
Abstract
Study Design
Retrospective cohort study.
Objective
To examine national and regional trends in preoperative patient optimization and surgical outcomes among patients undergoing posterior lumbar interbody fusion (PLIF) in the United States from 2011 to 2022.
Methods
Patients who underwent PLIF were identified in the PearlDiver Patient Claims Database using ICD-9, ICD-10 and CPT codes. Demographic characteristics, comorbidities, and postoperative outcomes were analyzed over 11 years and by U.S. region (Midwest, Northeast, South, West). Variables included age, body mass index, tobacco use, Charlson Comorbidity Index (CCI), opioid use, 30-day complications, 90-day readmissions, infection, and hospital length of stay (LOS). Statistical analysis was performed using R (α = 0.05).
Results
434 214 patients underwent PLIF from 2011 to 2022. Nationally, LOS, 30-day complication, and 90-day readmission worsened over time. Hospital LOS increased (P < .0001) and infection rate decreased for all regions (P < .001). The Northeast showed significant improvement, whereas the South, Midwest and West all had rising complications and readmissions. Patients in 2021-2022 were older, with more comorbidities, more likely to use tobacco, and had higher rates of overweight and obesity. Significant decreases were observed in preoperative opioid use (P < .0001).
Conclusions
Despite an emphasis on preoperative optimization and demonstrated reductions in preoperative opiate use, surgical outcomes including 30-day complications, 90-day readmissions, and length of stay increased in recent years. Worsening outcomes imply potential gaps in optimization efforts and regional outcome variability may suggest a need for region-specific preoperative optimization strategies.
Keywords
Introduction
In the past decade, presurgical optimization, implementation of enhanced recovery protocols, and technological advancements have received increasing attention to maximize outcomes, reduce adverse events, and improve efficiency of spine surgery. Successful institutions reported improved outcomes including shorter hospital length of stay and lower complication rates. 1 However, it remains unknown whether similar outcomes have been achieved on a national scale.
Risk factor modification is a high-priority topic in the spine literature. Common comorbidities and lifestyle risk factors such as malnutrition, dyslipidemia, hypertension, diabetes mellitus, and nicotine use are all correlated with increased readmission rates and mortality after spine surgery. 2 Preoperative risk factor mitigation has repeatedly been shown to improve outcomes after lumbar fusion surgery.3,4 Further evolution of preoperative patient optimization is the development and implementation of standardized enhanced recovery pathways for preoperative comorbidities (eg, nutritional status, BMI, bone health, diabetes mellitus, hypertension, smoking) which have been shown to improve patient outcomes while simultaneously reducing costs on the healthcare system.5–12
The volume of elective lumbar fusion procedures in the United States rose by 62.3% between 2004 and 2013. 13 Between 2001 and 2010, expenditure on admissions related to spine fusion rose from $13.3 billion to $49.9 billion, largely attributable to complications and readmissions. 14 Given the societal impact of lumbar fusion surgery, this study aims to provide an updated assessment of national surgical outcomes following lumbar fusion surgery, focusing on posterior lumbar interbody fusion (PLIF), a commonly performed fusion technique. Additionally, we aim to describe changes in the average patient profile of those undergoing lumbar fusion surgery as an assessment of the status of spine surgery patient optimization.
Materials and Methods
Data Source and Study Design
The PearlDiver Mariner Patient Claims Database (PearlDiver Technologies, Colorado Springs, CO) is a publicly available and Health-Insurance Portability and Accountability Act (HIPAA)-compliant national database with more than 170 million patient deidentified records from 2011-2022. Institutional review board approval was not required for this study. Claims data included all payer types including commercial, Medicare, Medicaid, government, and cash payers. Data were retrieved using Current Procedural Terminology (CPT) codes, International Classification of Diseases, Ninth and 10th Revision (ICD-9 and ICD-10) codes, and National Drug Codes.
Patients
PearlDiver was queried for patients, ages 18-85, who underwent PLIF surgery between 2011 and 2022. Deidentified patient data were retrieved using the following ICD (ICD-9-P-8108, ICD-10-P-0SG007J, ICD-10-P-0SG00AJ, ICD-10-P-0SG00JJ, ICD-10-P-0SG00KJ, ICD-10-P-0SG00ZJ) and CPT codes (22630, 22633).
Study Variables
Demographic patient data collected included age and sex. Patient risk factors abstracted were obesity classification (underweight (<18.5 kg/m2), healthy (18.5-24.9 kg/m2), overweight (25.0-29.9 kg/m2), obese (30.0 < 39.9 kg/m2), morbidly obese (≥40.0 mg/m2)), tobacco use in the preceding 365 days, opioid use in the preceding 90 days, and Charlson Comorbidity Index (CCI). Surgical outcomes collected included hospital length of stay (LOS), infection, 30-day complications, and 90-day all-cause hospital readmission. Length of stay analyses were derived from ICD-10 codes only. Data were collected in 2-year intervals between 2011 and 2022. Patients were grouped by U.S. Census regions (Midwest (MW), Northeast (NE), South, and West) for analysis. A complete list of states included in each region is available in Supplemental Table 1.
Statistical Analysis
All analyses were performed using the R-based statistical platform available within the PearlDiver database, 15 with a significance threshold of α = 0.05. Surgical outcomes were compared between 2011 and 2022 by region. Univariate analyses were performed to explore changes in patient surgical risk factors that may have influenced patterns in surgical outcomes. Categorical variables were reported as percentages, and between groups comparisons were made using Chi-squared analyses. Continuous variables were reported as mean ± standard deviation and compared by two-tailed T-tests. Kaplan-Meier survival curves were created to assess time to complication, readmission, and infection.
Results
There were 434 214 patients who underwent PLIF in the study period of 2011-2022. The total number of PLIF procedures increased over the 11-year period by 3%. PLIF were most performed in the South, accounting for approximately 41.1% of PLIFs in 2021-2022.
Surgical Outcomes
Hospital Length of Stay
Changes in Surgical Outcome Measures Between 2011-2012 and 2021-2022

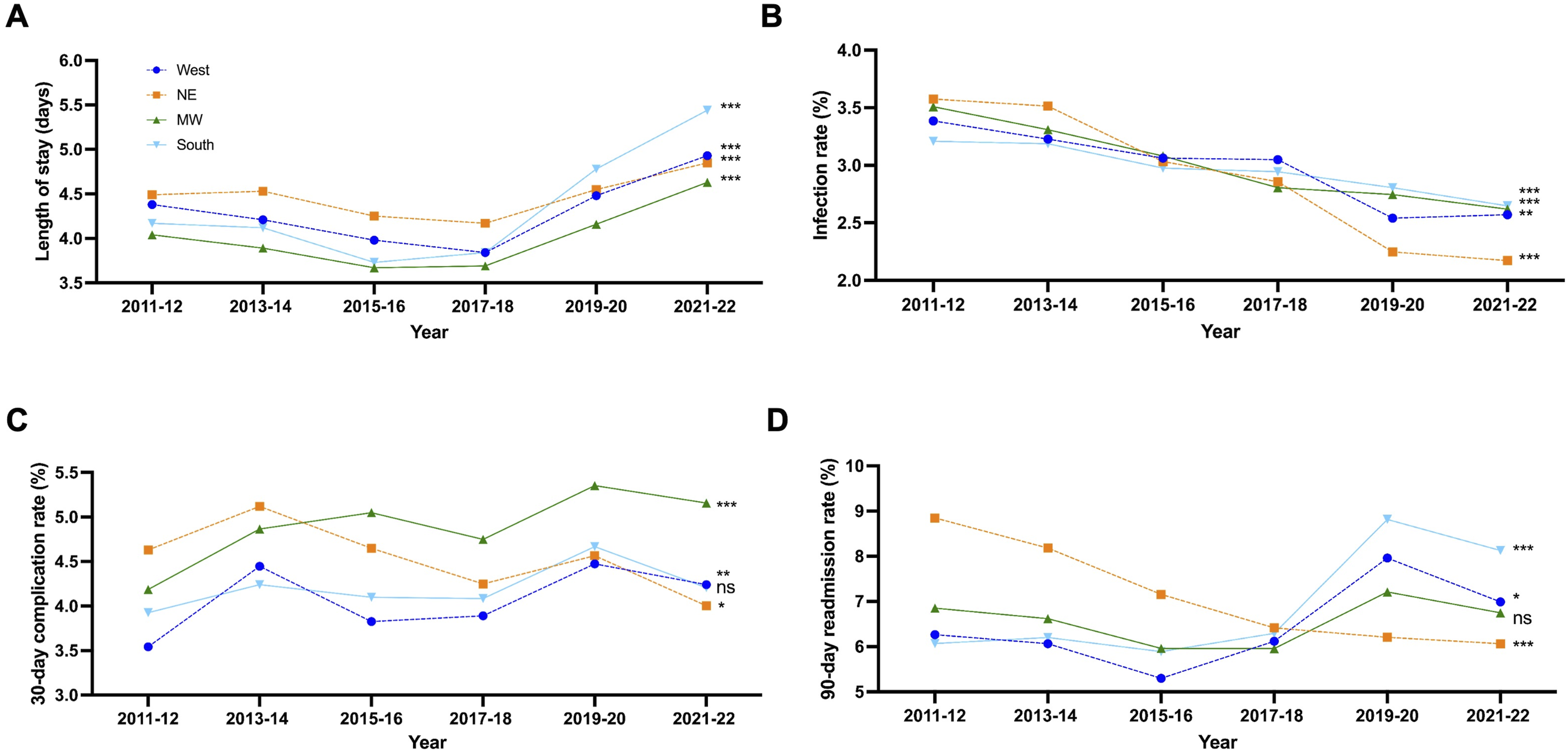
Regional variations in post-operative hospital LOS (A), infections (B), medical complications (C), and hospital readmissions (D) in the United States following PLIF performed between 2011 and 2022. Statistical analyses were performed comparing 2011-2012 and 2021-2022. ns: not significant, *P < .05, **P < .001, ***P < .0001
Infection Rate
Infection rates were comparable across regions and significantly decreased over the 11-year period (Table 1, Figure 1B). The NE experienced the greatest improvement in infection (3.5% vs 2.2%, x2 = 37.3, P < .0001). In the West, MW, and South, infection rates decreased from 3.4% to 2.6% (x2 = 12.253, P < .0005), 3.5% to 2.6% (x2 = 26.478, P < .0001), and 3.2% to 2.6% (x2 = 16.761, P < .0001), respectively.
30-Day Complications
Nationally, there was a significant 11% increase in the odds of 30-day complication (OR 1.11, 95% CI 1.05-1.16, P < .0001) (Table 1). Regionally, 30-day complication rates rose from 2011-2012 to 2021-2022 in the West (3.5% vs 4.2%, x2 = 7.30, P = .0069) and MW (4.2% vs 5.2%, x2 = 20.937; P < .0001). The NE experienced a decrease in complication rate (4.6% vs 4.0%, x2 = 4.952, P = .026). There was no change in complication rate in the South (Figure 1C).
90-Day Readmissions
Nationally, the rate of 90-day readmissions increased from 2011 to 2022 (OR 1.08, 95% CI 1.14-1.23, P < .0001) (Table 1). However, these rates varied regionally. The South and West experienced significant increases in 90-day readmission rate over 11 years (6.1% vs 8.1%, x2 = 97.874, P < .0001 and 6.3% vs 7.0%, x2 = 4.786, P = .0287, respectively) (Figure 1D). There was no difference in readmission rate in the MW (6.9% vs 6.7%, x2 = 0.178, P = .67) from 2011 to 2022 (P = .64). In the NE, 90-day readmission rate decreased over the study period (8.8% vs 6.1%, x2 = 59.224, P < .0001).
Surgical Risk Factors
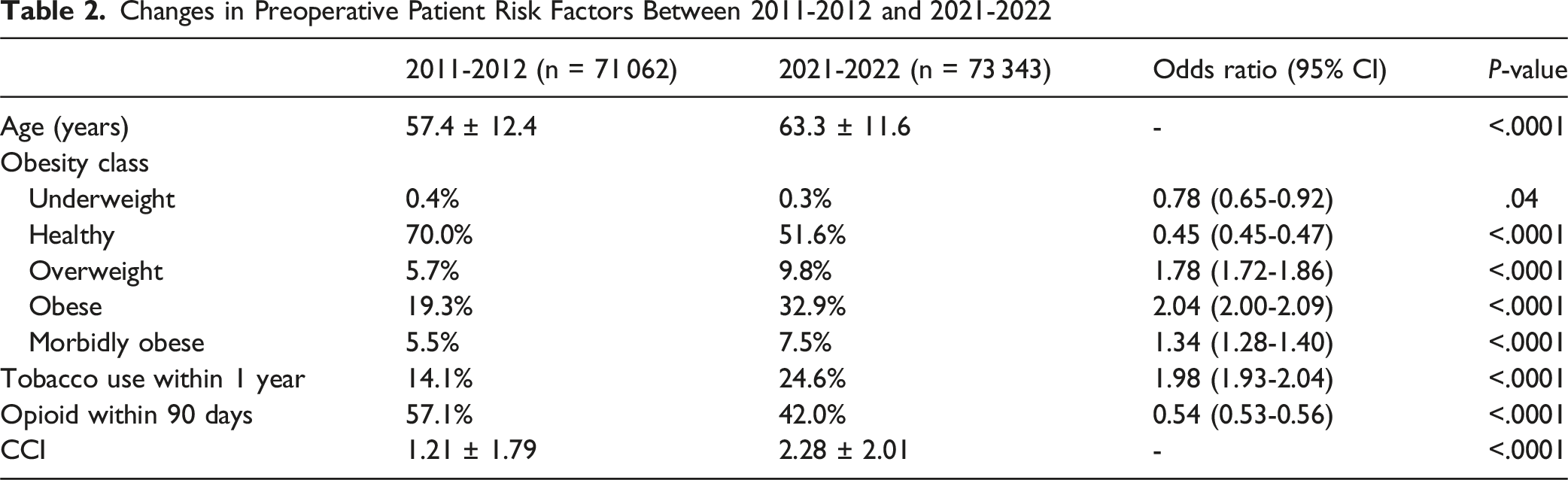
Changes in Preoperative Patient Risk Factors Between 2011-2012 and 2021-2022
Surgical outcomes were stratified by obesity classification. Patients classified as normal BMI had longer times to infection, complication and readmission. At 120 days, a greater proportion of morbidly obese (n = 30 484) patients developed postoperative infection (Figure 2A). Those in classified as underweight (n = 1578) experienced quickest time to complication and readmission (Figure 2B,C). Right-censored Kaplan-Meier curves, stratified by obesity classification, depicting infection-free (A), complication-free (B), and readmission-free survival (C) after PLIF
Discussion
This study is the first to assess both national and regional surgical outcomes after PLIF. Over the 11-year period examined in our study, there was significant worsening of three major postoperative outcome measures – hospital LOS, 30-day complication rate, and 90-day readmission rate – despite an improvement in infection rate. Our study found patients undergoing PLIF in 2021-2022 were significantly older, had a greater comorbidity burden, proportion of obese and morbidly obese, and tobacco use when compared to 2011-2012. These findings are overall unexpected in the context of increased preoperative optimization efforts,16,17 which are generally intended to enhance postoperative metrics.
There is growing literature demonstrating the benefit of preoperative optimization focused on key risk factors: smoking, nutrition, BMI, preoperative anemia, diabetes, alcohol, bone health, opioid use and psychiatric comorbidities. 16 Enhanced recovery pathways that utilize preoperative optimization protocols have shown notable improvement in outcomes. 1 However, these studies were largely conducted at academic centers which perform a fraction of total spine surgeries in the United States. Our results reflect the practice of all spine surgeons nationally, both private and academic, and suggest that overall many outcomes are worsening. This suggests that despite demonstrated success at an institutional level, the adoption and implementation of preoperative optimization pathways may not have successfully translated nationwide.
The reduction in infection rate nationally poses an interesting question – what is the reason for rising complication and readmission rates, in the setting of fewer infections? Across all regions, infection rates declined over time – a testament to widespread acknowledgement of the importance of operating room and perioperative sterility. Notably, this reduction occurred despite an overall increase in postoperative complications, readmission and hospital length of stay, suggesting that infections were not the primary driver of worsening outcomes. This discrepancy implies that other complication types are contributing disproportionately to the observed trends. Some considerations include deep venous thrombosis or pulmonary embolism, wound dehiscence, or other complications related to unoptimized comorbidities in an aging surgical population with high comorbidity burden. Although reoperation was not studied as its own outcome, hardware failure in the setting of rising obesity and tobacco use may also contribute. An increasing number of spinal deformity surgery/long segment fusions are performed which carries greater complication risk profile compared to short segment fusions. Finally, in 2017 laws meant to curb opiate use were passed which coincide with rising readmission rates. This could reflect provider reluctance to prescribe necessary postoperative opioid dosing in the setting of the opioid crisis. Given the regional variability in complication and readmission trends, this question might be better answered at the regional or institutional level. Further analysis with increased granularity is warranted to better characterize the specific complications responsible for the increase in adverse outcomes.
Age and Medical Complexity
We found that the mean age increased from 57.4 years in 2011-2012 to 63.3 years in 2021-2022, consistent with prior literature which noted increasing mean age from 51.2 years in 2006 to 60.6 years in 2016. 18 Several studies have shown a correlation between increasing age and incidence of complications after spine surgery.19,20 While age itself is not a modifiable risk factor, age is strongly associated with other modifiable factors affecting health in the elderly. 24
In addition to increasing age over time, mean CCI increased from 2011-2012 to 2021-2022. The CCI is a score developed to predict 10-year survival based on comorbidity burden. It is a collection of 17 comorbidity variables (eg, age, myocardial infarction, congestive heart failure, diabetes mellitus, moderate to severe chronic kidney disease, cancer/tumor). These data suggest that patients undergoing PLIF surgery are older with greater comorbidity burden, thus raising the complexity of performing surgery. 21
BMI/Obesity
We found that the proportion of overweight, obese, and even morbidly obese patients undergoing surgery increased over time. Obesity, defined as BMI >35, is associated with increased morbidity, greater blood loss, prolonged procedures, increased complications (including wound complications), poor satisfaction with spine surgery, early complications in revision surgery and longer hospital stays,16,22–25 which aligns with our findings. This is congruent with rising rates of obesity nationally, and regional variations in obesity rates may further influence these outcomes. 26 Between 2019 and 2022, the South and Midwest both reported obesity in 42-45% of the population, compared to 36-39% in the West and Northeast regions. 27 Although preoperative BMI optimization is known to improve postoperative outcomes, our results suggest that surgery is increasingly offered to those with higher BMI, which could be contributing to the poorer outcomes observed. High BMI may reflect the rising rate of obesity in the United States 28 and on its own does not indicate whether patients attempted any preoptimization strategies. Counseling by a nutritionist or dietician may be helpful if accessible, and the recent popularization of GLP-1 agonists for weight loss also hold promise in improving spine surgery outcomes. 29
In our study, underweight patients also demonstrated worse complication-free and readmission-free survival compared to those with normal BMI (Figure 2). This finding is consistent with previous studies of spine surgery which have shown that underweight patients experience higher rates of postoperative complications and readmission rates relative to patients with normal BMI.30,31 Although the mechanisms underlying these inferior outcomes are not fully understood, proposed explanations include poor nutritional reserve, sarcopenia, impaired wound healing, and a diminished immune response. 32 In other surgical populations, an “obesity paradox” has been described in which low BMI is associated with worse outcomes, potentially due to limited physiologic reserve and nutritional deficiency.30–33 In contrast to morbid obesity, where adverse outcomes may be in part driven by technical challenges, cardiopulmonary comorbidities, wound healing difficulty and thromboembolic risk, low BMI may reflect frailty or underlying chronic illness that is not fully captured by traditional comorbidity indices.32–34 Currently, there is a paucity of literature on spine surgery outcomes in underweight patients, in part because underweight individuals comprise of just 2% of the US population. 31 Nonetheless, our findings, together with prior studies, suggest that low BMI represents an important and underrecognized risk factor for adverse postoperative outcomes in spine surgery.
Diabetes
Diabetes has been cited as a key opportunity for presurgical optimization. Diabetes impacts 38.4 million people of all ages or approximately 11.6% of the U.S. population. 35 Diabetes has been associated with longer surgical time, increased infections, longer LOS, higher medical expenditure, and carries and increased risk of postoperative cardiovascular disease, mortality and pseudarthrosis.16,22,36-41 Literature suggests preoperative optimization with a target hemoglobin A1c of <716. Although diabetes is included in the CCI, a more detailed analysis of the influence of hemoglobin A1c on these current surgical outcome trends is warranted.
Smoking
We identified an increase in patients using tobacco within the year of surgery up to 24.5% in 2021-2022 from 14.09% in 2011-2022. This is incongruent with previous outcomes data that examined trends in posterior lumbar fusion from 2006 to 2016 and reported a decrease in tobacco use. 18 Considering that insurance reimbursement is often predicated on tobacco cessation prior to elective spine fusion surgery, in addition to the continually lowering rate of tobacco use in the U.S., it is surprising that we observed an increase in patients using tobacco within a year of surgery. Smoking impairs fusion and has been associated with increased complications and readmission rates after spine surgery, including impaired wound healing and higher occurrence of wound infections.16,22,42–47 Preoperative smoking cessation can reduce infection rates and prior literature has demonstrated a 41% risk reduction in postoperative complications in patients who quit 4 weeks prior to surgery (across multiple surgical subspecialities).16,48 Despite known benefits of smoking cessation and insurance reimbursement restrictions with tobacco use, poorer outcomes may be related to offering surgery to an increasing number of patients with recent tobacco exposure.
Opioid Use
Use of preoperative opioid medications decreased over the study period. These trends may represent success in some areas of presurgical optimization. Preoperative opioid use is strongly linked to negative outcomes such as increased postoperative opioid use, longer hospitalizations, higher healthcare costs, and a greater risk of surgical revision.49,50 In contrast to our findings, Stratton et al 51 found no difference in opioid use among Canadian patients waiting 6 weeks for surgery between 2014 and 2017. This discrepancy may stem from state legislation in the U.S. aimed at curbing opioid misuse. Godil et al 52 found that states with enacted laws in 2017 saw reduced opioid prescriptions 90 days before surgery. Our findings suggest progress, reflecting either heightened awareness among physicians about opioid risks or the impact of new policies aimed at addressing the opioid crisis.
Regional Variability
We assessed surgical outcomes nationally and regionally and report collective worsening of outcome measures. This stands in contrast to a prior study that found no significant changes in 30-day complication or readmissions between 2006-2016 after elective posterior lumbar fusion. 18 However, the prior study ended in 2016 and used the ACS-NSIP database, whereas the current study examined 2011-2022 using the PearlDiver database. Uniquely, the current study revealed regional outcomes differences. The South consistently performed the greatest number of PLIF surgeries, which is consistent with prior studies that have reported high rates of fusion in the South.53–56 Further, our updated assessment also reports significantly longer hospital LOS and readmission rates in the South. The greatest change in both complication and readmission rates were in the West. The MW did not experience a change in complication rate and the South had no difference in readmission rate over the study period. The NE was the only region observed to have significant reductions in complication and readmission rates.
An explanation of regional variability in outcomes is challenging and likely multifactorial. Prior studies have reported improved outcomes, including lower mortality and complication rates, for lumbar spine surgeries performed at high-volume hospitals and by high-volume surgeons.57,58 Data supporting the use of patient optimization strategies and enhanced recovery pathways largely came from academic institutions. Although the South performs the highest rates of PLIF, academic spine surgeons are most densely concentrated in the NE (3.28 spine surgeons per 1 million people; MW: 2.04/1M people; West: 1.92/1M people; South: 1.42/1M people). 59 The NE also has the smallest geographic footprint of the regions. The NE, with a high density of academic surgeons, may have better disseminated and implemented optimization protocols that resulted in notable outcomes. Contrast this against the South which covers a large geographic area, with significant areas of rural communities, and a lower density of academic spine surgeons. These findings suggest that regional differences in access to high-volume academic spine care may contribute to observed outcome disparities, though further study is needed to directly evaluate the impact of surgeon and institutional volume on these findings.
Factors external to medicine including regional environmental and socioeconomic differences also influence health outcomes 60 ; therefore, cultural or community-level factors may play a considerable role. Rural communities have greater rates of chronic, preventable diseases including obesity and diabetes as well as high rates of smoking, sedentary lifestyles, and an overall higher proportion of elderly individuals.61–63 According to the 2010 U.S. Census, nearly 50% of all people living in rural areas reside in the South emphasizing this region as a potential at-risk population. 64 Additionally, smaller, rural hospitals are more likely to perform both elective and nonelective lumbar spine fusion surgery compared to larger urban hospitals, 65 highlighting differences in clinical decision making across regions. Weinstein et al 54 suggested several factors contributing to these regional variations, such as the absence of conclusive scientific evidence favoring one surgical approach over another, financial incentives or disincentives related to surgical procedures, variations in clinical training and professional opinions, and the adoption of new technologies. Socioeconomic factors should also be considered in the preoperative and postoperative phases.
Impact of COVID-19 Pandemic
This study captures trends spanning 2011-2022 and thus includes the COVID-19 pandemic, during which hospital utilization, case selection, discharge disposition, and postoperative care may have been affected. In 2020, the first year of the COVID-19 pandemic, elective lumbar surgery declined dramatically while the volume of emergent procedures remained relatively stable. 66 Interestingly, our dataset did not reflect a significant drop in PLIF volume, which may be due to 2019 and 2020 data batching as well as rapid rebound of spine surgery.67,68 During the pandemic, spine surgery focused on higher-acuity/emergent cases with consideration of less invasive options when available and an emphasis on reducing hospitalization time given the significant shortage of hospital beds. 69 The pandemic disrupted all facets of healthcare which resulted in delays to spine care and comorbidity management that may have added to patient complexity as elective surgeries were resumed which would influence observed trends in length of stay, complications, and readmissions. 70
Limitations
This study faces limitations common to retrospective analyses of large databases. Data may be affected by coding or reporting biases, although such biases are unlikely to vary significantly over time within the database. We included both CPT and ICD codes to capture surgeries performed in both in outpatient or day surgery centers, as well as hospital admissions as this best represents the national landscape. However, we might expect greater case complexity associated with hospital admissions by ICD coding alone which may reflect a population more amenable to optimization. To this point, the data was not differentiated by surgical complexity (ie, number of instrumented levels) which likely impacts the short-term outcome measures assessed.
Our assessment focused on few selected variables and outcome measures to provide a gestalt of preoperative optimization success. Tobacco use could be extracted in a time-relevant manner and provides indirect insight into bone health optimization. Preoperative opiate use gained recognition as associated with postoperative pain management, increasing length of stay, complications, and revisions after spine surgery. 53 CCI was selected to evaluate the impact of comorbidities overall rather than assessing each potentially relevant diagnosis as an independent variable (ie, diabetes, osteoporosis, anemia). Importantly, the patient characteristics evaluated here are proxies for, but are not direct measures of optimization as large database studies are unable to assess with this level of granularity. Additionally, multivariable modeling to identify which risk factors were driving outcomes was not pursued in favor of focusing on the study goal to identify patterns of optimization and outcomes. Based on regional findings, we anticipate that driving factors may differ by region and would be an interesting next avenue of study.
Outcomes studied were also limited to length of stay, 30-day complications, 90-day readmissions, and infection. Reoperation was incorporated in 90-day all-cause readmission but was not specifically queried. Specific questions on varying reoperation rates across regions would be an interesting next step in study. Although CCI was evaluated as a risk factor (which predicts 10-year survival), mortality was not selected as an outcome measure of interest given that it is an uncommon complication relative to the selected outcome variables.
Despite these limitations, these data provide valuable information on updated outcome trends and patient characteristics of those receiving posterior lumbar instrumented fusion in the United States.
Conclusion
In conclusion, this study offers a high-level assessment of the surgical outcomes associated with PLIF over an 11-year period, revealing a trend of overall worsening national and regional outcomes, despite anticipated progress with preoperative patient optimization. Our findings indicate that we are operating on older patients with increasing medical complexity, obesity, and tobacco use associated with nationally increased hospital LOS, 30-day complication rate and 90-day readmission rate, though there are significant regional differences. This unanticipated increase in adverse outcomes underscores the need for more granular analysis to elucidate the multifactorial contributing factors to explain divergent regional trends. Multidisciplinary collaboration between primary care physicians, nutritionists, endocrinologists, social workers, and spine surgeons are encouraged to improve outcomes in spine surgery.
Supplemental Material
Supplemental material - Nationwide and Regional Trends in Surgical Outcomes After Posterior Lumbar Interbody Fusion Over an 11-Year Period
Supplemental material for Nationwide and Regional Trends in Surgical Outcomes After Posterior Lumbar Interbody Fusion Over an 11-Year Period by Lauren A. Nguyen, Erin A. Yamamoto, Maryam N. Shahin, Josiah N. Orina, Clifford Lin, Jung Yoo, and Won Hyung Ryu in Global Spine Journal
Footnotes
Ethical Considerations
This study used publicly available, de-identified data and did not involve human subjects or protected health information. Therefore, institutional review board (IRB) approval and informed consent were not obtained.
Author Contributions
LAN: analysis, manuscript draft, final approval. EAY: analysis, interpretation, manuscript draft, final approval. MNS: analysis, interpretation, manuscript draft, final approval. JNO: study design, manuscript critical review, final approval. CL: study design, manuscript critical review, final approval. JY: study design, manuscript critical review, final approval. WHAR: study conception, study design, manuscript critical review, final approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets are publicly available through the PearlDiver database.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.