
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Gender appears to play in important role in surgical outcomes following acute cervical spine trauma, with current literature suggesting males have a significantly higher mortality following spine surgery. However, no well-adjusted population-based studies of gender disparities in incidence and outcomes of spine surgery following acute traumatic axis injuries exist to our knowledge. We hypothesized that females would receive surgery less often than males, but males would have a higher 1-year mortality following isolated traumatic axis fractures.
Methods:
We performed a retrospective cohort study using Medicare claims data that identified US citizens aged 65 and older with ICD-9 (International Classification of Diseases, Ninth Revision) code diagnosis corresponding to isolated acute traumatic axis fracture between 2007 and 2014. Our primary outcome was defined as cumulative incidence of surgical treatment, and our secondary outcome was 1-year mortality. Propensity weighted analysis was performed to balance covariates between genders. Our institutional review board approved the study (IRB #16-0533).
Results:
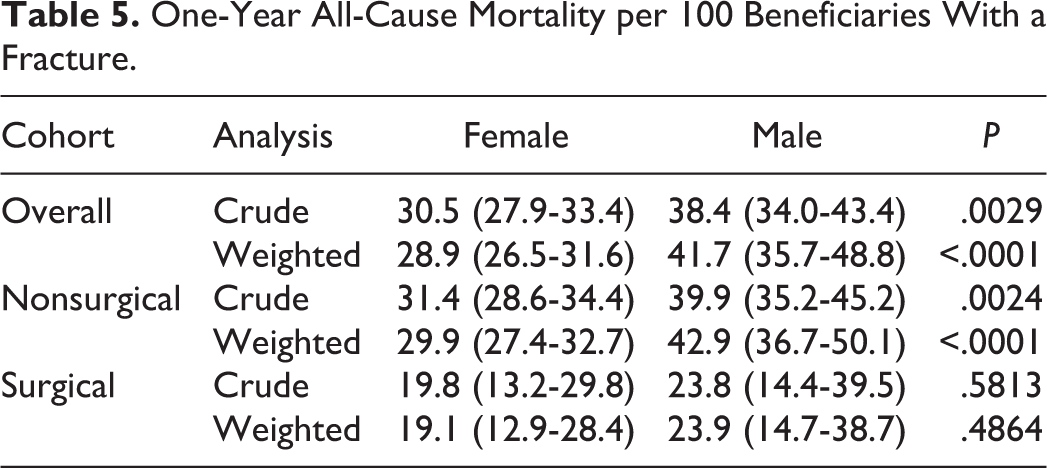
There was no difference in incidence of surgery between males and females following acute isolated traumatic axis fractures (7.4 and 7.5 per 100 fractures, respectively). Males had significantly higher 1-year weighted mortality overall (41.7 and 28.9 per 100 fractures, respectively, P < .001).
Conclusion:
Our well-adjusted data suggest there was no significant gender disparity in incidence of surgical treatment over the study period. The data also support previous observations that males have worse outcomes in comparison to females in the setting of axis fractures and spinal trauma regardless of surgical intervention.
Introduction
Gender plays an important role in surgical outcomes after spine trauma. 1 Traumatic fracture of the axis, or the second cervical vertebra, is the most common cervical spine injury in the elderly and associated with high morbidity. 2 Gender differences in female cervical spine morphology may contribute to injury susceptibility, with axis fractures occurring more commonly in females, although males have been shown to have a higher mortality. 3 -5 Surgical intervention can promote fracture healing through internal stabilization but also introduces perioperative risk, especially for those with comorbid health conditions. 4,6 Elderly females are at a higher risk for osteoporotic disease of the cervical spine, which may limit surgical options and increase the risk of hardware failure. 7 However, females appear to fair better regardless of treatment. 4,8 Recent studies of morbidity and mortality after spine surgery showed that males had a 63% higher odds of mortality compared with females after spine surgery despite no difference in complications. 9,10 So, despite the predilection for osteoporotic disease and relative susceptibility of cervical spine injury in older females, it is unclear whether or not this has led to significant gender disparity in the surgical treatment and outcomes at a population level. No well-adjusted population studies of gender disparities in spine surgery treatment exist to our knowledge. Our specific aim was to estimate cumulative incidence of surgical treatment and 1-year cumulative mortality by gender among older adults with acute traumatic axis fractures. We hypothesized that (1) females would receive surgery less often than males but that (2) males would have a higher 1-year mortality.
Methods
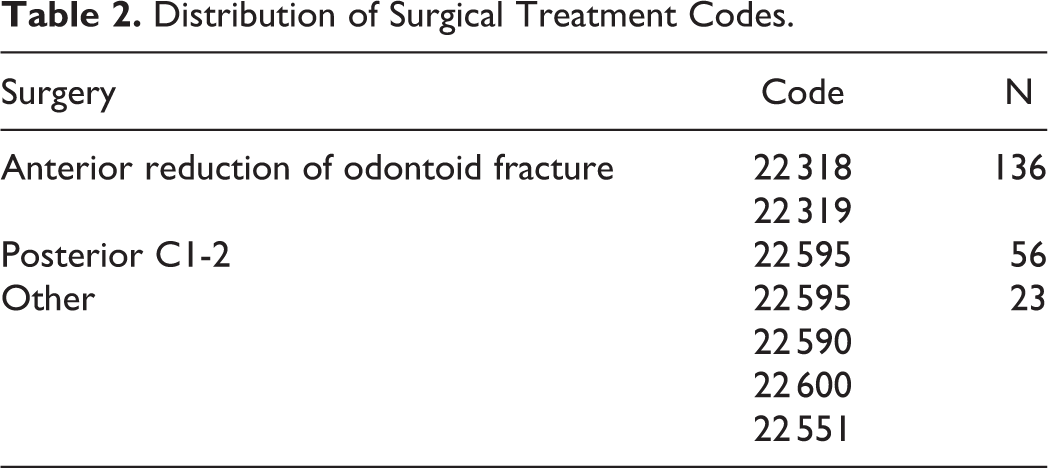
We performed a retrospective cohort study using Medicare claims data in US citizens aged 65 and older. We used a 20% random sample of all fee-for-service beneficiaries with concurrent Medicare Parts A, B, and D coverage in at least 1 month between 2007 and 2014. Our institutional review board approved the study (IRB #16-0533). Eligible beneficiaries were continuously enrolled in fee-for-service Medicare for at least 12 months. We defined isolated acute traumatic axis fractures according to the following inclusion criteria: an inpatient hospitalization with a primary, secondary or tertiary discharge 805.02 ICD-9 (International Classification of Diseases, Ninth Revision) code, or a physician claim with 805.02 as the primary diagnosis during a hospitalization. Patients were excluded if they had any cervical fracture or spinal cord injury in the prior 12 months, except for outpatients who had eligible inpatient claims within 30 days of index hospitalization. We also excluded patients with codes for severe brain injury, skull fractures, coma, concurrent atlas-axis fractures, multiple cervical fractures, and pathologic fractures. Surgical axis fracture treatment was defined by preselected Common Procedure Terminology (CPT; 22 318, 22 319, 22 551, 22 590, 22 595, 22 600) codes during the index hospitalization. Due to the nature of claims data, only E code and the race variable had missing data on predictors of surgery. “No E code” was included as a categorical variable, and beneficiaries with unknown race were grouped with “Other” race.
The primary outcome was cumulative incidence of surgical treatment and secondary outcome was 1-year cumulative mortality. Primary exposure was gender. In order to balance baseline (prefracture) variables potentially affecting surgery and mortality between men and women, we used propensity weighting (Table 1). Both males and females were weighted to the overall population so that the final proportion of each covariate was similar in males and females. We did this by first estimating the probability of being female based on all measured covariates and then weighting each patient by the inverse of the probability of their actual gender (inverse probability weights). This resulted in pseudo-cohorts of men and women with similar covariate distributions. Standardized absolute mean differences of less than 0.1 are usually regarded as an indication of good covariate balance. This removes confounding by measured covariates by balancing, for example, comorbid conditions that may affect their surgical candidacy and enables us to directly compare the 2 genders. Once groups were weighted, the incidence of surgery for each gender was calculated. In a similar fashion, propensity weights were used to estimate 1-year mortality. For this analysis we stratified by surgical treatment to estimate gender disparity in 1-year mortality (1) overall, (2) without surgery, and (3) with surgery. We generated cross-tabulations and used Pearson χ2 tests to compare distributions. Data is reported as the cumulative incidence proportions over the specified timeframe for each outcome variable.
Incident Fracture Population Characteristics (Crude and Weighted Baseline Characteristics by Gender).
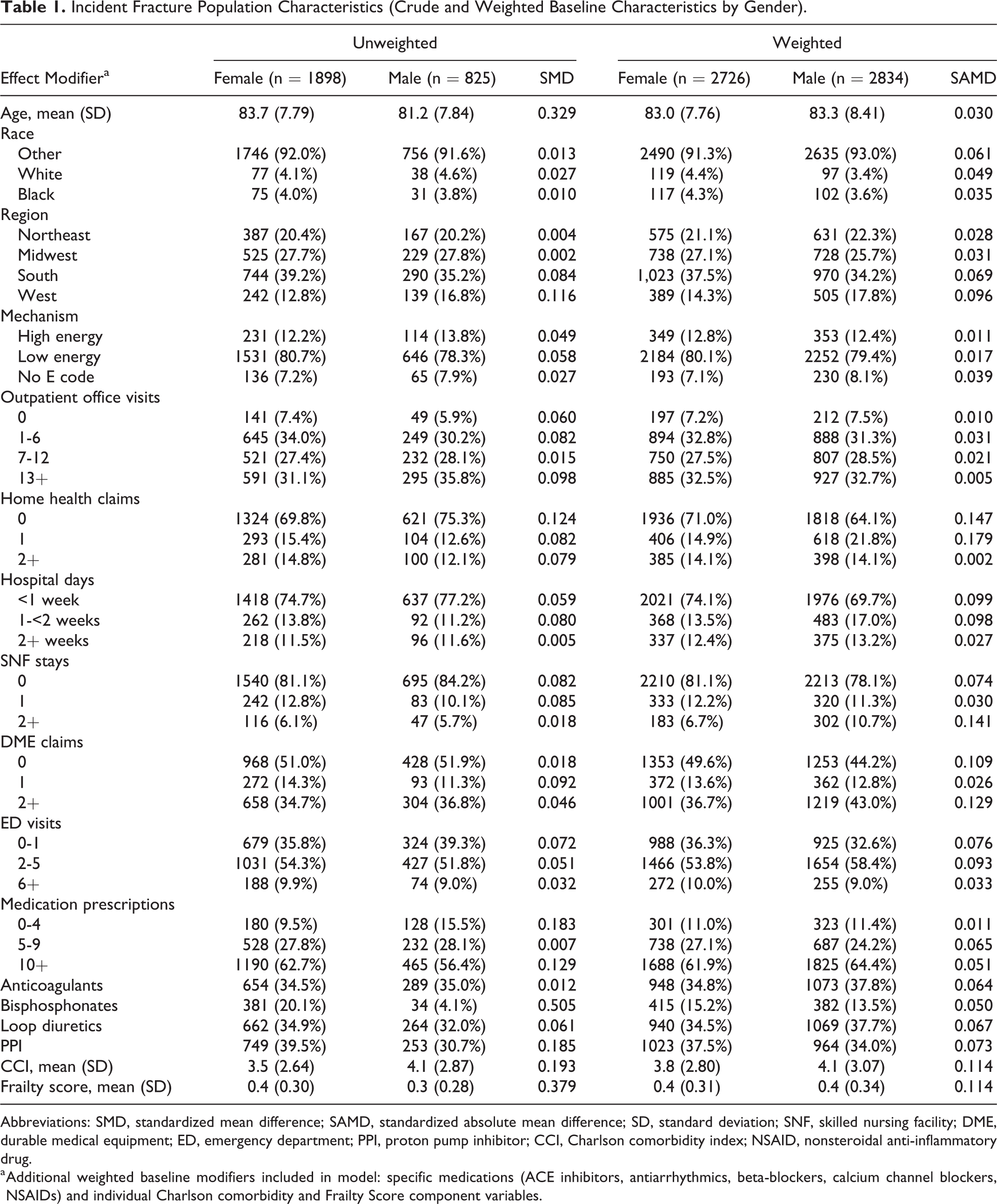
Abbreviations: SMD, standardized mean difference; SAMD, standardized absolute mean difference; SD, standard deviation; SNF, skilled nursing facility; DME, durable medical equipment; ED, emergency department; PPI, proton pump inhibitor; CCI, Charlson comorbidity index; NSAID, nonsteroidal anti-inflammatory drug.
a Additional weighted baseline modifiers included in model: specific medications (ACE inhibitors, antiarrhythmics, beta-blockers, calcium channel blockers, NSAIDs) and individual Charlson comorbidity and Frailty Score component variables.
Results
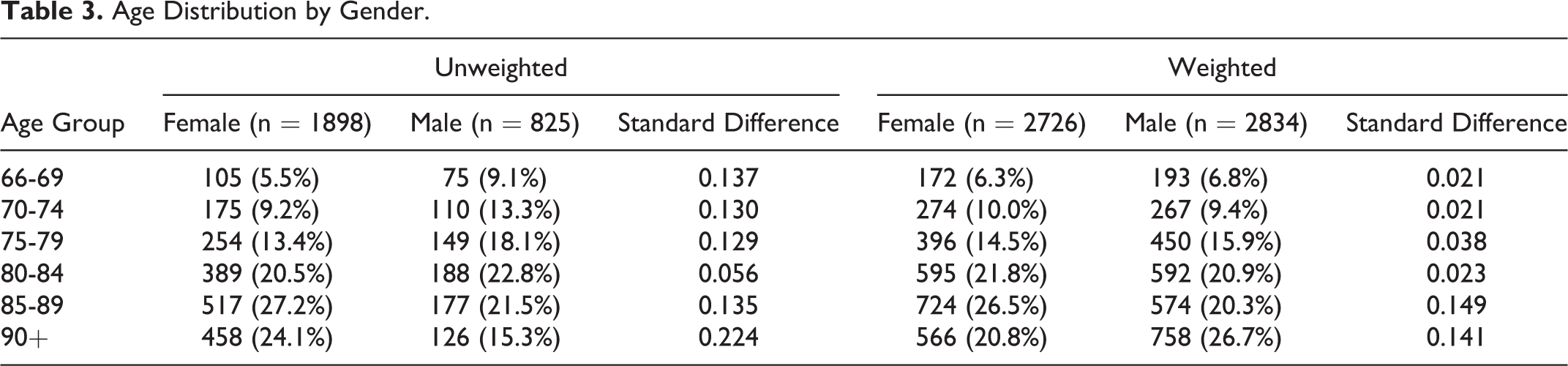
There were 1898 females and 825 males that met inclusion and exclusion criteria for the primary outcome (cumulative incidence of surgery). Surgical case code distributions are reported in Table 2. Crude and weighted covariates are presented in Table 1. The groups were well balanced except for baseline hospital days, skilled nursing facility stays, and durable medical equipment claims; females were generally healthier at baseline. Males also had slightly higher Charlson comorbidity index (CCI) at baseline. Crude and weighted age distributions are shown in Table 3. There were 1592 females and 672 males with 1-year follow-up available for the mortality analysis. Both CCI and the frailty score were well balanced between males and females in the weighted nonsurgical group, but CCI remained higher in males within the weighted surgical group.
Distribution of Surgical Treatment Codes.
Age Distribution by Gender.
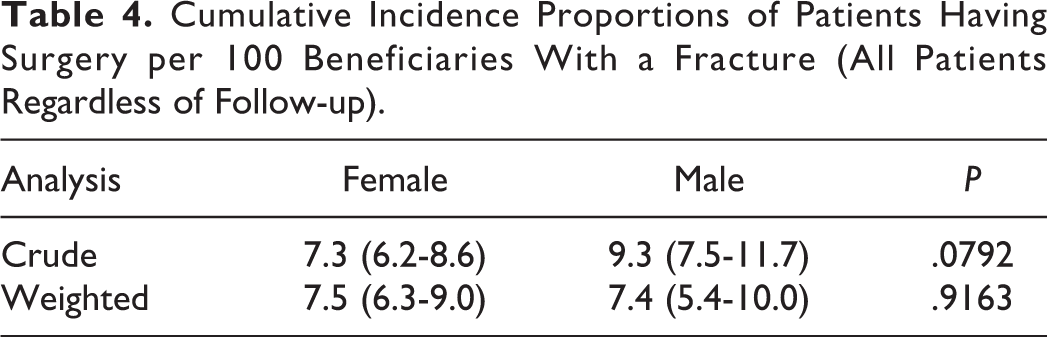
For our primary outcome, the crude and propensity weighted cumulative incidence of surgery by gender is shown in Table 4. Females had a slightly lower unweighted incidence of surgery (7.3 per 100 with a fracture) than males (9.3), but this difference was not significant after weighting. For our secondary outcome, the 1-year propensity weighted mortality by gender and surgical treatment are presented in Table 5 Males had higher mortality regardless of surgical treatment, even after propensity weighting. The surgical group outcomes were limited by the smaller sample sizes.
Cumulative Incidence Proportions of Patients Having Surgery per 100 Beneficiaries With a Fracture (All Patients Regardless of Follow-up).
One-Year All-Cause Mortality per 100 Beneficiaries With a Fracture.
Discussion
In this study, we used propensity weights to balance covariates between genders to disentangle the effects of gender and covariates, including comorbidity and frailty on the cumulative incidence of surgery and 1-year mortality after acute traumatic axis fractures in older US adults. We found that there was no gender disparity in surgical treatment during the study period. Weighted cumulative incidences of surgical treatment were essentially equal, and thus we conclude that gender did not independently exert an effect on surgical decision making during the years studied. We also show that, as expected, 1-year mortality was higher for males compared with females. As seen in other specialties, we show that clinical impressions are typically a result of crude rather than adjusted values. 11 This would be most evident in a limited dataset, but with our nationally representative data, we were able to show adjusted incidence of surgical treatment was actually equal, and our clinical intuition was partially explained by confounding. So while females may be more susceptible to traumatic injury of the axis (68.7% of our sample), our data supports previous observations that males fare poorer in comparison to females in the setting of axis fractures and trauma overall. 12
There are limitations of the study that must be addressed. The most important limitation of this study is the reliance on the accuracy of coding within the Medicare database and the inability to confirm the diagnoses and treatments. While we attempted to exclude patients with major comorbidities or concurrent injuries, if not captured in the coding then male mortality in particular may be inflated given the proven susceptibility of males to the sequela of trauma. Furthermore, given limitation in ICD-9 coding, odontoid fractures, which are the most common and deadly fracture of the axis, cannot be distinguished from other axis fractures. Nonetheless, almost 90% of axis fractures in older adults are odontoid fractures, and given the biomechanical stability of these fractures as borne out by Müller et al, it is unlikely that these nonodontoid fracture contribute to higher mortality in this age group. 13,14 If, however, odontoid fractures were unbalanced in the groups, this would lower the mortality of the group with lower number of odontoid fractures. Conversely, if our assumption is incorrect and the nonodontoid fractures were more morbid, mortality would increase. Given the lack of granularity in our data we cannot draw meaningful conclusions about fracture morphology, treatment, and gender. We have attempted to be fairly rigid in our inclusion and exclusion criteria, unlike other studies, which is a strength of our methods but does limit our sample size. 15 Finally, surgical decision making includes numerous unmeasurable variables that are not included in this study. There was a relatively high rate of anterior cervical approaches in our study (Table 2). The choice of anterior versus posterior approach likely depends on variables including fracture morphology and surgeon preference, which we cannot account for in this model. We did include key comorbidities that were all adjusted for in our propensity weighted cohort. A population-centered trend in surgical treatment disparities should, however, be detected in this nationwide study with a representative sample of Medicare patients.
For our primary objective, we show equal incidence of surgical treatment. This small subset of patients with axis fractures represents a limited sample because we attempted to identify only isolated acute axis fractures and exclude multiple fractures, chronic fractures, and traumatic brain injury patients. This may limit the generalizability of our results, but it nonetheless describes the most likely scenario encountered in clinical practice. For our secondary objective, we show that males have a higher mortality than females. We found that for every 100 patients with isolated acute axis fractures, 13 more males were dead at 1 year than females. Despite correcting for numerous comorbidities, the higher mortality for males is consistent with previous studies and likely related to higher baseline unmeasurable mortality risk in males. 10,12
Surgeons are oftentimes faced with patients who, despite suffering from a surgically fixable problem, have a low likelihood of successful outcome due to confounding factors that cloud decision making when using clinical intuition reflective of only crude associations. Older adults with isolated acute axis fractures present a clinical decision-making challenge. For almost the last decade, it appears that gender equality has been preserved in this decision-making process, despite males having a significantly higher postoperative mortality than females.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Michael P. Catalino receives investigator-initiated research funding from the North Carolina Spine Society.
Brice A. Kessler, Virginia Pate, and Drew Cutshaw have no conflicts of interest to disclose.
Til Stürmer receives investigator-initiated research funding and support as principal investigator (AG056479) from the National Institute on Aging (NIA), and as co-investigator (R01 CA174453; R01 HL118255), National Institutes of Health (NIH). He also receives salary support as Director of the Comparative Effectiveness Research (CER) Strategic Initiative, NC TraCS Institute, UNC Clinical and Translational Science Award (UL1TR002489), and from the Center for Pharmacoepidemiology (current members: GlaxoSmithKline, UCB BioSciences, Merck, and Takeda) and research support from pharmaceutical companies (Amgen, AstraZeneca) to the Department of Epidemiology, University of North Carolina at Chapel Hill. Dr Stürmer does not accept personal compensation of any kind from any pharmaceutical company. He owns stock in Novartis, Roche, BASF, AstraZeneca, and Novo Nordisk.
Deb A. Bhowmick is an educational consultant for Medtronic, PLC. He receives investigator-initiated research funding from NC TraCS Institute; he has received contracted educational compensation from Medtronic Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The database infrastructure used for this project was funded by the Pharmacoepidemiology Gillings Innovation Lab (PEGIL) for the Population-Based Evaluation of Drug Benefits and Harms in Older US Adults (GIL200811.0010); the Center for Pharmacoepidemiology, Department of Epidemiology, UNC Gillings School of Global Public Health, the CER Strategic Initiative of UNC’s Clinical Translational Science Award (UL1TR001111); the Cecil G. Sheps Center for Health Services Research, UNC, and the UNC School of Medicine.