
Abstract
Study Design
Retrospective Cohort Study Objectives: Robot-assisted spine surgery (RASS) is a rapidly evolving technique with potential benefits for improving surgical outcomes. A number of studies on RASS learning curve have focused on early iterations of the Mazor robot. Limited research exists on the learning curve associated with using the Globus Medical ExcelsiusGPS® system. In this retrospective study, we aimed to evaluate the learning curve of RASS using the ExcelsiusGPS® system at a single institution.
Methods
A total of 95 patients (541 screws) who underwent RASS between 2021 and 2022 were included. Variables including operative time, robot registration time, screw placement time, fluoroscopy utilization, and complications were analyzed. Statistical analysis was performed using descriptive statistics and two-sample t-tests.
Results
The average operative time significantly decreased after the first 14 cases, indicating a learning curve. However, no significant improvement was observed in robot registration time. Notably, screw placement time significantly improved after approximately 13 cases. When controlling for the number of levels fused, the trends remained consistent.
Conclusions
Our study confirmed the presence of a learning curve in RASS using the ExcelsiusGPS® system and demonstrated rapid proficiency development. Our findings highlight the relatively quick learning curve of 1 RASS system.
Keywords
Introduction
Robot-assisted spine surgery (RASS) has gained popularity in recent years as a minimally invasive alternative to traditional open spine surgery.1,2 While the use of robotic technology in spine surgery has shown potential in improving surgical outcomes and minimizing patient risks, it is still a relatively new technology. As such, there is limited research on the learning curve associated with RASS. In their recent publication, Pennington et al 3 conducted a systematic review of learning curves in RASS and proposed a framework for incorporating this technology into residency curricula. The authors found that the learning curve is similar to that of other minimally invasive, non-robotic spine surgeries. 3 Given the potential benefits of this technology, understanding the learning curve for RASS is important in optimizing patient safety and surgical outcomes. However, despite numerous papers on learning curves in robotic surgery, most studies focused on the early Mazor system.
More recently, the ExcelsiusGPS® system (Globus, Audubon, Pennsylvania) has been approved for the US market. This system utilizes preoperative (CT or MRI) or intraoperative (CT or fluoroscopy) patient imaging to allow for comprehensive screw trajectory planning as well as real-time tracking with dynamic reference markers and camera feedback. This system has been shown to improve screw placement accuracy.4,5
However, there is limited literature on the ExcelsiusGPS® system. Only 3 studies have specifically investigated the learning curve for the ExcelsiusGPS® system.6-8 Among these studies, only 1 involved a relatively large patient sample size of more than 100 patients. 7 Notably, 1 of the papers failed to demonstrate any discernible learning curve associated with the use of the ExcelsiusGPS® system. 6 This information suggests that more research is needed to better understand the learning curves and proficiency development associated with this particular robotic surgery system. Hence, in our study, we aimed to expand upon prior findings by conducting an institutional retrospective analysis on the learning curve in robot-assisted spine surgery for the ExcelsiusGPS® system. By doing so, we aimed to contribute to best practices for the use of robotic technology in spine surgery and contribute to the growing body of literature on this topic. We hypothesized that there is a learning curve associated with the ExcelsiusGPS® system in particular, and that this curve is similar to that of other minimally invasive spine surgeries. Specifically, we predicted that surgical outcomes, such as operative time, will improve as surgeons gain experience with the technology.
Method
A retrospective, institutional review board-exempt review was conducted to analyze all cases of navigated RASS during 1 full academic year using the ExelsiusGPS system at a single, high-volume academic institution. The study period spanned from the academic year 2021 to 2022. All cases of RASS with the ExelsiusGPS system were done by 1 senior attending surgeon during the specified timeframe were included in this study. The attending surgeon has accrued over 27 years of experience in spinal surgery and has performed hundreds of robotic-assisted surgery since the dawn of this technology.
Patient demographic information, such as age at the time of the surgical procedure, sex, body mass index, diagnosis, and spinal pathology, was collected from a review of electronic medical records (EMR). Additional data were collected from the RASS planning software and intraoperative 3-dimensional (3D) imaging. Operative data, including the number of operative levels, operative time, surgical complications were recorded from the EMR as well. All cases were assisted by a surgical fellow. Spine fellows participated in screw placement with attending supervision.
Surgical workflow has been discussed in a previous publication from our institution.
9
Please also see Figure 1. In brief, all patients underwent the preoperative CT protocol; patients were placed in the prone position; reference markers were placed in each posterior superior iliac spine, and the fluoroscopy registration fixture was attached to an image intensifier; after obtaining and confirming accuracy of the fluoroscopic images with respect to preoperative CT imaging, the robot was draped sterilely and brought into the surgical field. The robotic arm then guided the end effector/surgeon to the planned screw trajectory, with real-time visualization during screw placement. (A) Intraoperative positioning of the patient, robot, and surgeon/staff (reproduced from globus medical with permission). (B) Intraoperative screw placement with the robotic arm. Screw placement is overlayed on preoperative CT scan (reproduced from Jain et al
9
with permission).
The variables of interest in this study encompassed various aspects of robot-assisted surgery. First, total surgery time was recorded to understand the overall utilization of the robotic system during the surgical procedures. Robot registration/system setup time, which is less commonly studied with only a few articles focusing on it, was investigated as well. Robot registration time included draping the robot, draping the X-ray machine, getting the robot in position, taking X-rays for registration, performing registration, and verifying registration. This was measured as the time from the first incision for the reference array/quatro spike to first incision for pedicle screw. Screw placement time, which has been extensively examined in previous studies, was analyzed to evaluate the time taken to accurately position the screws. Fluoroscopy utilization was collected, measured in terms of total radiation dosage in mGy. Lastly, complications and the need for return to the operating room were monitored to assess the occurrence of adverse events and postoperative challenges.
Statistical Analysis
Descriptive statistics were used to summarize the collected data. Quantitative variables were reported as means, while categorical variables were reported as frequencies and percentages. Two-sample t test was performed comparing each these parameters. Statistical significance was set at P < .05.
Results
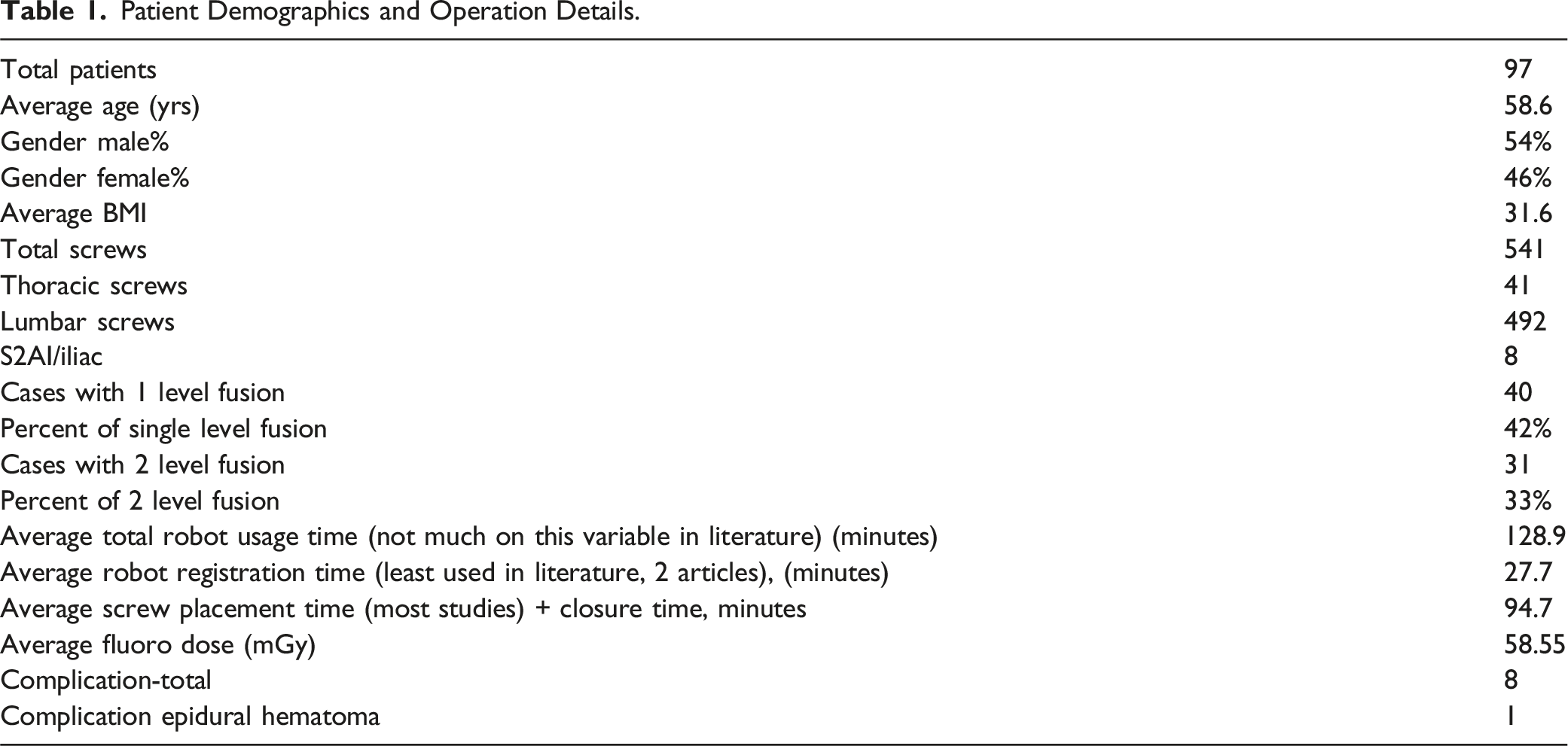
Patient Demographics and Operation Details.
Comparing Total Case Numbers
A total of 541 screws were placed. The great majority (492) were lumbar screws. 41 were thoracic while 8 were S2AI/ILIAC screws. All screws were placed as a supplement to an interbody implant. Interbodies were placed through the anterior, posterior or lateral approach. From existing literature, a wide variety of numbers were quoted for proficiency. Some studies used screw numbers while others used case numbers. Since we used surgery time as our variable studied, we decided to use case number instead of number of screws placed. Generally in the literature, numbers needed to be proficient ranged from 3 to 30 cases. 3
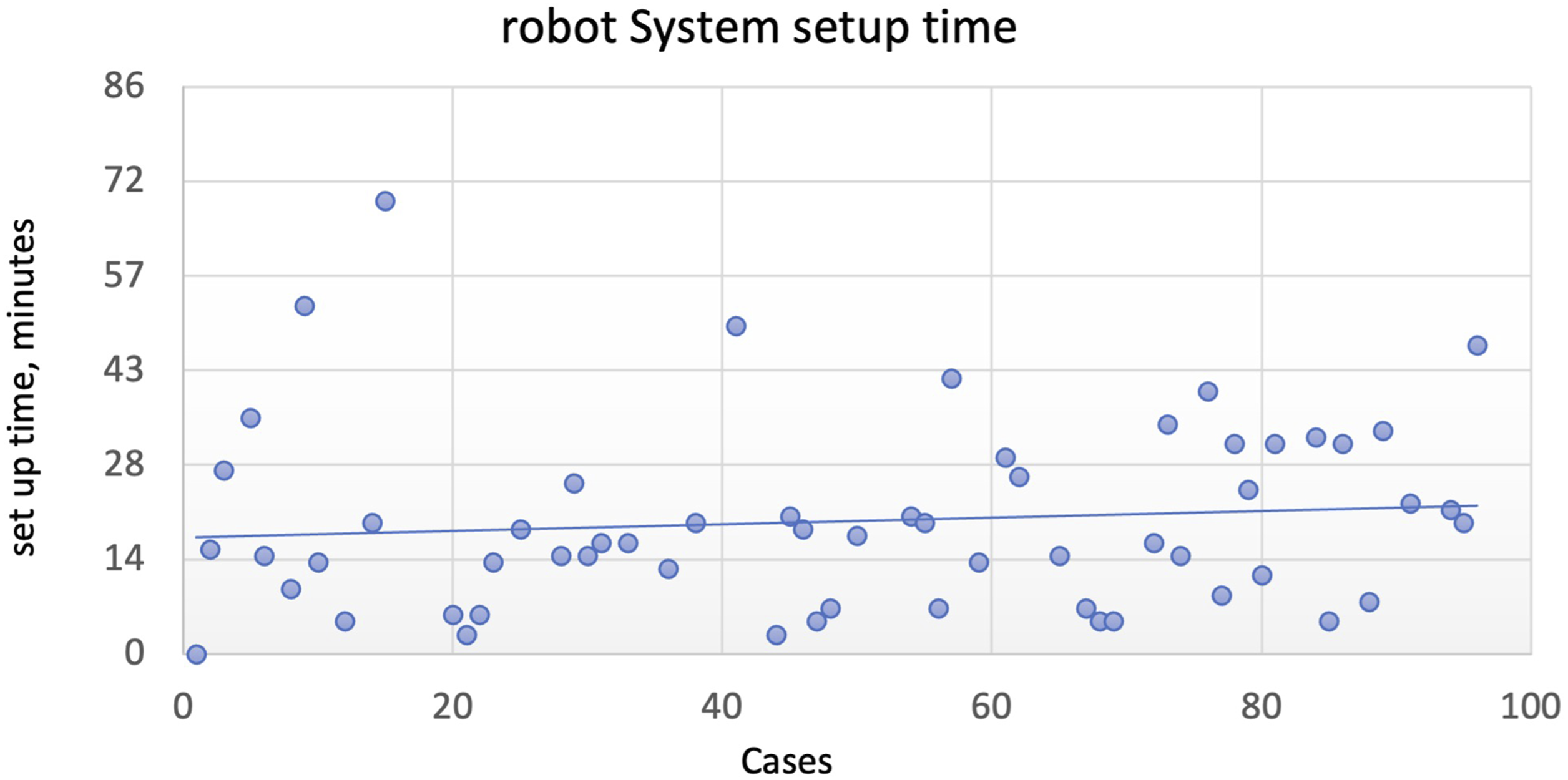
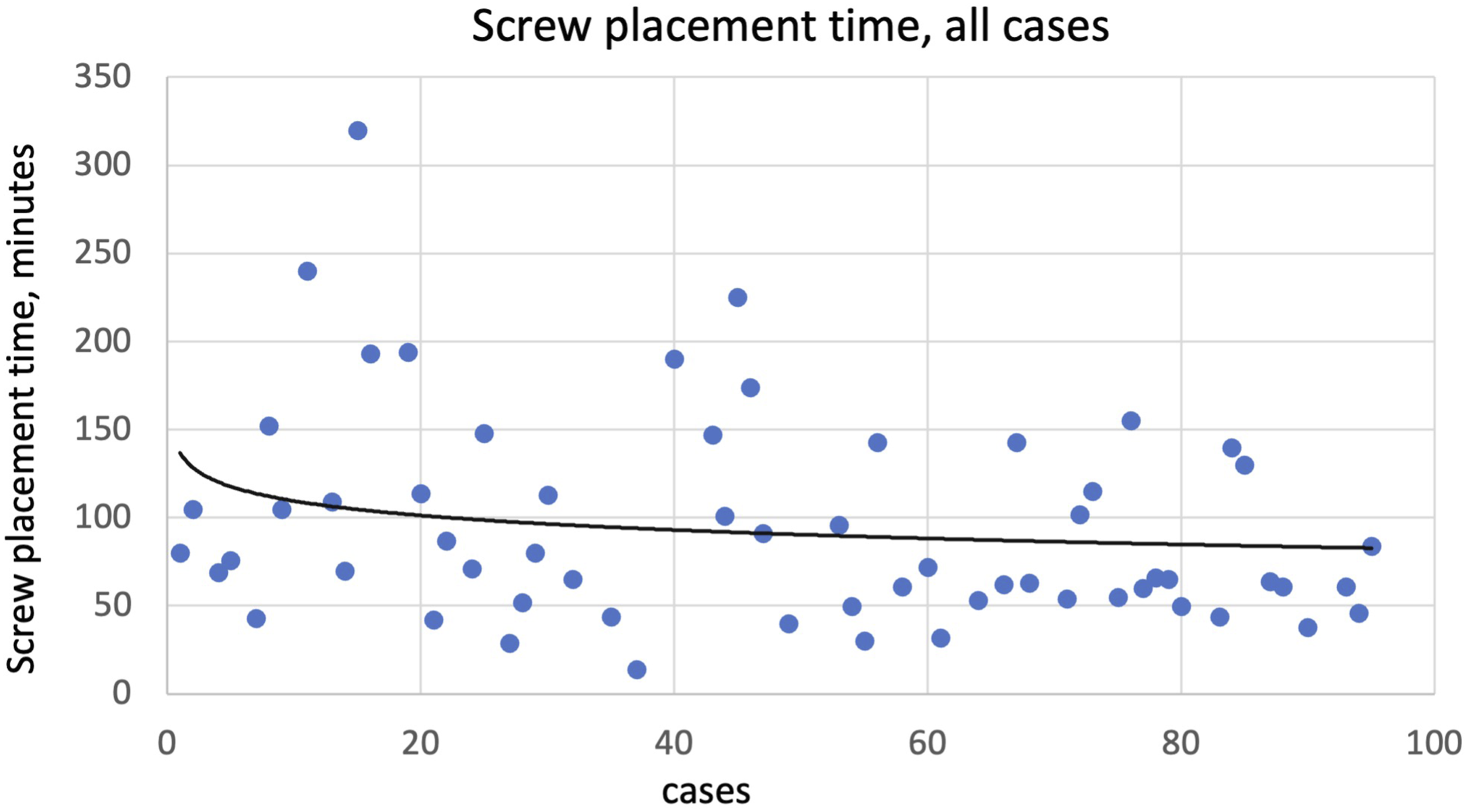
Total case time was plotted in Figure 2. We performed statistical analysis between operative time for the first 30 cases and that of the remaining cases and found it to be statistically significant (P = .01). Average time for the first 30 cases was 165 min, while that of the remaining was 112 min. We then tried to use different case number cutoffs to find at which point did it become statistically significant. We found that at case #14, the statistical significance disappeared (P = .11). We then did the same with registration time (Figure 3) and screw placement time (Figure 4) respectively. Interestingly, we found no statistical significance with registration time at any case cutoff (all P > .05). When comparing screw placement time, statistical significance was reached around case 13 (P = .03). Average time for the first 13 cases was 135 min while that of the remaining was 87 min. Total case time (minutes), all cases. Robot system setup time (minutes), all cases. Screw placement time (minutes), all cases.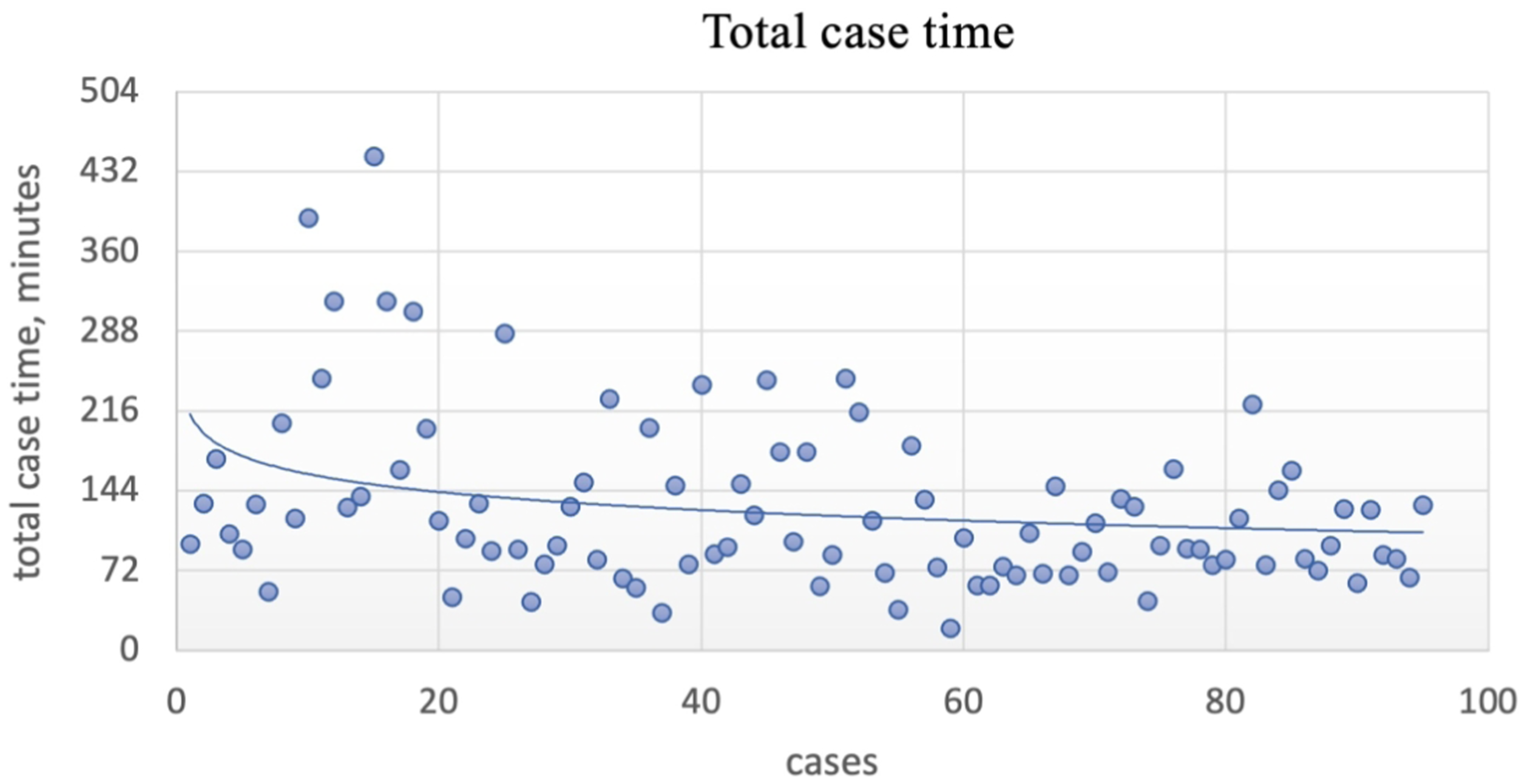
Controlling for Number of Levels Fused
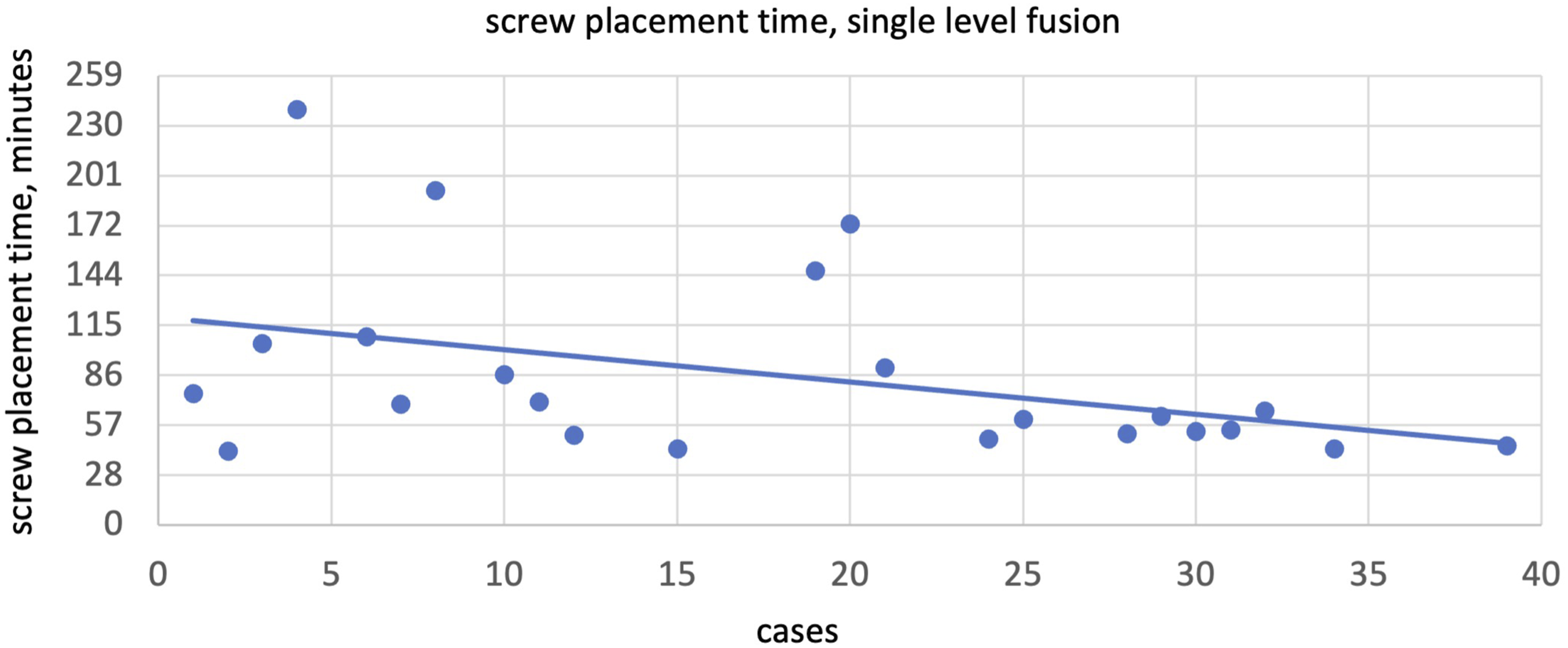
Expectedly, operative time will be different depending on how many levels are done. We then tried to control this by separating the cases per level. Only single and 2 level fusions have significant case numbers to be meaningful at 41 and 30 cases respectively. When we separate the cases by number of levels, the trend still held. For single level fusions (Figure 5), we found a statistically significant different between case 9 (P > .05) and 10 (P = .039). The average time for total robot time for single level is 175 min vs 106 min. No statistical significance with registration time at any case cutoff (all P > .05) was reached. When comparing screw placement time for single level fusion, statistical significance was reached around case 13 (P = .01). Average time for the first 13 cases was 108 min while time of the remaining was 58 min. Total case time (minutes), single level fusion.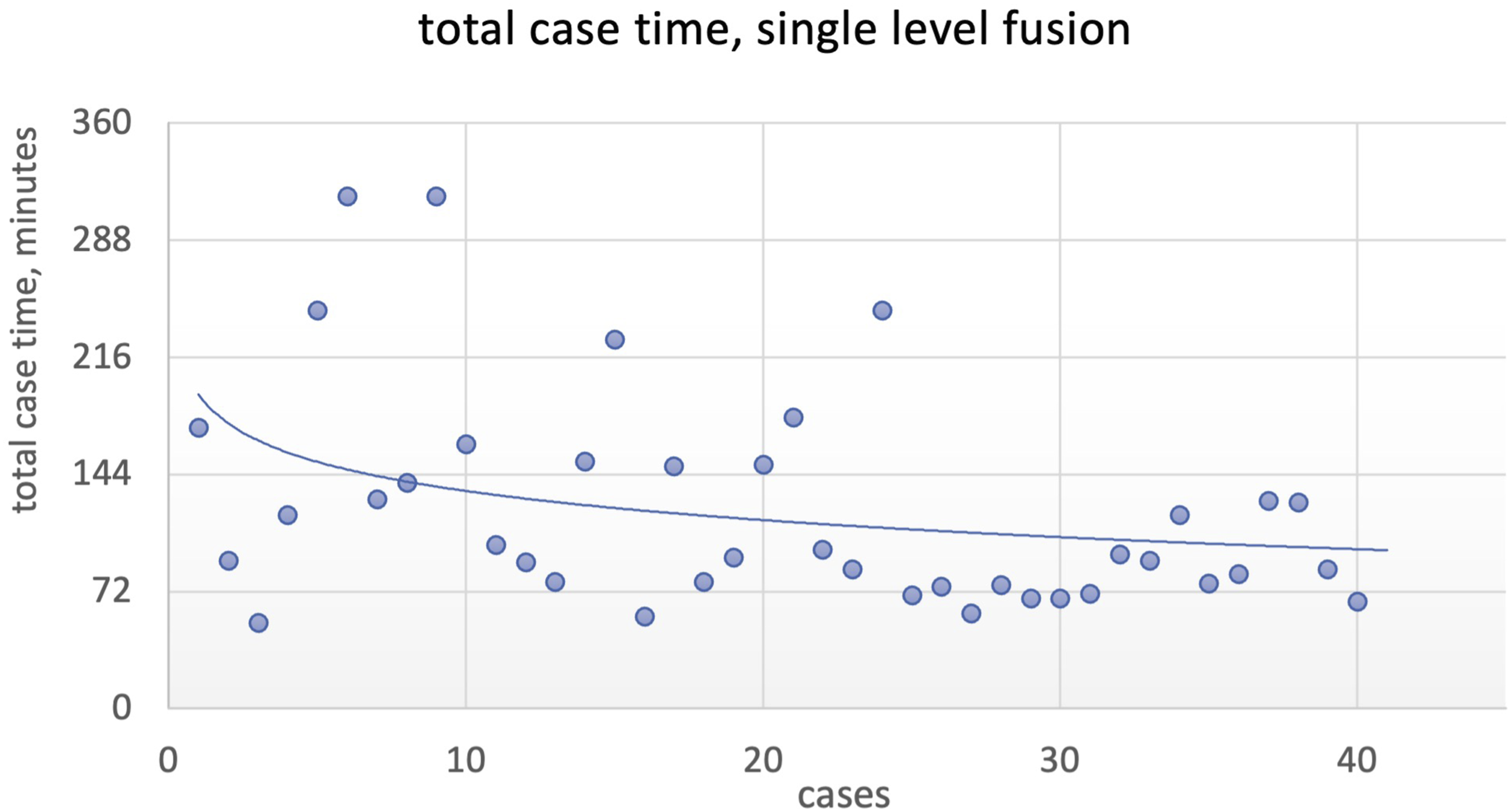
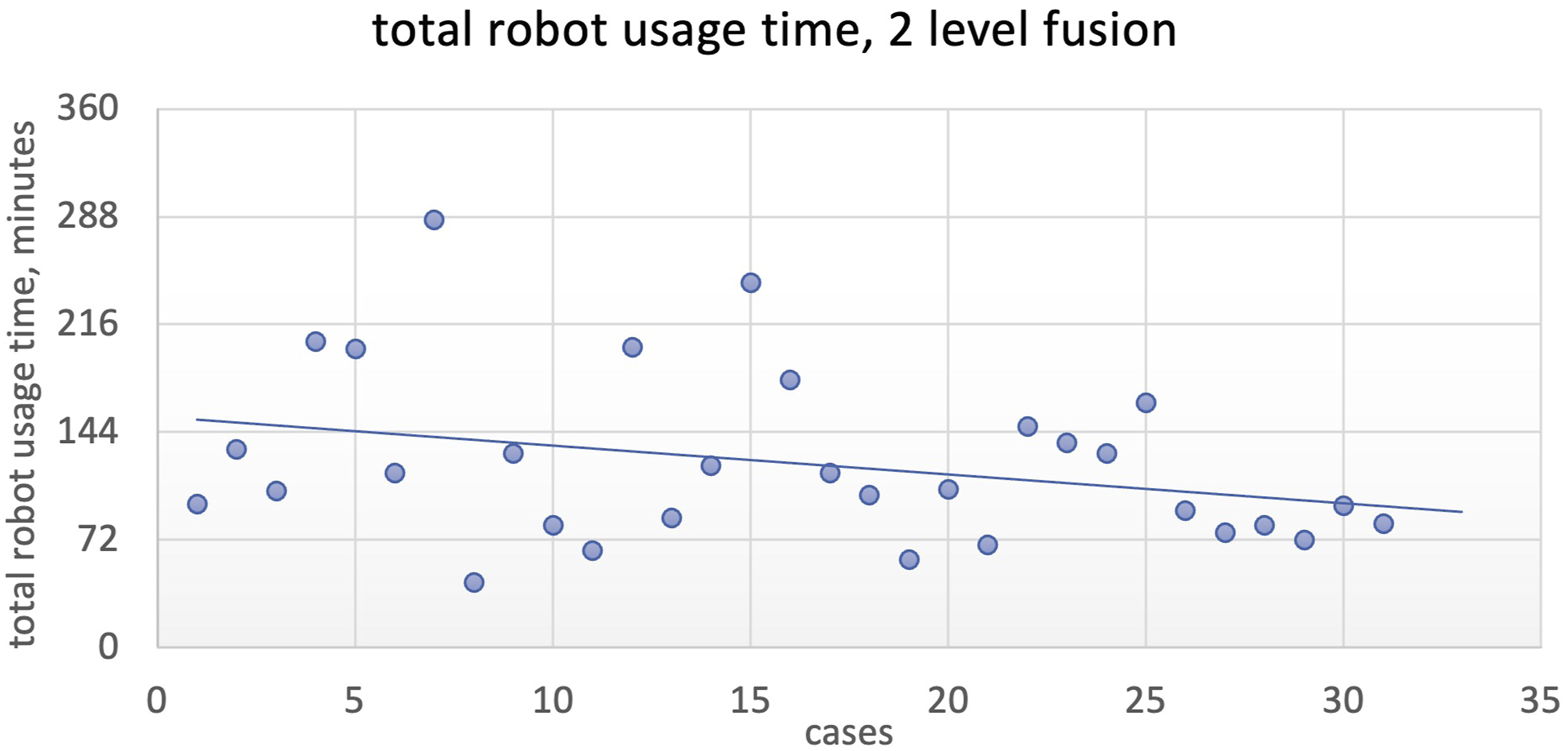
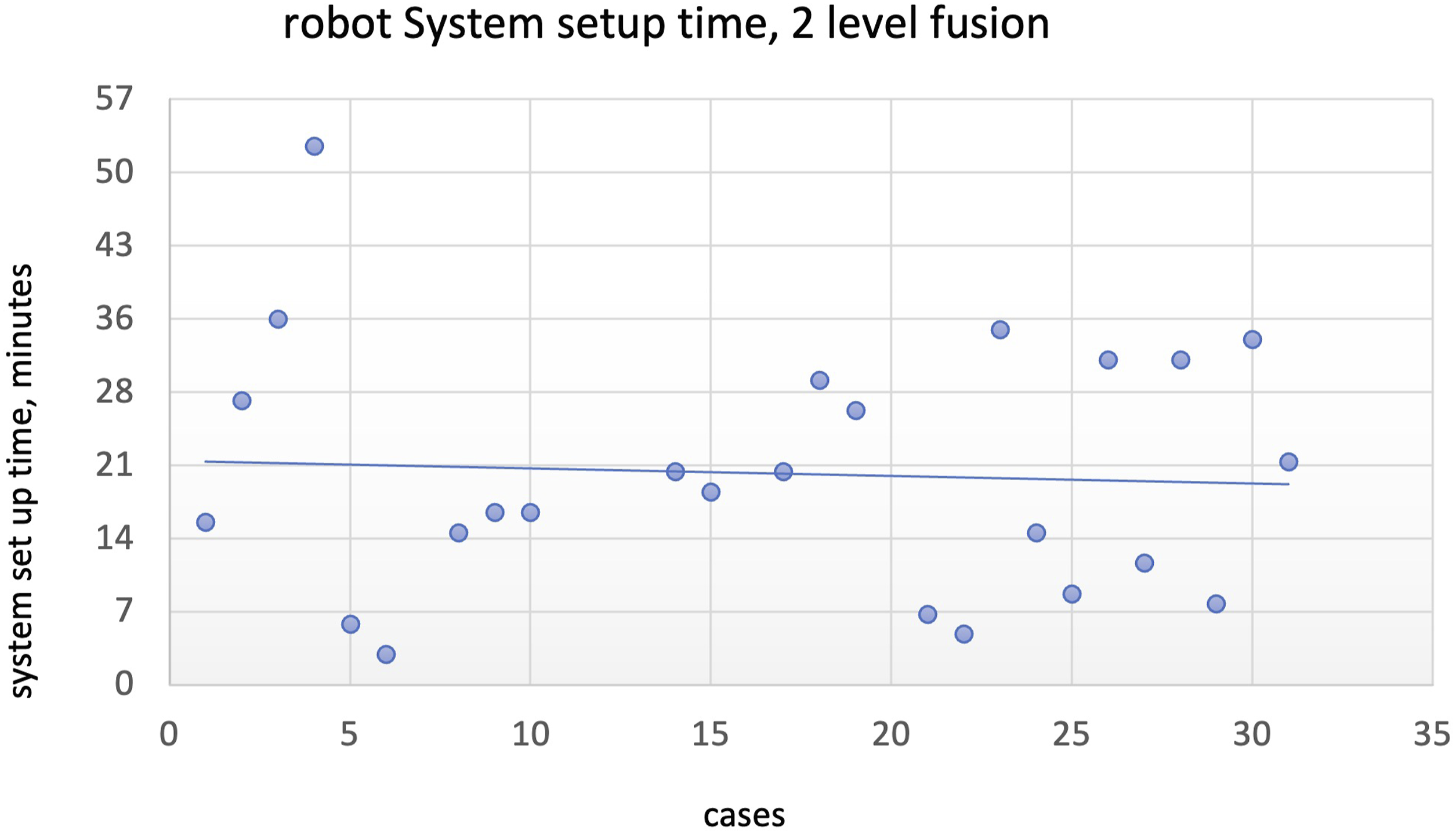
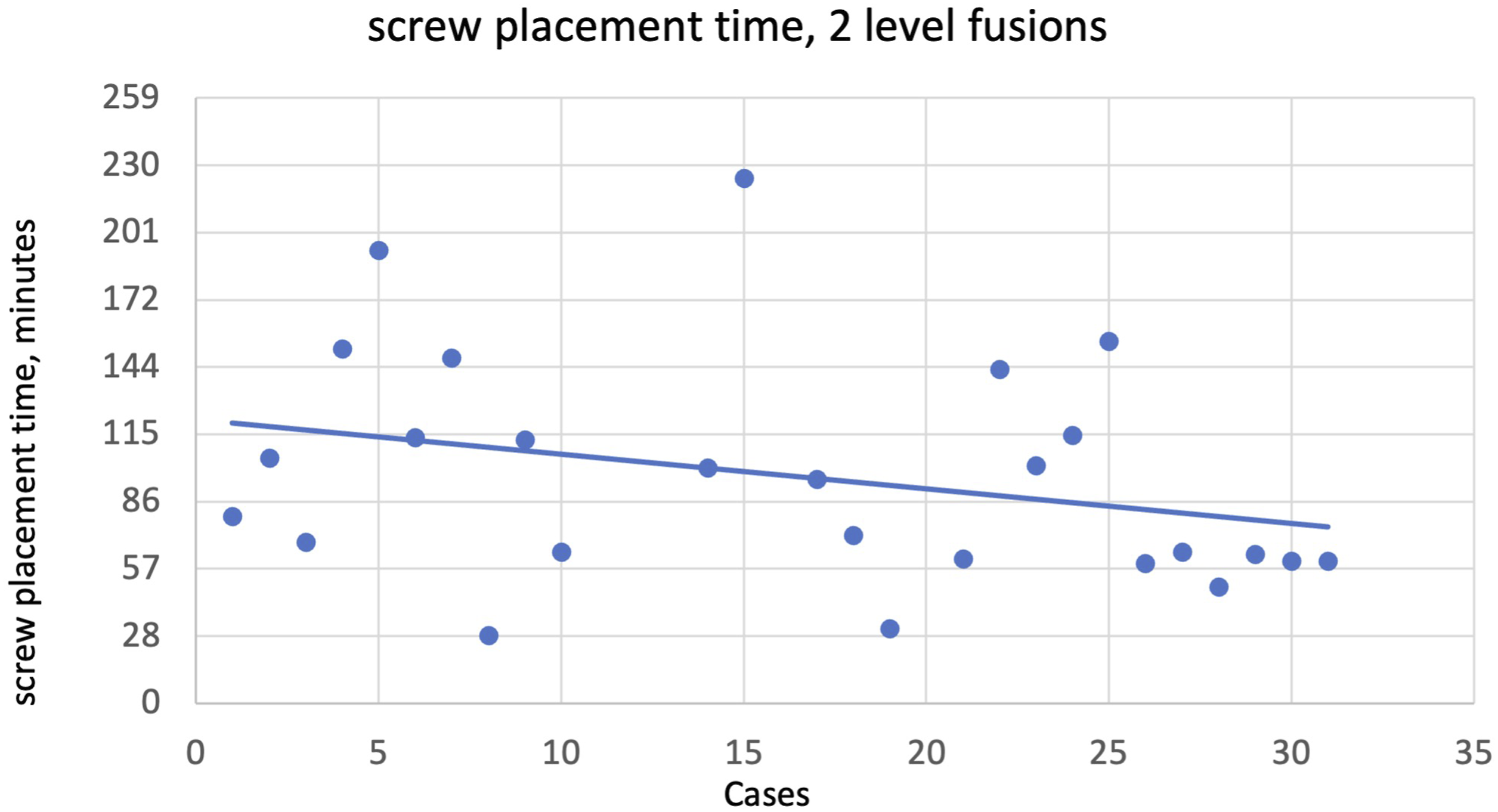
Similarly, for 2 level fusions, total robot usage time for 2-level fusions showed statistical significance at 24 cases (P = .04, 131 vs 95 min). Again, no statistical significance when comparing robot registration time (P > .05) was reached. Screw placement time reached statistical significance at 20 cases (P < .05). Average time for the first 20 cases was 108 min while that of the remaining is 60 min.
Please see Figures 2–10 for further representation of study results. Robot system setup time (minutes), single level fusion. Screw placement time (minutes), single level fusion. Total case time (minutes), 2-level fusion. Robot system setup time, 2-level fusion. Screw placement time (minutes), 2-level fusion.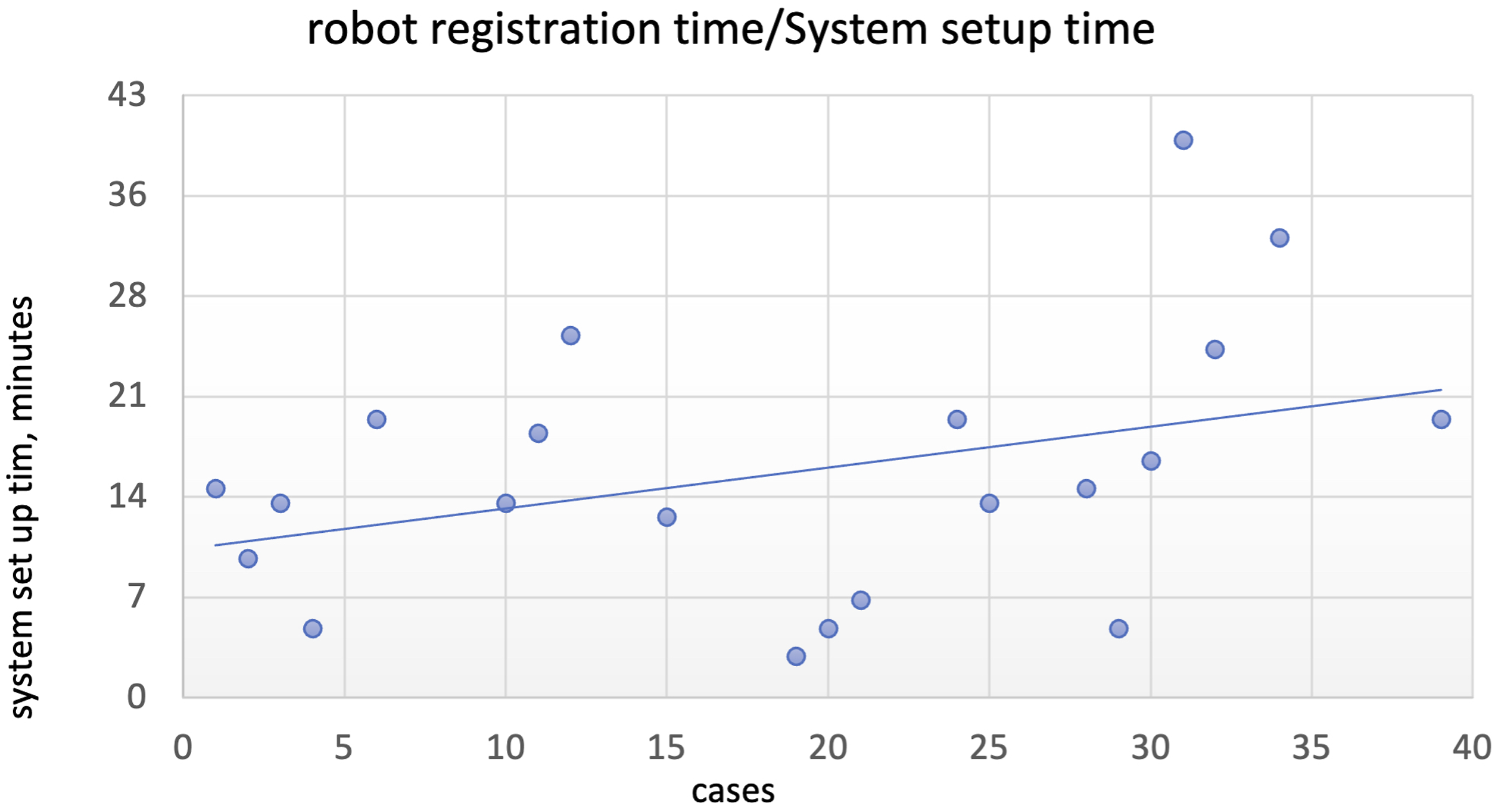
Discussion
Out of the 21 articles reviewed on the learning curve of robotic spine surgery, 3 14 described the experiences of a single attending surgeon, while 5 described the pooled experiences of multiple attending surgeons. One study examined the learning curve experienced by supervised residents or spine fellows, and another study explored the experiences of a single attending surgeon working alongside 2 spine fellows. Among the reviewed papers, 18 out of 21 observed the presence of a learning curve in robotic spine surgery. However, 3 studies failed to demonstrate a significant learning curve.8,10,11 Two of these studies had small sample sizes of 13 patients using the Mazor Renaissance system 11 and 20 patients using the ExcelsiusGPS® system. 8 Conversely, 1 study with a larger sample size of 112 patients examined the learning curve associated with the Mazor spine-assist system. 10
Among these studies, the majority (13 out of 21) employed dichotomous analysis, 3 utilizing predetermined thresholds based on either the number of cases performed or the number of screws placed. These thresholds typically ranged from 3 to 30 cases or 15 to 62 screws. In 10 out of the 21 studies, linear regressions were conducted to examine the relationship between the examined endpoint and the number of cases performed or screws placed. The Avrumova et al 12 study specifically focused on screw placement time. On the other hand, the study conducted by Chen et al 13 assessed the relationship between operative time and robot usage time with respect to case number. The findings of Chen’s study indicated a relative plateau in these variables after approximately 20 cases.
Although most of the studies focused on the Mazor system, there are 3 specifically focused on the ExcelsiusGPS® system.6-8 These studies included patient sizes of 20, 28, and 120 individuals, respectively. As aforementioned, 1 small sample study failed to demonstrate a learning curve.
One in particular by Siddiqui and colleagues 7 investigates the accuracy of pedicle screw placement during robot-assisted surgery. The study involved 1 attending surgeon and 2 fellows who collectively performed the procedure on 120 patients. The outcomes measured in this study included screw tip deviation, tail deviation, and angular deviation from the intended trajectory. All surgeons exhibited enhanced accuracy in screw tail placement after the placement of 30 screws. Unlike our study, their focus is primarily on screw accuracy and not case time.
Another paper on ExcelsiusGPS® learning curve by Fayed et al. 8 focused on assessing screw accuracy in robot-assisted surgery. The study involved 2 attending surgeons and a total of 20 patients. The primary outcome measured was the rate of screw breach. The results indicated a minor trend toward a decrease in screw breach rates in the second half of screws compared to the first half. However, because of a low sample size, they failed to reach statistical significance. Expectedly, they likely failed to reach statistical significance due to a lack of power for their study since it is well known that screws placed robotically will have a high accuracy with low number of screw breaches.
The third paper on ExcelsiusGPS® learning curve is by Jiang et al. 6 Though only a small sample size of 28 patients, they studied, amongst other variables, operative time and screw accuracy. They found a 4 min per case reduction in total case time without plateauing of time reduction. They postulated that likely >30 cases are needed for significant learn curve. Notably, the greatest decrease in operative time was observed within the initial 10 cases.
Our study aims to validate their results by focusing on the less studied ExcelsiusGPS® system and operative time. In our study, total operation time decreased as expected. This trend still held when controlling for number of levels. However, to our surprise, we did not find a statistical significance with robot setup/registration time but a significant decrease in screw placement time. This means that the proficiency gained from total case time reduction was entirely due to the screw placement time. We postulate that the lack of change in robot setup/registration time may be due to the constant changes in nursing and other operating room staff across different days; however, more research will be needed to investigate the cause. Yet because the operating surgeons stayed constant, their improvement in technique and workflow over time reflects in the learning curve. We showed that on average, a total of 14 cases is needed before 1 starts to see a significant drop in operation time. This also holds true after controlling for the number of levels fused. Our study confirmed that the learning curve for the ExcelsiusGPS® system does exist and is a rapid one—this time with adequate patient sample size. We showed that education for ExcelsiusGPS® robotic system is possible as well.
Finally, this study has several limitations that should be acknowledged. Firstly, the retrospective design of the study introduces inherent biases as the selection of cases for robot-assisted spine surgery (RASS) was not randomized. Next, all procedures were done by a single attending surgeon; while the lack of surgeon variability controls for variability in workflow and surgical technique, it also limits the applicability of the learning curve results seen in this study. Moreover, further research is necessary to track long-term patient outcomes. We predict that, given its accuracy and fast learning curve, RASS will yield comparable if not superior patient functional outcomes compared to non-robotic alternatives.
Conclusion
The utilization of RASS systems holds great promise for improving patient outcomes and enhancing the proficiency of future spine surgeons. Our findings suggest that there is a learning curve associated with the ExcelsiusGPS® system, and proficiency is rapidly attainable within approximately 14 cases. We observed a significant decrease in total operative time, primarily driven by improvements in screw placement time. Notably, there was no statistical significance observed in robot setup or registration time. Our study contributes to the limited existing research on the learning curve of the ExcelsiusGPS® system and underscores the importance of incorporating this technology into surgical practice to optimize patient outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.