
Abstract
Objectives
This study analyzed the effects of rosuvastatin and zoledronic acid in combination on patient recovery following percutaneous vertebroplasty (PVP) that was performed to treat senile osteoporotic vertebral compression.
Methods
Senile patients with osteoporotic vertebral compression fracture (n = 120) were included in this retrospective study, and they were classified into two groups. Those in the control group (n = 60) were treated with PVP + caltrate and those in the observation group (n = 60) received this treatment with combined zoledronic acid and rosuvastatin. Between-group comparisons were made at both pre- and post-treatment regarding bone density, type I procollagen peptide (CTX) and bone-specific alkaline phosphatase (BAP) levels, visual analog scale (VAS) score, Oswestry Disability Index (ODI) score, and adjacent centrum refracture.
Results
Bone density was higher and BAP and CTX levels as well as ODI and VAS scores were lower at post-treatment in the observation group compared with the control group. The refracture rate in the observation group was lower compared with the control group.
Conclusion
Treatment with a combination of rosuvastatin and zoledronic acid following PVP can improve the condition of senile osteoporotic vertebral compression fracture and patient’s functional status, and it can also alleviate pain.
Keywords
Introduction
Clinically, osteoporosis is a systematic disease that is characterized by low bone density and a high risk of fracture, having a higher incidence of hip, waist, or ankle fractures compared with non-osteoporotic patients. 1 As the Chinese population continues to age, an increasing number of senile patients are presenting with osteoporotic vertebral compression fractures that are severely affecting both their overall health status and quality of life. 2
Percutaneous vertebroplasty (PVP) is an advantageous and extensively used clinical procedure because of its minimal invasiveness, established efficacy, and low complication incidence. 3 However, its success is somewhat limited because of pain arising from the loss of vertebral height in the later stages of the procedure; this also causes refracture of adjacent centrums, and it severely compromises patients’ quality of life.4,5 Zoledronic acid, a novel drug used in the clinical treatment of osteoporosis, can accelerate fracture healing and reduce the refracture risk. Recent studies have suggested that statins can inhibit osteoclasts and promote osteogenesis.6,7
To promote healing of senile osteoporotic vertebral compression fracture, rosuvastatin was combined with zoledronic acid in this study, and this combination was administered to patients who had undergone PVP. The present study analyzed the clinical efficacy of rosuvastatin and zoledronic acid in combination, which was administered following PVP to senile patients who had osteoporotic vertebral compression fracture, and the effects of this combination on fracture healing were examined. Patients were classified into two groups: PVP + Caltrate (control) group and PVP + Caltrate + rosuvastatin + zoledronic acid (observation) group.
Materials and methods
Patients
One hundred twenty senile patients who were admitted to our hospital for the treatment of osteoporotic vertebral compression fracture were included as study participants, and the clinical data were retrospectively collected. The study was approved by the Peking University First Hospital medical ethics committee, and all patients or their legal guardian provided written informed consent.
Patients were classified into two groups based on the treatment method that was used. Those who received only PVP were placed into the control group, whereas the remaining patients were treated with rosuvastatin and zoledronic acid in addition to the routine treatment that was administered to the control group and then classified as the observation group. Patients who were diagnosed with single-segment thoracolumbar vertebral compression fractures based on the American Society of Anesthesiologist classes I and III without surgical contraindications and those who provided informed consent were included in this study. Patients who were previously treated with drugs that may affect bone metabolism, such as antiosteoporotic medications, anesthesia, and steroids; those who had nervous system, digestive system, or cardiovascular system diseases; or those who presented with severe liver and kidney insufficiency, poor general condition, allergic constitution, and a history of spinal surgery or preoperative abnormalities in the coagulation function were excluded.
Methods
Patients in the control group were treated with PVP that was assisted by a C-arm X-ray machine (Nanjing Perlove Medical Equipment Co. Ltd., Nanjing, China). After positioning, the needle was inserted into the radix arcus vertebrae via a bilateral vertebral pedicle approach under the guidance of the X-ray machine to create a passage. A cobalt drill was advanced to the one-third junction at the front and middle positions of the centrum to inject 3 to 5 mL of bone cement. The injection was terminated if there was resistance or if the edge of the centrum was reached. When the bone cement is concreted, the surgical cannula was removed, any seepage of bone cement and any abnormality in the patient’s heart rate, respiration, or other vital signs were carefully monitored; postoperatively, patients were required to lie in bed for 12 hours and were approved for out-of-bed activities 48 hours thereafter. Caltrate (approval document number: GYZZ H10950029; Wyeth Pharmaceutical Co., Ltd., Suzhou, China) was then administered orally at a dose of 600 mg once a day for 12 months.
At this point, patients in the observation group were additionally administered a combination of zoledronic acid and rosuvastatin. Specifically, 3 to 7 days postoperatively, 5 mg of zoledronic acid (approval document number: GYZZ H20113138; Chiatai Tianqing Pharmaceutical Group Co., Ltd.) and 500 mL of 0.9% sodium chloride (approval document number: GYZZ H33020614; Zhejiang Dubang Pharmaceutical Co., Ltd., Quzhou, China) were administered through an intravenous drip; additionally, 10 mg of rosuvastatin calcium tablets (approval document number: GYZZ H20113246; Nanjing Simcere Dongyuan Pharmaceutical Co., Ltd., Nanjing, China) were administered once a day for 12 months. Patients in both groups were followed up for 12 months.
Observation indices
Bone density was measured pre- and post-treatment in both groups using an X-ray bone densitometer (Nanjing Simcere Dongyuan Pharmaceutical Co., Ltd.). To evaluate bone metabolism, 5 mL of venous blood was obtained from each patient following fasting at pre- and 12 months post-treatment, and the blood sample was centrifuged to harvest the liquid supernatant for bone-specific alkaline phosphatase (BAP) level assessment using an enzyme-linked immunosorbent assay and type I procollagen peptide (CTX) analysis via the chemiluminescence method. Additionally, pain intensity was assessed using a visual analog scale (VAS) score at pre- and 12 months post-treatment. A horizontal 10-cm long line was drawn on a paper, which was labeled 0 at one end, indicating no pain, and 10 at the other end, indicating severe pain. 8 The two groups were also scored using the Oswestry Disability Index (ODI) at pre- and 12-months post-treatment, with a higher score indicating more severe symptoms.9,10 Finally, considering the refracture of adjacent centrums, patients in both groups completed the 12-month follow-up post-treatment review to compare the refracture status of adjacent centrums. Patients in both groups were followed up for 12 months, and the incidence of adverse reactions during treatment was analyzed statistically.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) version 22.0 (IBM Corp., Armonk, NY, USA). Numerical data were expressed as the mean ± standard deviation, and comparison studies were performed using independent-sample t-tests for normally distributed data or the Mann–Whitney U test for non-normally distributed data. Nominal data were expressed as n (%), and comparisons were performed using the χ2 test for intergroup comparisons. For all statistical comparisons, the significance was defined as P < 0.05.
Results
Comparison between the observation and control groups based on general characteristics
Forty men (66.67%) and 20 women (33.33%) aged 61 to 80 (71.58 ± 2.28) years with a body mass index (BMI) of 21 to 29 (24.18 ± 1.08) kg/m2 were included in the observation group. The control group comprised 38 (63.33%) men and 22 (36.67%) women aged 60 to 79 (71.09 ± 2.27) years with a BMI of 22 to 28 (24.09 ± 1.05) kg/m2. The observation group included 30 (50%) patients who were injured by heavy objects, 20 (33.33%) who were injured by falls, and 10 (16.67%) with other types of injuries, whereas the control group included 32 (53.33%), 17 (28.33%), and 11 (18.33%) patients corresponding to the same three categories, respectively. No statistical differences were observed between the two groups in terms of gender (Figure 1), mean age, average BMI, or type of injury (Figure 2; Table 1).
Comparison between male and female patients in the observation and control groups.

Comparison of injury types in the observation and control groups.
General patient characteristics in the observation and control groups.
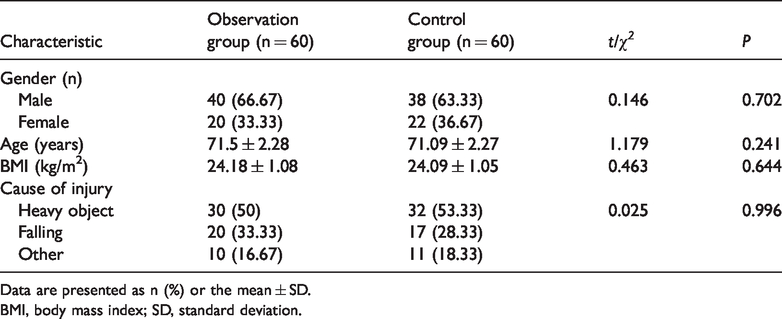
Data are presented as n (%) or the mean ± SD.
BMI, body mass index; SD, standard deviation.
Comparison between the observation and control groups based on bone density
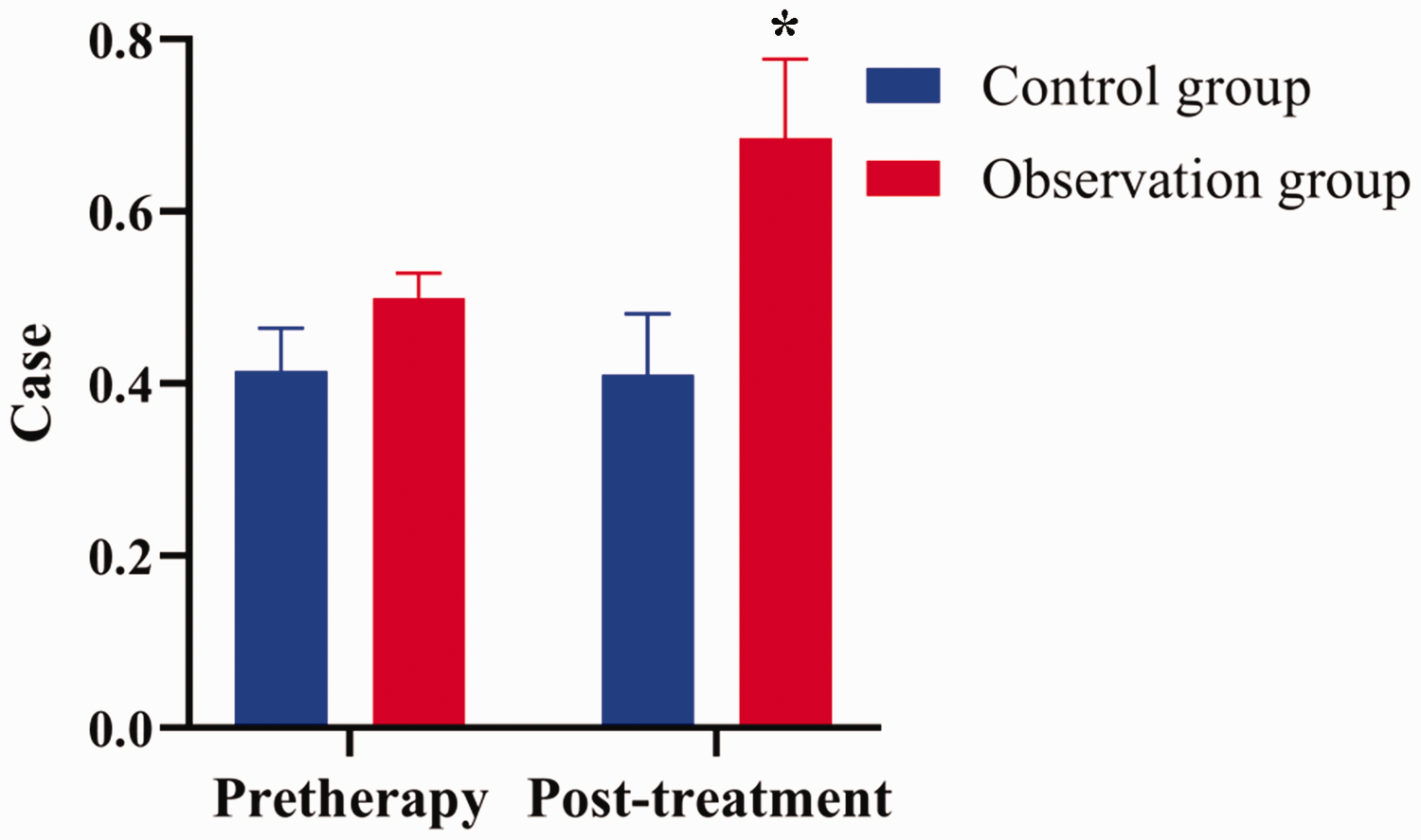
The difference between the groups was not statistically significant at pretreatment and both groups showed increased bone density at post-treatment compared with pretreatment (P < 0.05). The increase was found to be significantly greater in the observation group compared with the control group (P < 0.05; Table 2 and Figure 3).
Bone density in the observation and control groups.

Data are presented as the mean ± SD.
SD, standard deviation.
Comparison of bone metabolism indices in the observation and control groups.
Comparison between the observation and control groups based on bone metabolism indices
The two groups showed no statistical differences in terms of various bone metabolism indices at pretreatment, and each group showed reduced BAP and CTX levels at post-treatment compared with pretreatment (P < 0.05), but the decrease was greater in the observation compared with the control group (P < 0.05; Table 3).
Bone metabolism indices in the observation and control groups.

Data are presented as the mean ± SD.
BAP, bone-specific alkaline phosphatase; CTX, type I procollagen peptide; SD, standard deviation.
Comparison between the observation and control groups based on ODI and VAS
The difference in ODI and VAS scores was not significant at pretreatment, and these scores were subsequently significantly reduced at post-treatment in both groups (P < 0.05). However, post-treatment scores were significantly lower in the observation group compared with the control group (P < 0.05; Table 4).
ODI and VAS results in the observation and control groups.
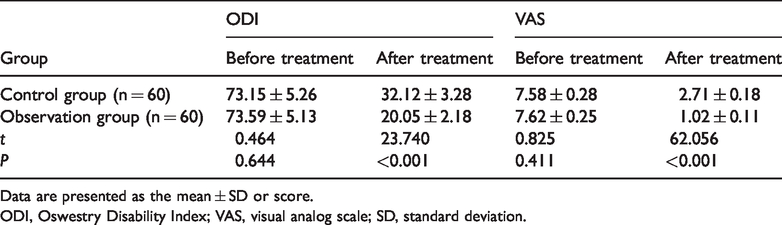
Data are presented as the mean ± SD or score.
ODI, Oswestry Disability Index; VAS, visual analog scale; SD, standard deviation.
Comparison between the observation and control groups based on refracture of adjacent centrums
At 12 months post-treatment, the observation group demonstrated a refracture rate of 1.67% for adjacent centrums, which was lower compared with that of 15% in the control group (P < 0.05; Table 5 and Figure 4).
Refracture status of adjacent centrums in the observation and control groups.


Comparison of the refracture rate in adjacent centrums in the observation and control groups.
Comparison between the observation and control groups based on adverse reactions
During the treatment period, one patient had muscle pain, two had joint pain, and one had fever in the control group, with an adverse reaction incidence of 6.67%. The corresponding adverse reactions in the observation group occurred in two, two, and one patient, respectively, with an adverse reaction incidence of 8.33%. The difference in adverse reaction incidence between the two groups was not significant.
Discussion
Osteoporotic vertebral compression fracture is an orthopedic disease that commonly occurs in the senile population. Its major manifestations include paroxysmal pains in the waist and back, restricted movement, and rachiterata, which significantly affect patients’ quality of life and health.11,12 Currently, several therapies are available to treat patients with the disease, which can be categorized into surgical and nonsurgical treatments.
PVP is one of the most common minimally invasive surgical procedures to address senile osteoporotic vertebral compression fractures. With the help of a C-arm X-ray machine, bone cement is injected into the centrum to effectively reinforce the sclerotin, improve the osteoporosis status, stabilize the spine, and alleviate pain.11,13 However, although this surgical procedure can reduce patients’ symptoms to a certain degree, it may also lead to a loss of vertebral height postoperatively and easily trigger pain. Additionally, the refracture rate of adjacent centrums is high and can severely affect the patients’ quality of life post-treatment. Therefore, administration of medications that can promote or support fracture healing is suggested postoperatively.
Vertebral compression fractures in senile patients are often accompanied by pain and other such symptoms, which may require long-term bed rest. This significantly affects patients’ quality of life because of the comparatively high associated disability and fatality rates.14,15 Second, after fracture, the rate of bone healing decreases, leading to increased difficulties in surgical treatment and a higher risk of postoperative refracture. Therefore, the clinical treatment for senile osteoporotic vertebral compression fracture should aim to effectively relieve pain in these patients so that they can perform activities as early as possible to maintain the stabilization of the coronal and vertical sections of the spine, and thereby avoid neurothlipsis at later stages.16,17 Currently, drugs that promote fracture healing include bone formation promoters, bone mineralizers, and bone absorption inhibitors. In the present study, the observation group achieved a higher bone density and lower BAP and CTX levels compared with the control group at post-treatment (P < 0.05), indicating that the rosuvastatin and zoledronic acid combination that was administered to the observation group can improve senile osteoporotic vertebral compression fracture outcomes following PVP by increasing the centrum bone density and reducing bone absorption activity. Moreover, the refracture rate for the adjacent centrums in the observation group was 1.67% and that in the control group was 15% (P < 0.05), which further supports the effectiveness of rosuvastatin combined with zoledronic acid following PVP.
Palmer et al. 18 also obtained similar results in their study, in which zoledronic acid was administered to senile patients with osteoporotic vertebral compression fractures following PVP, resulting in lower ODI and VAS scores and effective improvements in the injured centrum. These effects can be attributed to bisphosphonic acid drugs that are extensively used clinically to suppress osteoporosis, reinforce the osteoclast activity, reduce bone absorption, and increase bone density. 19 Zoledronic acid can activate osteoblasts by suppressing the osteoclast activity, by maximally avoiding osteolysis and destruction, to effectively increase the bone mass and improve osteoporosis.20,21 Statins were recently found to increase bone density, promote bone formation, and inhibit bone tissue absorption. 22 The type 1 collagen n-terminal peptide level is one index that reflects the bone absorption status. Its value can be significantly reduced, and bone absorption status can be prominently improved by statins. In the current study, ODI and VAS scores were lower in the observation group compared with the control group at post-treatment (P < 0.05), thereby confirming that this drug combination can improve the functional status and relieve pain postoperatively because both drugs can possibly promote fracture healing and accelerate bone callus formation. Zoledronic acid has demonstrated that it effectively inhibits osteolytic lesions to ease pain and induces apoptosis in osteoclasts and their precursor cells to reduce osteoclast activity, which resists bone absorption. Rosuvastatin promotes the upregulation of BMP-2 expression in bone cells as a precondition of osteoblast formation, reproduction, and differentiation. It can also contribute to fracture healing and prevent refracture. 23
In conclusion, rosuvastatin and zoledronic acid can be used in combination to treat senile patients with osteoporotic vertebral compression fracture following PVP because this method improves fracture and functional status, increases bone density in the centrum, reduces bone absorption activity, relieves pain, and effectively prevents refracture of adjacent centrums. However, considering the limited sample size of the present study, this investigation did not obtain representative results. Future studies should involve larger sample sizes, extend over a longer period of time, and cover more aspects to explore the clinical efficacy of rosuvastatin combined with zoledronic acid following PVP when treating senile patients with osteoporotic vertebral compression fracture.