
Abstract
Study Design:
This was a prospective cohort study.
Objectives:
To introduce the iliac connectors as fixation options in spinal constructs used for correction of severe scoliosis at locations other than the lumbopelvic region.
Methods:
Nine patients with severe rigid scoliosis undergoing surgical release and posterior instrumentation in the period between January 2013 and January 2015 were included in this prospective cohort study. Mean age was 18.4 years; 8 had triple structural curves, and the remaining patient had double structural curves. Cobb angles of the primary and compensatory curves were compared with the immediate, 1-year, and 2-year postoperative measurements using the F test, with P value ≤.05 indicating statistical significance. Screw densities of the final constructs were calculated and compared with the screw densities when the offset iliac connectors were not used.
Results:
One to 4 offset iliac connectors were used in all 9 patients, increasing screw density by a mean of 6.24 (P < .001). The mean Cobb angle of the major curve was corrected from 98.44° to 58.2° (P < .001), that of the first compensatory curve, from 56.55° to 38.33° (P < .001), and that of the second compensatory curve, from 40.75° to 26.63° (P < .001). There were no intraoperative neurological complications. After a mean follow-up of 30.6 months, the construct remained stable in all patients with no loss of correction.
Conclusion:
Offset iliac connectors can be a valuable tool to increase screw density in correction of severe scoliosis, thus increasing overall biomechanical strength of the final construct.
Background
Segmental pedicle screw constructs or hybrid constructs using pedicle screws, hooks, wires, or cables are the current trends for posterior instrumentation anchoring options. Since their introduction by Boucher, 1 the segmental thoracic pedicle screws gained popularity by Suk and are currently considered the gold standard for scoliosis surgery. It is common in severe neglected scoliosis, to have residual massive lateral transitory apical shift in spite of maximum possible release. In such conditions, the rods must be severely bent to accommodate the residual curvatures. The ultimate result of correction is a compromise between the rigidity of the scoliosis and the corrective forces provided by these methods. From the biomechanical point of view, excessive bending of the rods weakens them. 2,3 Also, too much bending of the rod particularly at the concave side of the curve, displaces it away from the midline. This results in additional bending stresses on the rod in the axially loaded spine. In addition, scoliosis surgeons are sometimes confronted with difficulties in rod screw assembly that can end by removal of one or more screws because the polyaxial screws cannot alone compensate for the malalignment present between the heads of the screws.
Despite the growing biomechanical data simulating curve correction with variable implant density suggesting that a minimum density screw pattern may result in a comparable outcome as found with a high-density construct, none of these studies was performed on severe or rigid curves. 4 -6 In addition, reduction of the implant density also means that the load exerted on each anchor point is increased. 7 The end result is often a lower-density instrumentation with subsequent construct failure in such cases of severe and rigid scoliotic curves.
The use of long iliac screws with a 90° offset connector between the iliac screw and the rod avoids complex lumbopelvic 3-dimensional rod bends. 8 To the best of our knowledge, this is the first report on the use of the offset iliac connectors in scoliosis surgery at locations other than the lumbopelvic region.
Methods
Nine patients with severe rigid scoliosis were included in this prospective study after institutional review board approval. All patients were treated at our institute in the period between January 2013 and January 2015 at Alexandria University Hospital, Egypt. All patients were examined clinically and radiologically. Prior to surgery, plain radiographs of whole spine standing and bending views were obtained. Only patients with no significant deformity correction in the bending views were included.
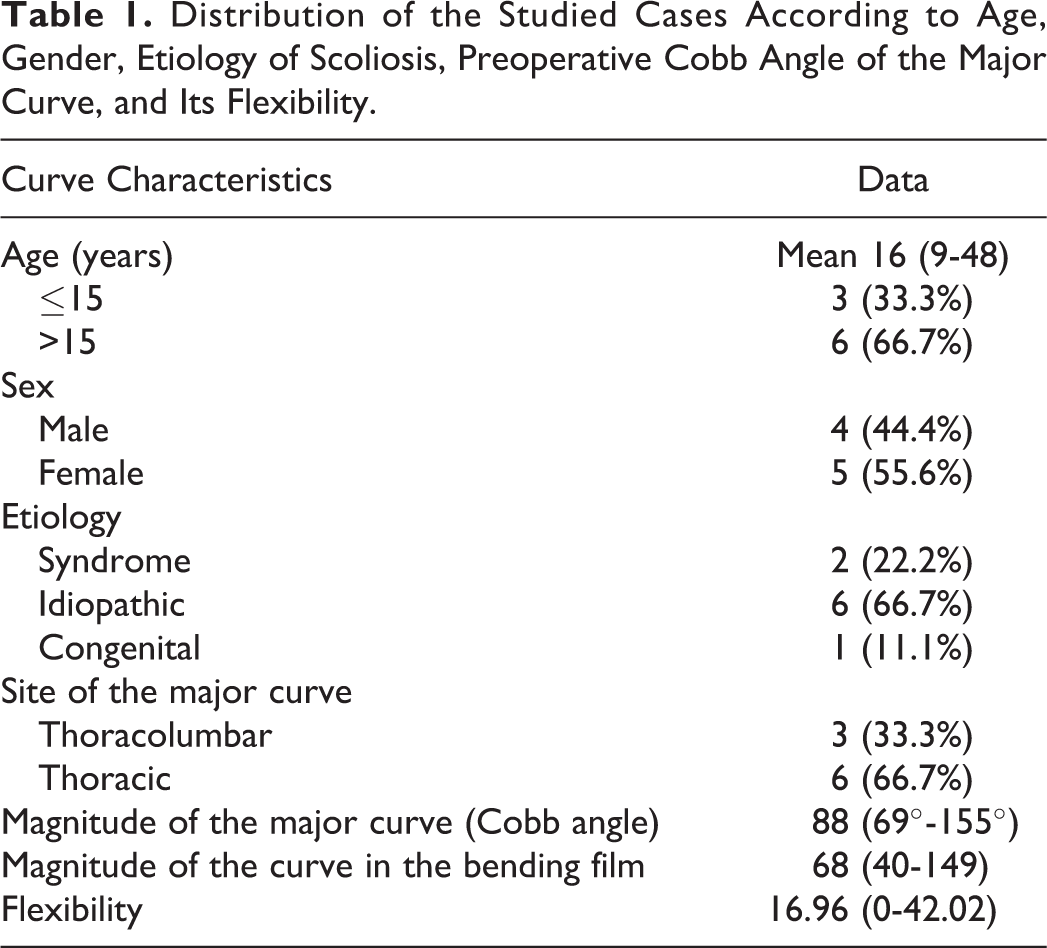
Five patients were female, and 4 were male. The age of the patients at the time of surgery ranged between 9 and 48 years, with a mean of 18.4 and SD of 11.7. The scoliosis was idiopathic in 6 patients (66.67%), syndromic in 2 (22.22%), and congenital in the remaining patient (11.11%). Two of them had undergone previous spinal surgeries. All patients had triple structural curves except for 1 patient who had double structural major curves. The major curve was thoracic in 6 patients (66.67%) and thoracolumbar in the remaining 3 patients (33.33%). The Cobb angle of the major curve ranged between 69° and 159° (mean: 98.44; SD: 30.75). The flexibility of the major curve ranged between 0 and 42.02 (mean: 16.91; SD: 12.96). Primary curve characteristics are given in Table 1.
Distribution of the Studied Cases According to Age, Gender, Etiology of Scoliosis, Preoperative Cobb Angle of the Major Curve, and Its Flexibility.
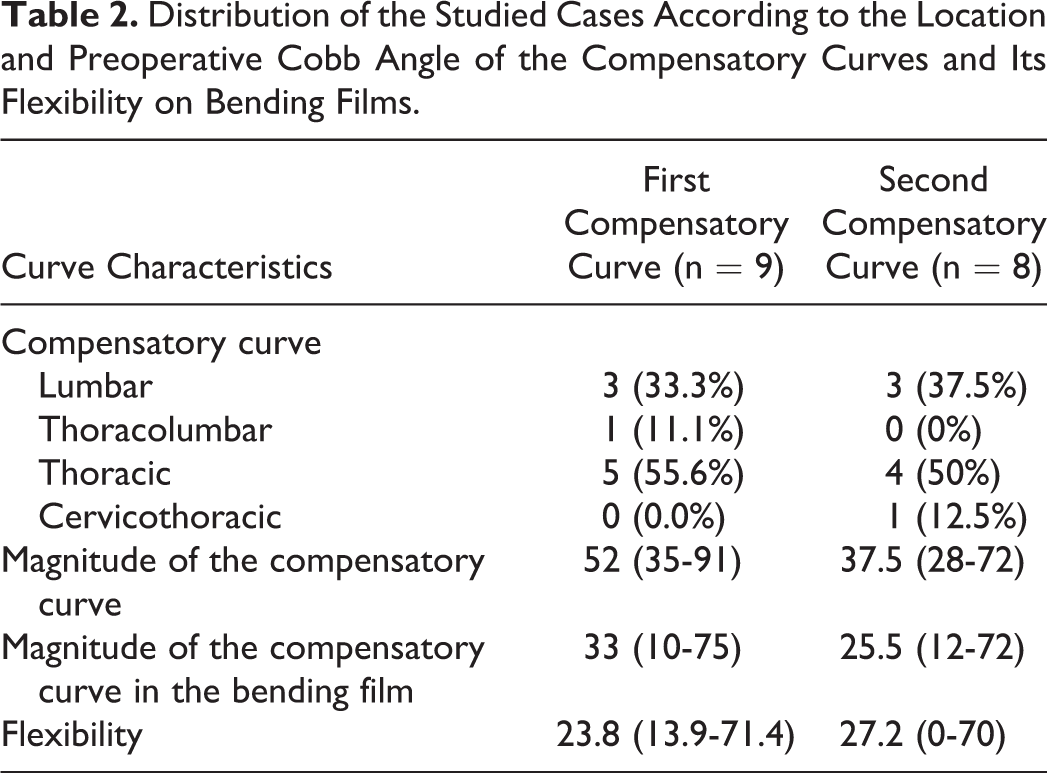
The first compensatory curve was thoracic in 5 patients (55.56%), thoracolumbar in 3 (33.33%), and lumbar in the remaining one (11.11%). The Cobb angle of the first compensatory curve ranged between 39° and 72° (mean: 56.55; SD: 20.13). The flexibility of the first compensatory curve ranged between 13.88 and 71.42 (mean: 32.38; SD: 21.16). As for the second compensatory curve, the Cobb angle ranged between 28° and 72° (mean: 40.75; SD: 13.47). The flexibility of the second compensatory curve ranged between 0 and 70 (mean: 32.25; SD: 24.26). Compensatory curve characteristics are shown in Table 2.
Distribution of the Studied Cases According to the Location and Preoperative Cobb Angle of the Compensatory Curves and Its Flexibility on Bending Films.
Preoperative height ranged between 132 and 173 cm (mean: 153; SD: 15.07). All patients were monitored intraoperatively using motor-evoked potentials (MEPs). The follow-up period ranged between 24 and 38 months (mean: 30.6; SD: 4.8). Sagittal profile measured between D5 and D12 levels was unmeasurable in 4 patients and measurable in the remaining 5 patients. It ranged between 12° and 35°, with a mean of 24.2°. Sagittal profile measured between D12 and S1 levels ranged between 35° and 71° with a mean of 44.8°.
All surgeries were performed by the senior author (HES) after obtaining an informed written consent for surgery as well as for publication purposes and inclusion of images. A standard posterior midline incision was made and exposed to the tip of the transverse processes bilaterally, staying strictly subperiosteal to reduce bleeding. The usual correction maneuvers of the scoliosis were performed. 9 -16 In those patients in whom the apical screws could not be included in the construct without extensive rod bending, an iliac offset connector was used to connect the apical screws to one of the rods. This allowed inclusion of apical screws in the construct, thus increasing screw density without excessive rod bending or contouring. The implant density was defined as the number of fixation screws divided by the number of available anchor sites within the main curve. 15
Postoperatively, all patients were mobilized on the second postoperative day, and control radiographs were performed. Patients were followed up at 3 months and 6 months, and then yearly both clinically and radiologically for at least 2 years postoperatively.
Postoperative measurements of the major curve and first compensatory and second compensatory curves were obtained immediately postoperatively and at 1 year and 2 years postoperatively. SPSS (IBM Corp, Released 2013, IBM SPSS Statistics for Windows, Version 21.0, Armonk, NY) was used for all statistical analyses. The preoperative Cobb angles of the primary curves and compensatory curves were compared with the immediate and 1- and 2-year postoperative measurements using the F test (ANOVA) with repeated measures, with P value ≤.05 indicative of statistical significance.
Screw densities of the final constructs were calculated and compared with the screw densities when the offset iliac connectors were not used in the constructs.
Screw density = Number of screws/(Number of instrumented levels × 2).
Results
The intraoperative blood loss ranged between 750 and 3500 mL (mean: 1905.5; SD: 897.3), whereas the operative time ranged from 180 to 620 minutes (mean: 276.6; SD: 133.7). There were no intraoperative neurological deficits and no patient with pseudoarthrosis. One patient had metal failure without any consequences.
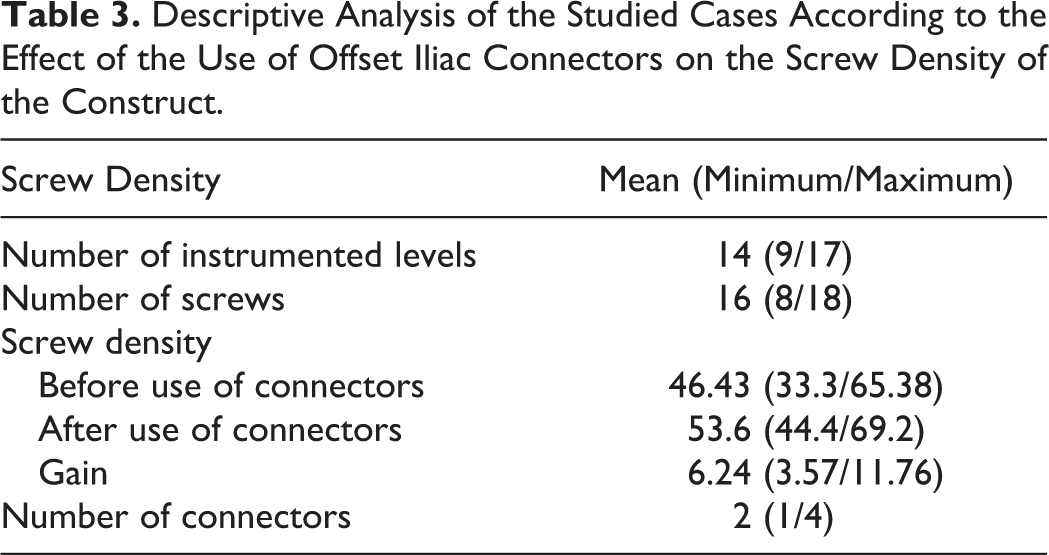
Table 3 shows the effect of using the offset iliac connectors on the final screw density of the construct. Four iliac offset connectors were used in 1 patient (11.1%), 2 iliac offset connectors were used in 4 other patients (44.4%), and 1 iliac connector was used in the remaining 4 of 9 patients (44.4%). This extra use of iliac offset connectors significantly increased both the number of instrumented levels and the screw density, with a mean increase in screw density of 6.24 (P < .001). The screw density after the use of offset iliac connectors was 53.6 as compared with 46.43 if these connectors were not used. The benefit of this significant increase in the screw density owing to this technique is in terms of more biomechanical stability to the construct in addition to the other advantage of avoiding severe rod bending to accommodate such severe and rigid scoliotic curves (Figures 1 –6).
Descriptive Analysis of the Studied Cases According to the Effect of the Use of Offset Iliac Connectors on the Screw Density of the Construct.
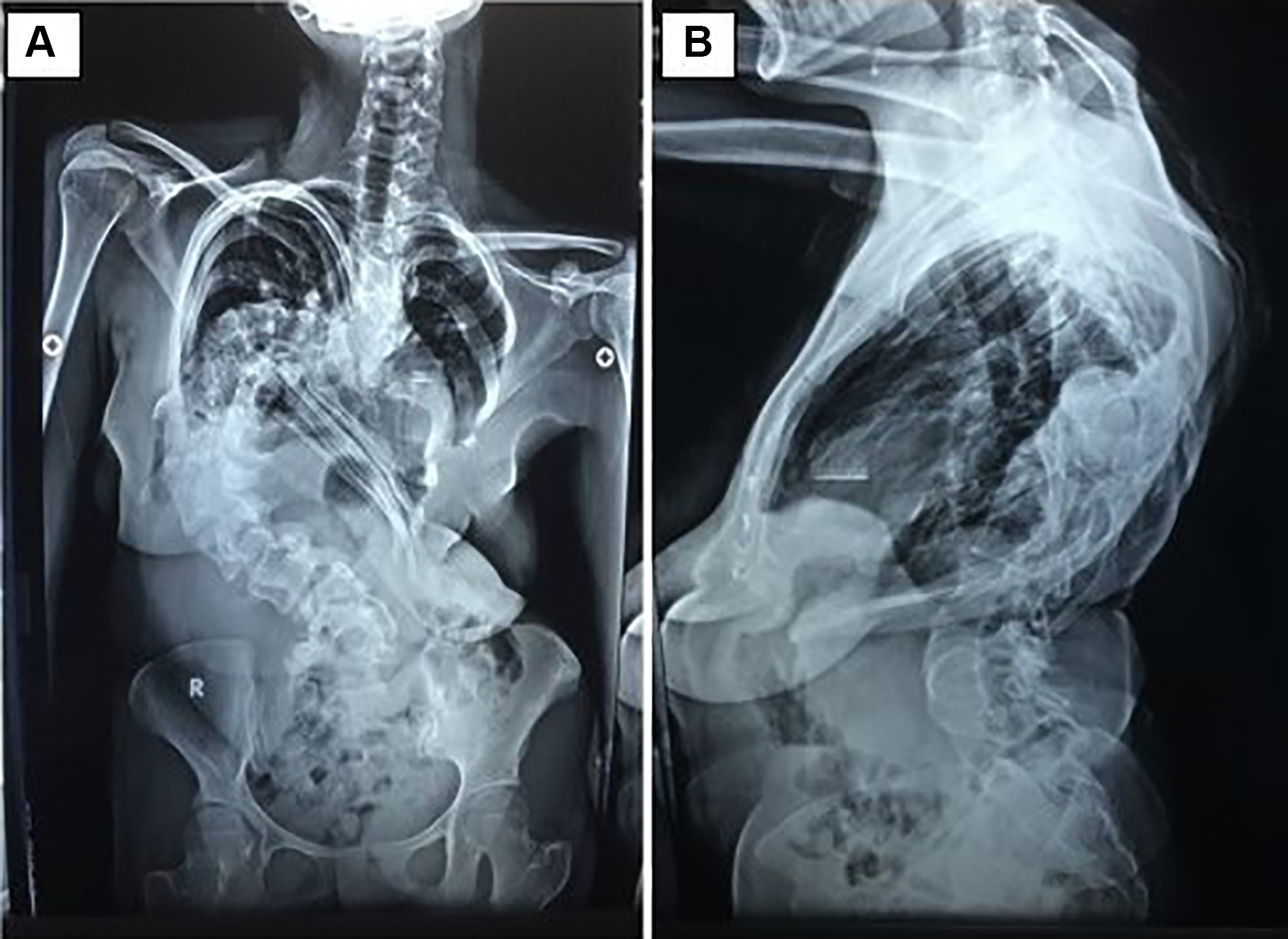
Anteroposterior (A) and lateral (B) radiographs of a syndromic scoliosis with a major thoracic curve in a 20-year-old woman. Note the severity of the curve in the coronal plane (Cobb angle 155°) and the immeasurability of the saggital profile because of nonidentification of the end plates.
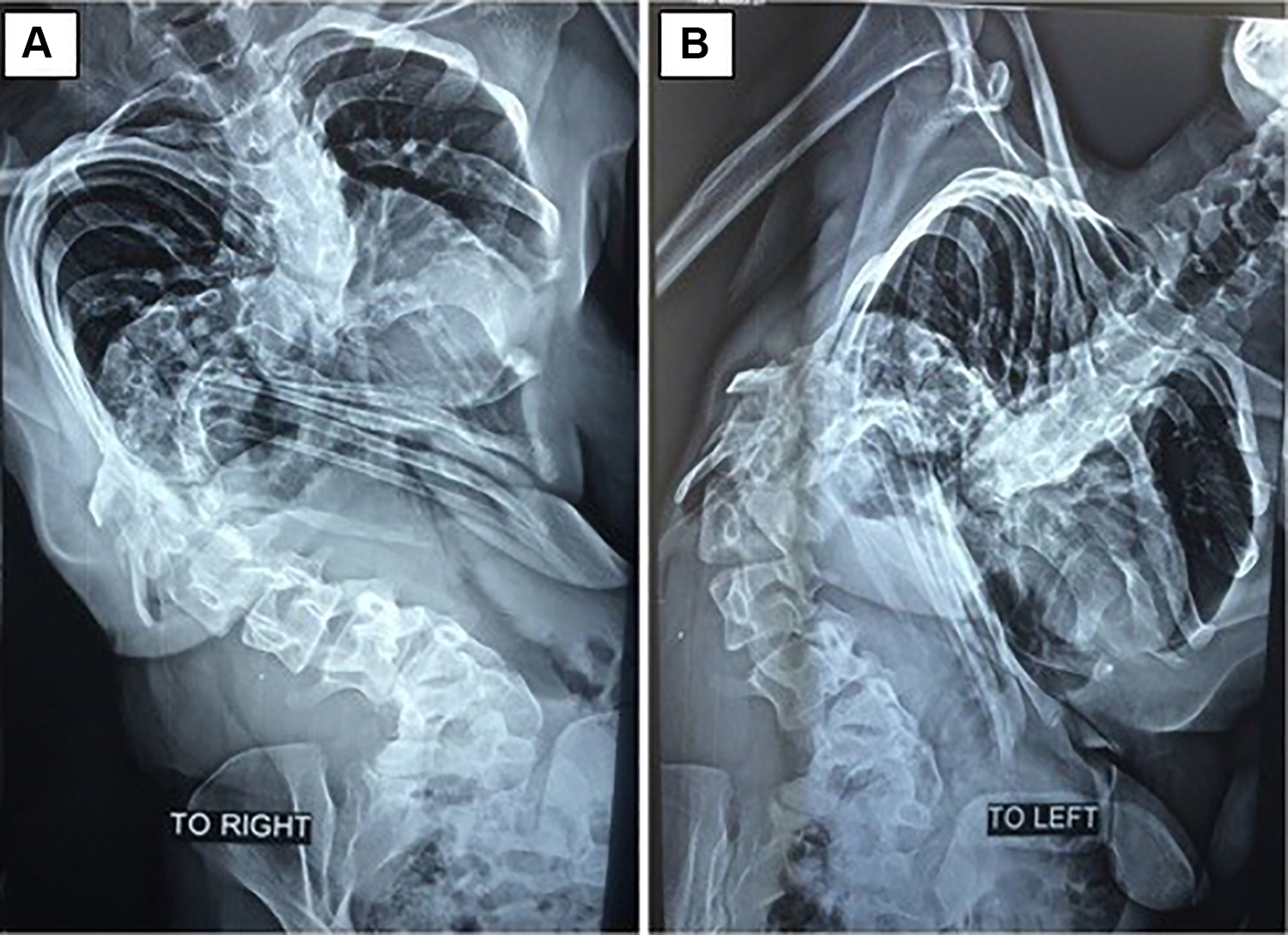
Bending films of the same patient to the right (A) and to the left (B). Magnitude of the primary curve in the bending film is 149° (flexibility 3.87); magnitude of the first compensatory curve in bending is 62° (flexibility 13.88) and that of the second compensatory curve, 72° (flexibility 0).
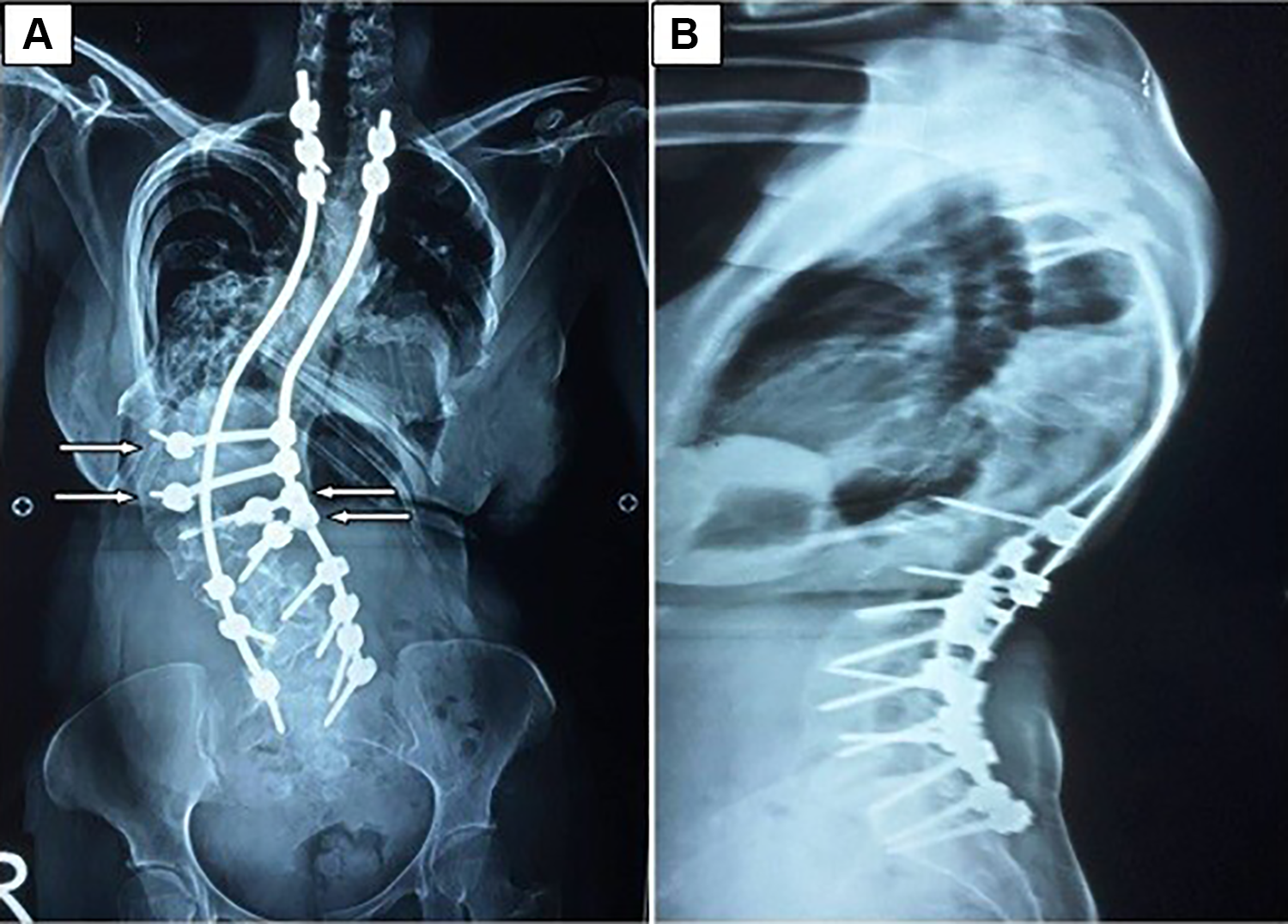
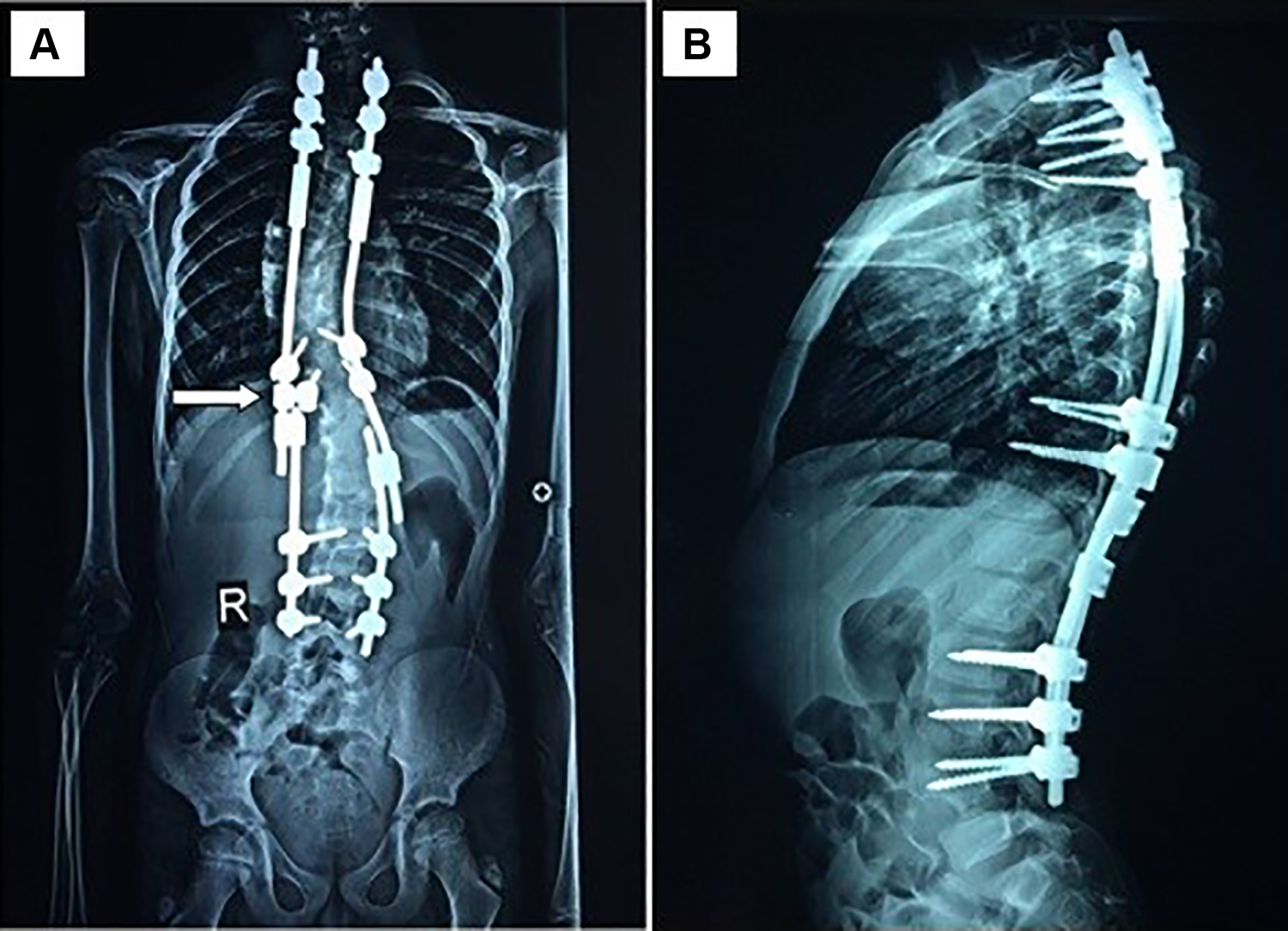
Anteroposterior (A) and lateral (B) 3-year postoperative radiographs. Cobb angle, after 2 years of follow-up, of the major curve is 118°, of the first compensatory curve is 45°, and of the second compensatory curve is 54°. Note the use of 4 offset iliac connectors (white arrows) as anchoring points, allowing for the use of 4 more pedicular screws and increasing the screw density subsequently without excessive rod bending.
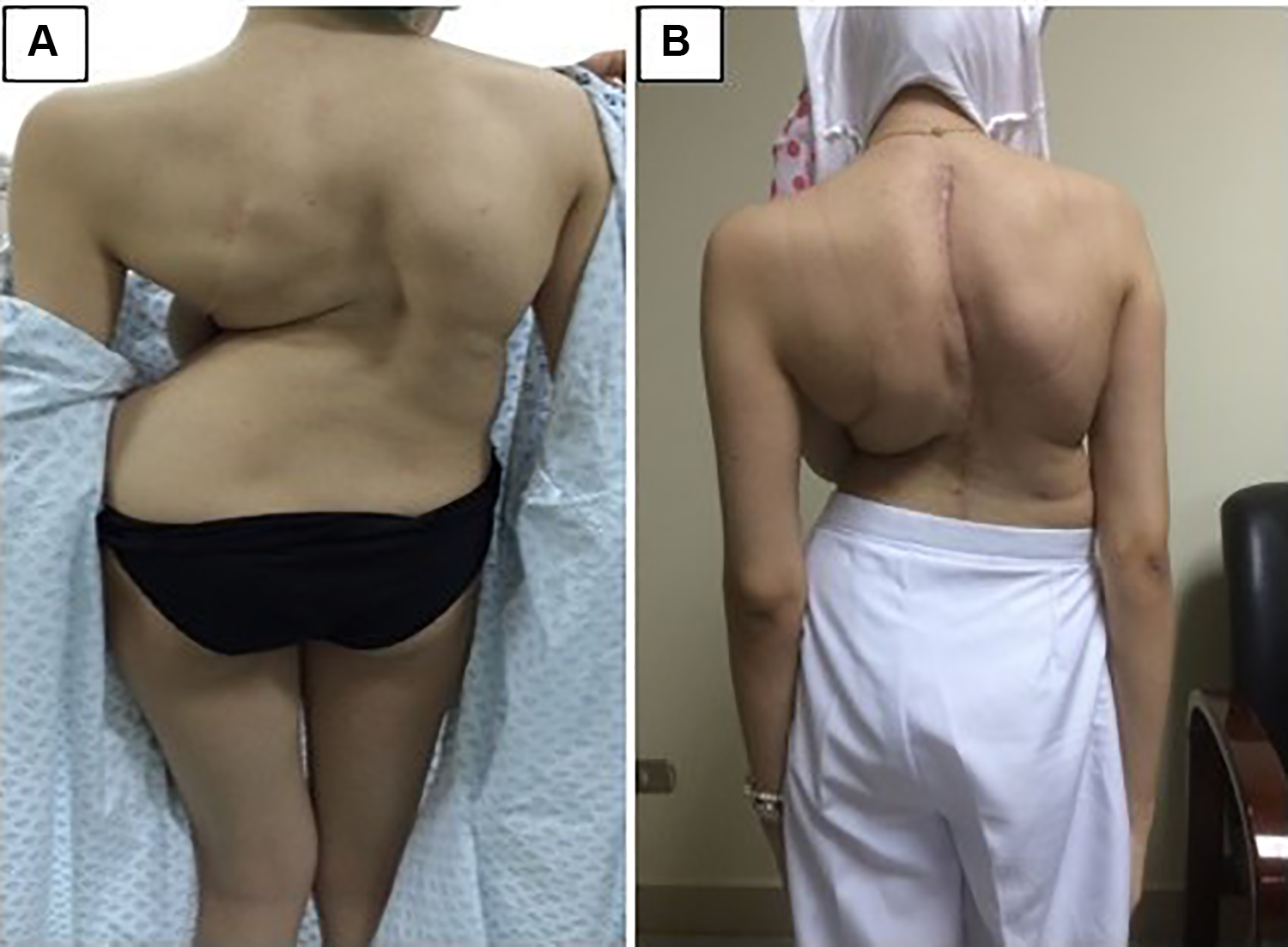
Preoperative photograph of the patient (A) and a postoperative photograph (B). The preoperative height was 151 cm, and the postoperative height was 155 (with 4 cm gain in height). There were no intraoperative neurological deficits.
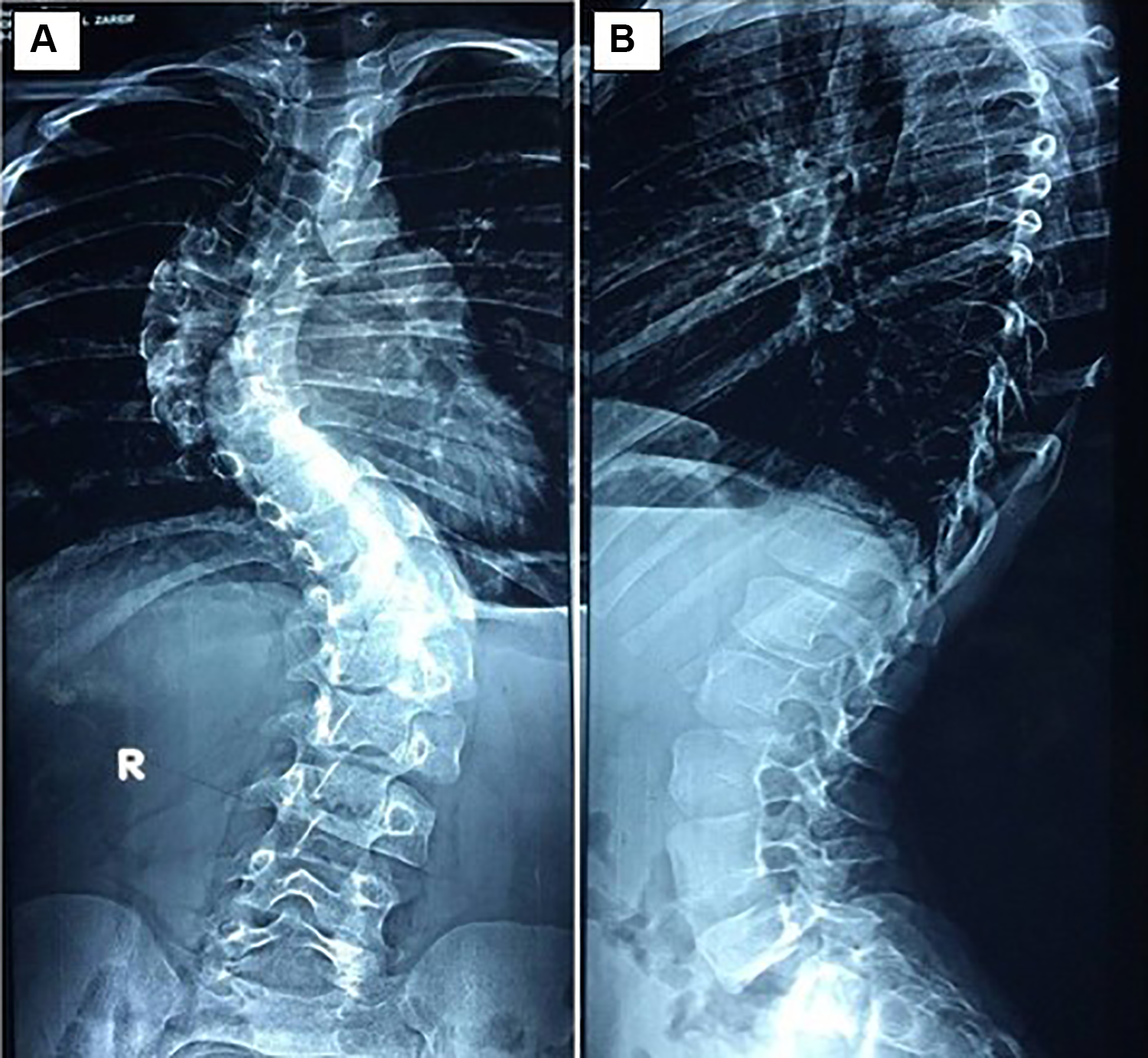
Preoperative anteroposterior (A) and lateral (B) radiographs of a 9-year-old man with thoracic idiopathic scoliosis. The primary curve Cobb angle was 69° in the coronal profile while being 28° in the D5 to D12 sagittal profile and 42° in the D12 to S1 sagittal profile. The first compensatory curve was thoracic and had a magnitude of 52°, whereas the second compensatory curve was also thoracic and had a magnitude of 35°. Plumb line showed no deviation, and both the shoulders and pelvis were symmetrical.
A 30-month postoperative radiograph showing anteroposterior (A) and lateral (B) views. The number of instrumented levels is 16 and with 16 screws. Note the use of 1 iliac offset connector in a growing double-rod technique (white arrow). The Cobb angle of the major curve at the end of the follow-up was 32°, of the first compensatory curve, 31°, and of the second compensatory curve, 25°. There was a 4-cm gain in height from a preoperative height of 132 cm.
The Cobb angle of the major curve was significantly corrected from a mean of 98.44° to 58.2° at 2 years postoperatively (P < .001). Both the first compensatory curves and the second compensatory curves significantly corrected from a mean of 56.55° to 38.33° and from a mean of 40.75° to 26.63°,respectively (P < .001). During the 2 years of follow-up, no significant loss of correction was noted in comparison to the immediate postoperative period, as shown in Table 4.
Descriptive Analysis of the Studied Cases According to the Cobb Angle of the Major Curve, and First and Second Compensatory Curves With Comparison Between Preoperative and Postoperative Measurements.

Standing height was restored by a mean of 3.78 ± 0.67 cm postoperatively. Plumb line, shoulder level, and pelvic symmetry were all significantly clinically and radiologically improved. Preoperative plumb line was neutral in 1 case and deviated to one side in the remaining 8 cases. It was deviated to the left in 5 cases, with a mean of 4.4 cm, and deviated to the right in 3 cases, with a mean of 6 cm. On comparison to preoperative measurements, the plumb line neutralized in 4 cases; deviated to the left in 3 cases, with a mean of 3 cm; and deviated to the right in 2 cases, with a mean of 2 cm.
The preoperative pelvic tilt was neutral in 3 cases; the left hemipelvis was higher in 4 cases, with a mean of 2.5 cm, and the right hemipelvis was higher in 2 cases, with a mean of 2 cm. The postoperative pelvic tilt was neutral in 5 cases; the left hemipelvis was higher in 3 cases, with a mean of 2 cm, and the right was higher in 1 case, with only 1 cm.
The preoperative shoulder level was neutral in only 1 case; the left shoulder was higher in 3 cases, with a mean of 3 cm, and the right shoulder was higher in 5 cases, with a mean of 3.2 cm. Postoperatively, the shoulder level was neutral in 2 cases; the left was higher in 4 cases, with a mean of 1.25 cm, and the right was higher in 3 cases, with a mean of 2.3 cm.
Discussion
It is not rare in surgery for correction of severe scoliosis to excessively bend the rods and/or to remove one or more properly placed screws because of failure of the polyaxial screws to solve a malalignment present between the heads of the inserted screws. The end result is often a low-density construct with subsequent metal failure. There is no data in the literature available on the efficacy of the iliac connectors as a tool decreasing the need for excessive bending of the rods and avoiding removal of a malaligned screw(s) in corrective surgery of spinal deformities of the dorsal and dorsolumbar spine.
The mechanical philosophy of the use of offset connectors is not new. Offset connectors have established their role in spinopelvic fixation. They provide modularity, avoiding complex lumbopelvic 3-dimensional rod bending. 8
van Royen et al 17 adopted a new spinopelvic fixation system in which iliac screws are side-to-side connected to the posterior thoracolumbar rod construct, independent of the angle between the rod and the iliac screw. They described 3 different cases where the open-angled parallel connectors are used to connect short iliac rods from the posterior rod construct to the iliac screws on both sides.
The use of the offset connectors in our technique for scoliosis correction surgery reduced the difficulties that would be encountered from a complicated 3-dimensional bending of the rods. It allowed a powerful anchorage at the periapical region, with its advantage in partial correction of the curve and achieving a strong construct.
Another important advantage is increasing the screw density and, thus, increasing the overall construct strength. 7 This was supported by many authors, such as Daher et al, 18 who concluded that in the surgical treatment of neuromuscular scoliosis, the correction of the curve increases as the implant density increases.
Similarly, Gotfryd and Avanzi 19 studied and compared 2 groups of 23 patients with adolescent idiopathic scoliosis who underwent surgeries with higher and lower implant densities. No statistically significant difference was observed in the radiological results, but greater correction of the rib cage was shown.
Garcia et al 20 conducted a biostatistical study that showed that the group with up to 50% screw density had a rate of correction of 82.1%, and the group with 100% density was corrected to around 86.8%. On the other hand, Bharucha et al 21 identified no clinical, radiographic, perioperative, or complication-related advantage of constructs with higher implant density patients with flexible idiopathic scoliosis. Cost was significantly higher in higher-density constructs. Despite that, he stated that optimal implant density should rely on a number of factors, including curve magnitude and rigidity, bone density, and desired correction. However, this study only evaluated flexible curves, so a comparison of results between groups with more severe curves and with patterns more complex than Lenke 1 could show differences in effectiveness between using low- and high-density implants.
Gebhart et al 22 conducted a retrospective study of 119 patients with adolescent idiopathic scoliosis (Lenke 1, 2, 3, 4, and 6). The correction of the principal thoracic curve was closely correlated with the flexibility of the curve and not with the density of the screws.
The biomechanical advantages of using iliac connectors in this technique can be summarized as follows: The use of offset iliac connectors increased the instrumentation density that is desirable in correction of severe scoliosis and for achieving a strong construct. It allowed correction of the curve without complex 3-dimensional bending of the rods, which is not only demanding, but also has the mechanical disadvantages of weakening the rod and rod placement on the concave side away from the midline. It allowed use of screws at the apex and periapical region, which is known to be the best for achieving correction and fixation of the curves.
10
In addition, the lateral offset connectors decreased the loads on the periapical screws, particularly the pull-out forces that would come into play if the rods were assembled directly into the heads of the screws.
Finally, spine surgeons who are acquainted with the use of offset connectors in spinopelvic fixation can readily adopt the same principle in severe scoliosis with massive uncorrectable apical or/and lateral transitory shift.
Nevertheless, biomechanical testing and long-term follow-up are needed for better assessment of the technique.
Conclusion
This study presented the preliminary results of a novel use of offset iliac connectors in correction of severe scoliotic curves, which significantly increased screw density in correction of severe and rigid scoliosis. However, the small sample size and lack of a comparison group for other correction techniques, such as convex pedicle screw, would warrant further studies to better validate our technique. Further randomized controlled trials with a larger sample size and comparison to other correction techniques are thus warranted. 23 In our experience, we have found that the implementation of this technique in scoliosis surgery is feasible and allows correction of severe scoliosis, which would otherwise require excessively bending the rods or removing one or more properly placed screws, leading to a lower screw density and, thus, a biomechanically inferior construct.
Footnotes
Authors’ Note
AB is the corresponding author and was involved in data collection, interpretation, and writing of the article. HES is the senior author and main surgeon for the cases described in the article. YEM was responsible for revising the article. All authors read and approved the final article. All procedures performed were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards, and ethical approval was obtained from the research ethics committee at our institute (Alexandria University Hospital, Egypt). Informed written consent was obtained from all individual participants included in the study as well as for publication purposes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.