
Abstract
Study Design
Retrospective cohort study.
Objectives
To compare 5-year clinical and radiographic outcomes between single-level Bryan and ProDisc-C cervical disc arthroplasty (CDA).
Methods
Patients undergoing single-level Bryan or ProDisc-C arthroplasty for cervical spondylosis radiculopathy and/or myelopathy between March 2004 and August 2014 were enrolled. Clinical outcomes included Visual Analog Scales for arm/neck pain (VAS-A/N), Neck Disability Index (NDI), and modified Japanese Orthopedic Association (mJOA) scores. Radiographic evaluation included cervical lordosis, range of motion (ROM), functional spinal unit (FSU) height, cervical sagittal vertical axis (cSVA), T1 slope, heterotopic ossification (HO), and adjacent segment degeneration (ASD). Evaluations were performed preoperatively and postoperatively within 3 months, 1 year and 5 years.
Results
Among 113 patients with 5-year follow-up (51 Bryan, 62 ProDisc-C), both groups showed significant improvements in VAS-N, VAS-A, NDI, and mJOA scores at all timepoints (all P < .001). No significant intergroup differences were detected between the two cohorts at baseline (all P > .05). ROM and cervical alignment remained stable in both cohorts. Compared to Bryan arthroplasty, ProDisc-C demonstrated greater index-level segmental lordosis (4.3° ± 5.0° vs 1.2° ± 4.7°; P = .001), more FSU height restoration (35.2 ± 3.4 mm vs 32.9 ± 3.6 mm; P < .001), and less segmental kyphosis incidence (21.0% vs 39.2%; P = .032). However, ProDisc-C arthroplasty had higher rates of ASD (58.1% vs 37.3%; P = .028) and HO (67.7% vs 33.3%; P < .001).
Conclusion
Both prostheses achieved comparable 5-year clinical outcomes. ProDisc-C arthroplasty better maintained cervical sagittal alignment, whereas Bryan arthroplasty demonstrated lower ASD and HO incidence.
Keywords
Introduction
Cervical disc arthroplasty (CDA) has emerged as a motion-preserving surgical alternative to anterior cervical discectomy and fusion (ACDF) for treating cervical degenerative disc disease (CDDD). Over the past decade, accumulating evidence has established CDA is a safe and effective operation.1-3 Comparative studies have consistently demonstrated that CDA achieves comparable or superior clinical outcomes to ACDF, including significant pain relief and functional improvement, while significantly reducing the incidence of symptomatic adjacent segment degeneration (ASD).4-6
Multiple CDA prostheses with distinct structural designs are currently available in the global market, each offering unique biomechanical characteristics and theoretical advantages for clinical applications. 7 Nowadays, various device designs have been approved by the Food and Drug Administration (FDA) in the United States. 8 The Bryan (Medtronic Sofamor Danek, Memphis, TN) and ProDisc-C (Centinel Spine, West Chester, PA) cervical disc prostheses are two typical FDA-approved devices, serving as prototypical examples of first-generation unconstrained and constrained designs, respectively. Numerous studies have documented the clinical and radiographic outcomes following Bryan or ProDisc-C arthroplasty across various follow-up periods.9-14 Most recently, 20-year radiographic follow-up data for the Bryan prosthesis have been reported in the literature. 15 It is well recognized that the design of cervical disc prostheses, including structural design and material properties, plays a critical role in postoperative cervical kinematics and biomechanics.16,17 Understanding the design-specific advantages and limitations of different prostheses can provide valuable scientific guidance for surgical decision-making and prosthesis selection. However, few studies have directly compared these distinct prosthesis designs within a single study. This paucity of comparative data limits evidence-based understanding of how implant design characteristics influence postoperative outcomes.
The purpose of this study was to compare 5-year clinical and radiographic outcomes between single-level Bryan and ProDisc-C arthroplasty, and to evaluate the influence of prosthesis design on these outcome measures.
Methods
Study Design
This single-center retrospective observational study received ethical approval from the Institutional Review Board of the Peking University Third Hospital (IRB Approval No.: M20241093). The patients with single-level cervical spondylosis radiculopathy and/or myelopathy, who were treated with a Bryan or ProDisc-C prosthesis between March 2004 and August 2014, were consecutively included in this study.
Patient Selection
Patient inclusion criteria were CDDD at one level of C3-C7 leading to radiculopathy and/or myelopathy, showed no improvement after at least 12 weeks of conservative treatment, unless immediate surgical intervention was required (eg, severe myelopathy). Exclusion criteria were previous cervical spine surgery, ossification of the posterior longitudinal ligament, severe osteoporosis or osteoarthritis, obvious cervical instability, cervical deformity, trauma, tumor, infection, and history of neuromuscular diseases such as motor neuron disease.
Surgery and Follow-Up
All procedures were performed by two experienced senior surgeons under identical conditions, using general anesthesia and supine position through a standard anterior approach according to Smith-Robinson. Prosthesis selection was based on device availability, surgeon preference, and patient choice when applicable. A complete and accurate decompression was obtained during surgery. Each patient was followed up with preoperative and regular postoperative evaluations for 3 months, 1 year, and 5 years. Clinical and radiological outcome parameters were collected preoperatively and at each postoperative time point.
Clinical Evaluation
Clinical outcomes were determined using self-assessment questionnaires, including the 10-point Visual Analog Scale (VAS-A) for arm pain and (VAS-N) for neck pain, the Neck Disability Index (NDI), and modified Japan Orthopedic Association (mJOA) scores.
Radiological Evaluation
Radiographic outcomes were evaluated by lateral static and dynamic flexion-extension lateral images (Figure 1), including segmental and global cervical lordosis (CL), total ROM, and segmental ROM at the index and adjacent levels, functional spinal unit (FSU) segment height and adjacent level disc height, cervical sagittal vertical axis (cSVA), T1 slope, ASD, and heterotopic ossification (HO). The disc height was calculated as the mean of the anterior, middle, and posterior intervertebral disc space on neutral lateral X-ray.
18
HO was classified grades I to IV according to McAfee’s classification.
19
Intervertebral disc degeneration was assessed using Walraevens’ scoring system, which classifies severity into three grades (mild, moderate, and severe) based on cumulative scores for height loss, anterior osteophytes, and endplate sclerosis.
20
A diagnosis of developed ASD is made when the total postoperative degeneration score increases by ≥1 point compared to the preoperative baseline. Measurement of radiological parameters. (A) Pre-operative neutral lateral radiographs, (B) post operative neutral lateral, (C) extension, and (D) flexion radiographs. GCL, global cervical lordosis; SCL, segmental cervical lordosis; SADH, disc height of superior adjacent level; IADH, disc height of inferior adjacent level; FSUDH, disc height of functional spinal unit; TROM, total range of motion; SROM, segmental ROM at index level; SAROM, superior adjacent ROM; IAROM, inferior adjacent ROM
Statistical Analysis
Continuous variables are presented as means ± standard deviations (SD), and categorical variables are presented as frequencies and percentages. Continuous variables were analyzed using independent samples t-tests for between-group comparisons and paired samples t-tests for pre-vs post-operative comparisons within the same group. Chi-square test was used to compare categorical variables, and Fisher’s exact test was employed if any expected cell count was less than 5. Statistical analyses were conducted using SPSS 23.0 software (IBM Corp., Armonk, NY, USA) by an investigator who was not involved in the data collection. Statistical significance was set at P < .05.
Results
Patient Demographic
Demographic and Clinical Preoperative Characteristics
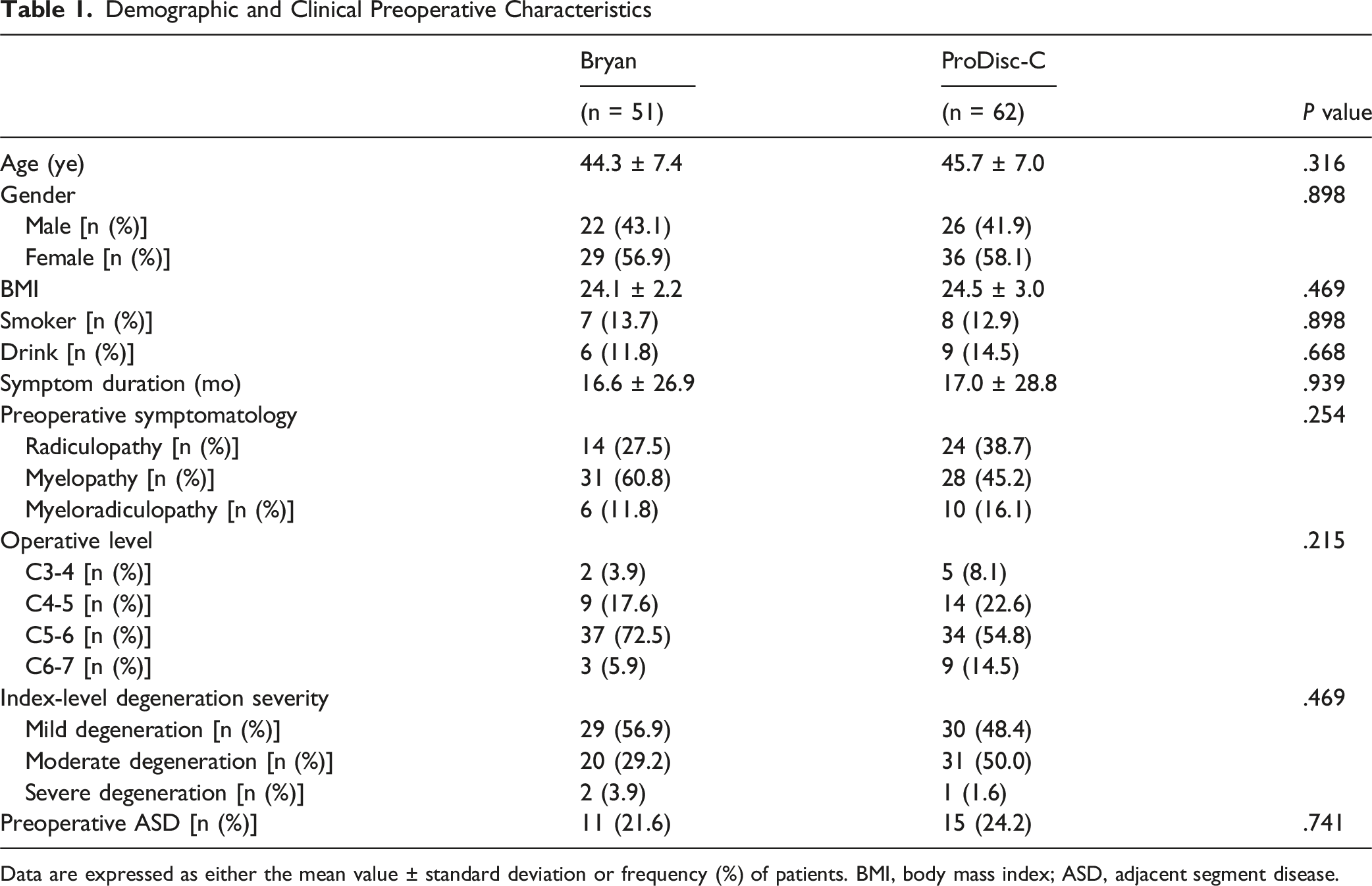
Data are expressed as either the mean value ± standard deviation or frequency (%) of patients. BMI, body mass index; ASD, adjacent segment disease.
Clinical Outcomes
The Improvement of Clinical Outcomes Between Bryan and ProDisc-C Prosthesis
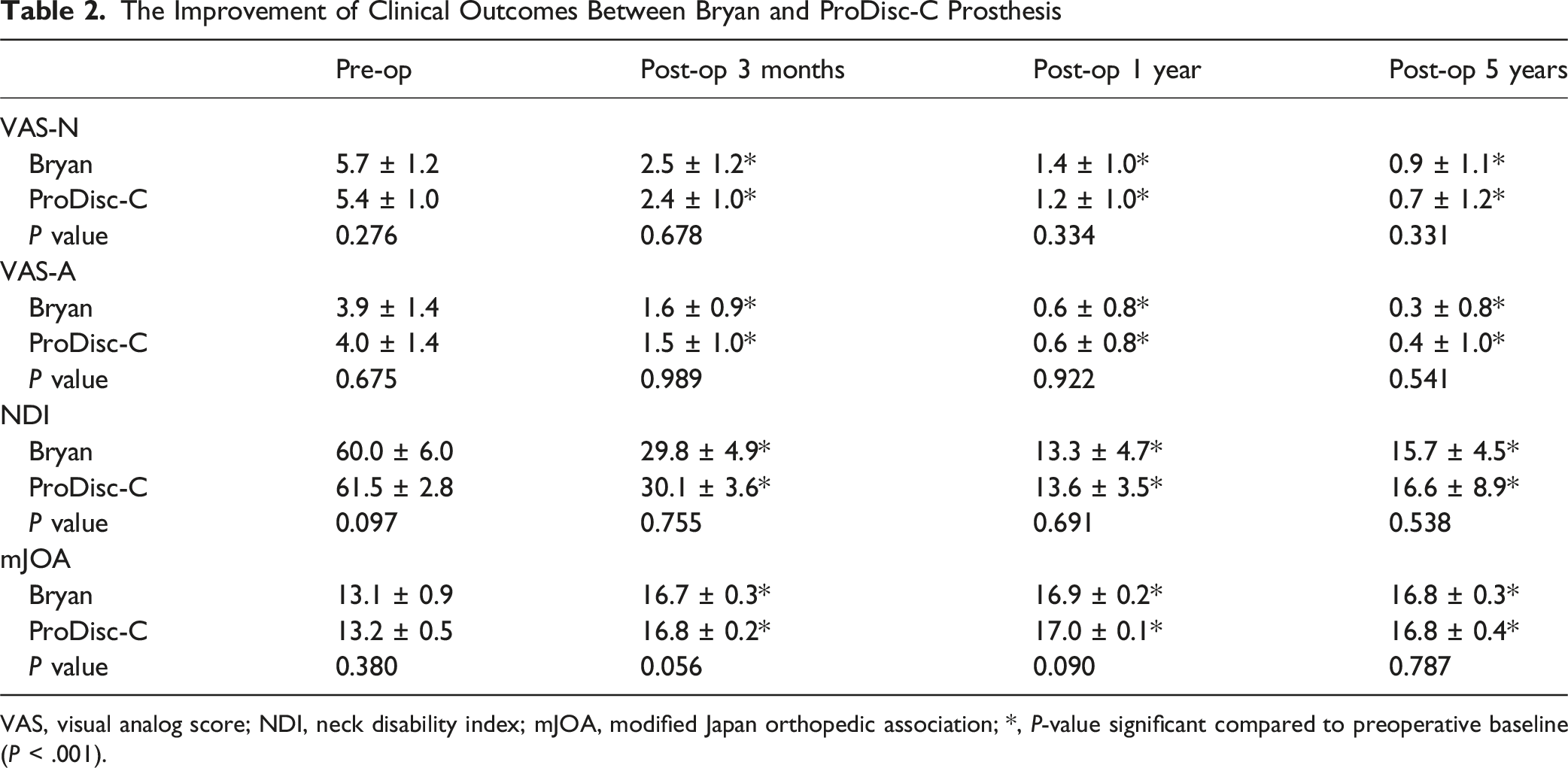
VAS, visual analog score; NDI, neck disability index; mJOA, modified Japan orthopedic association; *, P-value significant compared to preoperative baseline (P < .001).

The improvement of clinical outcomes between Bryan and ProDisc-C prostheses. (A) VAS-N; (B) VAS-A; (C) NDI; (D) mJOA. * indicates P-value significant compared to preoperative baseline (P < .001)
Radiological Outcomes
Comparison of Radiographic Parameters Preoperatively and at Each Postoperative Time Points
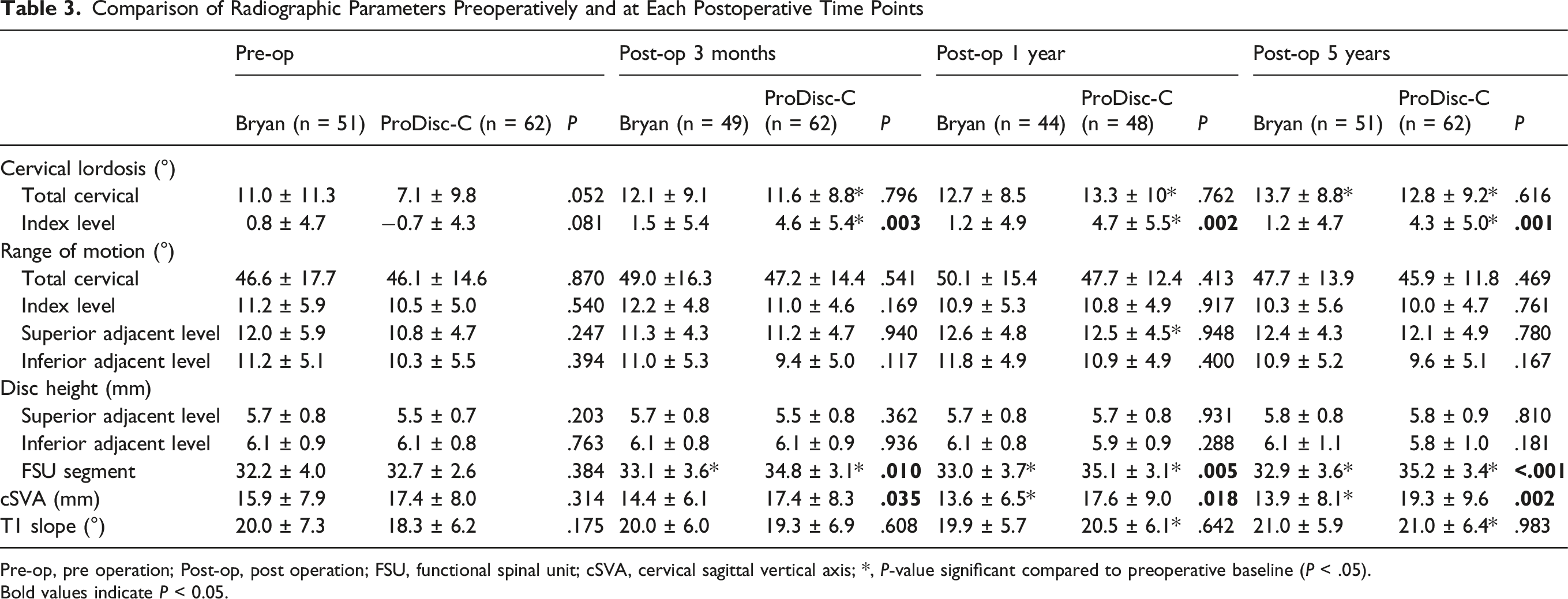
Pre-op, pre operation; Post-op, post operation; FSU, functional spinal unit; cSVA, cervical sagittal vertical axis; *, P-value significant compared to preoperative baseline (P < .05).
Bold values indicate P < 0.05.
The ROM of the index level, adjacent levels and overall cervical spine were well maintained from pre-operation to the 5-year follow-up in both CDA groups (Table 3; Figure 3A-B). Intergroup comparisons of global and segmental ROM demonstrated no significant variations between the Bryan and ProDisc-C cohorts at baseline or during the follow-up period (all P > .05). Comparison of radiographic parameters preoperatively and at each postoperative time points. (A) Total CL; (B) Index-level segmental alignment; (C) cSVA; (D) T1 slope. * indicates P-value significant compared to preoperative baseline (P < .05). # indicates significant intergroup differences between two groups (P < .05)
Following Bryan arthroplasty, both global cervical lordosis and index-level segmental alignment well maintained throughout the follow-up period (Figure 3C-D). Notably, a statistically significant improvement in overall cervical curvature was demonstrated at the 5-year postoperative evaluation (11.0° ± 11.3° at baseline vs 13.7° ± 8.8° at 5-year follow-up; P < .05). Differently, the ProDisc-C group exhibited significant increases in these parameters, with statistically different index-level segmental alignment at 3-month (Bryan 1.5° ± 5.4° vs ProDisc-C 4.6° ± 5.4°; P = .003), 1-year (Bryan 1.2° ± 4.9° vs ProDisc-C 4.7° ± 5.5°; P = .002), and 5-year follow-ups (Bryan 1.2° ± 4.7° vs ProDisc-C 4.3° ± 5.0°; P = .001). At 5-year follow-up, segmental kyphosis developed in 20 (39.2%) Bryan arthroplasty patients and in 13 (21.0%) ProDisc-C arthroplasty patients, with mean kyphosis angles of −3.6° ± 3.2° and −2.5° ± 1.5°, respectively. Significant intergroup differences existed in segmental kyphosis incidence (P = .032).
Both Bryan and ProDisc-C arthroplasty demonstrated significant increases in FSU height (Figure 4), with ProDisc-C showing greater height restoration at 3-month (Bryan 33.1 ± 3.6 mm vs 34.8 ± 3.1 mm ProDisc-C; P = .010), 1-year (Bryan 33.0 ± 3.7 mm vs ProDisc-C 35.1 ± 3.1 mm; P = .005), and 5-year follow-ups (Bryan 32.9 ± 3.6 mm vs ProDisc-C 35.2 ± 3.4 mm; P < .001). Comparison of functional spinal unit (FSU) segment height preoperatively and at each postoperative time points. * indicates P-value significant compared to preoperative baseline (P < .05). # indicates significant intergroup differences between two groups (P < .05)
The cSVA significantly decreased from 15.9° ± 7.9° at baseline to 13.9° ± 8.1° at 5-year follow-up in Bryan group (Figure 3E; P = .047). Inversely, the ProDisc-C group exhibited significant increases in cSVA, with statistically different at 3-month (Bryan 14.4° ± 6.1° vs ProDisc-C 17.4° ± 8.3°; P = .035), 1-year (Bryan 13.6° ± 6.5° vs ProDisc-C 17.6° ± 9.0°; P = .018), and 5-year follow-ups (Bryan 13.9° ± 8.1° vs ProDisc-C 19.3° ± 9.6°; P = .002).
The T1 slope of cervical spine was maintained from pre-operation to the 5-year follow-up in Bryan group (Figure 3F; all P > .05). Meanwhile, the T1 slope significantly increased from 18.3° ± 6.2° at baseline to 21.0° ± 6.4° at 5-year follow-up in ProDisc-C group (P < .001).
Comparison of Developed Adjacent Segment Disease (ASD) Between Bryan and ProDisc-C Prosthesis
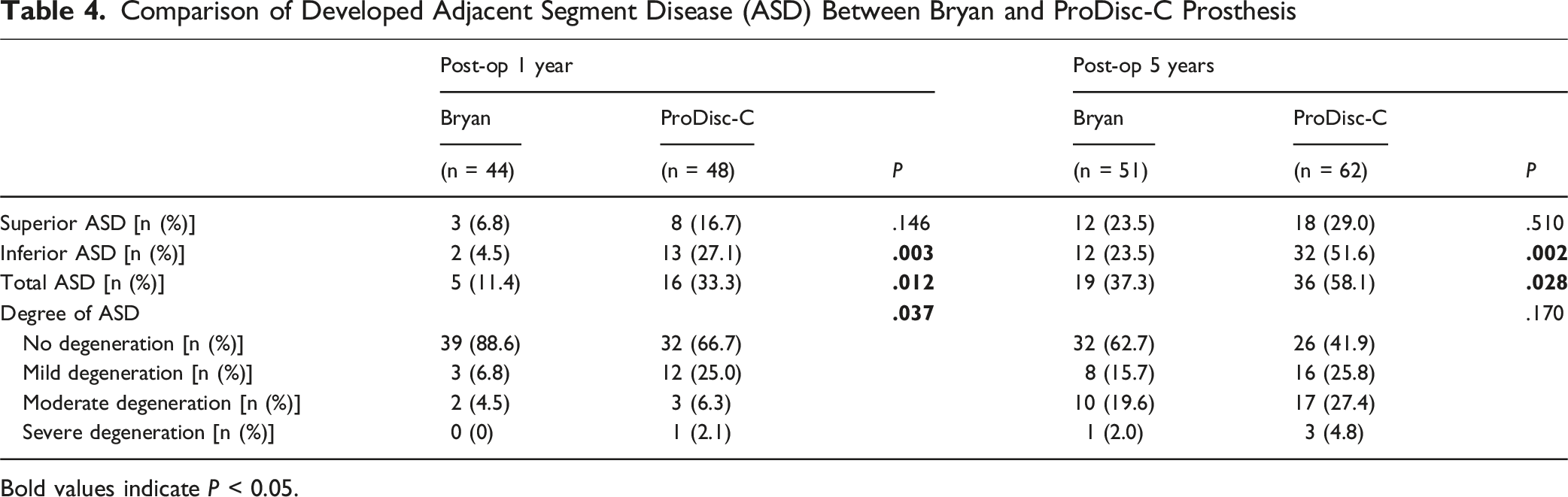
Bold values indicate P < 0.05.

Comparison of adjacent segment disease (ASD) between Bryan and ProDisc-C Prostheses. (A) Prevalence rate of ASD; (B) Degree of ASD. * indicates significant intergroup differences between two groups (P < .05)
Comparison of Heterotopic Ossification (HO) Between Bryan and ProDisc-C Prosthesis
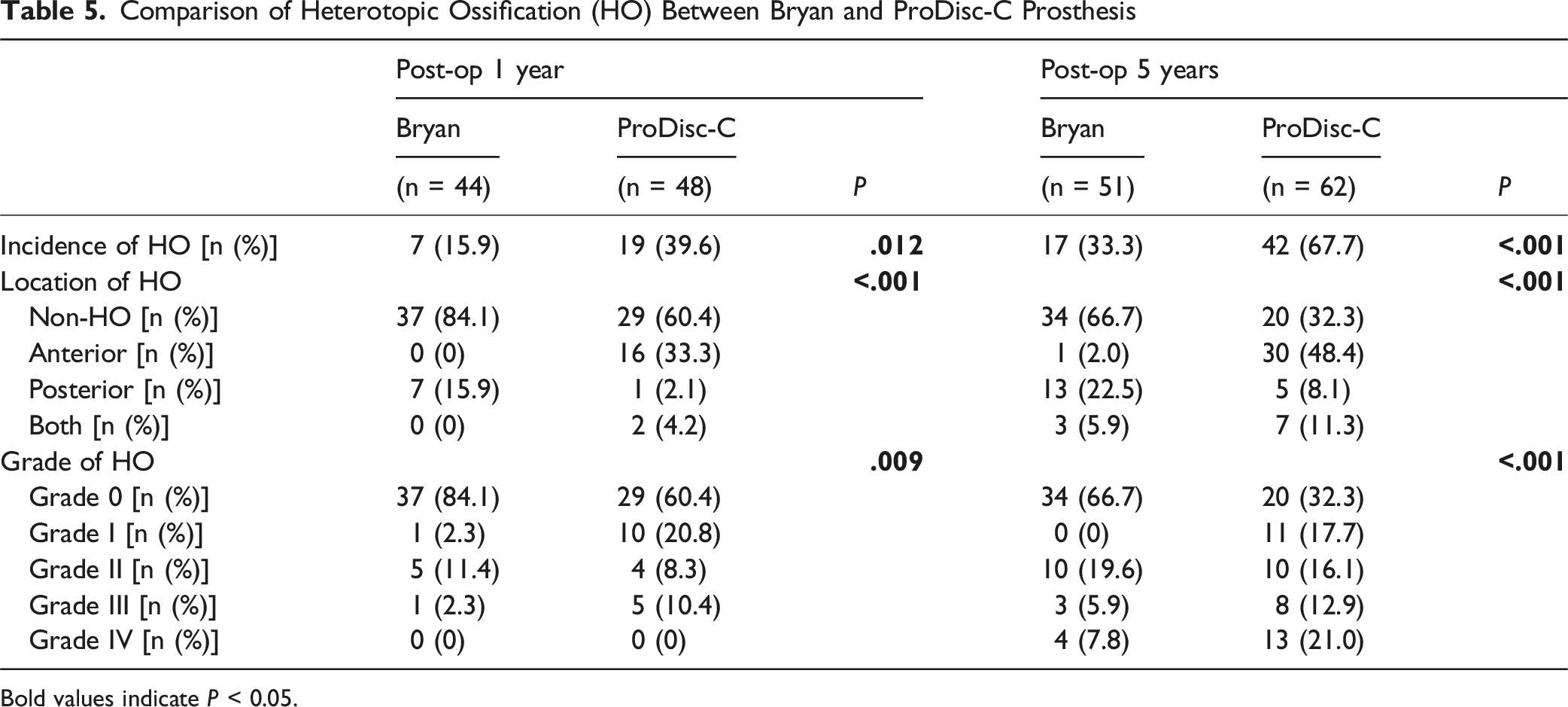
Bold values indicate P < 0.05.

Comparison of heterotopic ossification (HO) between Bryan and ProDisc-C Prostheses. (A) Prevalence rate of HO; (B) Grade of HO. * indicates significant intergroup differences between two groups (P < .05)
Discussion
This study represents the first comparative analysis of 5-year clinical and radiographic outcomes between two predominant FDA-approved CDA devices (Bryan and ProDisc-C prostheses). Overall, our findings indicate both implants provide comparable, favorable long-term clinical outcomes with preserved segmental mobility. However, significant inter-device differences were observed in cervical sagittal alignment maintenance, ASD incidence, and HO development.
Clinical Outcomes
Both Bryan and ProDisc-C arthroplasty have demonstrated favorable clinical outcomes in previous studies.21-24 Our study confirms significant postoperative improvement in both cohorts (Figure 2), consistent with established evidence. Crucially, adequate neural decompression (spinal cord and nerve roots) underpins successful clinical outcomes following CDA. 13 Adequate intraoperative decompression reduces neck/arm pain and improves neurological function, accounting for similar outcomes between groups. Notably, other disc prostheses likewise achieve satisfactory results when decompression is achieved.5,25-27
Range of Motion
CDA were designed to preserve index-level motion while preventing adjacent segment hypermobility. Our findings confirm that both Bryan and ProDisc-C arthroplasty maintain overall and segmental ROM without increasing adjacent-level ROM through 5-year follow-up (Table 3). Sasso et al 28 reported the index-level ROM of single-level Bryan arthroplasty slightly increased from 6.5° at baseline to 8.0° at 2 years and 8.5° at 4-year follow-up. Similarly, Lavelle et al 10 documented ROM progression from 6.5° at baseline to 8.1° at 1 year, 8.5° at 5 years, and 8.7° at 10-year follow-up. Zigler et al 29 observed ROM maintenance of single-level ProDisc-C arthroplasty with 8.5° preoperatively vs 8.1° at 5-year follow-up. Contrastingly, Goffin et al 30 reported decreased ROM after single-level Bryan arthroplasty (9.3° preoperatively to 7.3° at 4 years), aligning with our earlier observations.11,12,14 Previous study identified strong associations between ROM reduction and HO formation. 31 Therefore, initially broader surgical indications may increase incidence of high grade HO, which may subsequently compromise postoperative ROM. Although our current study showed no significant differences of ROM vs preoperative baselines, a declining trend emerged (Figure 3A-B). Longer-term comparative studies are warranted to clarify ROM trajectories.
Cervical Alignment and Sagittal Balance
The normal cervical alignment is essential for physiological motion and load transmission. Inversely, cervical kyphosis creates a nonphysiological biomechanical environment by substantially elevating anterior column loading, disrupting normal load transmission, and accelerating degenerative changes.32-34 Thus, maintaining physiological cervical lordosis is objectives of CDA. This study found that the Bryan disc prosthesis maintained overall CL and segmental alignment postoperatively (Figure 3C-D). However, segmental kyphosis developed in 39.2% of Bryan group patients at 5-year follow-up, a rate significantly higher than that observed in the ProDisc-C group. The uniform anterior-posterior height design and compressible polymer core of the Bryan implant inherently limit its ability to correct cervical kyphosis, as demonstrated in multiple clinical studies.35-37 Although the ProDisc-C device is theoretically also limited in its capability, 16 our results demonstrate significant improvement in both overall and segmental cervical lordosis. This correction remained stable throughout the 5-year follow-up period, corroborating the findings of Colman et al. 38 The design of the ProDisc-C implant, comprising two cobalt–chromium-molybdenum endplates and an interposed, non-compressible ultra-high-molecular-weight polyethylene core, may contribute to mitigating the tendency towards segmental kyphosis. Furthermore, the significantly greater FSU height achieved in the ProDisc-C group compared to the Bryan group is likely another advantage attributable to the non-compressible polymer core. Given the influence of prosthesis design on postoperative cervical alignment, the Bryan implant may not be the most appropriate choice for patients with preexisting straightening or kyphotic alignment. In such cases, the ProDisc-C prosthesis appears to be a more suitable option. Therefore, the observed effect of implant type on sagittal alignment in this study provides an important consideration for patient selection.
Regarding sagittal alignment parameters, although the postoperative cSVA was significantly higher in the ProDisc-C group than in the Bryan group, both values remained within the normal range reported in the literature. 39 No significant difference in T1 slope was observed between the groups. These findings demonstrate that both Bryan and ProDisc-C prostheses can achieve favorable postoperative sagittal balance.
Adjacent Segment Degeneration
The primary objective of CDA implant design is to preserve segmental mobility, prevent hypermobility at adjacent levels, and thereby reduce the incidence of ASD. Several high-quality meta-analyses have consistently demonstrated a significantly lower ASD rate following CDA compared to ACDF.40-42 Further analysis reveals variations in ASD rates among different types of prostheses. At 5-year follow-up, Zhou et al. 31 reported an overall ASD rate of 22.6% after Bryan disc arthroplasty, while Zhao et al. 14 documented a rate of 36.7% for ProDisc-C. Dufour et al. 43 reported ASD rates of 39.1% at the cephalad level and 42.2% at the caudal level following Mobi-C implantation. Consistent with this, the current study observed a higher incidence of ASD and a greater proportion of moderate-to-severe degeneration in the ProDisc-C group compared to the Bryan group. Additionally, within the ProDisc-C group, ASD occurred more frequently at caudal levels than cephalad levels. A meta-analysis by Zavras et al. 44 demonstrated that prosthesis constraint affects clinical and radiographic outcomes, with unconstrained and semi-constrained designs associated with significantly lower ASD rates than ACDF, whereas constrained prostheses exhibited rates similar to those of ACDF. The author believes that long-term preservation of physiological dynamics following CDA may facilitate improved longitudinal patient outcomes, including a reduction in ASD incidence. 44 As a classic unconstrained prosthesis, the Bryan device can effectively preserve the physiological cervical motion pattern. 45 In contrast, the constrained design of the ProDisc-C can alter postoperative cervical kinematics, such as shifting the center of rotation anteriorly. 37 The kinematic advantages of mobile prostheses may explain the lower ASD rates observed following Bryan disc arthroplasty in this study. However, the underlying kinematic mechanisms warrant further investigation.
Heterotopic Ossification
HO is a common complication following CDA. Although some studies demonstrated that HO does not compromise clinical outcomes, higher-grade HO significantly reduces segmental ROM. 11 This altered mobility can modify adjacent segment stress distribution, potentially accelerating ASD. 46 Reported HO incidence varies considerably in the literature, influenced by factors such as patient demographics, prosthesis type, surgical level, perioperative management, follow-up duration, and evaluation methodology.47-49 In this study, baseline characteristics were comparable between groups. However, the incidence and grade of HO were substantially higher in the ProDisc-C group compared to the Bryan group at both 1-year and at 5-year follow-ups (Figure 6), consistent with previous findings.14,31,49 Notably, HO following Bryan arthroplasty predominantly occurred posteriorly, whereas ProDisc-C demonstrated a predilection for anterior HO development (Table 5). While the keel design of ProDisc-C prosthesis provides solid immediate stability, it causes greater endplate disruption. Furthermore, as a constrained device, ProDisc-C prosthesis does not replicate physiological motion patterns, potentially leading to abnormal bone-implant interface stress distribution. 50 The increased stress contributes to greater wear debris generation. In contrast, the mobile-core Bryan prosthesis, which is shielded by a polyurethane membrane, produces less debris and effectively isolates it from contact with vertebral tissues. 48 These structural characteristics may represent key contributors to the observed differences in HO incidence. 49 Further biomechanical investigations are warranted to elucidate the mechanisms underlying prosthesis-specific variations in HO formation.
Limitation
This study has certain limitations. First, ASD and HO were assessed using plain radiographs rather than magnetic resonance imaging or computed tomography, potentially underestimating the incidence of these complications. Nevertheless, the results remain valid as all radiographic measurements and evaluations were performed by a single experienced surgeon, and the use of radiographs alone for assessment is well-documented in the literature.12,15,38 Second, while this comparative study identified differences in radiographic outcomes between prosthesis types and provided a scientific analysis of potential kinematic and biomechanical mechanisms based on implant design and existing literature, further in-vivo or in-vitro investigations are still required to confirm these mechanisms. Finally, although this 5-year follow-up study comparing Bryan and ProDisc-C prostheses provides evidence regarding their influence on clinical and radiographic outcomes, future research should include a broader range of prosthesis types and longer-term follow-up data.
Conclusion
This comparative study confirmed comparable, favorable long-term clinical outcomes following the Bryan and ProDisc-C arthroplasty with preserved segmental mobility and sagittal balance. The ProDisc-C prosthesis demonstrated advantages in maintaining cervical sagittal alignment, while the Bryan prosthesis showed superiority in preventing ASD and HO. The results of this study have guiding value for patient selection. Future studies should determine how specific prosthesis design characteristics influence clinical and radiological outcomes through kinematic and biomechanical mechanisms. This understanding will inform evidence-based cervical disc prosthesis design and selection.
Footnotes
Author Note
The manuscript submitted does not contain information about medical device(s)/drug(s).
Acknowledgments
We acknowledge the statistical consultation provided by the Clinical Epidemiology Research Center of Peking University Third Hospital.
Ethical Considerations
This study is compliance with ethical standards and approved by Research Ethics Committee (IRB Approval Number: M20241093).
Consent to Participate
Written informed consent was obtained from individual or guardian participants.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Key Research and Development Program of China (2023YFC3604404), the Natural Science Foundation of Beijing, China (Grant No. L234060), and the Postdoctoral Fellowship Program (Grade C) of China Postdoctoral Science Foundation under Grant Number GZC20251443.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.