
Abstract
Study Design
Retrospective cohort study.
Objectives
To determine whether preoperative cervical bone quality assessed by computed tomography Hounsfield units (CT HU) predicts pseudarthrosis, cage subsidence, or loss of cervical lordosis after anterior cervical discectomy and fusion (ACDF) and to identify perioperative predictors.
Methods
Consecutive patients who underwent 1-3-level ACDF with ≥5-year follow-up were reviewed. Outcomes included neck/arm pain visual analog scale scores, Neck Disability Index, and C2-C7 lordosis and segmental height. Bone quality was assessed by preoperative CT HU. Subgroup comparisons, multivariable regression, and receiver operating characteristic (ROC) analyses evaluated predictors.
Results
Among 253 patients, subsidence, pseudarthrosis, and loss of lordosis occurred in 15 (5.9%), 26 (10.3%), and 41 (16.2%), respectively. Index HU and clinical outcomes did not differ between subgroups defined by subsidence or pseudarthrosis. HU ≤ 231.5 was associated with a higher incidence of loss of lordosis. On regression, higher BMI and greater segmental lengthening independently predicted subsidence, while multilevel surgery predicted pseudarthrosis. Greater preoperative C2-C7 lordosis predicted loss of lordosis; very low HU (≤231.5) was significant in univariable analysis but not after multivariable adjustment. On ROC analysis, Index HU did not predict subsidence (AUC: 0.511), pseudarthrosis (AUC: 0.414), or loss of lordosis (AUC: 0.551). In contrast, segmental lengthening predicted subsidence (AUC 0.695) with threshold around 3 mm (3.12 mm).
Conclusion
Preoperative cervical CT HU did not predict pseudarthrosis or subsidence over ≥5 years after ACDF; low HU showed an unadjusted association with loss of lordosis. Bone quality alone may be insufficient to justify avoiding ACDF. Limiting segmental lengthening to ∼3 mm may mitigate subsidence risk.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is a commonly performed surgical procedure for degenerative cervical radiculopathy and myelopathy. Pseudarthrosis and cage subsidence are common complications following ACDF. These complications may result in suboptimal clinical outcomes and frequently necessitate revision surgeries.1,2
Low bone mineral density (BMD) is a well-recognized risk factor for implant failure and subsidence in lumbar spine fusion.3-6 However, BMD measured by dual-energy X-ray absorptiometry (DXA) has limitations because degenerative changes, such as osteophytes, can artificially increase the measured values. 7 Computed tomography–derived Hounsfield units (CT HU) measured directly within the vertebral body have emerged as a practical surrogate marker of bone quality8-11 and are increasingly used to predict postoperative complications.12-14
However, the extent to which poor bone quality predisposes to complications such as pseudarthrosis, cage subsidence, and loss of lordosis after cervical surgery remains unclear. Several recent studies have reported that osteoporosis or osteopenia do not significantly predict pseudarthrosis or subsidence following ACDF.15-17 Cadaveric studies have demonstrated substantial biomechanical differences between cervical and lumbar vertebrae, particularly in trabecular architecture and distribution.18,19 Therefore, the relationship between bone quality and complications after ACDF may differ from that observed in lumbar spine surgery.
This study aimed (1) to determine whether poor cervical bone quality, assessed by CT HU, is associated with increased risk of pseudarthrosis, subsidence, or loss of lordosis following ACDF; and (2) to identify perioperative factors associated with these complications.
Methods
Study Design and Population
This retrospective study was approved by the Institutional Review Board of the participating institution (2025-07-009), and informed consent was waived because of the study’s retrospective design. We reviewed 1231 patients (age range, 27-82 years) who underwent one- to three-level ACDF performed by a single surgeon at a single center between February 2006 and January 2020. Inclusion criteria were: (1) a diagnosis of degenerative cervical disease (eg, degenerative disc disease, cervical spondylosis) causing radiculopathy, myelopathy, or myeloradiculopathy; (2) receipt of one- to three-level plated ACDF; (3) availability of preoperative CT suitable for HU measurement; and (4) a minimum follow-up of 5 years. Exclusion criteria were: (1) prior cervical surgery; (2) concomitant procedures such as posterior fusion, vertebral body sliding osteotomy, or corpectomy; (3) ACDF using a cage alone (without plate fixation); (4) surgery for tumor, trauma, or infection. Based on these criteria, 253 patients were included in the final analysis (Figure 1). Flow diagram of patient selection for the study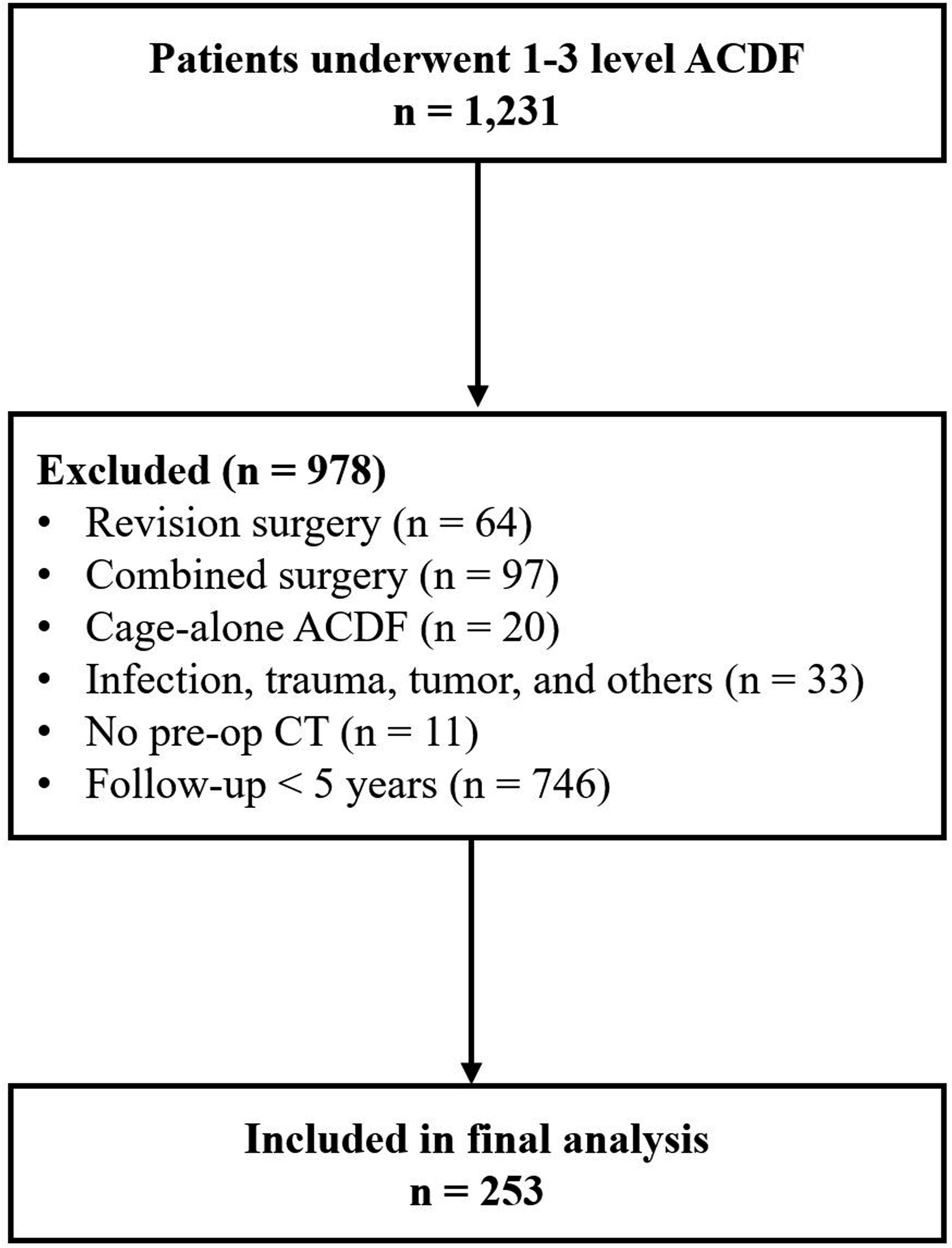
Surgical Technique
One surgeon performed all operations at a single center. The patient was positioned supine, and a standard left-sided Smith–Robinson approach was used to remove the intervertebral disc and osteophytes. Minimal decortication of the superior and inferior endplates was performed to minimize the risk of cage subsidence. Interbody cages were inserted at each level and packed with local autograft harvested during osteophytectomy and endplate preparation. When arm pain caused by foraminal stenosis was present, an additional uncoforaminotomy was performed. All operated levels were stabilized with an anterior cervical plate and variable-angle screw constructs to promote postoperative graft compression and gradual settling. The cage was positioned 2-3 mm posterior to the anterior vertebral body margin. A cervical collar was worn postoperatively for 6-12 weeks.20-22
Variables
Patient-reported outcomes included neck pain visual analog scale (VAS), arm pain VAS, and the Neck Disability Index (NDI) scores, which were assessed preoperatively, at 2 years postoperatively, and at the final follow-up (≥5 years). Neck and arm pain were measured using a 10-point VAS.
Variables Definitions and Assessment Timings

HU, Hounsfield unit; CT, computed tomography; ISM, interspinous motion.
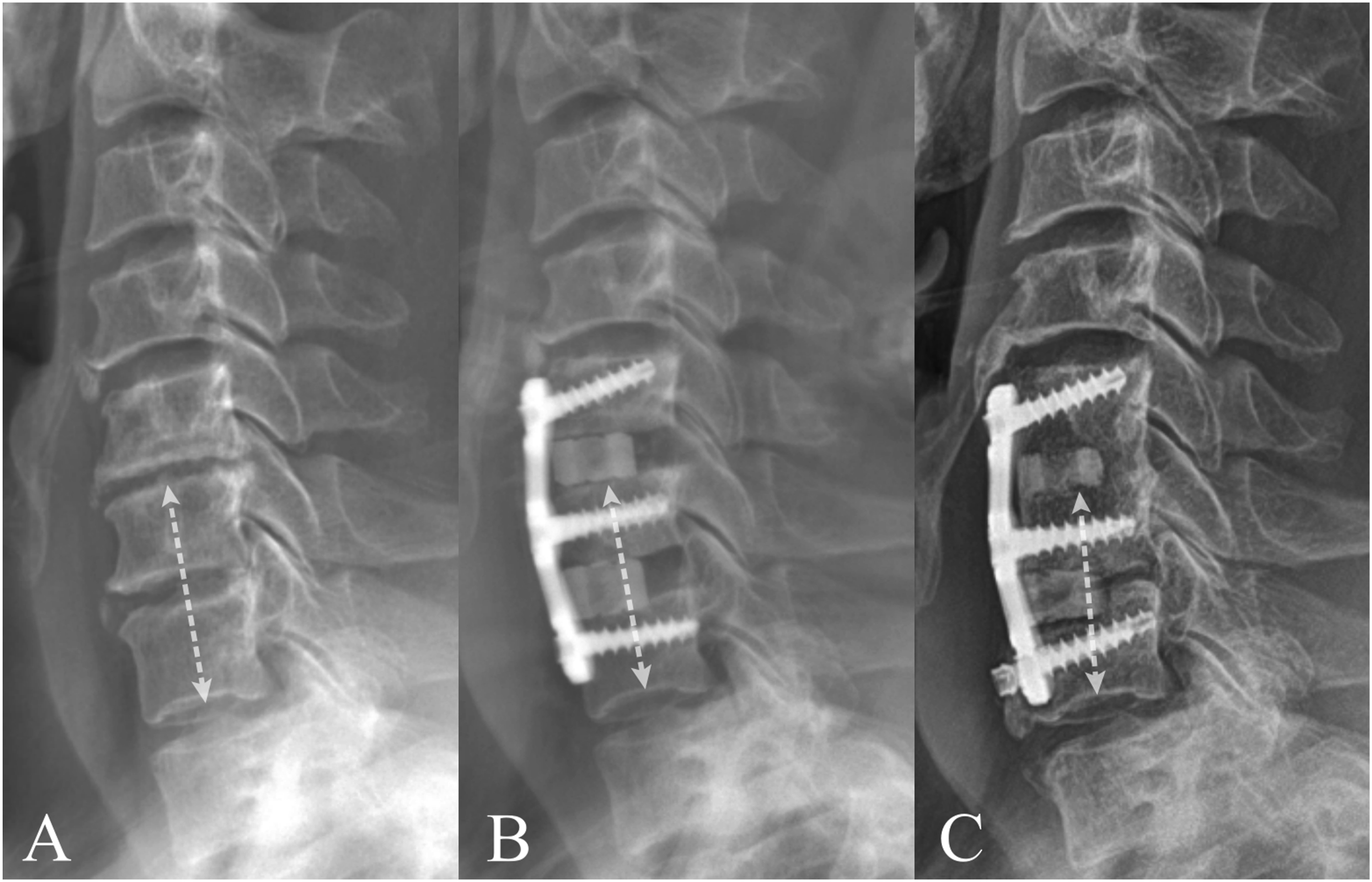
Radiographic measurement of segmental height, segmental lengthening, and subsidence.
Pseudarthrosis was defined using two complementary criteria, consistent with prior validated methods20,30-34: (1) interspinous motion (ISM) >1 mm on 150%-magnified dynamic lateral radiographs (flexion–extension), or (2) absence of bridging bone across the graft connecting adjacent endplates or outside the graft on CT. ISM and CT bridging were evaluated at 2 years and at the final follow-up, and union status or pseudarthrosis was recorded at each time point (Table 1) (Figure 3). Evaluation of pseudarthrosis using CT and dynamic radiographs.
Cervical alignment was assessed as C2-C7 lordosis on neutral lateral radiographs obtained preoperatively, within 1 week postoperatively, and at the final follow-up. Loss of lordosis was defined as a decrease of ≥5° at the final follow-up relative to the preoperative value35,36 (Table 1) (Figure 2).
Cervical bone quality (Index HU) was derived from preoperative noncontrast CT by measuring HU on mid-sagittal vertebral body reformats using small trabecular regions of interest (ROIs) that excluded the cortical rim, endplate sclerosis, and osteophytes. HU values were obtained from each operative-level vertebral body, and the Index HU was defined as the mean of these values. For multilevel surgeries, the Index HU represented the average HU across all vertebral bodies included in the fusion construct
25
(Table 1) (Figure 4). Measurement of preoperative bone quality using Hounsfield units (HU).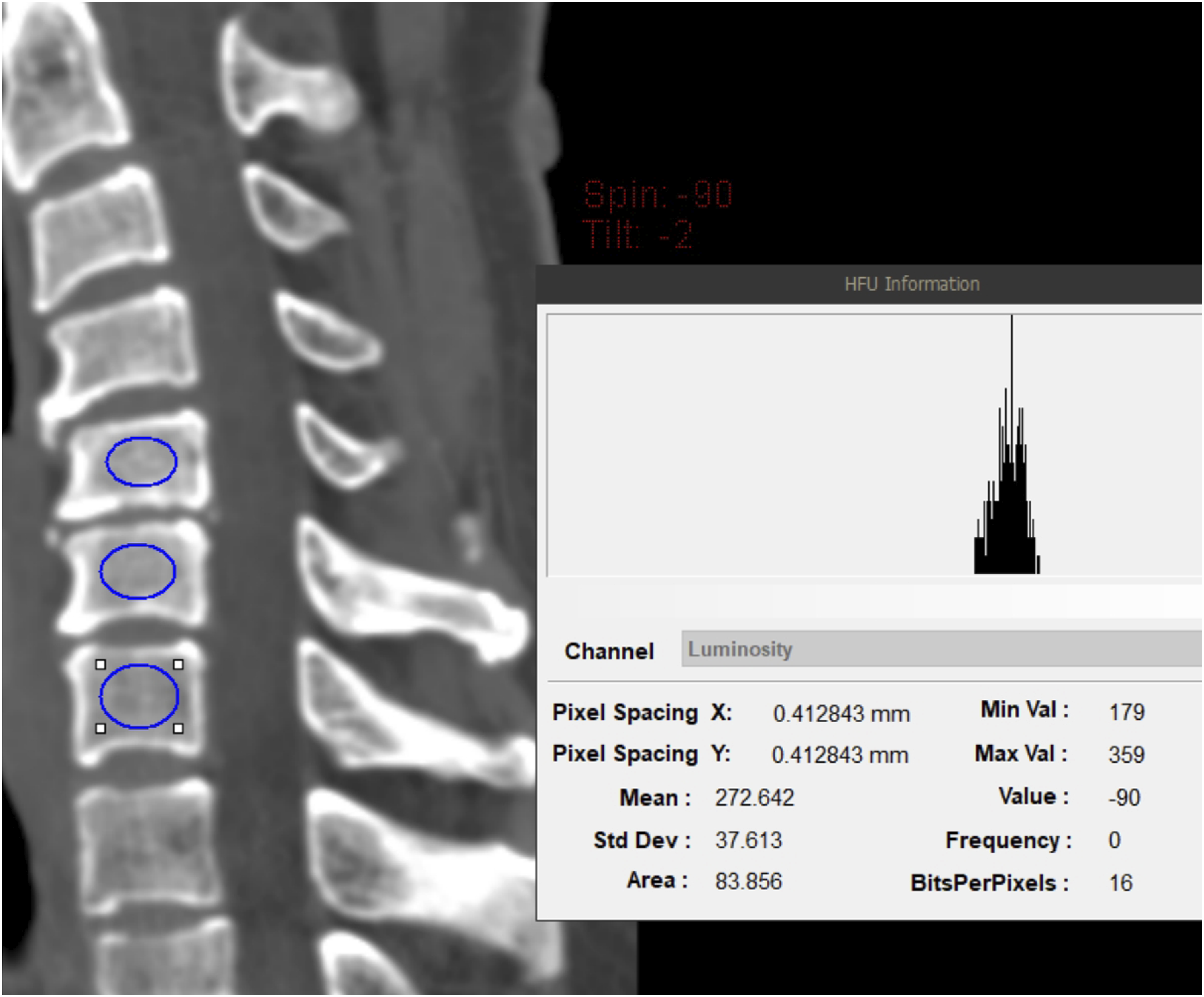
Two fellowship-trained attending spine surgeons independently performed all radiographic measurements to assess interobserver reliability, with intraclass correlation coefficients (ICCs) ranging from 0.842 to 0.953.
Statistical Analysis
The normality of continuous variables was assessed using the Shapiro–Wilk test. Subgroup analyses were conducted based on the presence or absence of subsidence, pseudarthrosis, and loss of lordosis at the final follow-up, using independent t-tests for continuous variables and chi-square tests for categorical variables. Intergroup analyses also used published CT HU thresholds for cervical osteoporosis—231.5 in a Korean cohort and 326.5 in a U.S. cohort.37,38
We conducted univariable and multivariable regression analyses to identify predictors of complications (subsidence, pseudarthrosis, and loss of lordosis). Candidate covariates included demographic variables and relevant preoperative and intraoperative factors. Variables with a screening P-value of ≤.100 in univariable analyses were entered into multivariable models.
Receiver operating characteristic (ROC) curves were constructed to evaluate the ability of the preoperative Index HU to predict pseudarthrosis, cage subsidence, and loss of lordosis. For each outcome, the area under the curve (AUC) and 95% confidence intervals (CI) were calculated. The optimal cutoff was determined by maximizing the Youden index (sensitivity + specificity − 1), and the corresponding sensitivity and specificity were reported. An identical ROC analysis was performed for postoperative segmental lengthening. All analyses were performed using IBM SPSS Statistics, version 29.0 (IBM Corp., Armonk, NY, USA), with statistical significance set at P < .05.
Results
Baseline Patient Characteristics
Among 253 patients, the distribution of operated levels was 1-level in 113 patients (44.7%), 2-level in 98 (38.7%), and 3-level in 42 (16.6%). The mean Index HU was 324.67 ± 77.07. At the final follow-up, subsidence occurred in 15 patients (5.9%). Pseudarthrosis was identified in 79 patients (31.2%) at 2 years; 67.1% (53/79) subsequently achieved delayed union, resulting in a final pseudarthrosis rate of 26 patients (10.3%) (Figure 5). Loss of lordosis was observed in 41 patients (16.2%). Subgroup analysis by subsidence status showed no significant difference in Index HU between groups (subsidence: 328.85 ± 70.76 vs no subsidence: 324.40 ± 77.58; P = .829) or in other demographic factors. Similarly, when stratified by pseudarthrosis status at the final follow-up, Index HU values did not differ significantly (pseudarthrosis: 307.53 ± 87.77 vs union: 323.63 ± 75.72; P = .232). When stratified by loss of lordosis, the mean Index HU was comparable between groups (P = .269). Notably, the proportion of patients with HU ≤ 231.5 was higher in the loss subgroup than in the no loss of lordosis subgroup (19.5% vs 8.5%; P = .047). The pseudarthrosis subgroup had a higher body mass index (BMI) (P = .047) and a greater proportion of smokers (P = .036). The distribution of underlying pathology differed between groups (P = .035), and multilevel procedures were significantly more frequent in the pseudarthrosis subgroup than in the union subgroup (P < .001) (Table 2, Supplemental Table 1). Change in union status from 2 years to ≥5 years after ACDF. Baseline Characteristics of Included Patients and Subgroup Comparisons by Subsidence and Pseudarthrosis at Final Follow-Up BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; Index HU, CT-measured mean vertebral Hounsfield Unit at index level. *P < 0.050.

Outcome Comparison Based on Complications
Clinical and Radiologic Outcomes at Final Follow-Up After ACDF; Comparison Based on Subsidence and Pseudarthrosis

VAS, visual analog scale; NDI, neck disability index.
*P < .050.
Stratification by pseudarthrosis revealed no between-group differences in neck pain VAS or NDI, except for higher preoperative arm pain VAS in the pseudarthrosis subgroup (P = .014). Radiographically, there were no significant between-group differences preoperatively or at the final follow-up. Subsidence occurred more frequently in the pseudarthrosis subgroup than in the union subgroup (23.1% vs 4.0%; P =.002), while revision surgery rates did not differ (P = .055) (Table 3).
When stratified by loss of lordosis, no significant between-group differences were observed in preoperative or final patient-reported outcomes (VAS and NDI). Radiographically, the loss subgroup had greater preoperative C2-C7 lordosis (16.01 ± 8.98 vs 3.94 ± 10.76; P < .001), whereas the final C2-C7 lordosis was comparable between groups (P = .061). Postoperative segmental lengthening was modestly smaller in the loss subgroup (1.14 ± 1.61 vs 1.76 ± 1.70; P = .032). Revision surgery was numerically more frequent in the loss subgroup, but the difference was not significant (12.2% vs 4.7%; P = .075) (Supplemental Table 2).
Comparison of Postoperative Complications by HU Cutoff Subgroups
Postoperative Complications According to HU Cutoffs of 231.5 and 326.5

HU, Hounsfield Unit.
*P < .050.
Regression and ROC Analysis for Predicting Complications
Multivariate Regression Analysis for the Predictors of Subsidence

VAS, visual analog scale; NDI, neck disability index; BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; SVA, sagittal vertical axis.
*P < .050.
Multivariate Regression Analysis for the Predictors of Pseudarthrosis

VAS, visual analog scale; NDI, neck disability index; CI, confidence interval; BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; SVA, sagittal vertical axis.
*P < .050.
Multivariate Regression Analysis for the Predictors of Loss of Lordosis

VAS, visual analog scale; NDI, neck disability index; CI, confidence interval; BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; SVA, sagittal vertical axis.
*P < .050.
ROC analysis showed that preoperative Index HU did not predict subsidence (AUC: 0.511; 95% CI: 0.372-0.649; P = .882), pseudarthrosis (AUC: 0.414; 95% CI: 0.298-0.530; P = .147) or loss of lordosis (AUC: 0.551; 95% CI: 0.447-0.655; P = .338). In contrast, segmental lengthening significantly predicted subsidence (AUC: 0.695; 95% CI: 0.550-0.840; P = .008), with an optimal cutoff of 3.12 mm (Figure 6). Receiver operating characteristic curve analysis for postoperative segmental lengthening.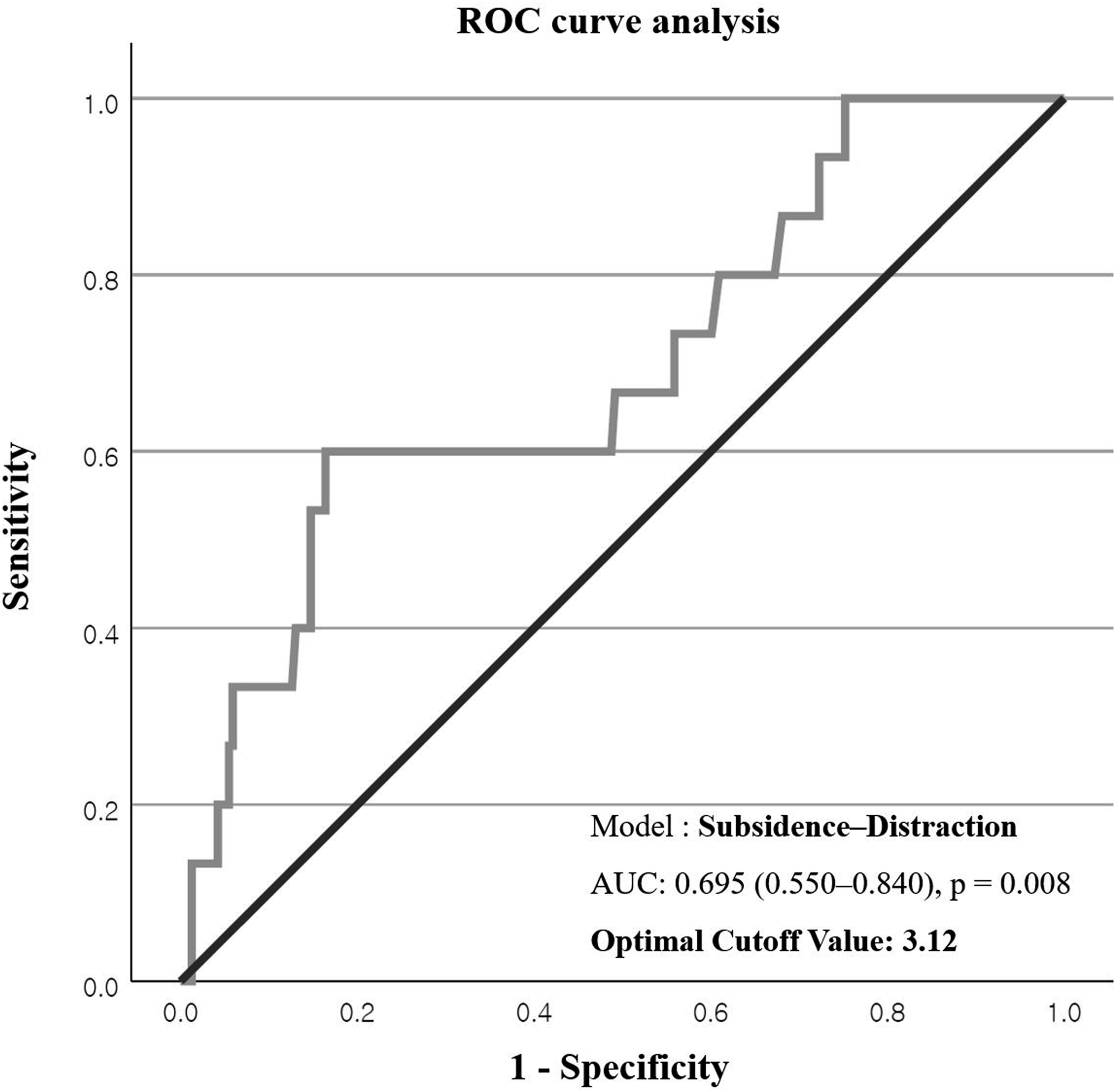
Discussion
This study assessed whether complications after ACDF—pseudarthrosis, subsidence, and loss of lordosis—were predicted by preoperative bone quality measured by CT HU over at least 5 years of follow-up. Cervical bone quality did not predict pseudarthrosis or subsidence, but lower HU values were associated with postoperative loss of cervical lordosis. Immediate postoperative segmental lengthening—used as a surrogate for intraoperative distraction—was associated with subsidence; a threshold of approximately 3 mm may guide operative planning. Overall, these findings highlight that differences in cervical and lumbar biomechanics warrant region-specific interpretation of bone quality.
Although lumbar fusion studies consistently linked osteoporosis-related bone quality to adverse outcomes and implant complications,4-6 recent cervical studies report no significant association between bone quality and pseudarthrosis or subsidence after ACDF.15-17 These findings support this site-specific distinction. Cadaveric studies by Schröder et al showed that cervical vertebrae have thicker, denser trabeculae and less age-related trabecular loss than lumbar counterparts.18,19 MRI-based vertebral bone quality studies similarly reveal distinct bone-quality profiles between the cervical and lumbar regions. 39 These microarchitectural features likely increase load-bearing capacity per unit area, suggesting greater cervical spine resilience to postoperative mechanical failure, even in osteoporotic bone.
Mechanically, ACDF involves a short moment arm between the plate and the fusion interface (cage–endplate), and the plate acts as a tension band limiting micromotion at the interbody surface.40-42 In contrast, posterior lumbar constructs have longer distances between pedicle screw–rod anchors and the fusion segment, transmitting greater bending moments to the anterior column under similar loads.43,44 These structural differences may explain why reduced bone quality does not directly lead to higher pseudarthrosis or subsidence rates following ACDF (Figure 7). Moment-arm contrast between ACDF and posterior lumbar constructs.
In this cohort, pseudarthrosis, subsidence, and loss of lordosis had limited effects on clinical outcomes, including pain scales and NDI. Notably, 67.1% of pseudarthroses identified at 2 years achieved delayed union by final follow-up, consistent with previous ACDF reports.20,32 Although the subsidence group had a higher revision rate, interpretation is limited by the small subgroup size (n = 15) and the few revision events. Revision rates did not differ significantly when outcomes were stratified by pseudarthrosis or loss of lordosis. Overall, the anatomic advantages of the cervical spine and the stability provided by the short moment arm in ACDF may mitigate both the incidence and clinical impact of mechanical complications, even in patients with low bone quality.
CT HU-based bone quality did not meaningfully predict pseudarthrosis or subsidence, suggesting that bone quality alone may be insufficient as a rationale to avoid ACDF. In clinical practice, low bone quality identified by screening measures (eg, BMD) should not, by itself, justify forgoing an anterior approach (potential undertreatment) or planning overly extensive combined procedures (potential overtreatment). In additional analyses, very low HU (≤231.5) was associated with an increased risk of postoperative loss of lordosis. The prevalence of HU ≤ 231.5 was higher in the loss subgroup, and a significant association was observed in univariable regression; however, this association was not retained after multivariable adjustment, suggesting limited independent predictive value. Few studies have directly linked preoperative bone-quality metrics to postoperative loss of lordosis after ACDF. These findings indicate that bone quality is more closely associated with alignment maintenance than traditional mechanical complications. Because postoperative loss of lordosis is strongly influenced by baseline alignment and extent of alignment correction, bone quality may be most appropriately interpreted alongside alignment-related variables rather than as a stand-alone metric.
Excessive segmental lengthening was associated with increased subsidence risk, consistent with previous studies30,45; this study corroborates that association in a large cohort and identifies a threshold around 3 mm (3.12 mm). Limiting segmental lengthening relative to preoperative disc height to approximately 3 mm may serve as a pragmatic guardrail to mitigate subsidence risk. Because higher BMI also independently predicted subsidence in this cohort, this threshold may be particularly relevant for patients with high BMI. However, univariable analyses suggested a directional trade-off in which smaller segmental lengthening was associated with more frequent loss of lordosis, indicating that the 3-mm threshold is best viewed as a guide to avoid excessive distraction rather than a universal rule for all patients. Accordingly, flexible application tailored to individual alignment, target correction, and clinical necessity may be required, and further studies are needed to refine distraction strategies that balance these competing risks.
Limitations
This study has several limitations. First, although the sample size was large and the follow-up was long-term, the retrospective design could not eliminate selection bias. Second, because the study was conducted at a single center, its findings may have limited generalizability. Third, although DXA-derived BMD is a widely used index of bone quality, it is not routinely obtained in cervical surgery candidates; therefore, it was not included in the analyses. Fourth, adjacent segment degeneration, an important long-term complication, was not systematically assessed, precluding evaluation of its relationship with bone quality and postoperative alignment. Finally, the study design did not allow determination of the temporal sequence among pseudarthrosis, subsidence, and loss of lordosis, precluding causal inference; future prospective studies are needed to clarify these relationships.
Conclusion
In this 5-year longitudinal cohort, preoperative CT HU did not predict pseudarthrosis or subsidence after ACDF. Very low HU (≤231.5) was associated with postoperative loss of lordosis in univariable analysis, but did not retain independent predictive value after multivariable adjustment. Notably, these complications had limited impact on 5-year patient-reported outcomes. Immediate postoperative segmental lengthening (a surrogate of intraoperative distraction), and higher BMI independently increased cage subsidence risk, whereas multilevel surgery independently predicted pseudarthrosis. These findings indicate that bone quality in the cervical spine should be interpreted differently from that in the lumbar spine, particularly with respect to mechanical failure. Accordingly, bone quality alone should not be used as a primary rationale to avoid ACDF. A pragmatic guardrail of approximately 3 mm of segmental lengthening relative to preoperative disc height may help mitigate subsidence risk.
Supplemental Material
Supplemental Material - Does Bone Quality Predict Pseudarthrosis, Subsidence, or Loss of Lordosis After Anterior Cervical Discectomy and Fusion? Minimum 5-Year Cohort Study
Supplemental Material for Does Bone Quality Predict Pseudarthrosis, Subsidence, or Loss of Lordosis After Anterior Cervical Discectomy and Fusion? Minimum 5-Year Cohort Study by San Kim, MD, Sehan Park, MD, PhD, Dong Ki Ahn, MD, PhD, Dong-Ho Lee, MD, PhD, Gumin Jeong, MD, Ki Chol Park, MD, Yong Kim, MD, and Changmin Choi, MD, PhD in Global Spine Journal
Footnotes
Ethical Considerations
This retrospective study was approved by the Institutional Review Board of the participating institution (IRB approval number: 2025-07-009).
Consent to Participate
Informed consent was waived because of the study’s retrospective design.
Author Contributions (CRediT)
Conceptualization: San Kim, Dong-Ho Lee.
Methodology: San Kim, Dong Ki Ahn, Ki Chol Park.
Formal analysis: San Kim, Sehan Park.
Investigation: San Kim.
Data curation: San Kim, Sehan Park, Gumin Jeong, Ki Chol Park, Yong Kim, Changmin Choi.
Validation: Sehan Park, Dong-Ho Lee.
Visualization: Changmin Choi.
Project administration: Dong Ki Ahn, Dong-Ho Lee.
Funding acquisition: San Kim.
Resources: Gumin Jeong.
Software: Yong Kim.
Supervision: Dong Ki Ahn, Dong-Ho Lee.
Writing – original draft: San Kim.
Writing – review & editing: Sehan Park, Dong-Ho Lee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from Jeju National University Hospital in 2025 (grant number 2025-22).
Declaration of Conflicting Interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.