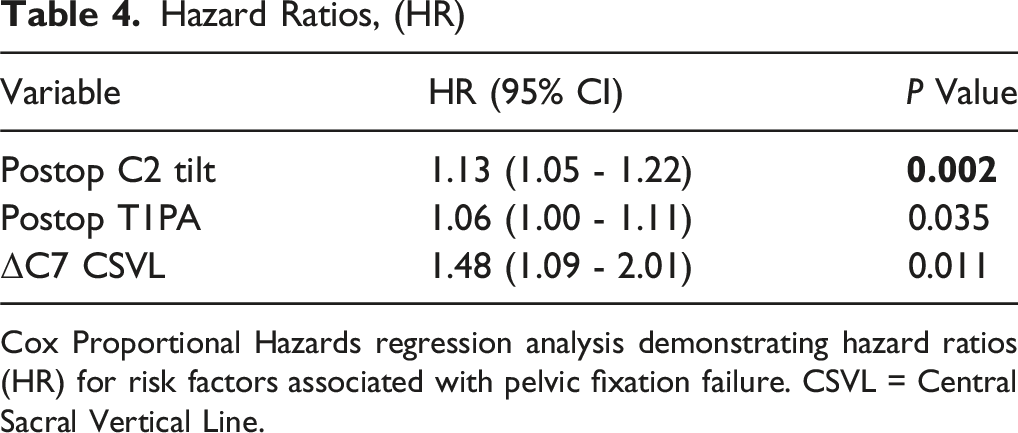
Cox Proportional Hazards regression analysis demonstrating hazard ratios (HR) for risk factors associated with pelvic fixation failure. CSVL = Central Sacral Vertical Line.

Spline curve demonstrating the association between postoperative C2T and the relative hazard of PFF. The shaded region represents 95% CI. The cutoff point for HR >1 was at 6.9° (red line). The dashed green lines denote the proposed safe zone for postoperative C2T (-2-0°)
Sensitivity Analysis
As demonstrated by univariable analyses, femoral neck bone density was significantly decreased in patients who experienced PFF (−1.23 ± 0.75 vs −0.40 ± 1.63, P = 0.015). However, due to inadequate reporting of bone density in several patients (41% missing), we excluded it from the primary core multivariable model. To account for this limitation, we performed a sensitivity analysis using a restricted cohort (n = 48; 21 PFF, 27 controls). Postoperative C2T (β = 0.144, P = 0.046) and ΔC7-CSVL (β = 0.592, P = 0.032) remained significant predictors of PFF while T1PA (β = 0.059, P = 0.195) and bone density did not achieve significance (β = −0.606, P = 0.105).
Discussion
In this study, we presented a matched control analysis to evaluate predictors and HR of PFF after surgery for ASD. Due to the wide range of reported PFF rates, a matched control analysis was critical to better isolate the effects of residual spinal malalignment and other predictors while controlling for confounders. Among 517 patients with >1 year follow-up, 31 PFFs were identified (5.99%). This rate is consistent with prior studies. 5 The AUC for our model indicated acceptable predictive performance (0.747) and clinical relevance for postoperative risk stratification (Figure 1). We identified that global measures of sagittal imbalance were more predictive of PFF than global measures of malalignment.
Specifically, using a matched cohort based on propensity matching scores (Supplemental Figure 1), we found that decompensated sagittal balance (i.e. increased postoperative C2T) was associated with a greater likelihood of PFF. ΔC7-CSVL was used to quantify the magnitude of coronal correction achieved, with the prediction that proper coronal correction would be a negative value, reflecting movement of the C7 plumb line towards the midline (e.g. a preoperative value of 6 cm that was corrected to 0 cm would yield a ΔC7-CSVL of -6 cm), whereas positive values or values closer to 0° would be more indicative of minimal or worsening coronal correction. Postoperative C2T was used as a measure of residual global sagittal imbalance where a higher C2T increases biomechanical load forces on the pelvis, which could contribute to PFF. 9 One measure of alignment (T1PA) trended toward significance (P = 0.062). Finally, time-to-event analysis revealed that residual imbalance and decreased coronal correction (C2T and ΔC7-CSVL) were most associated with a rapid occurrence of PFF.
The significant association between postoperative C2T and PFF observed in our cohort likely reflects a biomechanical mechanism rooted in persistent sagittal imbalance. Rather than representing an isolated independent driver, postoperative C2T likely functions as an integrated surrogate of residual global sagittal imbalance, reflecting the cumulative effect of unresolved alignment and exhausted balance compensatory mechanisms. C2T serves as a radiographic surrogate for the global anterior inclination of the spine above the pelvis. 13 There are a number of circumstances that can yield a persistently elevated C2T postoperatively even in the setting of perfect spinal alignment. However, in the absence of concomitant non-spinal musculoskeletal or neurological deficits, the most common cause of a persistently elevated C2T is persistent sagittal malalignment beyond the individual’s compensatory reserve. A persistently elevated C2T proposed failure mechanism is that this biomechanical stress is ultimately transmitted to the distal fixation points, increasing the risk of construct fatigue and PFF. This pattern is consistent with prior literature that suggests that balanced C2T falls between −2° and 0°.10,13 Our findings build on this notion by not only demonstrating a higher likelihood of PFF in patients with greater postoperative C2T but also an accelerated time to failure, suggesting that imbalance may impact both the incidence and timing of mechanical complications.
While gravitational load transmission through constructs is one explanation, another potential mechanism involves compensatory pelvic retroversion. Recent work by Ouchida et al demonstrated that patients with greater C2PA exhibit significantly increased PT, likely as a postural compensation. 15 This compensatory retroversion, while intuitive, was associated with thoracolumbar decompensation and worse clinical outcomes. This retroversion could theoretically alter the orientation of spinopelvic fixation and change force vectors at the lumbosacral junction, potentially contributing to mechanical failure.15–17 However, in our cohort, postoperative PT did not significantly differ between patients who did and did not experience PFF (P = 0.44), suggesting that pelvic retroversion is not the primary driver of failure in this setting.
Prior studies have identified multiple risk factors for PFF including rod slippage, displacement of set screws from screw tulip heads, and higher magnitude of surgical corrections in the sagittal plane.6,11 One study identified residual coronal plane deformity as a predictor. 7 In our cohort, postoperative C7-CSVL itself was not associated with PFF; however, increasing ΔC7-CSVL, representing a decreasing degree of coronal correction, was predictive. This suggests that the degree of correction in the coronal plane, rather than residual coronal imbalance alone, may influence distal construct mechanics. As with C2T, ΔC7-CSVL demonstrated a time-dependent association with PFF.
Interestingly, alignment parameters alone were not strong predictors of PFF in our cohort, while parameters representing imbalance, particularly postoperative C2T, were. Notably, none of the alignment measures we studied (L1PAE, Hip-axis error, T1PA, C2PA) alone predicted PFF with the exception of a weak T1PA relationship in the time to event model. Specifically, postoperative T1PA was not a significant predictor of PFF in our multivariable logistic regression model (P = 0.062) and only emerged as a significant but weak prediction factor in the Cox proportional hazard analysis (P = 0.035). As seen in prior literature, this discrepancy likely reflects the fact that logistic regression evaluates binary outcomes without accounting for timing, while Cox regression is able to capture time-sensitive effects.18,19 In other words, T1PA may not influence whether a patient ultimately experiences PFF, but amongst those who do fail, a higher T1PA (i.e. greater global malalignment) appears to accelerate the onset of mechanical failure. 20
Clinically, this aligns with biomechanical principles. High postoperative T1PA values indicate sagittal malalignment, which may predispose constructs to increased biomechanical stress and earlier failure (like residual C2T). However, some patients in our study with high T1PA and low C2T did not experience PFF, suggesting that sagittal malalignment alone may not uniformly translate into mechanical failure, particularly in the presence of global balance.
In our cohort, univariable analysis did not demonstrate a significant association between PFF and construct-related variables including the number of pelvic fixation points, number of rods, presence of side or transverse connectors, or the presence of anterior column support. Although several of these features have previously been considered protective against PFF,7,21 our findings suggest that residual global imbalance may supersede individual construct parameters in determining PFF risk.
These findings carry significant implications for surgical planning and postoperative management in ASD. First, our findings reinforce the importance of balance by achieving near-neutral C2T postoperatively as it significantly reduces the risk of PFF. Our spline analysis indicated that C2T >6.9° is associated with progressively increasing risk of PFF, reinforcing the need for meticulous sagittal alignment throughout the entire spinal axis (Figure 2). Notably, C2T may prove to be more informative than other segmental parameters, as it reflects the global position of the head with relation to the vertical plumb line anchored to the fulcrum of rotation (i.e. femurs). Second, the identification of ΔC7-CSVL as a risk factor highlights the importance of also addressing coronal plane correction intraoperatively. Each centimeter increase in ΔC7-CSVL, reflecting less coronal correction, was associated with a 40% increase in odds of failure.
Although the absolute differences in postoperative alignment parameters between groups were numerically modest, these differences represent persistent deviations from global balance, rather than isolated segment variation. Even small residual imbalance, when propagated across a long construct, may substantially increase distal bending moments and cyclic loading at the lumbosacral junction, thereby predisposing patients to PFF over time. From a surgical planning perspective, these findings suggest that achieving near-neutral postoperative C2T and minimizing residual coronal imbalance should be prioritized intraoperatively. Failure to achieve these global balance targets may expose distal fixation points to sustained mechanical stress, even in the presence of otherwise robust constructs.
Illustrative Case
To illustrate these principles, we present the case of a 73-year-old male with history of global sagittal and coronal imbalance (C2T = 17°, C7-CSVL = 2 cm) (Figure 3A). The patient underwent a T4-pelvis posterior spinal fusion with an L5 pedicle subtraction osteotomy (PSO) and bilateral pelvic fixation with SI- Bone granite screws. Six weeks postoperatively, the patient’s residual C2T was 7° and his ΔC7-CSVL was 0.2 cm (Figure 3B). He subsequently presented with disengagement of the posterior rods at S1 and his pelvic screws as well as loss of correction at the L5 PSO site (Figure 3C and D). Revision surgery from L4-pelvis was performed. Upsized and 2 additional SI-Bone screws were used to obtain dual bilateral pelvic fixation. Postoperatively, the patient’s C2T (7°) demonstrated sustained residual global sagittal malalignment with a forward flexion moment in the upper thoracic spine, creating distal biomechanical stress (Figure 3E). Radiographs obtained 6-month after revision demonstrated new bilateral rod fractures at L5 (Figure 3F). This case example highlights the role of global sagittal balance as a driver for acute PFF, underscoring the need for adequate intraoperative global balance correction. Preoperative (A) and immediate postoperative (B) radiographs demonstrating T4 topelvis fusion and correction of sagittal imbalance with a ΔC2T of -7°. Six-week postoperative radiographs (C) demonstrating catastrophic PFF and complete disengagement of bilateral rods from pelvic screw sites with a severe positive global sagittal malalignment. Associated CT scan (D) redemonstrating distal fixation failure 6 weeks postoperatively. Six-week postoperative radiographs (E) demonstrating revision of distal failure with new quad pelvic fixation. 6-month postoperative radiographs (F) demonstrating secondary failure with new bilateral vertical rod fractures at L5
Pseudoarthrosis
Although pseudoarthrosis accounted for a minority of failures in this series, it is important to recognize that these failures potentially represent a distinct biological failure mechanism compared with purely mechanical failures such as screw loosening or rod fracture. Pseudoarthrosis at the lumbosacral or pelvic fixation site reflects failure of bone fusion despite instrumentation, resulting in persistent motion across the junction that may lead to implant fatigue or loosening. This process is strongly influenced by biological and host-related factors, including smoking status, BMI, and fusion length.22,23
In contrast, mechanical failures such as rod fracture or screw loosening are more commonly attributable to excessive mechanical strain on an intact construct. These failures are influenced by construct-related factors such as magnitude of deformity correction, residual malalignment, and number of rods crossing the lumbopelvic junction. 66,7 Importantly, these mechanisms are not mutually exclusive, as pseudoarthrosis itself may lead to progressive implant loosening due to persistent motion at the fusion site.
Limitations
Given the retrospective nature of this study, our results have several limitations that are worth considering. Incomplete or missing radiographic and bone density data limited sample sizes. As a result, there is an increased risk of type II error for variables that did not reach statistical significance, and these findings should be interpreted with caution. Furthermore, our patients were from a single tertiary care center, limiting generalizability. Future studies should attempt to replicate our findings using a larger sample size from multiple institutions to account for potential differences in surgical management. Additionally, because PFF was defined based on reoperation, it may underappreciate asymptomatic cases of failure or cases where a patient chose not to undergo surgery. Moreover, when using propensity matching, there is always a risk of unmeasured confounding variables affecting observed associations despite appropriate matching scores. Additionally, due to data availability, only 1 year follow-up was feasible, but >2 year follow-up would be preferred in future studies to fully capture more subtle pelvic fixation failures.
Conclusions
In this matched control analysis, PFF occurred in 5.99% of ASD patients. Radiographically, decreased coronal correction and residual sagittal imbalance more than malalignment is more predictive of PFF. Specifically increased postoperative C2T and ΔC7-CSVL, were identified as independent predictors of PFF. Time-to-event analysis highlighted a faster rate of failure with increasing residual imbalance. Lower femoral neck bone density was also identified as a predictor of PFF, suggesting a multifactorial etiology of mechanical and biological predictors. These findings provide further clarity regarding postoperative balance thresholds and preoperative risk profiles that may predispose patients to a greater likelihood of PFF.
Supplemental Material
Supplemental Material - The Impact of Global Imbalance on Pelvic Fixation Failure: A Single Institution Matched Case-Control Study
Supplemental Material for The Impact of Global Imbalance on Pelvic Fixation Failure: A Single Institution Matched Case-Control Study by Karan Joseph, Samuel Vogl, Jeffrey T. Galla, Alexander T. Yahanda, Vivek P. Gupta, Salim Yakdan, Miguel A. Ruiz-Cardozo, Benjamin Plog, Tim Bui, Noah D. Poulin, Sundeep Chakladar, Francisco Narro-Garcia, Jason Ng, Matthew Wang, Braeden Benedict, Samuel Brehm, Hana Hallak, Karma Barot, Nicholas Pallotta, Munish C. Gupta, Brian J. Neuman, Jacob K. Greenberg, Wilson Z. Ray, Camilo A. Molina in Global Spine Journal.
Footnotes
Acknowledgments
We extend our gratitude to the Washington University School of Medicine in St. Louis Neurosurgery Department for their support and encouragement throughout this project.
ORCID iDs
Consent to Participate
Given the retrospective design of this study, informed consent was waived.
Author Contributions
Conception and design: KJ & CM; Acquisition of Data: KJ, SV, JTG, ATY, MRC, TB, NDP, SC, FNG, JN, MW, BB, SB; Analysis and interpretation of data: KJ, SV, JTG, CM; Drafting the article: KJ, SV, JTG; Critically revising the article: KJ, AY, VP, SY, MRC, BP, TB, HH, KB, NP, MG, BN, JKG, WZR, CM; Project Supervision: CM. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
This study was approved by Washington University School of Medicine in St. Louis Institutional Review Board (202302010).
Data Availability Statement
The data used for this study were obtained from electronic medical records from Barnes-Jewish Hospital (St. Louis, MO) and contain protected health information. Due to institutional policies and patient confidentiality regulations, this data is not publicly available. Data access is restricted to approved researchers in compliance with ethical and regulatory requirements. Please contact Washington University’s Institutional Review Board for further information on data access.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.