
Abstract
Study Design
Retrospective cohort study.
Objective
To compare in-hospital mortality, complications, and resource utilization among patients undergoing fusion, decompression/discectomy, or instrumentation for spine trauma at Level I vs Level II trauma centers.
Methods
The National Trauma Data Bank was queried for adult patients with isolated spine trauma who underwent fusion, decompression/discectomy, or instrumentation at a Level I or Level II center. Multivariable logistic and linear regression models were used to adjust for patient demographics, injury severity, comorbidities, and hospital characteristics, comparing in-hospital mortality, complications, and length of stay (LOS).
Results
We identified 10 295 patients (6588 at Level I; 3707 at Level II). Level I patients were younger, had more severe spinal injuries, and had a higher incidence of spinal cord injury, particularly involving the cervical spine. Unadjusted outcomes showed similar mortality, but longer hospital and ICU LOS at Level I centers. After risk adjustment, treatment at a Level I center was associated with a 34% lower adjusted odds of in-hospital mortality (OR 0.66; 95% CI 0.46-0.96; P = .030). There were no significant differences in adjusted odds of any in-hospital complication or in adjusted hospital and ICU LOS.
Conclusion
Treatment at a Level I trauma center was associated with a significant survival benefit for patients undergoing operative management for spinal trauma. This mortality advantage was achieved without increasing complications or LOS. Given the retrospective design, causality cannot be inferred. Nevertheless, these findings suggest that Level I centers are associated with a distinct survival advantage for this high-acuity patient population.
Introduction
Spinal trauma is a major public health concern in the United States, contributing substantially to morbidity, mortality, and healthcare expenditures.1-3 Management — especially when surgery is required — demands timely diagnosis, specialized surgical expertise, and coordinated perioperative care.4-6 To facilitate these processes and improve patient outcomes, regionalized trauma systems have been widely adopted.7,8 Within this framework, the American College of Surgeons (ACS) designates trauma centers at various levels based on case volume, resource availability, and research engagement. 9 The majority of patients with severe spinal trauma receive treatment at Level I and/or Level II centers, which are equipped to provide the most comprehensive care.
Previous research has demonstrated that Level I trauma centers offer a significant survival advantage for severely injured patients compared to non-trauma centers.10,11 This advantage is also observed in direct comparisons between trauma center levels, as evidenced by studies showing improved survival and better functional outcomes for patients treated at Level I centers compared to those at Level II centers.12,13 More specifically, for patients with traumatic spinal cord injuries (SCI), treatment at a designated trauma center was found to be associated with reduced risk of paralysis, and direct admission to a Level I center has been shown to result in greater neurological recovery than transfer from other facilities.14,15 Despite the established benefits of Level I trauma centers as a whole, there remains a paucity of studies that directly compare outcomes for spinal trauma patients treated at Level I vs Level II centers.
The analysis of national data from 2013 to 2015 by Baron et al remains one of the few direct comparisons of outcomes in this population, using an older ACS Trauma Quality Improvement Program (TQIP) cohort and a mixed operative/non-operative sample. 16 While patients at Level II centers had higher overall complication rates, those at Level I centers experienced increased rates of certain infectious complications, with no clear mortality advantage. 16 Notably, the authors recognized the ambiguity of these findings and emphasized the need for additional research using alternative data sources to more clearly define the impact of trauma center designation. Since the study, contemporary trauma care has evolved—broader use of advanced intraoperative techniques and neuromonitoring, protocolized neurocritical care (early extubation, standardized VTE prophylaxis, and infection-prevention bundles), and more mature regional pathways—potentially shifting outcomes, particularly mortality, between Level I and II centers. Accordingly, an updated analysis using a recent, comprehensive national dataset is warranted to re-evaluate outcomes in operatively managed spine trauma.
To this end, the primary objective of our study was to compare in-hospital mortality, complications, and resource utilization for patients with spine trauma at Level I vs Level II trauma centers, using data from the 2023 National Trauma Data Bank. Additionally, we sought to control for patient-, injury-, and hospital-level confounders to isolate the independent effect of trauma center designation. We hypothesized that, following risk adjustment, treatment at a Level I trauma center would be associated with lower in-hospital mortality, but with similar rates of in-hospital complications and length of stay (LOS) despite higher patient acuity, compared to treatment at a Level II center in patients undergoing operative management for spinal trauma.
Methods
Data Source
We conducted a retrospective observational study using 2023 data from the American College of Surgeons (ACS) National Trauma Data Bank (NTDB). The NTDB is the largest aggregation of U.S. trauma registry data, maintained by the ACS as part of its Trauma Quality Programs. 17 It compiles standardized information submitted annually by participating trauma centers on patient demographics, injury characteristics, interventions, and outcomes, thereby serving as a nationally representative resource for trauma research. Data undergo quality checks before release in the Participant Use File (PUF). Because the NTDB contains de-identified information, this study was exempt from Institutional Review Board (IRB) approval.
Cohort Identification and Exclusion Criteria
Spine trauma cases were identified using Abbreviated Injury Scale (AIS) diagnoses limited to the spine body region, excluding encounters with any non-spine injury of moderate severity or greater. Isolated spine trauma was, therefore, defined as an encounter with at least one spine injury (AIS body region: Spine), permitting extra-spinal injuries only if AIS ≤2 and excluding any encounter with non-spine injuries of AIS ≥3. Interfacility transfers were excluded. We required a hospital length of stay (LOS) of at least 1 day; records with missing LOS were excluded. The cohort was restricted to ACS-verified Level I and Level II trauma centers.
We limited the analytic cohort to encounters without extra-spinal injuries of AIS ≥3 to reduce confounding from moderate-to-severe polytrauma, where early mortality, complications, and resource utilization may be predominantly driven by non-spinal injuries, like traumatic brain injury or major thoracoabdominal trauma, rather than the spine injury and its operative management. This restriction was intended to better isolate spine-specific associations with trauma center level.
Operative Cohort Classification
Within the spine trauma cohort, patients were classified as operated if they underwent an ICD-10-PCS procedure consistent with spine surgery; eligible procedures included fusion, decompression/discectomy, and instrumentation. Spinal cord injury (SCI) was defined from ICD-10-CM diagnoses using category-level groupings for acute traumatic SCI at the cervical, thoracic, and lumbosacral levels.
Injury Severity
Spine injury severity was quantified as the maximum AIS severity within the spine region (range 1-6) and analyzed in 4 categories: 1-2 (minor/moderate), 3 (serious), 4 (severe), and 5-6 (critical/max).
Mechanism of injury was derived from ICD-10-CM external cause-of-injury codes recorded in the NTDB PUF. Encounters were categorized as relating to falls (W00–W19), motor vehicle/transport-related mechanisms (V00–V99), intentional self-harm (X60–X84), or other (all remaining external-cause codes, including assault, undetermined intent, and other specified mechanisms).
Comorbidities
Preinjury comorbidities were mapped to a 12-item comorbidity count comprising hypertension, dementia, diabetes, bleeding disorder, congestive heart failure, peripheral arterial disease, chronic obstructive pulmonary disease, cirrhosis, disseminated cancer, alcohol use disorder, substance use disorder, and chronic renal failure. The count was calculated as the sum of present conditions.
Hospital Characteristics and Arrival Physiology
Hospital bed size was categorized as ≤200, 201-400, 401-600, or >600 beds. Teaching status was grouped as community, non-teaching, or academic, taken directly from the NTDB facility teaching variable per NTDS definitions; in general, academic denotes a university/teaching hospital, whereas non-teaching and community denote non-academic facilities as categorized by the NTDB.
Patient Characteristics by Trauma Center Level
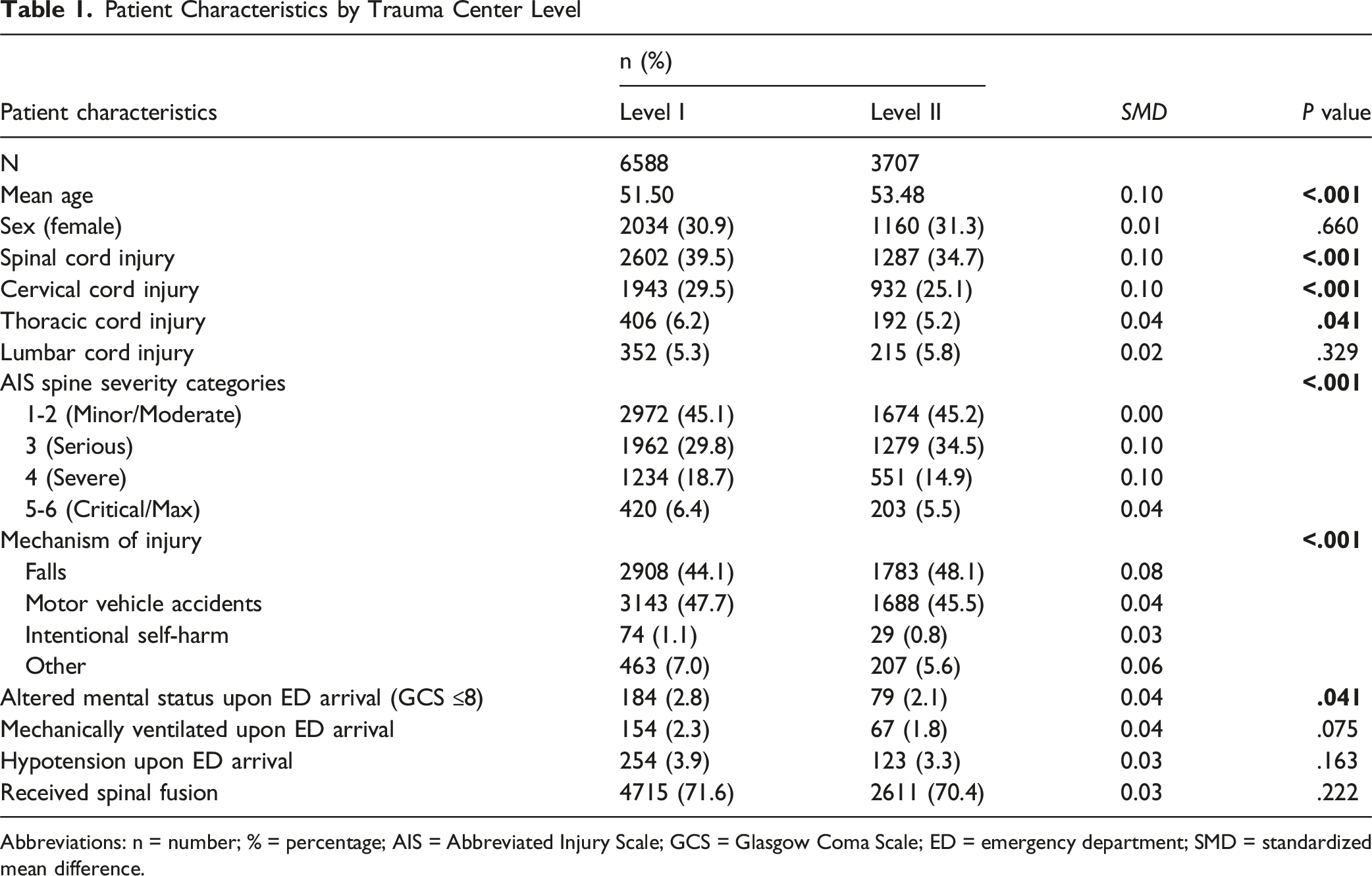
Abbreviations: n = number; % = percentage; AIS = Abbreviated Injury Scale; GCS = Glasgow Coma Scale; ED = emergency department; SMD = standardized mean difference.
Outcomes
Primary in-hospital complications were derived from standardized NTDB event indicators and included ventilator-associated pneumonia, catheter-associated urinary tract infection, unplanned intubation, deep vein thrombosis, delirium, pressure ulcer, cardiac arrest, pulmonary embolism, acute kidney injury, severe sepsis, acute respiratory distress syndrome, stroke, and unplanned ICU admission. A composite “any complication” and an “other complication” category (events outside the named list) were created. Secondary outcomes were in-hospital mortality, hospital LOS (days), and ICU days.
Statistical Analysis
Patient, injury, and hospital characteristics were summarized by trauma center level. Records were excluded if they lacked key demographic or clinical variables necessary for risk adjustment, including trauma center level designation, age, sex, spinal cord injury flag, Glasgow Coma Scale (GCS ≤8) indicator, systolic blood pressure–based hypotension flag, or Injury Severity Score (ISS). After applying these criteria, 202 of 10 497 encounters (1.9%) were excluded due to missing data, yielding a final analytic cohort of 10 295 patients.
Group comparisons used t-tests for continuous variables and chi-square tests with Fisher’s exact test as needed for categorical variables. For binary outcomes (mortality; any/other complication; each named complication), multivariable logistic regression estimated the association with trauma center level (Level II as reference), adjusting for age, sex, spine-region AIS severity category, SCI, GCS ≤8, hypotension on arrival, hospital bed size, teaching status, and the 12-item comorbidity count. ISS was not included as a covariate because it is mathematically derived from AIS scores; therefore, including ISS alongside regional AIS severity measures would introduce collinearity and redundancy, potentially destabilizing model estimates. While mechanism of injury was included in descriptive tables to provide cohort context, it was not included in the multivariable models because our primary adjustment focused on downstream clinical severity markers (spine AIS category, SCI, and arrival physiology), which are the proximate determinants of triage decisions and in-hospital outcomes in this operative isolated spine trauma cohort. When rare events or separation were present, Firth bias-reduced logistic regression was used. Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs).
For continuous outcomes (LOS and ICU days), multivariable linear regression with the same covariate set was applied. To account for potential non-constant variance in the residuals, heteroskedasticity-robust standard errors were applied. Analyses were restricted to encounters with complete data across model covariates (listwise deletion). Of the 10 295 operative spine trauma encounters in 2023, 10 288 (99.9%) were included in the LOS model and 5516 (53.6%) were included in the ICU-days model after excluding records with missing values. The larger exclusion for ICU-days primarily reflects that, in the NTDB PUF, ICU days are frequently not populated for patients without an ICU stay; therefore, the ICU-days model should be interpreted as ICU LOS among encounters with documented ICU utilization. P values <.05 were considered statistically significant. All analyses were performed in R (version 4.3.3; R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Demographics
We identified 10 295 operative spine trauma encounters across ACS-verified centers in 2023: 6588 (64.0%) at Level I and 3707 (36.0%) at Level II. Level I patients were younger (51.50 vs 53.48 years, P < .001) with a similar female proportion (30.9% vs 31.3%, P = .660). Spinal cord injury (SCI) was more frequent at Level I (39.5% vs 34.7%, P < .001), driven by higher cervical (29.5% vs 25.1%, P < .001) and thoracic (6.2% vs 5.2%, P = .041) involvement; lumbar SCI was comparable (5.3% vs 5.8%, P = .329). Spine AIS distributions differed overall (P < .001): Level I had more severe (AIS 4: 18.7% vs 14.9%) and critical (AIS 5-6: 6.4% vs 5.5%) injuries, whereas Level II had more AIS 3 (34.5% vs 29.8%). Motor vehicle accidents were the predominant mechanism of injury at Level I centers (47.7% vs 45.5%, P < .001). Arrival physiology was broadly similar: although GCS ≤8 differed statistically, the absolute difference was small and of limited clinical relevance (2.8% vs 2.1%, P = .041), mechanical ventilation on arrival was comparable (2.3% vs 1.8%, P = .075), and hypotension rates were similar (3.9% vs 3.3%, P = .163). Treatment with spinal fusion was common and did not differ (71.6% vs 70.4%, P = .222; Table 1).
Hospital Characteristics
Hospital Characteristics by Trauma Center Level
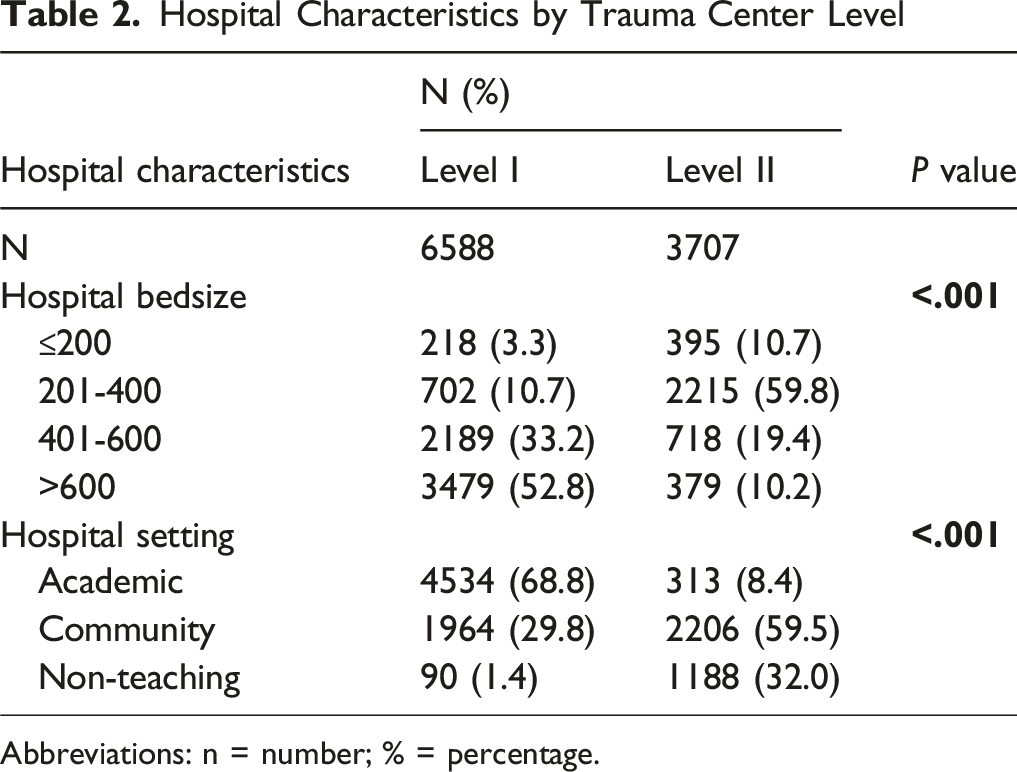
Abbreviations: n = number; % = percentage.
Unadjusted Outcomes
Complications and Hospital Course by Trauma Center Level
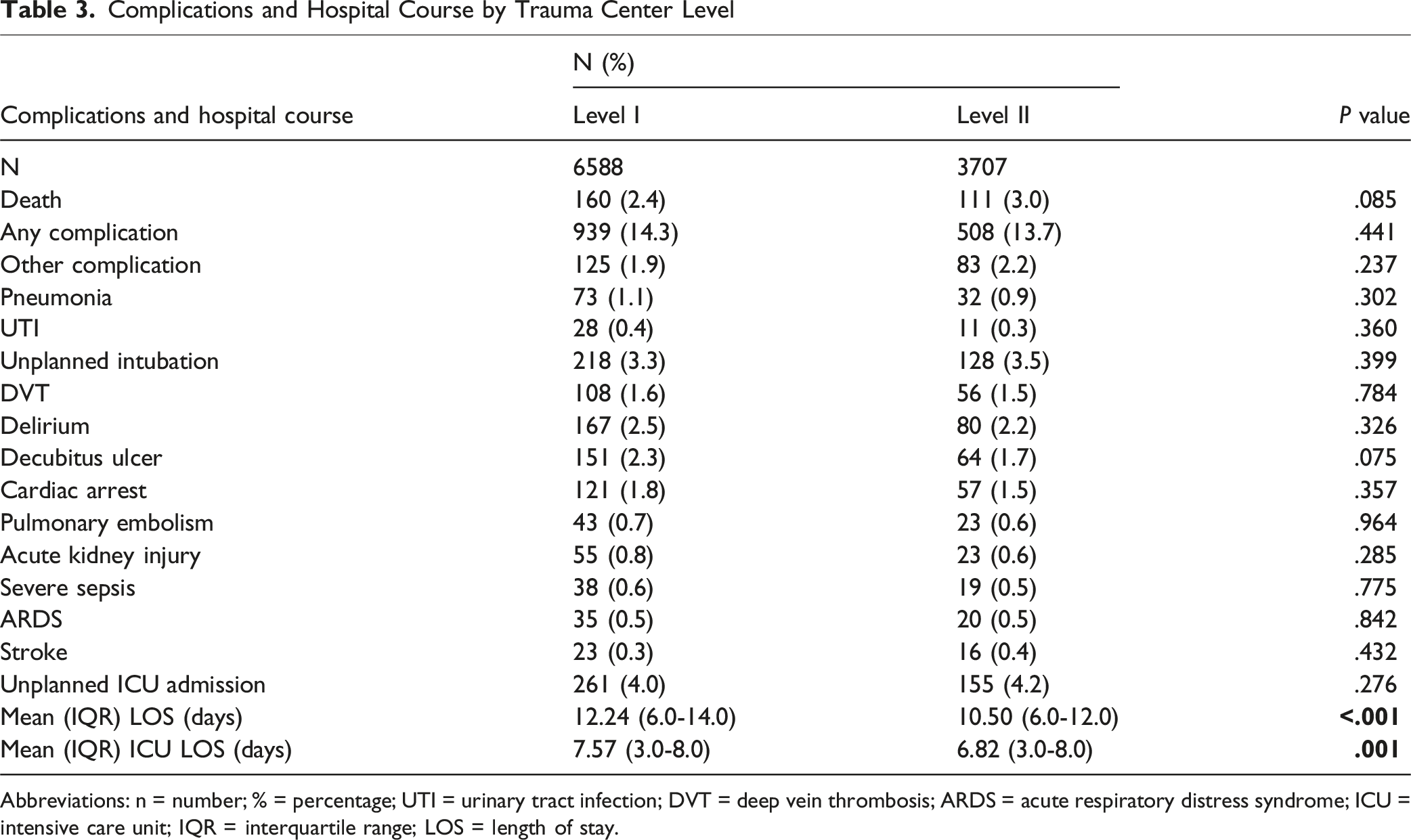
Abbreviations: n = number; % = percentage; UTI = urinary tract infection; DVT = deep vein thrombosis; ARDS = acute respiratory distress syndrome; ICU = intensive care unit; IQR = interquartile range; LOS = length of stay.
Adjusted Analyses
Multivariate Logistic Regression Analysis of Complications by Trauma Center Level
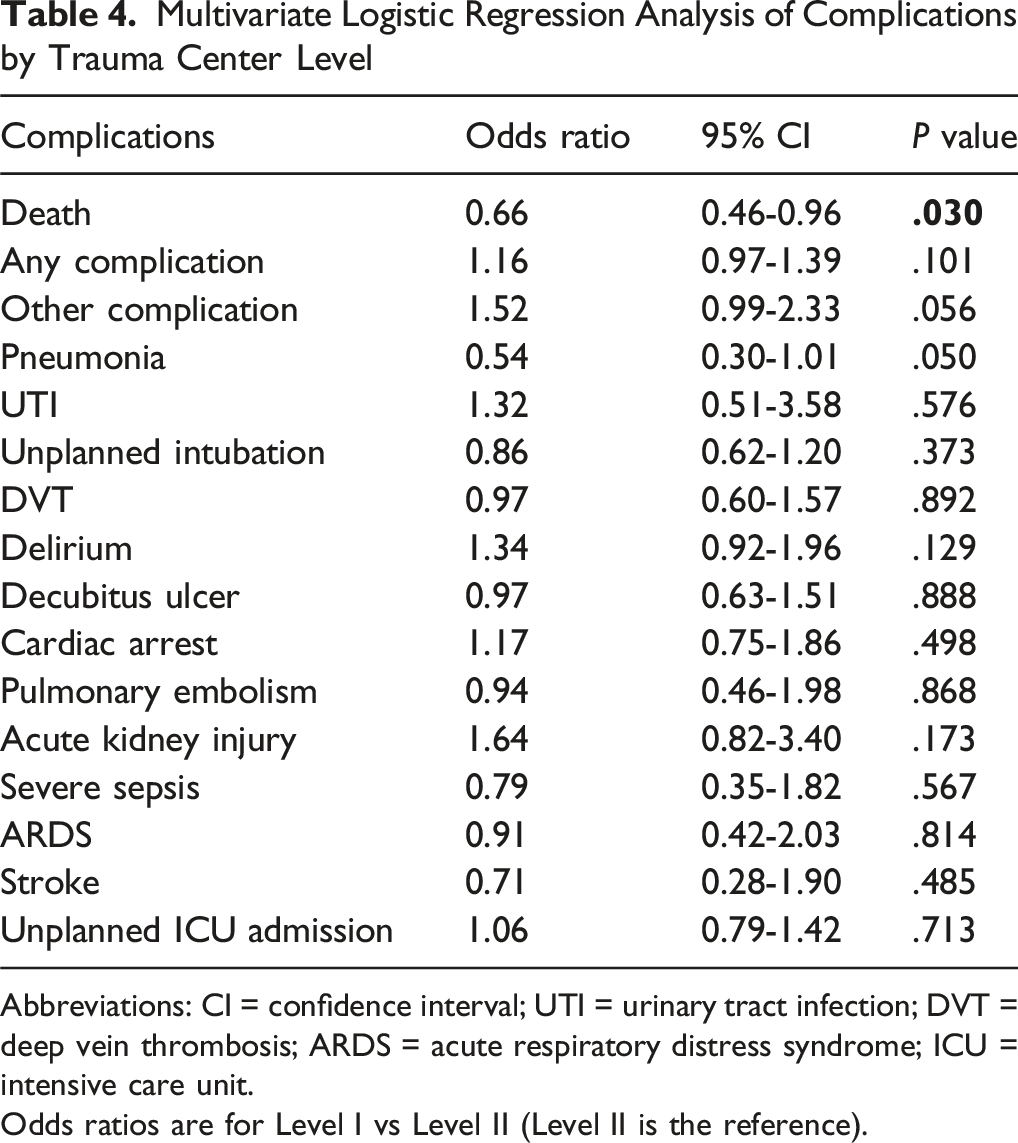
Abbreviations: CI = confidence interval; UTI = urinary tract infection; DVT = deep vein thrombosis; ARDS = acute respiratory distress syndrome; ICU = intensive care unit.
Odds ratios are for Level I vs Level II (Level II is the reference).
Multivariate Linear Regression of Hospital Course by Trauma Center Level

Abbreviations: CI = confidence interval; ICU = intensive care unit; LOS = length of stay.
Discussion
Spinal trauma remains a significant public health concern, with optimal management dependent on the resources and organization of trauma systems.1-3,5,6 Although regionalized trauma care has become the standard, the comparative advantages of Level I and Level II centers for patients with spinal trauma are not fully understood.7,8 While prior studies have established a survival benefit for severely injured patients at Level I centers, the study by Baron et al reported no mortality difference specifically among spine trauma patients.
16
An updated assessment using recent national data was due with advances in trauma care and system infrastructure over the past decade. As such, the present study aimed to compare in-hospital mortality, complications, and resource utilization among patients undergoing operative management for spinal trauma at Level I and Level II trauma centers using the 2023 National Trauma Data Bank. In unadjusted analyses, patients treated at Level I centers had longer hospital and ICU stays, with similar mortality and complications rates, despite greater injury severity. After adjustment for patient, injury, and hospital-level factors, however, treatment at a Level I center was independently associated with lower odds of in-hospital mortality, with no significant differences in complication rates or resource utilization. Although Level I centers managed a higher-acuity cohort, the mortality association persisted after adjustment for cervical SCI, GCS ≤8, hypotension, mechanical ventilation, spine AIS category, comorbidity burden, and hospital factors. Clinically, this suggests that resource concentration at Level I centers may improve early survival, while standardized perioperative and ICU pathways across centers help maintain similar complication rates and lengths of stay (Figure 1). Adjusted Odds Ratios: Level 1 versus Level 2 Trauma Centers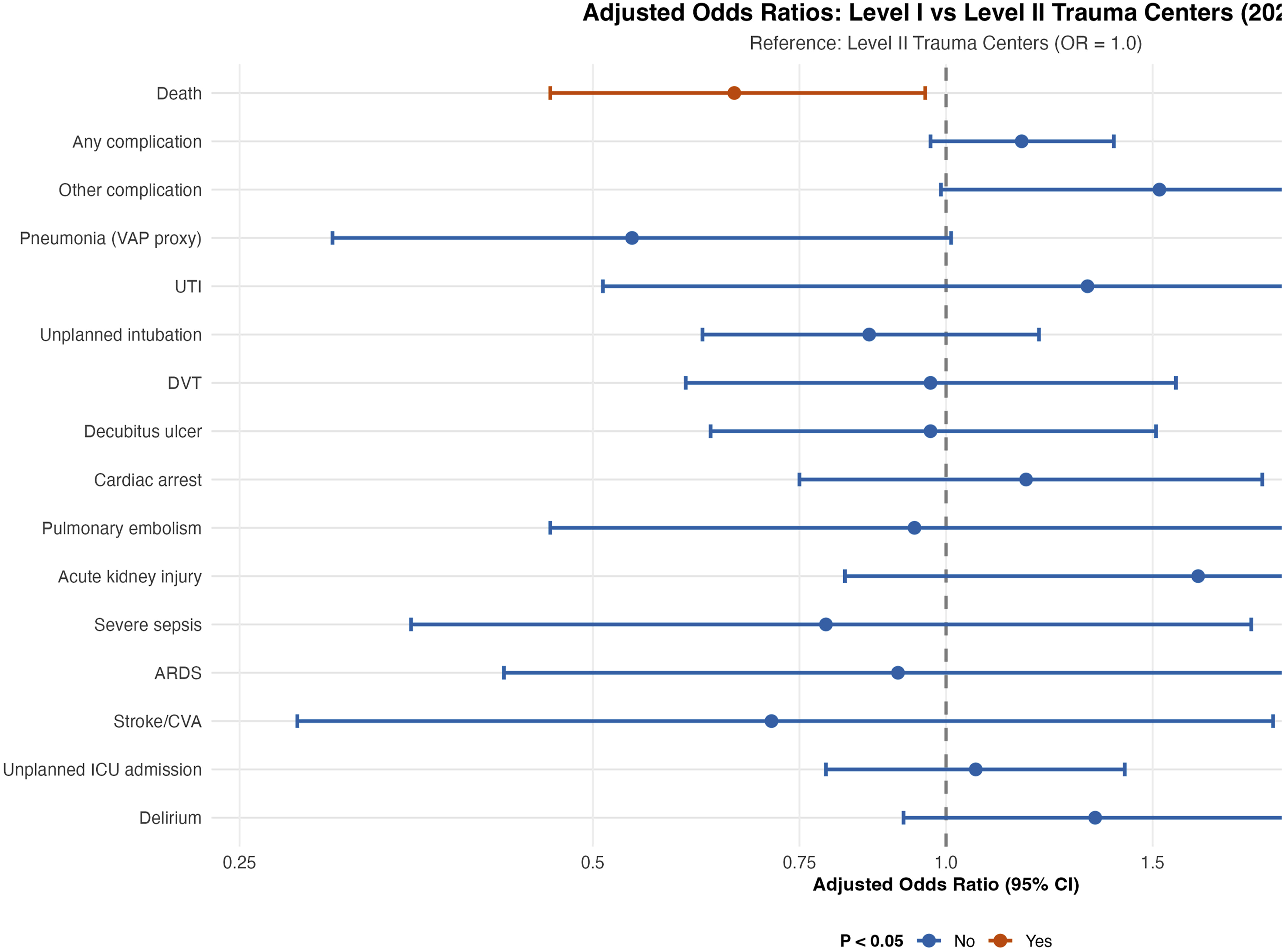
Several baseline differences in patient and hospital characteristics observed in this study align with existing literature. Patients treated at Level I trauma centers were younger, presented with more severe injuries as indicated by higher AIS scores, and exhibited a greater incidence of spinal cord injury, particularly at the cervical level. They were also more likely to arrive with altered mental status (GCS ≤8). A prior study by Cudnik et al similarly found that patients at Level I centers in Ohio were younger (43.6 years vs 50.9 years, P < .05) and had higher injury severity scores (15 vs 11, P < .05) compared to those at non-trauma centers. 12 Additionally, Amidei et al reported that cervical lesions were the most common among patients with traumatic spinal cord injuries (52.1%). 18 Collectively, these findings indicate that Level I centers care for a more severely injured patient population, consistent with their role as regional referral centers for complex trauma cases. Institutionally, Level I centers were primarily large, academic hospitals, with most having more than 400 beds, while Level II centers were generally smaller, community-based facilities. This distinction aligns with ACS verification criteria, which require Level I centers to serve as regional referral resources, support substantial teaching and research activities, and meet higher minimum patient volume thresholds.19,20
In bivariate analyses, in-hospital mortality rates were similar between Level I and Level II trauma centers. However, after adjusting for demographic factors, injury severity, and hospital characteristics in multivariate regression, care at a Level I center was independently associated with lower mortality. This finding contrasts with the prior study by Baron et al, which found no difference in mortality rates between Level I and Level II centers (OR 1.18; 95% CI 0.92-1.52; P > .10). 16 Similarly, an NTDB retrospective review on patients with combined traumatic brain injury and solid organ injuries also reported no mortality difference between trauma center levels. 21 In contrast, a study by Chalouhi et al demonstrated that in patients with severe traumatic brain injury, treatment at a Level II center was independently associated with in-hospital mortality (OR 1.2; 95% CI 1.03-1.37; P = .01). 22 Additionally, a systematic review by Van Ditshuizen et al found that for severely injured patients, admission to a Level I trauma center offered a survival benefit compared to Level II centers. 23 Taken together, these mixed findings suggest that the survival benefit associated with Level I trauma centers may be specific to certain high-acuity populations. Within this context, the current study provides important evidence by demonstrating a significant mortality benefit for operative spine trauma patients treated at Level I centers. This advantage is likely attributable to the greater availability of specialized neurosurgical and orthopedic spine expertise, advanced intraoperative monitoring, and dedicated neurocritical care teams more consistently available at these higher-level institutions. 20 Beyond specialist availability, Level I centers typically maintain 24/7 in-house spine/neurosurgical coverage and operating room readiness, enabling earlier definitive decompression/stabilization when indicated. They also offer advanced intraoperative monitoring, structured trauma triage pathways (prehospital/hospital activation with expedited imaging and OR access), and protocolized neurocritical care (eg, standardized ICP/MAP targets, ventilatory strategies, and targeted hemodynamics) with multidisciplinary coordination among trauma surgery, anesthesia, and rehabilitation services. Together, these structural and process advantages may translate into faster time-to-operation and improved survival for operative spine trauma at Level I centers; however, the NTDB does not capture key process-level measures (such as staffing or protocol adherence), so these mechanisms cannot be confirmed and causality cannot be inferred from this retrospective analysis.
In the present study, the rates of postoperative complications were comparable between Level I and Level II trauma centers. Our findings contrast those of Baron et al, who reported that, although Level I centers had lower overall complication rates, they exhibited higher rates of infectious complications such as pneumonia and urinary tract infections (UTIs). 16 This divergence likely reflects the evolution of the trauma systems and critical care practices over the past decade.24-28 For instance, a study by Katoka et al found that the implementation of an infection prevention bundle in the ICU resulted in declines of 58.6%, 56.7%, and 82.6% in bloodstream infections, urinary tract infections, and ventilator-associated pneumonia, respectively, from 2007 to 2017 compared to 1996 to 2006. 29 Therefore, the implementation of evidence-based infection control protocols, especially those addressing ventilator-associated pneumonia and catheter-associated urinary tract infections, may have been particularly effective for the higher-acuity patients managed at Level I centers. These advances parallel national quality initiatives from the ACS Trauma Quality Program and the TQIP, which promote standardized benchmarking, best-practice guidelines, and infection-prevention pathways across verified trauma centers. 17 Consistent with this, our adjusted analysis demonstrated a non-significant trend toward lower odds of pneumonia at Level I centers, effectively reversing the earlier observed risk. These improvements suggest that advances in multidisciplinary care pathways and infection prevention have enabled Level I centers to achieve complication rates comparable to those of Level II centers, while continuing to provide specialized care for complex trauma patients.
After adjusting for patient, injury, and hospital-level factors, we found that both hospital and ICU lengths of stay were similar for patients treated at Level I and Level II trauma centers. At the unadjusted level, longer LOS at Level I centers likely reflects case-mix and system factors—greater multisystem injury complexity requiring sequential consultations and rehabilitation/skilled-nursing placement delays across wider referral regions—rather than inefficiency. In contrast, Baron et al found that Level I centers were associated with longer hospital and ICU stays, even after adjusting for similar factors. 16 One possible explanation for this discrepancy is the differing complication profiles between the 2 studies. In the analysis by Baron et al, Level I centers experienced higher rates of infectious complications, such as pneumonia and UTIs, which are well-established drivers of prolonged hospital and ICU stays.16,30-32 However, in the present study, the rates of these complications were not significantly different between Level I and Level II centers. Therefore, the comparable complication rates for our cohort likely account for the comparable resource utilization, suggesting that Level I centers have mitigated the infection risks that previously contributed to longer stays.
The current study is not without limitations. First, its retrospective design limits our ability to establish causality and introduces the potential for selection bias. Additionally, because we excluded interfacility transfers, mortality comparisons may be biased if higher-acuity patients are preferentially transferred to Level I centers, potentially underestimating a true survival advantage. The NTDB does not capture cause-of-death detail, limiting mechanistic inference and precluding comparison of specific fatal events by center level; results should be interpreted as associations rather than causal effects. Second, the National Trauma Data Bank (NTDB), while comprehensive, is subject to billing and coding errors that may result in misclassification of inpatient complications. Third, our analysis was restricted to in-hospital outcomes. The NTDB does not capture post-discharge data, including long-term mortality rates, readmission or reoperation rates, or patient-reported functional outcomes. As a result, we were unable to evaluate whether the observed in-hospital mortality benefit at Level I centers translates to improved long-term recovery. In addition, our observed complication rate of 14% is likely conservative; complications in the NTDB may be under-reported due to variable documentation and lack of post-discharge capture, potentially attenuating between-level differences. Similarly, because in-hospital mortality was infrequent in this cohort, statistical power and precision are limited, so small between-level differences may not be detectable. Importantly, by excluding encounters with non-spine injuries of AIS ≥3, the isolated spine trauma cohort may not be fully generalizable to polytrauma patients, in whom outcomes may be more strongly influenced by concomitant injuries and their time-sensitive management. Fourth, the NTDB does not provide granular data on the specific surgical technique used, including the number of levels fused. Timing to operative decompression/stabilization is an important determinant of outcomes in spine trauma, but operative timing was not captured in this analysis and therefore could not be adjusted for. These unmeasured variables may influence outcomes and represent a potential source of confounding. Finally, despite our robust multivariable adjustment, the potential for residual confounding from unmeasured variables remains. For instance, mechanism of injury was not directly included in regression models and may not be fully captured by the available severity and physiologic covariates, which could influence triage patterns and outcomes. Nonetheless, the current study is strengthened by its use of a large, nationally representative dataset, which enhances the generalizability of our findings. By focusing on a specific, high-acuity cohort of operative spine trauma patients, our analysis offers valuable, updated evidence that clarifies the mortality benefit of Level I trauma centers.
Conclusion
We sought to provide an updated comparison of outcomes for operative spine trauma patients treated at Level I vs Level II centers using the NTDB. After adjusting for significant differences in patient acuity and hospital characteristics, treatment at a Level I center was independently associated with lower in-hospital mortality. Notably, this survival benefit was achieved without a concomitant increase in complication rates or length of stay. These findings contrast with prior literature and suggest that, in the context of modern trauma care, Level I centers may confer a survival advantage for this high-acuity patient population, underscoring their critical role within a regionalized trauma system. Findings support preferential triage of complex operative spinal trauma to Level I centers, particularly when early decompression/stabilization or advanced neurocritical care is anticipated.
Footnotes
ORCID iDs
Ethical Considerations
This study utilized a publicly available national database. As such, Institutional Review Board approval was not required for the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available upon reasonable request.