
Abstract
Study Design
Retrospective cohort study.
Objective
To compare the clinical outcomes and cost-effectiveness of vertebroplasty augmented with demineralized bone matrix (VPDBM) and conventional bone cement vertebroplasty (VPBC) in osteoporotic vertebral compression fractures (OVCFs).
Methods
One hundred eighty-seven patients with acute OVCFs were reviewed (VPDBM, n = 103; VPBC, n = 84). Clinical outcomes were assessed using Visual Analog Scale (VAS) and Koval grade, and radiographic outcomes included vertebral kyphotic angle (VKA), local kyphotic angle (LKA), and correction angle. Treatment failure was defined as refracture requiring hospitalization or reoperation, persistent or worsening pain or function, or radiographic deterioration. Deterioration-free survival (DFS) was analyzed using Kaplan–Meier and Cox regression. Cost-effectiveness was evaluated from the hospital perspective.
Results
Both groups showed significant postoperative improvement in VAS and Koval grade, without between-group differences at 12 months. Immediate correction angle favored VPBC (P = .041), but this was not sustained. Composite treatment failure was lower with VPDBM (12.6% vs 27.4%), with odds ratio 0.38 (95% CI, 0.18-0.81), risk ratio 0.46 (95% CI, 0.25-0.85), and absolute risk reduction 14.8% (NNT 6.8; P = .010). Kaplan–Meier analysis showed superior DFS in VPDBM (log-rank P = .034). Adjusted Cox regression showed no significant difference (aHR 0.58; 95% CI, 0.24-1.39; P = .222). VPDBM was cost-effective, with ICER ₩43 978 ($32.0) per 1% DFS gain, below common willingness-to-pay thresholds.
Conclusion
VPDBM reduced treatment failures and improved DFS compared with VPBC, while remaining cost-effective in OVCF management.
Keywords
Introduction
Osteoporotic vertebral compression fractures (OVCFs) are a common and debilitating condition in the aging population, often resulting in persistent pain, reduced mobility, and increased healthcare burden. Percutaneous vertebroplasty (PVP) has become an established minimally invasive treatment for symptomatic OVCFs, offering rapid pain relief and functional recovery by stabilizing the fractured vertebral body with polymethylmethacrylate (PMMA) bone cement. However, the efficacy of PVP in preventing progressive vertebral collapse or adjacent segment fractures remains a topic of debate, particularly in severely osteoporotic patients with compromised bone healing potential.
PVP has been widely established as a cost-effective and clinically beneficial treatment for OVCFs. Several studies across different healthcare systems, including South Korea, the United States, and Japan, have confirmed that vertebroplasty significantly reduces acute pain and improves mobility while maintaining a favorable cost-effectiveness profile compared to conservative treatment. A Korean cohort study showed that PVP shortened hospital stays and reduced healthcare costs without compromising outcomes, 1 and similar findings were observed in economic analyses from Europe and Asia.2,3 These findings have reinforced the role of PVP as a favorable treatment strategy in health systems seeking efficient management of OVCFs.
While PMMA provides excellent mechanical stability, it lacks osteoinductive properties and generates significant heat during polymerization, which may lead to thermal cytotoxicity. 4 These material limitations have motivated interest in adjunctive biologic materials that can enhance bone healing and biocompatibility. To improve structural and biological outcomes, the integration of osteoinductive materials such as demineralized bone matrix (DBM) has garnered increasing interest. DBM is an allogeneic graft material processed to retain collagen, growth factors, and bone morphogenetic proteins (BMPs), enabling it to serve as both an osteoconductive scaffold and osteoinductive stimulus. In spinal fusion surgeries, DBM has been widely utilized as a graft extender or autograft substitute, particularly in lumbar and cervical fusion, showing comparable fusion rates with reduced donor-site morbidity.5-8 Its use has expanded through improved formulations such as putties and composites with calcium phosphate cement, which enhance handling, injectability, and biomechanical compatibility. Specifically in vertebral augmentation procedures such as PVP and kyphoplasty, DBM composites have shown favorable physical properties including low setting temperature and excellent injectability, which may reduce thermal injury risk and better integrate with osteoporotic bone compared to PMMA alone. 9 Despite these potential advantages, the clinical effectiveness and cost-efficiency of DBM use in vertebral augmentation remain underexplored. Most existing studies are either technical reports or small-scale retrospective series, and the economic implications of DBM use in routine PVP practice have not been adequately evaluated.
The present study aims to evaluate whether the use of DBM in PVP improves clinical and radiographic outcomes and reduces failure events compared to conventional PMMA-only PVP. Furthermore, we assess the cost-effectiveness of DBM augmentation using real-world hospitalization data and material cost-based analysis. We hypothesize that DBM augmentation will demonstrate favorable cost-effectiveness by reducing clinically relevant failures, despite its added material cost.
Materials and Methods
Study Design and Patient Selection
This retrospective cohort study was conducted in accordance with STROBE (Strengthening The Reporting of Observational Studies in Epidemiology) guidelines after approved by the Institutional Review Board (IRB) of Samsung Changwon Hospital, Sungkyunkwan University School of Medicine (IRB No. 2025-02-005). The IRB formally granted a waiver of informed consent because this study involved a retrospective review of de-identified clinical data, posed minimal risk to participants, and did not involve any intervention beyond standard clinical care. All procedures were conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments. It was conducted at a single tertiary care institution and included patients who underwent percutaneous vertebroplasty (PVP) for osteoporotic vertebral compression fractures (OVCFs) between January 2020 and March 2025. The diagnosis of fracture was made based on simple radiographs and magnetic resonance imaging (MRI). Only patients with acute OVCFs were included in the present study. Acute fracture was defined as the presence of bone marrow edema on magnetic resonance imaging and symptom onset within 6 weeks prior to PVP. All included patients were aged 60 years or older and met the diagnostic criteria for osteoporosis based on the bone mineral density (BMD) threshold specified by the Korean Health Insurance Review and Assessment Service. In accordance with national reimbursement criteria and institutional practice, PVP was considered only after at least 2 weeks of adequate conservative management, including active analgesic treatment and mobilization with a rigid type thoracolumbosacral orthosis (TLSO) brace. PVP was performed when substantial limitations in activities of daily living persisted or when follow-up radiographs demonstrated progressive vertebral body collapse or worsening kyphotic deformity.
Patients with multiple vertebral compression fractures, associated non-spinal fractures, pathologic fractures, or history of spinal fusion surgery at other segments were excluded. Additional exclusion criteria included treatment by other departments during the same hospitalization period (eg, pneumonia, hemodialysis, or active malignancy) and extraosseous or intradiscal cement leakage that could compromise construct stability, whereas isolated venous leakage (cement confined to segmental or basivertebral veins without extraosseous pooling) was permitted. After applying these criteria, 103 patients who underwent PVP with DBM plus PMMA were included in the VPDBM group, and 84 patients who received PMMA alone were included in the VPBC (vertebroplasty with bone cement alone) group. All procedures were performed under a standardized clinical pathway to ensure consistent perioperative care. Baseline characteristics, including age, sex, BMD, fracture level, and comorbidities (diabetes mellitus, hypertension, cardiovascular disease, chronic kidney disease, rheumatoid arthritis, steroid use, and smoking), were recorded to confirm group homogeneity. Systemic osteoporosis medication exposure was abstracted from the electronic medical record and pharmacy records. “Before surgery” was defined as any active osteoporosis prescription within the 6 months preceding vertebroplasty, and “after surgery” was defined as any osteoporosis prescription initiated or continued within the 12 months following vertebroplasty. Regimens were classified as none, bisphosphonate, denosumab, teriparatide, or romosozumab.
Surgical Procedure
All PVPs were performed under local anesthesia with the patient in the prone position. Either an unipedicular or bipedicular approach was used via the transpedicular route, depending on the vertebral level and fracture morphology. In the VPDBM group, 1 cc of injectable DBM (Rafugen DBM putty, Korea Bone Bank, Korea) was delivered into the fractured vertebral body prior to cement application (Figure 1). No cellular bone allograft or bone marrow aspirate was employed. In the VPBC group, only PMMA was injected. According to the procedural protocol, the target injected cement volume was at least 4 mL at thoracic levels and at least 5 mL at lumbar levels to achieve adequate vertebral fill while minimizing the risk of leakage. The exact injected volume at each level, the viscosity at the time of injection, and the radiographic distribution of cement were not systematically recorded for analysis. All procedures were performed by three board-certified spine specialists, including one orthopedic surgeon and two neurosurgeons. Operative workflow of PVP with adjunctive DBM, shown as paired intraoperative C-arm fluoroscopic images (left) and matching schematic diagrams (right). (A) Transpedicular access to the vertebral body with the stylet engaged in the cannula. After stylet withdrawal, DBM (red dots) is delivered through the sheath into the vertebral body; DBM itself is not radiopaque and is indicated in the schematic. (B) The stylet is fully reinserted to clear the sheath, leaving DBM within the vertebral body. (C) PMMA (gray shading) is injected during the doughy phase to achieve adequate vertebral fill while avoiding leakage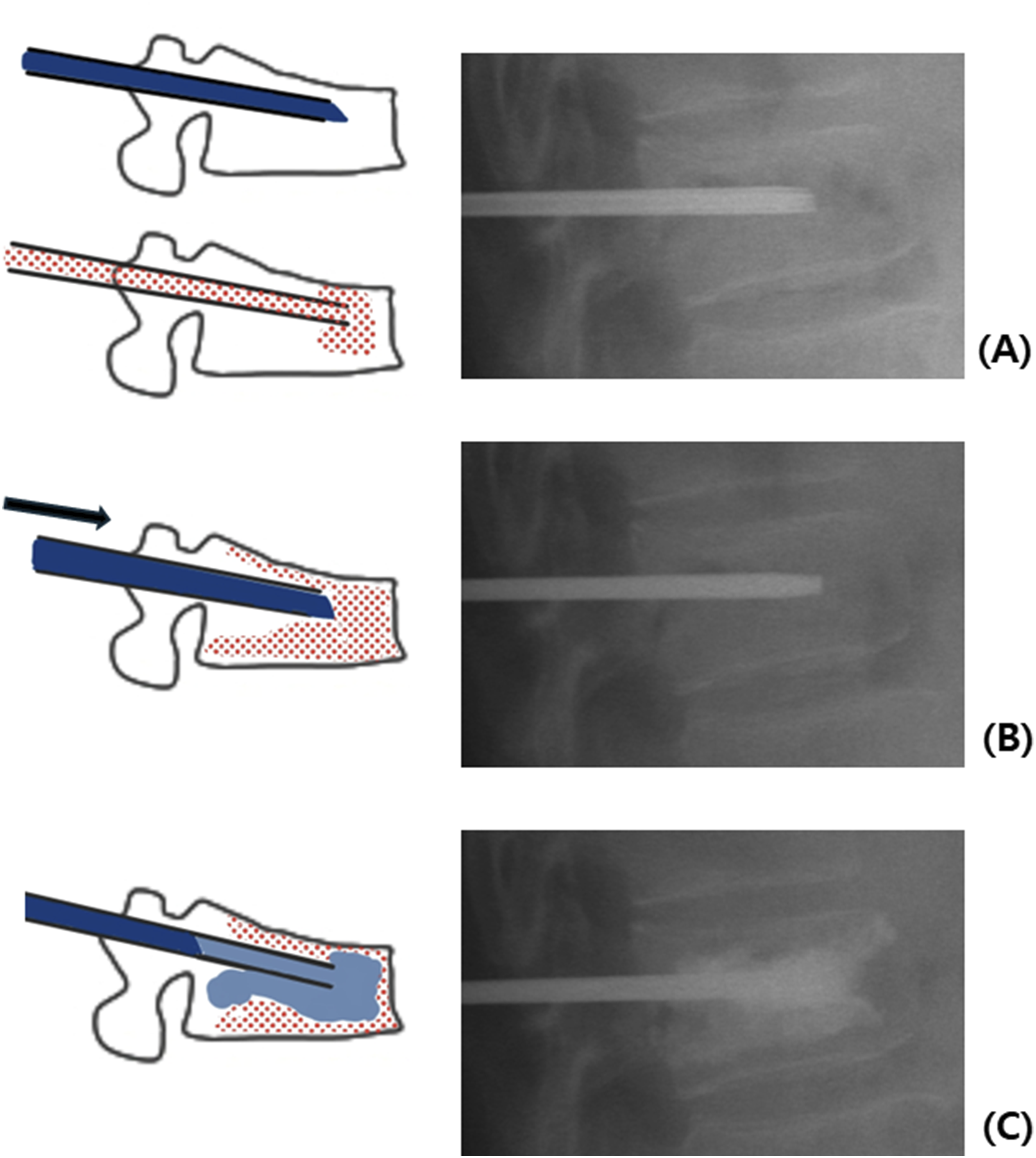
Postoperative Care
After surgery, patients remained on absolute bed rest (ABR) for 6 hours. They then began ambulation with a TLSO brace. The TLSO was worn continuously, except while lying down, for the first 6 weeks postoperatively. After the initial 6-week period, the brace was required only during vehicle transportation or while engaging in strenuous physical activities for an additional 6 weeks.
Outcome Measures
Clinical and radiologic outcomes were assessed at five standardized time points: preoperatively, postoperative day 1, and at 3, 6, and 12 months of follow up. Pain intensity was evaluated using the Visual Analog Scale (VAS; 0-10), with higher scores indicating greater subjective pain.
Functional status was assessed using the Koval grade, a 7-point scale widely used to classify ambulatory ability after spinal or hip injury. The scale ranges from Grade 1 (independent community ambulator) to Grade 7 (completely nonambulatory), allowing for stratified interpretation of postoperative functional outcomes and rehabilitation needs. This scale has been previously validated in vertebral fracture and elderly orthopedic populations as a reliable indicator of ambulatory status and postoperative recovery.10,11 Radiographic measurements, including vertebral kyphotic angle (VKA) and local kyphotic angle (LKA), were independently performed by two orthopedic surgeons with more than 10 years of clinical experience. The VKA was measured as the Cobb angle formed by the superior and inferior endplates of the index fractured vertebral body on lateral standing radiographs. Reviewers were blinded to group assignment and clinical data at the time of analysis. All measurements were conducted using the institutional picture archiving and communication system (PACS; INFINITT Healthcare Co., Ltd., Seoul, Republic of Korea) on lateral standing spine radiographs. The correction angle (CA) was defined as the difference between preoperative and postoperative VKA values. Follow up radiographs at 3, 6, and 12 months were used to assess maintenance of alignment and structural integrity over time.12,13,14
To assess long term clinical and structural outcomes, failure was defined as the occurrence of any of the following: (1) refracture at the treated or adjacent level requiring hospitalization or surgical intervention; (2) persistent or worsening pain (VAS score equal to or greater than preoperative value), or decline in ambulatory function (increase in Koval grade); and (3) radiologic deterioration, defined as an increase of >5° in VKA or LKA compared to the immediate postoperative measurement. Kaplan–Meier analysis was used to evaluate deterioration free survival in each group, a method previously employed in studies of vertebral augmentation and biologic bone substitutes.12,13
Cost-Effectiveness Evaluation
To evaluate the economic impact of demineralized bone matrix (DBM) use in percutaneous vertebroplasty (PVP), a cost-effectiveness analysis was performed using a hybrid approach that incorporated both real world hospitalization costs and direct material cost differences. All cost data were collected from institutional hospital billing records and were expressed in both Korean won (₩) and US dollars ($), based on the mean exchange rate over the preceding 3 months (₩1373 = $1).
The unit cost of DBM was fixed at ₩883 200 ($643.5) per case. In addition to this material cost, actual hospitalization expenses incurred during the inpatient stay were reviewed. The effectiveness of each intervention was defined as the number of patients who did not experience treatment failure over the 12-month follow up period. Treatment failure was defined as recurrent fracture, deterioration in pain or function, or radiographic collapse, as previously described. The incremental cost-effectiveness ratio (ICER) was calculated by dividing the difference in mean costs between the VPDBM and VPBC groups by the difference in the number of patients who avoided treatment failure. This approach conforms to established health economic guidelines and was used in prior vertebral fracture cost-effectiveness studies to evaluate biologic augmentation materials and vertebral augmentation procedures.1,2,15
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Chicago, IL, USA). Continuous variables were reported as mean ± standard deviation and compared between groups using independent t-tests or Mann–Whitney U tests, depending on the distribution. Categorical variables were analyzed using chi-square or Fisher’s exact tests, as appropriate. Paired t-tests were used to evaluate within group changes over time in clinical and radiologic outcomes.
To assess the interrater reliability of radiographic measurements, the VKA and LKA of 50 randomly selected patients were independently measured by a second orthopedic spine surgeon. Intraclass correlation coefficients (ICCs) were calculated to assess agreement between the two raters, using a two-way random-effects model for absolute agreement. ICC values were reported with 95% confidence intervals (CIs). Agreement was interpreted according to established criteria: <0.40 as poor, 0.40-0.59 as fair, 0.60-0.74 as good, and ≥0.75 as excellent reliability. 1 16
Deterioration-free survival (DFS) was estimated using the Kaplan–Meier method and compared between groups with the log-rank test. A multivariate Cox proportional hazards model was applied to adjust for potential confounders, including age, sex, baseline VAS score, fracture level, and BMD. Hazard ratios were reported with 95% CIs.
Patients with missing outcome data were excluded from analysis. The sample size was based on all eligible patients during the study period. Although no formal power analysis was performed, the study cohort was sufficient to detect clinically meaningful differences between groups. A two-tailed P-value <.05 was considered statistically significant.
Results
Comparison of Demographic Data Between the Two Groups
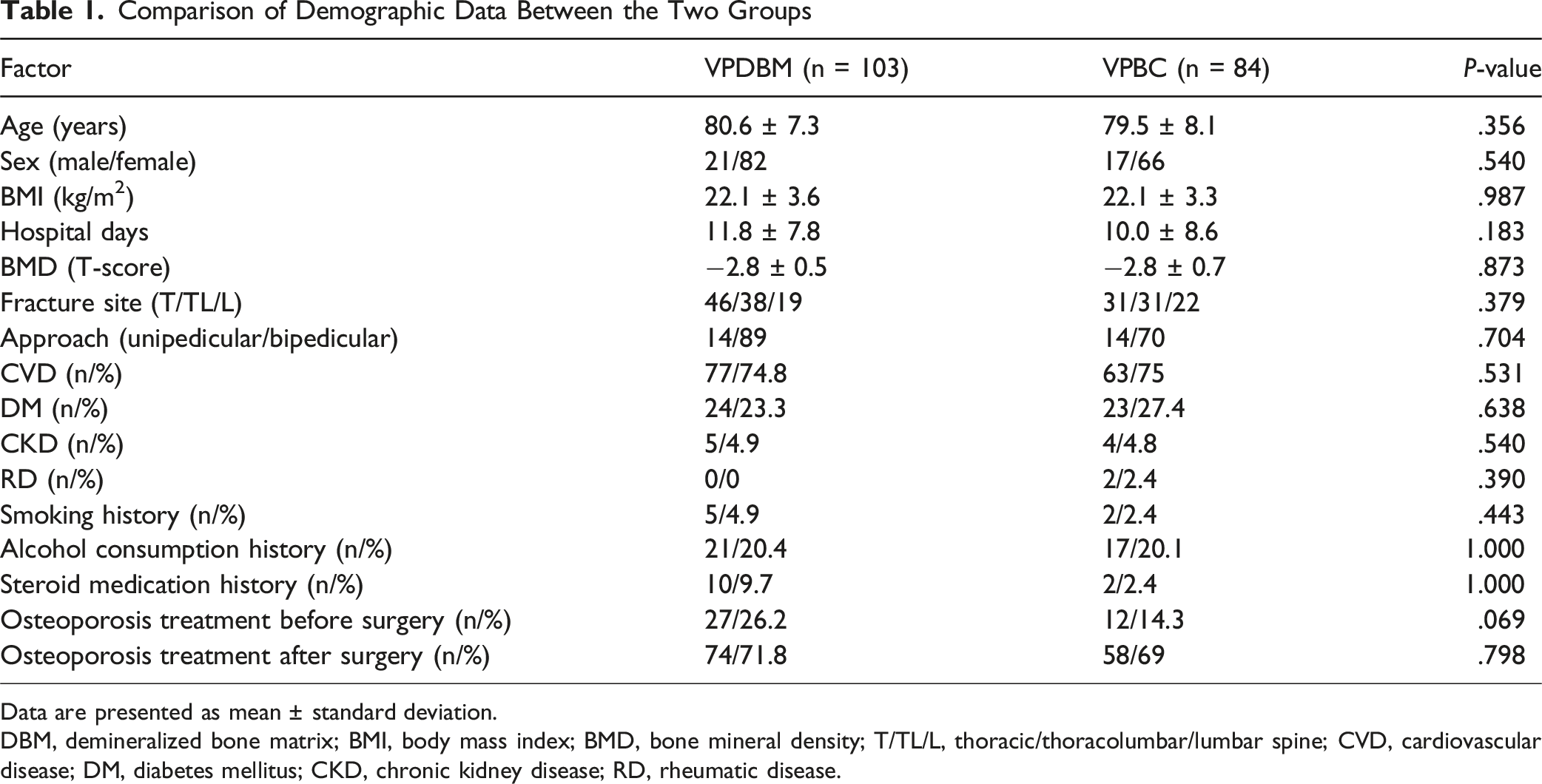
Data are presented as mean ± standard deviation.
DBM, demineralized bone matrix; BMI, body mass index; BMD, bone mineral density; T/TL/L, thoracic/thoracolumbar/lumbar spine; CVD, cardiovascular disease; DM, diabetes mellitus; CKD, chronic kidney disease; RD, rheumatic disease.
Postoperative Osteoporosis Medication
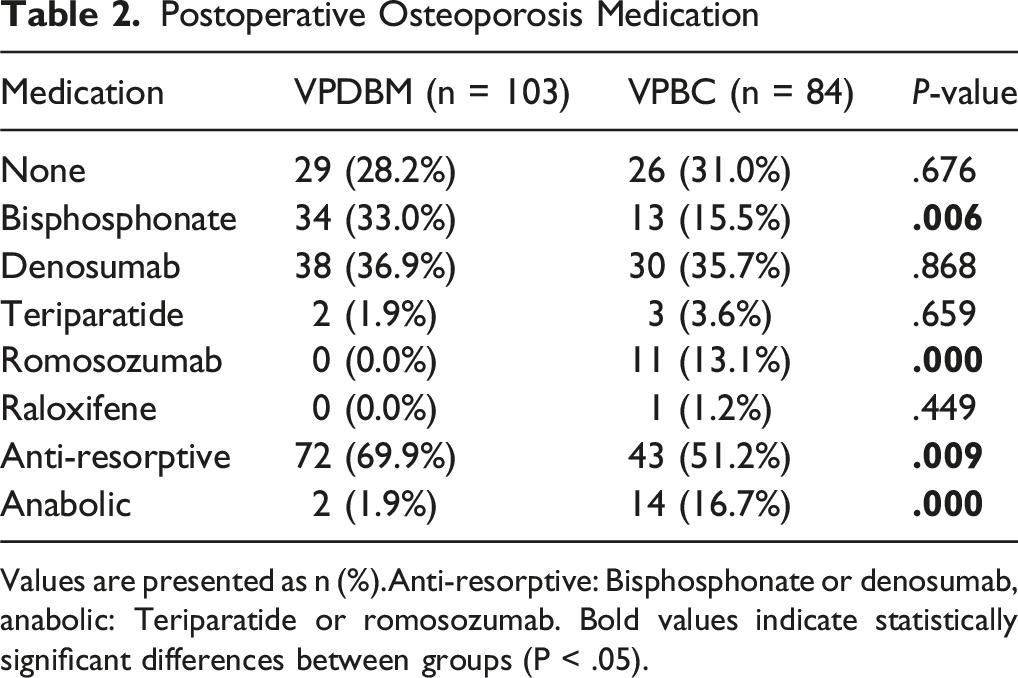
Values are presented as n (%).Anti-resorptive: Bisphosphonate or denosumab, anabolic: Teriparatide or romosozumab. Bold values indicate statistically significant differences between groups (P < .05).
Comparison of VAS Scores and KOVAL Grades Before and Postoperative in the Two Groups
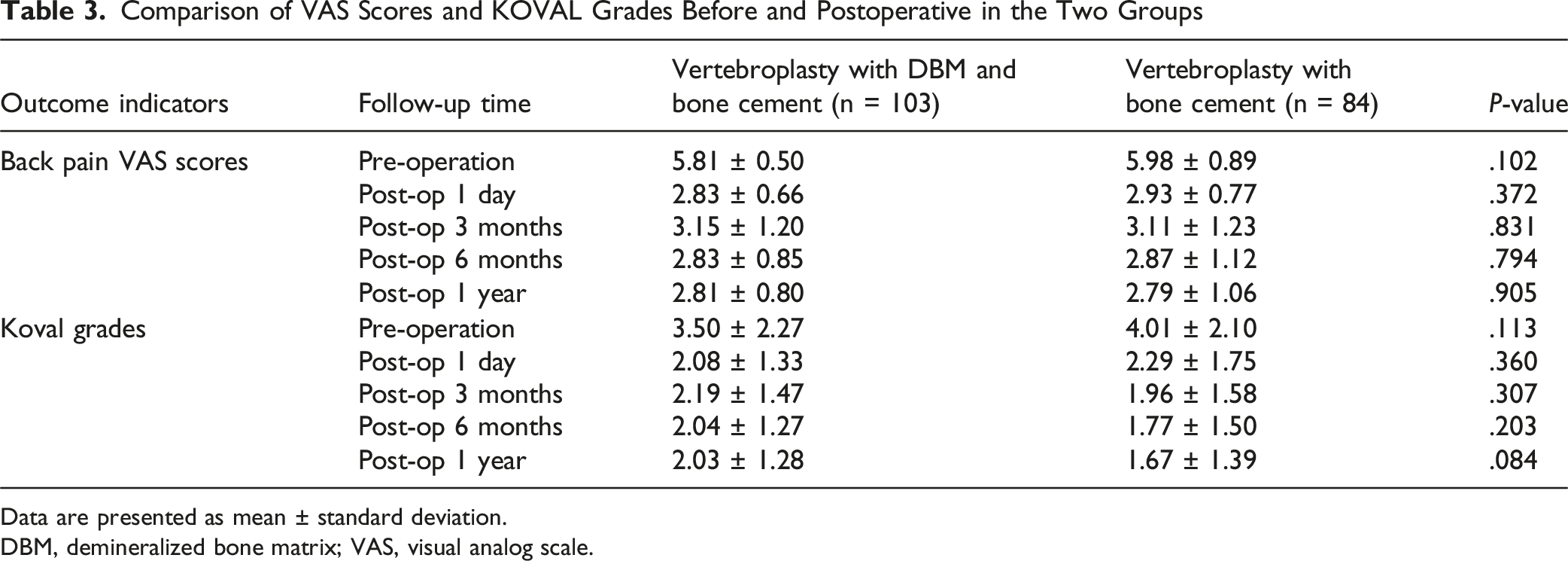
Data are presented as mean ± standard deviation.
DBM, demineralized bone matrix; VAS, visual analog scale.
Comparison of Radiological Results Before and Postoperative in the Two Groups
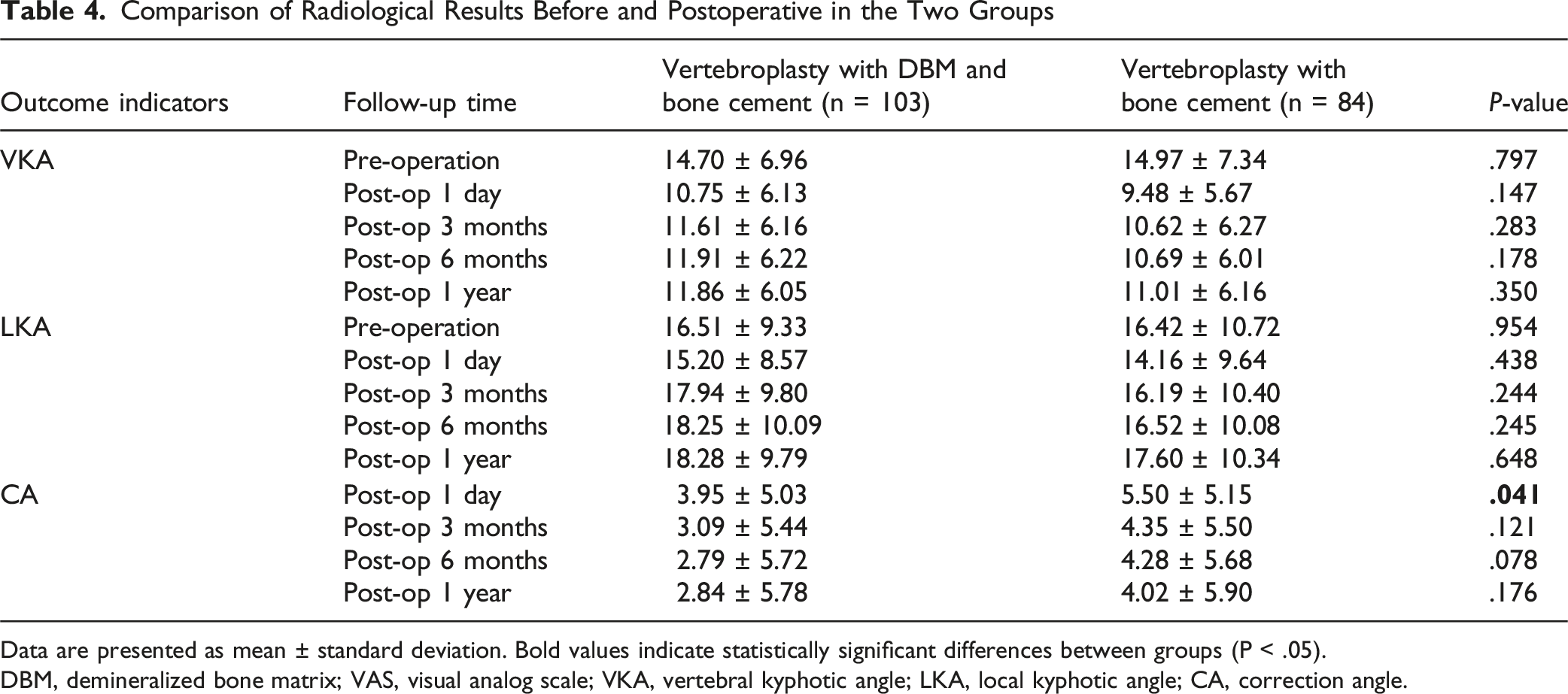
Data are presented as mean ± standard deviation. Bold values indicate statistically significant differences between groups (P < .05).
DBM, demineralized bone matrix; VAS, visual analog scale; VKA, vertebral kyphotic angle; LKA, local kyphotic angle; CA, correction angle.
The overall composite treatment failure rate was significantly lower in the VPDBM group than in the VPBC group (12.6% vs 27.4%), corresponding to an unadjusted odds ratio of 0.38 (95% CI, 0.18-0.81), a risk ratio of 0.46 (95% CI, 0.25-0.85), and an absolute risk reduction of 14.8% (number needed to treat = 6.8; P = .010). Kaplan–Meier analysis demonstrated superior deterioration-free survival in the VPDBM group compared with the VPBC group (log-rank P = .034), with early and sustained divergence of survival curves (Figure 2). In Cox regression adjusted for age, sex, and bone mineral density, VPDBM showed a trend toward a lower hazard of treatment failure; however, this association did not reach statistical significance (aHR 0.58; 95% CI, 0.24-1.39; P = .222). Kaplan–Meier curves for deterioration-free survival (DFS) through 12 months after percutaneous vertebroplasty for osteoporotic vertebral compression fractures. VPDBM (blue) and VPBC (red). Time zero is the day of surgery; patients were censored at last follow-up. Dots mark scheduled assessment time points (1, 3, 6, and 12 months). The VPDBM curve remains above VPBC throughout follow-up, with most failures in both groups occurring within the first 6 months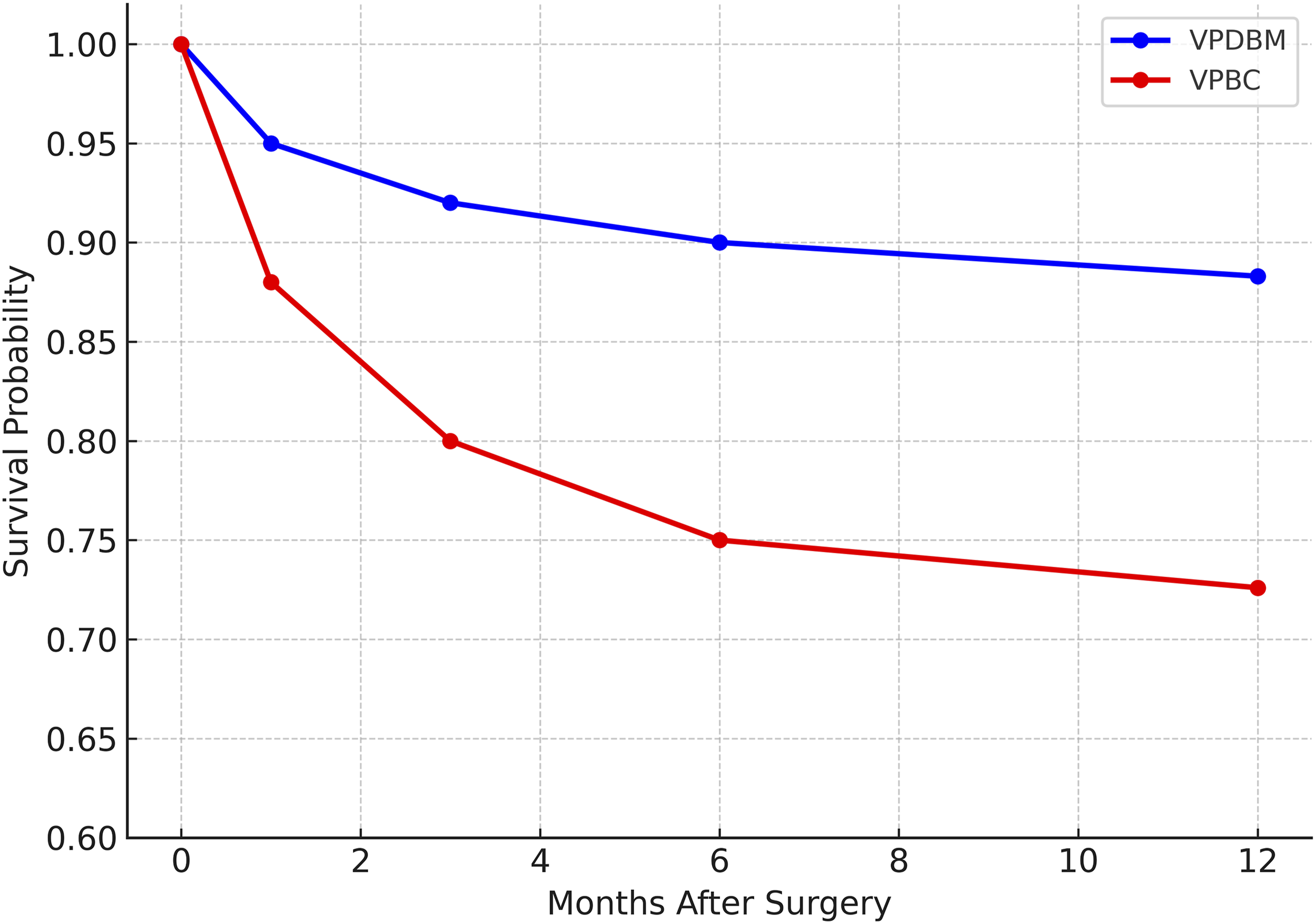
A cost analysis from the hospital perspective during the index admission incorporated the fixed device cost of DBM (₩883 200 [$643.5] per case) and actual inpatient expenses retrieved from hospital billing records. Per prespecified criteria, patients with prolonged hospitalization (≥14 days) or concurrent care for unrelated medical conditions were excluded from the cost analysis. The adjusted mean inpatient cost was ₩4 693 359 ($3419.7) in the VPDBM group and ₩4 121 060 ($3003.7) in the VPBC group. Despite the higher cost, VPDBM was associated with a lower composite failure rate and higher DFS. The ICER was ₩43 978 ($32.0) per 1% absolute increase in DFS, indicating that each 1% improvement required an additional cost of less than ₩50 000 ($36). This level of cost falls well below commonly accepted willingness-to-pay thresholds, suggesting favorable cost-effectiveness.
Discussion
This retrospective cohort study evaluated the clinical and radiographic efficacy, as well as the cost-effectiveness, of DBM augmentation during PVP for OVCFs. Over 12 months, pain relief and functional recovery, measured by the VAS and Koval grade, did not differ significantly between the VPDBM and VPBC groups. However, the VPDBM group exhibited a significantly lower composite failure rate and higher DFS. From the hospital perspective during the index admission, the incremental cost per 1% absolute increase in DFS was ₩43 978 ($32.0). Although this metric is not directly comparable to standard willingness-to-pay thresholds based on quality-adjusted life-years (QALYs), it provides a transparent, procedure-proximal measure that clinicians and payers can apply to real world decision making. Future studies should incorporate utility-based endpoints, prespecified thresholds, and uncertainty analyses to enable formal comparisons.
Most failures occurred within the first 6 months in both groups, indicating a clinically relevant early risk window. This timing supports closer surveillance during the initial postoperative period and may justify proactive osteoporosis optimization strategies immediately after vertebroplasty.
The absence of between‐group differences in pain and ambulation despite a lower composite failure rate in VPDBM implies a clinical–radiographic dissociation. Prior studies likewise report that height restoration or kyphotic angle correction correlate poorly with pain relief after vertebral augmentation.17,18,19 One plausible explanation is that early analgesia is primarily mediated by mechanical stabilization and PMMA-related neurolysis, whereas biologic consolidation from DBM contributes to structural resilience through its osteoinductive and osteoconductive effects and the maintenance of alignment over time, without necessarily producing additional short term analgesic benefit.7,17,18 In line with this dissociation, contemporary trials and consensus statements endorse composite efficacy and durability/survival oriented endpoints to capture longer term value beyond pain scores alone.20,21
The biological rationale for DBM augmentation lies in its intrinsic properties. DBM is osteoconductive, providing a scaffold for new bone ingrowth, and osteoinductive through growth factors such as bone morphogenetic proteins (BMPs) that stimulate mesenchymal stem cell differentiation into osteoblasts. 22 These biologic mechanisms are particularly relevant in the context of osteoporotic fractures, where impaired bone remodeling is a critical challenge. The incorporation of DBM into the vertebral body thus offers the potential to support biologic healing and long term structural integration capabilities that PMMA alone does not possess.
These findings suggest that the addition of DBM may enhance the long term stability of the augmented vertebral body, even if short term symptomatic outcomes are comparable. This aligns with prior studies that highlighted the osteoinductive potential of DBM in spinal applications and its use as an adjunct to autograft or allograft in various fusion procedures.7,23 While prior reports have focused on DBM’s role in fusion settings, our study expands its applicability to vertebral augmentation, where both mechanical reinforcement and biological restoration are critical for long term outcomes.
PMMA remains the mainstay of vertebral augmentation owing to its immediate load bearing capacity; however, it is biologically inert, generates heat during polymerization with potential thermal injury, and, because of its higher elastic modulus relative to cancellous bone, can create stress concentrations at the cement–bone interface, potentially predisposing adjacent level fractures. Although the VPBC group achieved a larger immediate correction angle (Table 4), this early mechanical advantage did not translate into durable radiographic superiority at 12 months. The convergence of correction angles over time suggests that short term alignment gains may be offset by subsequent structural remodeling. In contrast, DBM can support gradual trabecular restoration and load sharing within the treated vertebral body, which is consistent with the lower composite failure rate and superior deterioration free survival observed in VPDBM. Direct evidence that DBM attenuates PMMA-related thermal effects is limited; rather, its biologic activity may facilitate bone remodeling and vascular ingrowth at the fracture site. Moreover, computational biomechanical analyses indicate that augmentation materials with mechanical properties closer to native cancellous bone yield lower stress concentrations at the vertebral endplates than PMMA. 24 By promoting more physiologic load sharing through regenerated trabeculae, DBM may reduce abrupt stress transitions and the risk of fractures at adjacent levels. Prospective studies are needed to test this hypothesis.
A prior Korean study comparing conservative management, VP, and balloon kyphoplasty (BKP) for osteoporotic vertebral compression fractures demonstrated that, although VP incurred higher initial treatment costs than conservative care, it was associated with better pain relief, faster functional recovery, and lower rates of subsequent fracture and hospital readmission. Consequently, the ICER of VP was within a clinically acceptable range, whereas BKP had a much higher ICER due to its significantly greater procedural cost without proportionally greater clinical benefit. 1 In a large scale U.S. Medicare based analysis, Hopkins et al. similarly reported that both VP and BKP were associated with lower mortality, reduced hospital readmission, and decreased risk of subsequent vertebral fractures compared to conservative treatment. Although these procedures required greater upfront costs, the long-term clinical benefits translated into improved cost-effectiveness profiles, particularly in elderly populations at high risk for future skeletal events. 15 These findings parallel our current results, wherein DBM augmented VP demonstrated improved structural durability and a lower failure rate. Despite the added material cost of DBM, our analysis showed that it yielded superior deterioration free survival at a modest incremental cost. The resulting ICER remained well within the range reported in previous vertebral augmentation studies, suggesting that biologic augmentation may enhance the long term value of vertebral augmentation without substantially increasing the economic burden—especially in high risk populations such as elderly patients with advanced osteoporosis.
Osteoporosis treatment rates did not differ significantly before the index fracture or after vertebroplasty; however, the composition of postoperative regimens showed group level contrasts. Antiresorptive therapy (bisphosphonate or denosumab) was used more often in VPDBM, whereas anabolic therapy (teriparatide or romosozumab) was more common in VPBC. Because anabolic agents have potent bone forming effects and have shown greater fracture risk reduction than antiresorptives in randomized trials and guideline endorsed treatment pathways, the higher use of anabolic therapy in VPBC would be expected to bias outcomes in favor of VPBC rather than VPDBM. 25 The observation that VPDBM nevertheless demonstrated lower failure and better deterioration free survival therefore strengthens the inference that DBM itself contributed to structural durability, beyond differences in medication mix.
From a clinical standpoint, DBM augmentation may be most valuable in patients at heightened risk of structural failure, such as advanced age, severely reduced BMD, or fracture morphologies prone to progressive collapse. Although our cohort was elderly with broadly similar baseline characteristics, targeted selection based on risk stratification may further enhance value and merits prospective evaluation.
This study has limitations. First, the retrospective single center design introduces selection and information bias. Second, technical parameters at the level of the procedure, including the exact injected cement volume at each level, the viscosity at injection, and the cement distribution pattern, were not captured and therefore could not be analyzed for possible dose response relationships or for their association with failure risk. Third, adverse events such as cement leakage were not systematically captured as dedicated outcomes. Fourth, the cost analysis was limited to the index hospitalization and direct material costs, without a societal perspective or utility-based measures. Finally, although medication exposure was abstracted, residual confounding by regimen selection cannot be excluded. Future work should include prespecified sensitivity analyses, for example excluding patients on romosozumab or stratifying outcomes by antiresorptive vs anabolic therapy. It should also employ multivariable time to event models that report adjusted hazard ratios for failure.
Conclusions
In this retrospective cohort of elderly patients with OVCFs treated with PVP, DBM augmentation was associated with a lower composite failure rate and higher DFS at 12 months, without between group differences in pain or ambulation. The incremental cost was ₩43 978 ($32.0) per 1% absolute increase in DFS from the hospital perspective during the index admission, supporting clinical and economic viability. Failures clustered within the first 6 months, indicating the need for early surveillance and osteoporosis optimization. DBM may be most beneficial in high risk patients (advanced age, severely reduced BMD, morphology prone to collapse); confirmation in prospective studies with standardized technique and utility-based outcomes is needed.
Footnotes
Author Note
No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Ethical Considerations
This study was approved by the ethical committee of the hospital. The requirement for informed consent was formally waived by the IRB due to the retrospective nature of the study and the use of de-identified data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.