
Abstract
Study Design
Systematic Review.
Objectives
Demineralized bone matrix (DBM) is an allograft material commonly used as an adjunct in spinal fusion. This review summarizes literature from the past decade describing DBM use in spinal fusion and provides an updated analysis of fusion outcomes based on product type and characteristics.
Methods
A systematic search was conducted using MEDLINE and CENTRAL. Risk of bias was assessed with the Cochrane Back and Neck criteria for randomized studies and the Methodological Index for Non-Randomized Studies criteria for nonrandomized studies. Extracted data included study design, sample size, procedure type, DBM product, fusion outcomes, complications, and follow-up duration. Additional product characteristics, such as DBM form (fiber-based or particulate-based) and sterility method (aseptic or terminal irradiation), were identified from tissue bank data.
Results
Twenty-one studies met inclusion criteria: 3 randomized (level I evidence), 4 level II, ten level III, and 4 level IV. Seven studies examined cervical procedures, and 14 addressed lumbar procedures. Posterior lumbar fusion (n = 6) and anterior cervical discectomy and fusion (n = 6) were most common. Among 18 comparative studies, 17 found no significant difference in fusion outcomes between DBM and comparison groups.
Conclusions
DBM used as an autograft extender demonstrated fusion rates comparable to alternative graft materials. However, the predominance of nonrandomized, retrospective designs and limited controlled data result in low overall evidence quality. Further high-quality prospective studies are warranted to better define the role of DBM in spinal fusion.
Introduction
Over the past several decades, the incidence of spine fusion surgeries has increased significantly, driven by advancements in surgical techniques and an aging population. 1 Despite advancing techniques, pseudarthrosis continues to be a commonly associated complication, contributing to nearly one-fourth of spine fusion revisions. 2 Accordingly, graft augmentation has long been an extensively studied principle.3,4 Autologous iliac crest bone graft (ICBG) is considered the “gold-standard” graft material for spine fusion due to high fusion rates without the risk of rejection or disease transmission. 5 However, the limited availability and associated donor site morbidity limit the use of ICBGs clinically, prompting greater exploration and development of alternative solutions.6,7 This has translated to an expansive market of commercially available bone graft products, which spine surgeons in the current era must understand to select the most appropriate products. 8
Allopathic bone grafts, derived from human cadavers, are the most used alternative to autologous grafts such as ICBG. 9 Demineralized bone matrix (DBM) is an allograft material that has become an increasingly popular adjunct to fusion procedures, comprising approximately half of all allografts used in the US. 9 DBM is created by the acid treatment of cadaveric bone which removes most of the mineral content and retains the organic matrix, composed primarily of Type I collagen and growth factors including bone morphogenic proteins (BMP). The 0.5 M hydrochloric acid treatment is used by most tissue banks to mimic the natural bone regeneration process. Pre-clinical studies have demonstrated that a 2% residual calcium value leads to the greatest bone formation with less than 8% residual calcium required to meet the definition of a DBM per ASTM International Standard (F2529). 10
Many different DBM products are currently available, with variances in further processing and sterilization techniques resulting in differing properties. 11 One such variance is the processing of DBM either as fiber-based or as particulate-based. Martin et al studied the improved fusion outcomes of fiber-based DBM over particulate-DBM in a preclinical, posterolateral intertransverse process spine arthrodesis model. 12 The posterolateral spine can be a more challenging healing environment than interbody spine procedures and thus was used to provide a better understanding of the differences between fiber-based DBM and particulate-based DBM. It was demonstrated that the devitalized (nonosteoinductive) fiber-based DBM outperformed the devitalized particulate-based DBM as the fiber-based DBM also provided better osteoconductive properties. A comparison of DBM products as fiber-based vs particulate-based in thus warranted.
As the commercial DBM industry grew, tissue regulations transitioned from voluntary standards with the establishment of the AATB (American Association of Tissue Banks) in 1976 to the first published “the standards of tissue banking” in 1984 and finally to the FDA’s good tissue practices (GTP) enforcement in 2005 of all tissue establishments. 13 While an FDA tissue establishment is now required of all tissue banks, most musculoskeletal tissues are also distributed by tissue banks with AATB-accreditation. A sterility assurance level (SAL) 10−3 (1 in 1000) was established by the FDA as adequate for implantable medical biological devices. However, the Association for the Advancement of Medical Instrumentation (AAMI) and the AATB use SAL 10−6 as their standard. The FDA audits tissue banks and their methods of tissue processing, including sterilization, that include different biologic detergents, antibiotics, alcohol, or hydrogen peroxide with or without terminal irradiation as a final step.
Thus, another variance in processing of DBM is the sterilization technique. Early investigations of DBMs by Dr Marshall Urist in the 1960s-1970s led to an understanding that radiation affects the bone induction of DBM.14,15 Dr Everard Munting confirmed these findings in the 1980s by noting a 60% reduction in implanted bone content in a preclinical rat model due to sterilizing with gamma irradiation. 16 This has been studied further by others, including in 2005 by Dr Arthur Gertzman who noted a 53% reduction in the osteoinductivity score due to the terminal use of cold gamma irradiation. 17 The negative side-effects of irradiation have been observed when employed as terminal irradiation of the DBM whereby bone proteins are more readily exposed rather than as initial steps to lower the bioburden from a mineralized allograft pre-demineralization. Of note, Musculoskeletal Tissue Foundation (MTF) may pretreat some allograft tissue donors with low-dose gamma irradiation but does not use terminal irradiation. While the first commercial DBM, launched in 1991, (Grafton DBM Gel by Osteotech) does not use irradiation and follows aseptic sterility processing techniques, many tissue banks currently use low-dose gamma irradiation, high-dose gamma irradiation, or electronic beam (e-beam) irradiation such as AlloSource, Bone Bank Allografts, Community Tissue Services (CTS), LifeNet, RTI Biologics, Inc, and Tissue Banks International. 13 The possible mechanism by which irradiation reduces the osteoinductivity of DBMs has been investigated. A study in 2016 by Dr Uri Antebi observed reductions in the total protein of DBM samples as well as specifically BMP-2 and BMP-7 due to both gamma irradiation and e-beam irradiation of samples that were either lyophilized or frozen. 18 In 2024, Dr Ganesh Shankar presented at the Cervical Spine Research Society (CSRS) Meeting on the negative impacts of both e-beam and gamma irradiation on the biological properties of DBMs. Structural changes to the DBM fibers were observed under the scanning electron microscope (SEM) with increased enzyme degradation and increased protein loss over time. BMP-2 elution at 24 hr was very rapid for all irradiated samples. The aseptic processing preserved a three-dimensional surface while both the gamma irradiated and the e-beam irradiated surfaces were smoothed over. The biological changes due to irradiation observed by Drs. Antebi and Shankar provide a possible mechanism for the reduction in osteoinductive potential observed previously by Drs. Urist, Munting, and Gertzman.
More recently, Dr Yong-jie Zhao investigated the variability in BMP-2 content in DBM when processing cortical bone from the femur, tibia, humerus, or ulna. 19 Dr Zhao determined that BMP-2 concentration was greatest from the femur followed by the tibia, humerus, and ulna in descending order. Using a guanidine-HCL extraction (GuHCL), the enzyme-linked immunosorbent assay (ELISA) measured the femur as 5.6 times more than the tibia, 24.7 times more than the humerus, and 34.5 times more than the ulna. While it is unknown which tissue banks may or may not focus on specific cortical shafts in the production of their DBM, these differences in BMP-2 concentration may be an additional variance between different DBM formulations. Dr Hyun Bae in 2006 originally observed an intervariability and intravariability on BMPs in commercially available DBM products. 20 The DBM formulations studied varied in terms of fiber-based vs particulate-based, aseptic vs terminally irradiated, the percentage of DBM vs handling carriers, and likely the harvesting site of the DBM from the donors. Thus, many variables exist when reviewing DBM formulations and their clinical outcomes.
Despite the widespread use of DBM, few systematic reviews have been done assessing its use in spinal fusion. Furthermore, existing studies have analyzed DBM use only for specific spine procedures or in combination with non-spine surgeries and all were published more than 5 years ago.21-23 Here, we aim to systematically review the available clinical literature describing the use of DBM products in spinal fusion within the past 10 years, present an updated analysis of their impact on fusion outcomes, and assess results by known variances such as fiber-based vs particulate-based and aseptic processing vs terminally irradiated processing. By synthesizing the latest evidence, we seek to provide insights into the current state of DBM use in spine fusion and identify areas for future research.
Methods
We conducted this systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Cochrane Handbook for Systematic Reviews of Interventions guidelines.24,25 A literature search of MEDLINE (via PubMed) and Cochrane Central Register of Controlled Trials (CENTRAL) databases was conducted in July 2024. Search terms included “demineralized bone matrix”, “DBM”, “spine”, “fusion” and “arthrodesis” as described in previous studies. 26 The reference lists of selected papers captured in the search were also analyzed to identify any studies that may have been missed.
Our inclusion criteria were as follows: (1) clinical research studies involving the use of DBM in spinal fusion for at least ten patients, (2) studies explicitly stating the graft products used, (3) studies that report the rate of radiological fusion, and (4) studies published in English from January 2014 through June 2024. Studies that did not report original clinical data, including systematic reviews and meta-analyses, animal studies, and studies of DBM use in non-spinal surgeries were excluded. Two authors (M.B. and C.C.) independently reviewed the title, abstract, and, if necessary, the full text of studies to determine eligibility for inclusion. Any disagreement regarding the inclusion of studies was resolved by the senior author (F.V.). Two authors (M.B. and C.C.) independently extracted data including study design, sample size, type of procedure, DBM product used, DBM machining method, sterility methods, fusion outcomes, complications, and follow-up time from each study. There were no discrepancies between the authors.
Risk of bias was independently assessed by 2 authors (M.B. and C.C) and any disagreements were resolved by discussion, with involvement of the senior author (F.V.) as needed. We assessed randomized studies using the criteria recommended by the Cochrane Back and Neck Group, as described previously in other studies.23,27 Non-randomized studies were assessed using the Methodological Index for Non-Randomized Studies (MINORS), described in a previous systematic review of anterior cervical spine procedures. 13 Briefly, MINORS contains 12 items rated as follows: 0 when the article does not report the criterion, 1 if the criterion is reported but not sufficiently fulfilled, or 2 if the criterion is fulfilled. 28 A study’s total score is the sum of the criteria ratings, with higher scores indicating low risk of bias. Four of the 12 items only apply to comparative studies, so the highest possible score is 24 for comparative studies and 16 for non-comparative studies. A level of evidence, as described by Wright et al, was assigned for each included manuscript by 2 agreeing authors (M.B. and C.C.). 29
Results
Our database search generated 321 search results, of which 176 were duplicates and subsequently removed and 9 additional studies were identified by searching reference lists of relevant articles. Each study was screened by title and abstract, after which 116 were removed including 23 animal studies, 1 cadaver study, 34 review articles, and 58 unrelated or non-spine studies. The remaining 38 studies were reviewed in full to determine eligibility and 17 additional studies were excluded including 14 that did not report the DBM product used and 3 that did not report the rate of fusion or pseudoarthrosis. In total, 21 studies met the criteria for inclusion in our review (Figure 1). Flow diagram outlining our study search and inclusion process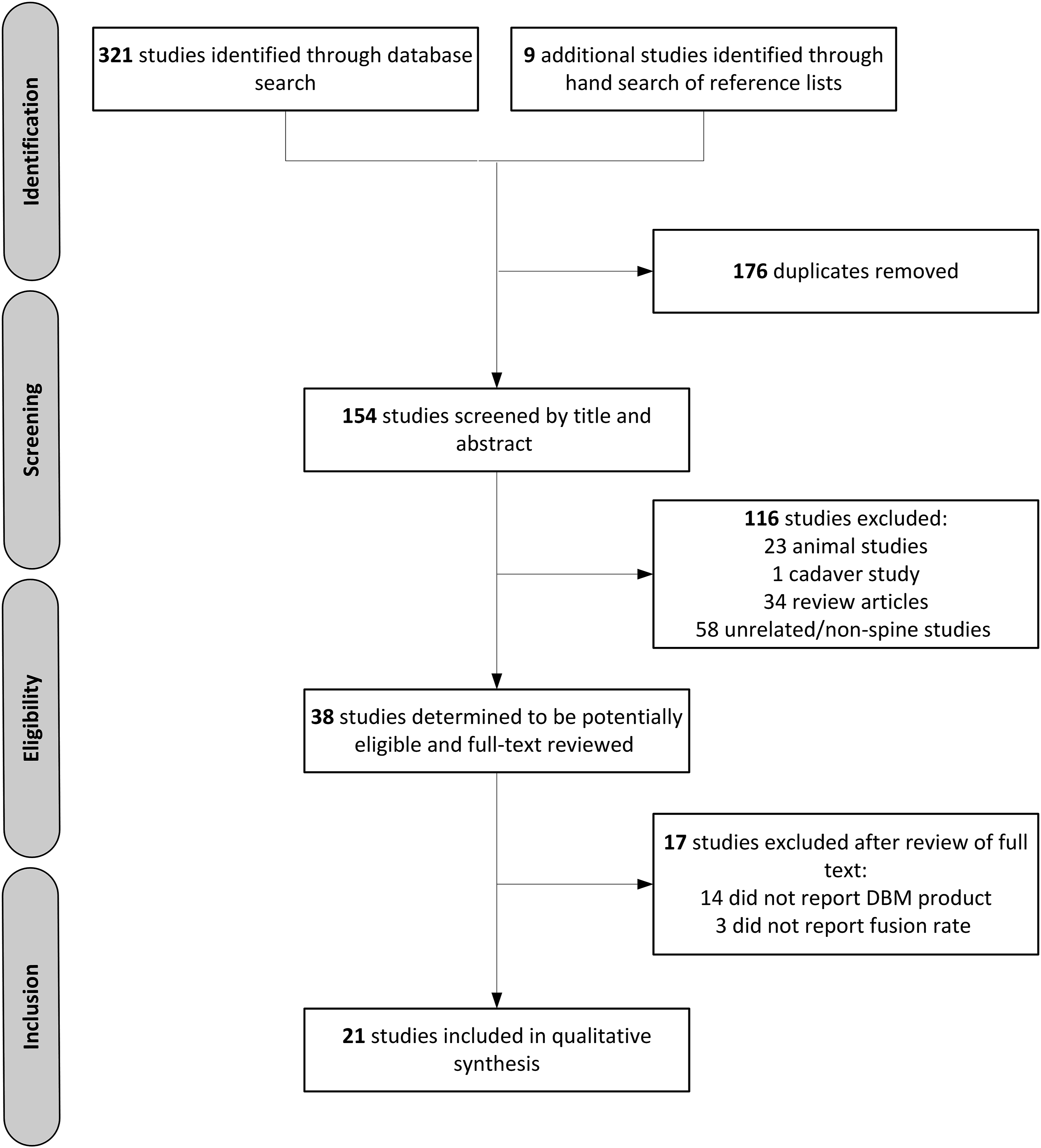
Risk of Bias for Randomized Studies Assessed With the 13-Item Criteria Recommended by the Cochrane Back and Neck Group
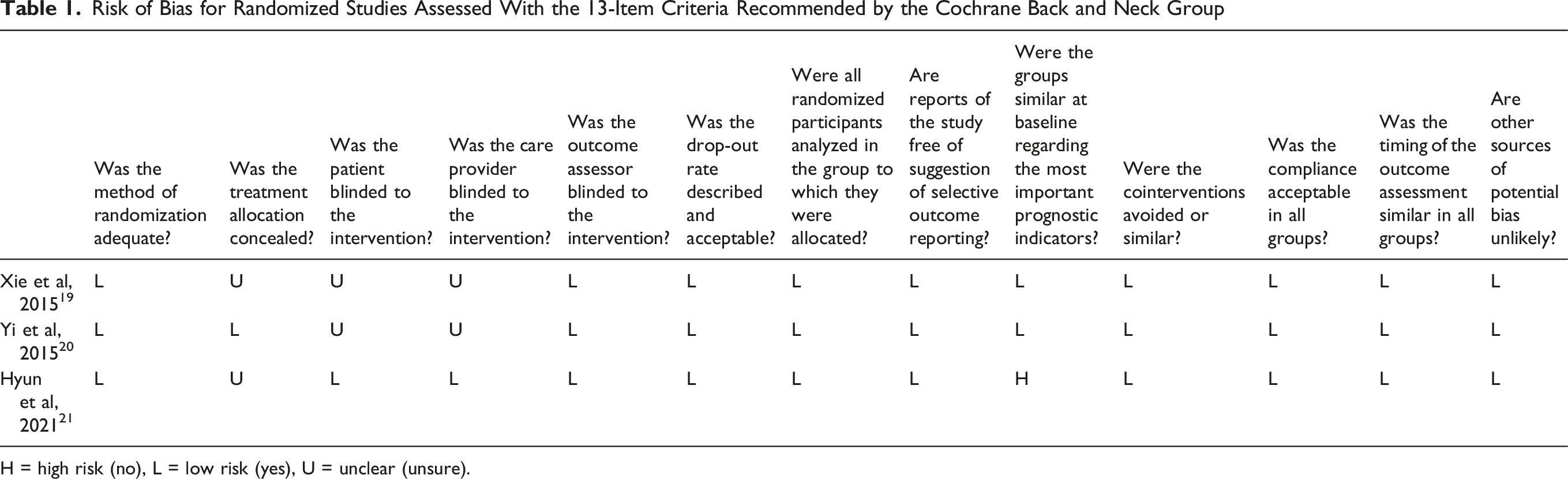
H = high risk (no), L = low risk (yes), U = unclear (unsure).
Risk of Bias for Non-randomized Studies Assessed With the MINORS Checklist
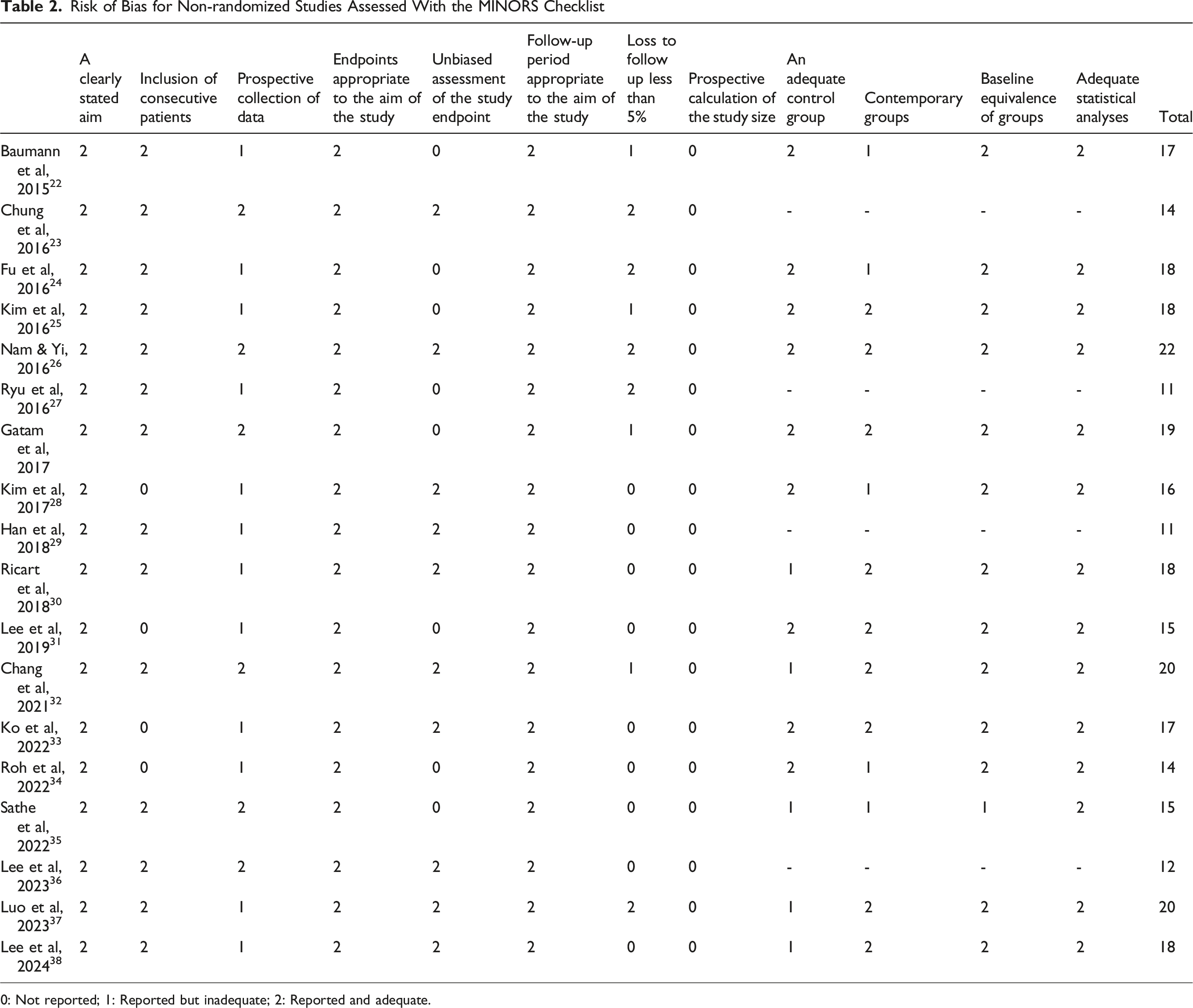
0: Not reported; 1: Reported but inadequate; 2: Reported and adequate.
Details and Pertinent Results of Studies Reporting the Use of DBM Products in Cervical Spine Procedures
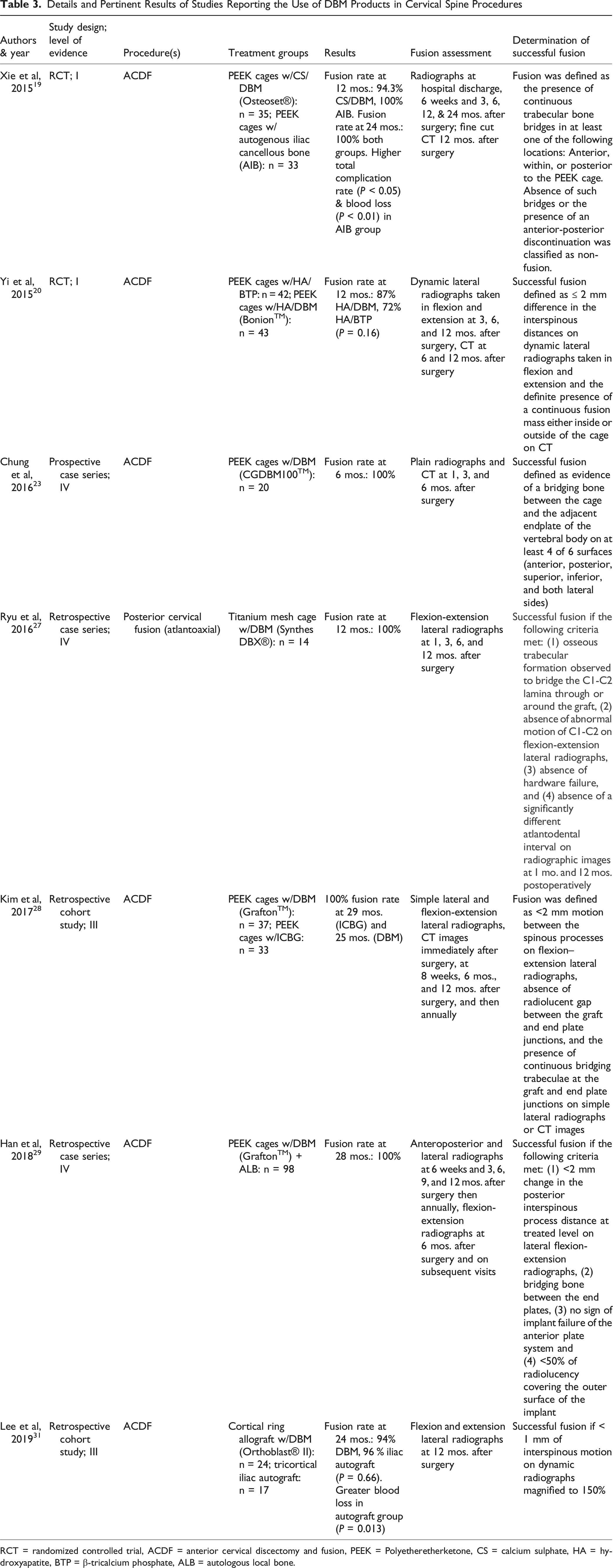
RCT = randomized controlled trial, ACDF = anterior cervical discectomy and fusion, PEEK = Polyetheretherketone, CS = calcium sulphate, HA = hydroxyapatite, BTP = β-tricalcium phosphate, ALB = autologous local bone.
Details and Pertinent Results of Studies Reporting the Use of DBM Products in Lumbar Spine Procedures
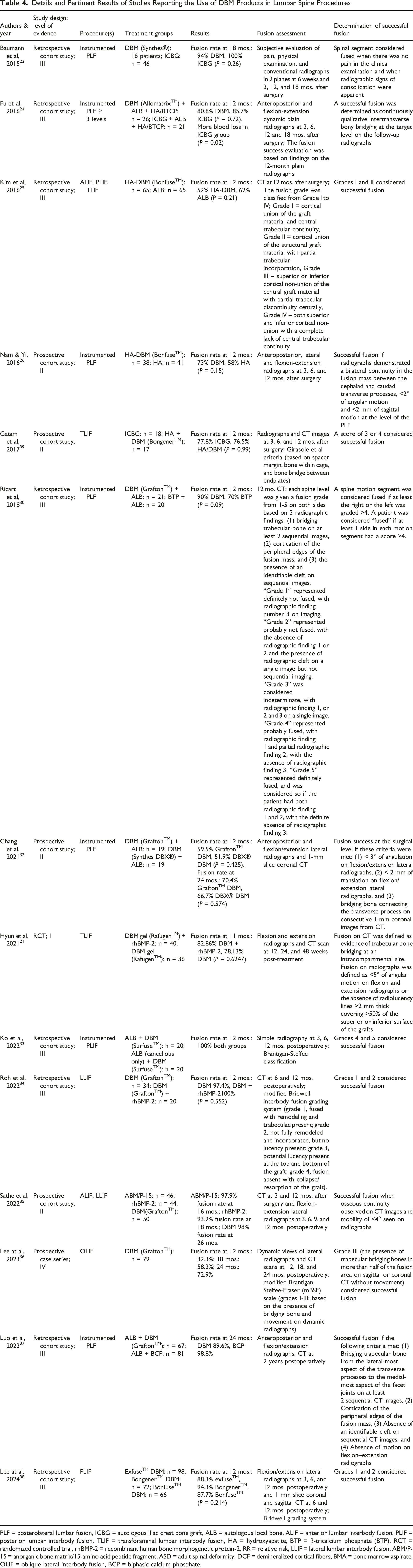
PLF = posterolateral lumbar fusion, ICBG = autologous iliac crest bone graft, ALB = autologous local bone, ALIF = anterior lumbar interbody fusion, PLIF = posterior lumbar interbody fusion, TLIF = transforaminal lumbar interbody fusion, HA = hydroxyapatite, BTP = β-tricalcium phosphate (BTP), RCT = randomized controlled trial, rhBMP-2 = recombinant human bone morphogenetic protein-2, RR = relative risk, LLIF = lateral lumbar interbody fusion, ABM/P-15 = anorganic bone matrix/15-amino acid peptide fragment, ASD = adult spinal deformity, DCF = demineralized cortical fibers, BMA = bone marrow aspirate, OLIF = oblique lateral interbody fusion, BCP = biphasic calcium phosphate.
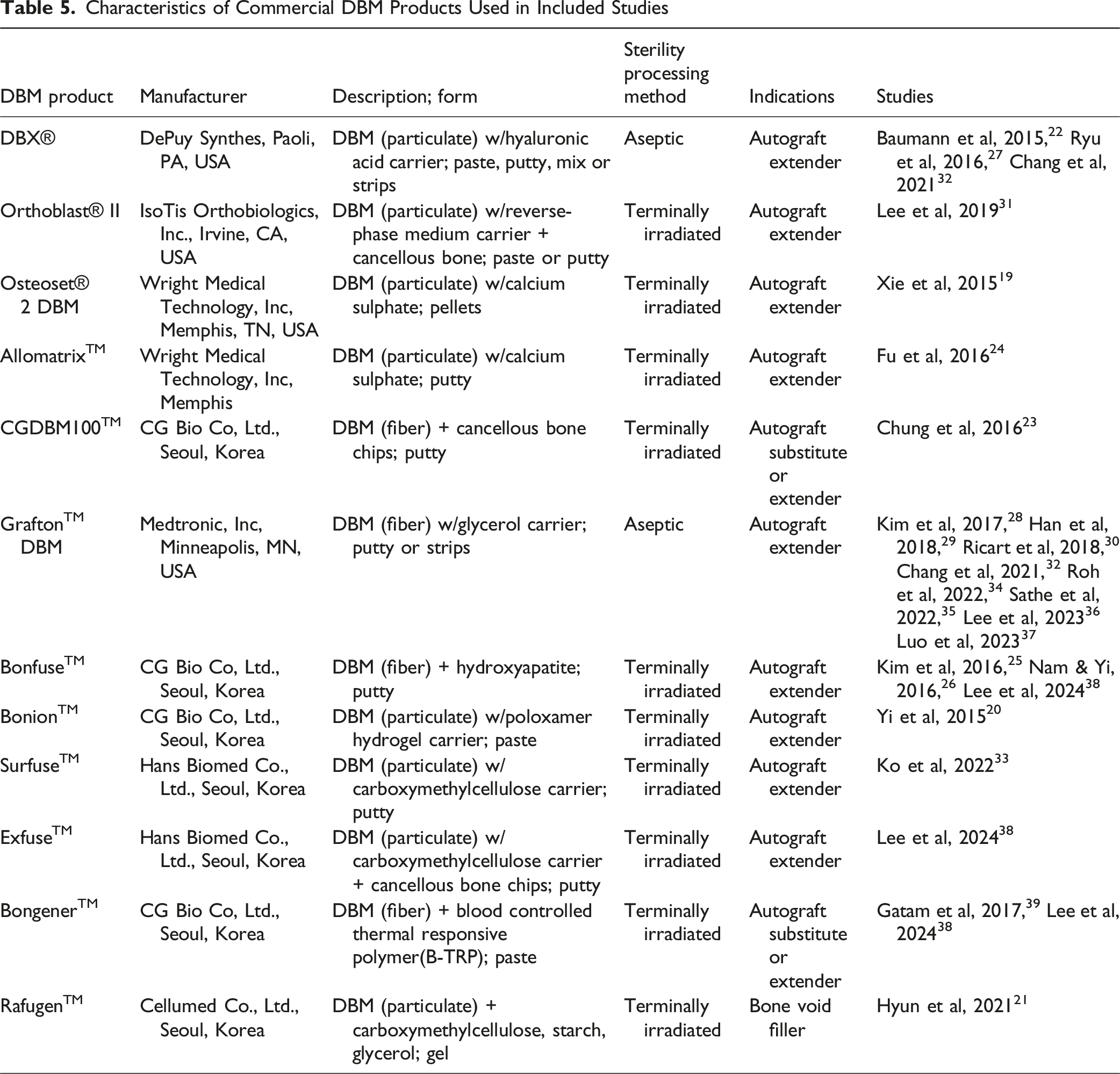
Characteristics of Commercial DBM Products Used in Included Studies
The remaining 8 studies involved DBM use for lumbar interbody fusion. Each of the comparative studies reported no significant difference in outcomes between treatment groups. In a retrospective study, Kim et al compared a commercially available HA/DBM product to autologous local bone in patients undergoing anterior lumbar interbody fusion (ALIF), posterior lumbar interbody fusion (PLIF) or transforaminal lumbar interbody fusion (TLIF) procedures. 44 Two other retrospective studies used DBM for PLIFs, including Ko et al who compared autologous local bone with DBM to only cancellous autologous local bone with DBM, and Lee et al who compared 3 different commercial DBM products.33,38 Roh et al compared DBM with and without rhBMP-2 in patient undergoing lateral lumbar interbody fusion (LLIF) procedures. 45 In the remaining 3 prospective studies, Sathe et al compared anorganic bone matrix/15-amino acid peptide fragment (ABM/P-15), rhBMP-2, and DBM for ALIF and LLIF procedures, Gatam et al compared HA with DBM to ICBG for TLIFs, and Lee at al. conducted a prospective case series studying DBM use in oblique lateral interbody fusion (OLIF) procedures reporting 72.9% fusion rate at 24 months.46-48 Additional descriptions of the commercial DBM products used in included studies are provided in Table 5.
Discussion
The Overall Quality of Evidence Among Included Studies of DBM in Spinal Fusion is Limited
The aim of this systematic review was to assess the clinical evidence for the use of DBM products in spinal fusion in the past 10 years. An extensive search of the literature yielded 21 studies that met our inclusion criteria and just 3 of these were randomized, constituting level I evidence. Four studies represented level II evidence, while most studies represented level III (10 studies) and IV (4 studies) evidence. Overall, studies were limited mainly to retrospective studies and many lacked a standard control group or used historical controls. Almost all studies reported no significant difference in fusion rates between treatment groups. However, in more than half of the non-randomized studies, it was unclear if their outcome assessment was unbiased as many did not disclose whether the assessors were blinded to the interventions. In the randomized studies, blinding of the patients and providers was unclear in 2 and only 1 reported concealment of treatment allocation which may represent sources of performance and selection bias, respectively. 27
DBM Products in the Studies Varied
Commercial DBM products are available by many different companies and in varying formats. Within the studies that met out inclusion criteria, GraftonTM DBM was the most studied product (8 studies) followed by Synthes DBX® and BonfuseTM which were each used in 3 studies. Products commercially available in the US consisted of GraftonTM DBM, Synthes DBX®, AllomatrixTM, Osteoset® II DBM, and Orthoblast® II DBM. Other products available outside of the U.S. consisted of BonfuseTM, BongenerTM, CGDBM100TM, BonionTM, RafugenTM, SurfuseTM, and ExfuseTM.
For the US commercial products, the DBM products were mostly used in combination with local bone as autograft extenders, but several were also used without local bone. For the Grafton DBM studies, 4 were used with autologous local bone and 4 were used alone. Grafton DBM Putty consists of DBM fibers with a glycerol carrier processed aseptically. One study (Sathe et al) used Grafton Orthoblend which includes allograft bone chips with the other components of Grafton DBM Putty. Synthes DBX was used once with autologous local bone and twice used alone. Synthes DBX consists of particulate-based DBM with a hyaluronan carrier processed aseptically. Osteoset II DBM consists of a mixture of particulate-based DBM and calcium sulfate terminally processed with irradiation and was used alone. Allomatrix is similar to Osteoset II DBM, but in the study it was combined with a biphasic hydroxyapatite/beta-tricalcium phosphate synthetic granules (Foramic: Maxigen Biotech, Inc, Taiwan) as well as autologous local bone. Lastly, Orthoblast II is a particulate-based DBM used alone inside a cortical allograft ring terminally processed with irradiation.
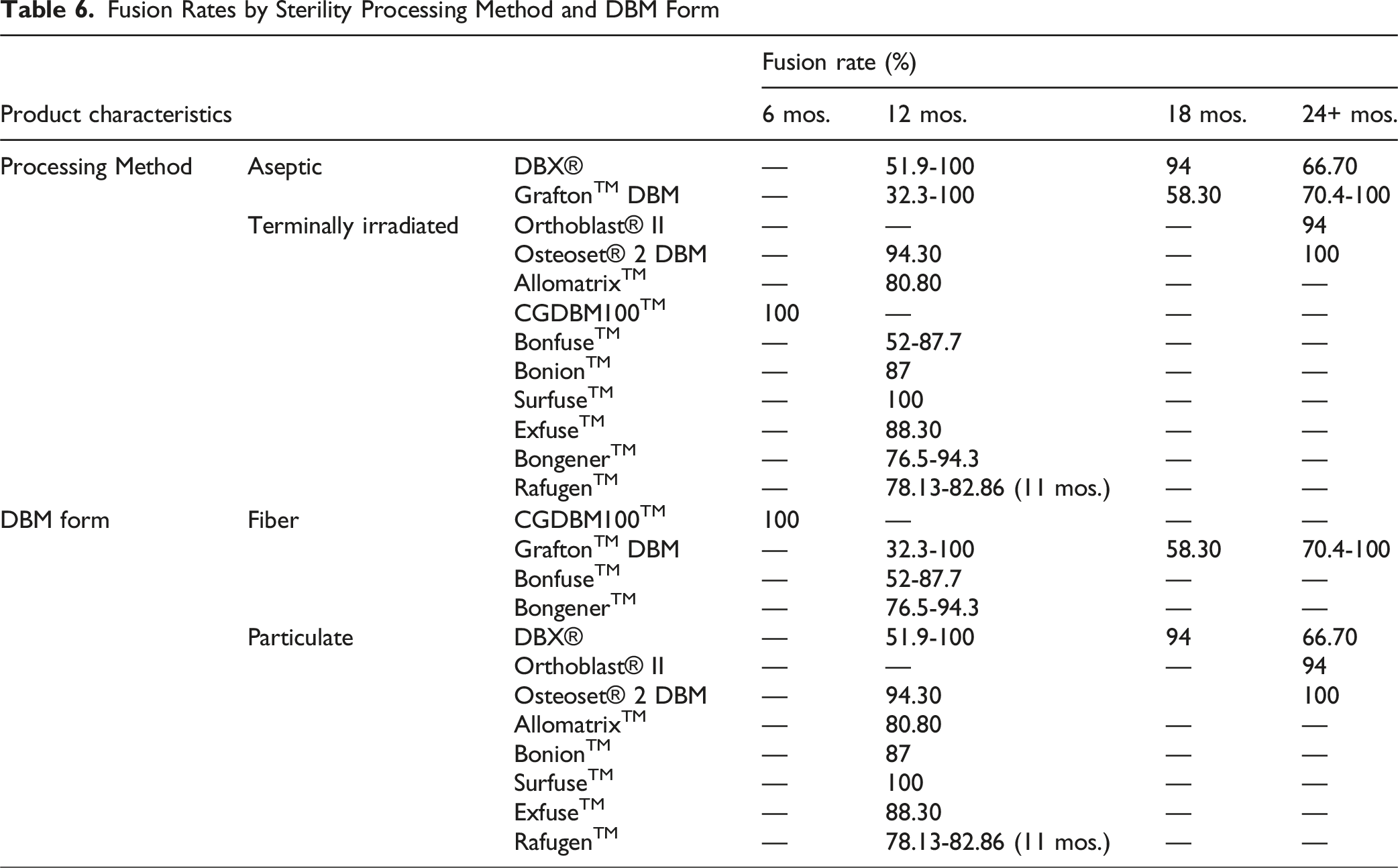
Fusion Rates by Sterility Processing Method and DBM Form
Understanding the Percentage DBM of the Products
One limitation of comparing the outcomes across these studies is not knowing the percentage composition of demineralized bone content within each product. Han et al characterized a quantitative assay for understanding the relative osteoinductivity of DBM products using both a C2C12 cell in-vitro assay as well as an intramuscular nude rat assay. 49 DBM particulate without a handling agent was prepared and then a portion rendered inactive. DBM was inactivated by deproteinizing the DBM and thus denaturing the BMP proteins from the collagen structure that remains when bone is demineralized. Within the in-vitro assay, alkaline phosphatase (ALP) bone activity varied linearly as the volume composition of active DBM increased vs inactive DBM. These same volume compositions with various combinations of active DBM and inactive DBM were also implanted into the in-vivo model. A linear correlation was observed when comparing the in-vitro ALP activity to the ALP activity of explants at 28 days from the in-vivo model. Thus, the percentage by volume of the active DBM component is the best predictor of osteoinductive activity.
Often the percentage value by weight may be known but this is not the best characterization of a DBM product for comparison. For example, the handling agents/carriers, such as glycerol, hyaluronic acid, or a reverse phase medium carrier, will vary by weight as well. Thus, a heavier carrier, like glycerol, reduces the relative weight percentage of the active DBM component but the actual DBM volume is often higher than other DBMs with a low-weight carrier. Another complication is that most handling agents/carriers will break down and be removed from the implant site by the body within 48-72 hours of implantation. The overall volume of bone graft will settle into less than the original implant volume and may variably affect the clinical use. Thus, the percentage by volume of the DBM component is more important than the percentage by weight.
The DBM products included within these studies also vary in their composition by other non-osteoinductive components, such as synthetic granules or cancellous chips. These mineralized components provide structural scaffolding that may be clinically useful to maintain the graft volume space, ie, for use in the posterolateral spine, but with no active release of BMPs from these components, the potential osteoinductivity of the overall product is reduced by the volume percentage of these components as well.
Additionally, the volume of DBM used in each study varied and in 1 study was not well controlled between the study groups (39). Luo et al compared the use of a biphasic calcium phosphate (BCP) to DBM for posterolateral fusions. 47 In 1 group, 5cc of the BCP was used per side combined with local autogenous graft. However, the other group was combined with only 2.5cc of DBM. Also, TLIFs were performed as needed and patients with or without a TLIF were not controlled for between the 2 study groups with a portion of the available autogenous bone graft used in the TLIFs as well.
Understanding Fusion Classifications Used in the Studies
The studies in this review used multiple fusion classification systems, each with distinct criteria that shaped the interpretation of surgical outcomes. Most authors relied on the Bridwell grading system, which defines fusion based on the continuity of trabecular bone across the graft and ranges from Grade I (definite fusion) to Grade IV (definite nonunion).50-53 This system remains the most widely adopted because it provides a reproducible way to distinguish between solid fusion and pseudarthrosis on plain radiographs or CT. Several studies instead used the Brantigan–Steffee classification, which grades interbody fusion from I to V and incorporates both radiographic and clinical stability, with Grades IV and V generally accepted as successful fusion. 54 Other investigators used binary definitions of fusion, categorizing patients simply as fused or not fused based on the presence of bridging trabecular bone on radiographs, CT scans, or dynamic studies.55,56 In more recent work, researchers applied CT-based grading systems, including modifications such as the Tan et al CT fusion grading scale, which separates complete fusion from partial fusion. 57 Collectively, these approaches reveal significant variability in how surgeons and radiologists define and report fusion. Understanding these differences is essential, as the choice of classification system directly influences reported success rates, complicates comparisons across studies, and highlights the need for standardization in future spinal fusion trials.
The Use of DBM as an Autograft Extender Instead of a Graft Substitute
Graft extenders promote bone formation and can be used in conjunction with autologous bone to reduce the amount required for achieving a similar fusion rate, or to enable the fusion of additional levels with a standard amount of autologous graft. DBM graft extenders generally contain a lower percentage of DBM due to the addition of handling carriers, synthetic granules, or mineralized bone chips. 10 Graft extenders may utilize sterility processing methods either aseptically or with terminal irradiation. Some DBM products are also indicated for use as graft substitutes, which can achieve similar fusion rates without the need for any autologous graft. 26 These “stand-alone” biologics typically consist of 100% DBM. Compared to stand-alone biologics, DBM graft extenders typically have lower DBM content and therefore less osteoinductivity, or degree to which graft materials induce host mesenchymal stem cells to differentiate into bone-forming osteoblasts. However, there can be a wide range of osteoinductivity between different DBM bone graft extenders. These products all contain various amounts of DBM, while some include carrier compounds and others include additional bone graft materials such as hydroxyapatite.47,50 Furthermore, previous studies have shown significant variations in BMP concentrations across different lots of the same product.51,52 These factors highlight the importance of analyzing the efficacy of DBM in a product-specific context. Due to the heterogenicity of product development and processing, we suggest that for future studies the specific DBM products used in a study should be reported.
Several studies in our review investigated DBM used alone and not in combination with allograft bone chips, autologous local bone, or synthetic granules such as hydroxyapatite. Kim et al published a retrospective cohort study (level III evidence) with 100% fusion of Grafton DBM alone in an ACDF procedure. 38 Roh et al published a retrospective cohort study (level III evidence) with 97% fusion of Grafton DBM alone in an LLIF procedure. 45 Lee et al published a case series (level IV evidence) with 73% fusion of Grafton DBM alone in an OLIF procedure. 47 Baumann et al published a retrospective cohort study (level III evidence) with 94% fusion of Synthes DBX alone in an instrumented PLF procedure. 33 Ryu et al published a case series (level IV evidence) with 100% fusion of Synthes DBX alone in a posterior cervical procedure. 37 All of these studies consisted of DBM processed aseptically without the use of terminal irradiation. Hyun et al published an RCT study (level I evidence) with 78% fusion of Rafugen in a TLIF procedure. 32 Lee et al published a retrospective cohort study (level III evidence) with 94% fusion of Orthoblast II in an ACDF with a cortical allograft ring. 40 Both Rafugen and Orthoblast II are terminally processed with irradiation. These studies support the use of DBM used alone, but clinical evidence is more limited compared to that of DBM used in combination with other materials.
The Use of DBM for Cervical Fusion Procedures Was Associated With Similar Fusion Rates and Fewer Complications Compared to the Use of Iliac Autograft
Studies reporting the clinical use of DBM products for cervical spine procedures comprised about one-third of all included studies and 2/3 randomized studies. Three of these, including 1 RCT (level I evidence) and 2 retrospective cohort studies (level III evidence) compared DBM to iliac autograft in ACDF procedures and reported no significant difference in fusion rates between treatment groups. Overall, all studies of DBM in cervical fusion did report high fusion rates (100% in 3 of 5 studies) or noninferiority of the DBM products. Studies in which ICBGs were used showed significantly greater blood loss in ICBG patients. A 2016 review of DBM use in ACDF procedures by Zadegan et al included all published studies to date and found 1 additional randomized study that compared DBM with freeze-dried allograft to autograft and reported non-inferior fusion results.23,53 There were several features of this study conferring a high-risk of bias, though, and Zadegan et al demonstrated a lack of high-quality evidence for DBM use in ACDF procedures. The findings of our review also indicate this, with the majority of our included studies constituting level III-IV evidence (67%). Furthermore, our review included only 1 study of DBM in posterior cervical fusion, which was a retrospective case series involving a small number of patients in which titanium mesh cages filled with DBM were used in atlantoaxial fusion (Level IV evidence). 37
DBM is Non-inferior to Iliac Autograft for Posterior Lumbar Fusion
Other studies in our review investigated DBM products for lumbar spine procedures, most commonly posterior lumbar fusions. Two retrospective cohort studies (level III evidence) compared DBM alone (without other graft products) to iliac autograft for posterior lumbar fusion and found no significant differences in fusion rate between the groups. The remaining studies used DBM products for posterolateral fusions and various lumbar interbody fusion procedures, and most indicate high or noninferior fusion rate in the DBM treatment groups. Among all studies of DBM in lumbar fusion, Luo et al were the only authors who reported a significantly lower fusion rate in the DBM group, concluding that DBM was inferior to BCP for two-level PLFs.
Hydroxyapatite With DBM Results in Similar Fusion Rates Compared to Autograft and Higher Fusion Rates Compared to Hydroxyapatite Alone for Lumbar Fusion Procedures
Hydroxyapatite with DBM was also investigated by several studies in our review. Three lumbar spine studies, including 2 interbody fusion and 1 PLF study, investigated HA with DBM compared to autologous local bone, ICBG, and HA alone. Both studies comparing HA-DBM to autograft reported no difference in fusion rates (level II and III evidence), and the study that compared HA-DBM to HA alone reported higher fusion in the group receiving DBM, though it was not statistically significant (level II evidence).36,44,48 Overall, these results suggest the noninferiority of HA plus DBM to autograft in lumbar fusions.
Clinical Implications and Suggested Algorithm
Based on the synthesis of available clinical data, a pragmatic, procedure-specific algorithm for DBM use can be proposed. In cervical fusion, particularly ACDF, DBM demonstrates consistently high fusion rates when used as an autograft extender, with several studies reporting noninferior fusion compared to ICBG and reduced donor-site morbidity. Given the relatively favorable biologic environment of the interbody space and the lower graft volume requirements, aseptically processed, fiber-based DBM used as an ICBG extender represents a reasonable first-line adjunct in ACDF, especially in single-level procedures or in patients in whom avoidance of iliac crest harvest is desirable.
A similar approach may be applied to PLF, where DBM is most appropriately used as an autograft extender rather than a stand-alone graft. Across included PLF studies, fusion rates using DBM combined with local autograft were generally comparable to ICBG, particularly in single-level or short-segment constructs. In this setting, aseptic fiber-based DBM may be favored over particulate or terminally irradiated formulations, as preclinical and clinical data suggest superior osteoconductive structure preservation and potentially greater osteoinductive capacity. This is particularly relevant in the posterolateral environment, which is more biologically demanding than interbody fusion beds. However, caution is warranted in long-segment or multi-level PLF, where graft volume requirements are substantially higher and fusion demands are increased. One included study demonstrated inferior fusion rates for DBM compared with biphasic calcium phosphate in two-level PLF, highlighting that DBM performance may be more variable in this context. 47 Accordingly, in multi-level PLF, DBM should be used judiciously as a supplement to robust local autograft, and surgeons should consider alternative or additional biologic strategies when host or construct-related risk factors for pseudarthrosis are present.
Limitations
This systematic review has several important limitations that should be considered when interpreting the findings. First, the overall quality of evidence remains limited. Most included studies were retrospective and nonrandomized, with relatively small sample sizes and heterogeneous control groups, restricting the ability to draw definitive conclusions regarding the comparative efficacy of DBM across procedures and product formulations. In addition, DBM was frequently used in combination with local autograft, synthetic materials, or other biologics, making it difficult to isolate the independent contribution of DBM to fusion outcomes.
Second, there was substantial methodologic heterogeneity across studies, including variability in surgical indications, number of fused levels, graft volumes, and DBM formulations. Fusion assessment methods were inconsistent, ranging from plain radiographs to CT-based grading systems, with differing definitions of successful fusion. This variability limits cross-study comparability and precluded meaningful quantitative synthesis or meta-analysis.
Third, product-specific factors—including DBM form (fiber vs particulate), sterility processing method, carrier composition, and relative DBM content—were not consistently reported or controlled for, despite known biologic variability among commercial products. Similarly, lot-to-lot variability in osteoinductive potential and BMP content could not be assessed from the available clinical data.
Finally, clinical outcomes beyond radiographic fusion were incompletely reported. Revision surgery, pseudarthrosis-related reoperation, and patient-reported outcomes were inconsistently captured, and none of the included studies incorporated cost or economic analyses. As a result, conclusions regarding the relative value of DBM compared with other graft options remain limited. Taken together, these limitations highlight gaps in the existing literature and underscore the need for more rigorous, standardized investigation.
Future Directions
Advancing the clinical understanding of DBM in spinal fusion will require prospective, procedure-specific randomized controlled trials, particularly in posterior lumbar and multilevel constructs where fusion demands are greatest and outcomes appear more variable. To enhance consistency and interpretability across studies, future trials should incorporate standardized CT-based fusion assessment, such as the Tan et al fusion grading scale, which allows more precise differentiation between complete fusion, partial fusion, and pseudarthrosis and minimizes variability associated with plain radiographic criteria. 58
Equally important is the integration of biologic characterization alongside clinical outcomes. Prior experimental work has demonstrated substantial variability in BMP concentration, protein preservation, and elution kinetics across DBM formulations and sterility processing methods. Incorporating BMP quantification and elution assays into clinical trial design may help establish biologic–clinical correlations and clarify why certain DBM products perform differently in more challenging fusion environments, including multilevel posterolateral fusion.
From a health systems perspective, economic evaluation represents a critical gap in the existing literature. Despite DBM frequently being selected to avoid iliac crest harvest or to reduce reliance on recombinant biologics, none of the available studies have formally assessed cost or cost-effectiveness. Future investigations should therefore include economic endpoints, such as graft-related costs, operative time, donor-site morbidity, revision and reoperation rates, and quality-adjusted life years (QALYs), to better define the relative value of DBM compared with ICBG, synthetic grafts, and rhBMP-2 within value-based spine care models.
Conclusions
Most studies of DBM in spinal fusion within the past 10 years have investigated its use as an autograft extender compared to other bone graft materials or other DBM products. Studies commonly reported no significant difference in fusion outcomes between treatment groups, though the nonrandomized, retrospective nature of most studies with few having adequate control groups contributes to a low overall quality of evidence. However, DBM was studied more frequently in ACDF and PLF procedures, and our results suggest its noninferiority to ICBG for these cases. Similarly, HA plus DBM appears to be noninferior to autograft for lumbar fusion procedures. Additional randomized controlled trials are needed to better evaluate the clinical efficacy of DBM products, particularly in lumbar and posterior cervical spine procedures. The biggest challenge is the lack of detailed scientific study design and the heterogenicity in product development. These factors prevent a comprehensive understanding of current technology. Nevertheless, there is no doubt that a better insight into product development and technology applications can serve our future patients better.20,59-65
Footnotes
Ethical Considerations
Ethics approval was not required for this systematic review.
Author Contributions
Conceived and designed the analysis M.B., C.C. and F.L.V.
Data collection: M.B. and B.M.
Data analysis and interpretation: M.B. and B.M.
Preparation of manuscript draft: M.B., B.M., and C.C.
Critical manuscript revision: M.Q., A.F.P. and F.L.V.
Approval of final manuscript draft: M.B., B.M., C.C., M.Q., A.F.P. and F.L.V.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All datasets generated during and/or analyzed in this study are available from the corresponding author upon reasonable request.