
Abstract
Study Design
Systematic review.
Objective
Surgery remains the gold standard in management of unstable spinal fractures in patients with spinal ankylosing disorders (SAD), especially in the presence neurodeficit. Certain studies have reported the effectiveness of non-surgical treatment in non-displaced and clinically stable fractures.
Methods
Our systematic review was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was conducted (15th July, 2025) across 4 different databases to identify studies reporting outcomes of conservative treatment of spinal fractures in the context of ankylosed spine. The patients were subclassified as groups A (surgically-unfit) and B (stable fractures) for further analysis.
Results
13 studies (187 patients) were reviewed. The underlying etiology was DISH (diffuse idiopathic spinal hyperostosis) in 86.4%. Overall, cervical, thoracic/thoracolumbar (TL) and lumbar fractures were observed in 14.1%, 72.7% and 13.2%, respectively. There were 66% in group B; and a majority were neurologically intact (ASIA E: 97.3%). Different conservative strategies are described (combination of bed rest, orthosis and regular surveillance). Overall fracture healing was 69.5% (group A–47.1% and group B–91%). The morbidity and mortality in these fractures are high (particularly, group A). Halo-immobilization was associated with high complications (especially in debilitated individuals).
Conclusion
In a selected group of patients with stable fracture patterns, conservative treatment is a viable management option in SAD patients with good healing rates. Based on our analysis of reviewed data, we have put forth criteria for decision-making and protocol for conservative management of these fractures.
Keywords
Introduction
The treatment of spinal fractures in patients with spinal ankylosing disorders (SAD) is challenging owing to diverse reasons. 1 A majority of these patients are relatively old; and suffer from diverse medical comorbidities including osteoporosis. 2 These fractures are typically unstable, considering the altered spinal alignment, biomechanics; and distractive or extension patterns of injury. 3 These injures are inherently predisposed to secondary displacement and delayed neurological deterioration. 4
Surgery (in the form of open fusion vs percutaneous stabilization) has remained the gold standard in these fractures, especially in the presence of unstable (or displaced) fracture morphology, epidural hematoma and neurological deficiency. 5 However, surgery is complex in these scenarios owing to altered or distorted anatomical landmarks, higher bleeding tendencies of the bones; as well as medical comorbidities (cardiac, pulmonary, renal, obesity etc.) or on-going medical therapies (such as anticoagulant medications).2,6 The overall 1-year mortality after such fractures has been reported to be as high as 32% (especially in cervical and thoracic fractures).5,7,8
On the other hand, conservative treatment is rarely recommended as the primary management in AO type B3 fractures in SAD due to high complication risks and inherent instability.9,10 The main indications for non-surgical treatment in SAD include non-displaced or clinically stable fractures, serious polytrauma, high surgical or anesthesia risks (in poly trauma or associated medical illnesses), and patients’ unwillingness to undergo surgery.4,11,12 In a review by Rustagi et al, 2 non-surgical treatment of fractures in SAD was associated with a 50% failure rate, which was attributed to delayed fracture displacement and patients’ intolerance to bracing regimen. There is still substantial ambiguity on the diverse issues concerning the conservative treatment of these rare fracture patterns, such as actual indications of non-surgical treatment, ideal treatment protocol, surveillance regimens, recommendations to consider surgical conversion, associated complications; and mortality rates.1,2,4-6,13-15 The current review was thus planned to comprehensively review the existing literature; and compile the pooled data of all the conservatively treated spinal fractures in patients with SAD. To our knowledge, there is no similar review article, hitherto published on this subject.
Methodology
Search Strategy
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was conducted across PubMed, Embase, Scopus, and Web of Science databases to identify studies reporting outcomes of conservative management of spinal fractures in the context of ankylosed spinal disorders. The search was structured using a combination of Medical Subject Headings (MeSH) and free-text terms. The following keywords and Boolean combinations were used: “conservative management”, “non-operative treatment”, “hyperextension injury”, “spine”, “trauma”, “AO type B3”, “extension-type fractures”, “ankylosing spondylitis”, “DISH”, “spinal ankylosing disorders.” No language or date restrictions were applied to maximize inclusivity. The final search was conducted on 15th July 2025, and results were screened independently by two reviewers. Discrepancies during screening were resolved through consensus.
Study Selection
Eligible studies included prospective cohorts, retrospective cohorts, case series, case reports, and multicenter reviews that reported clinical and/or radiological outcomes of non-operative treatment for AO type B3 hyperextension injuries in patients with spinal ankylosing disorders such as ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis. Studies, which focused exclusively on surgical interventions or did not report any outcome measures for conservatively-managed cohorts, were excluded. Studies published in languages other than English were excluded.
Quality Appraisal
The methodological quality of each included study was independently assessed by two reviewers using the Newcastle–Ottawa Scale (NOS), 16 which evaluates non-randomized studies across three domains: selection of study groups (maximum 4 stars), comparability of groups (maximum 2 stars), and ascertainment of the outcome of interest (maximum 3 stars). For case reports and very small series, only applicable domains were scored, with non-applicable domains marked accordingly. Discrepancies in scoring were resolved through discussion or, when necessary, consultation with a third reviewer. The total NOS score for each study was calculated by summing the domain scores, with higher scores indicating better methodological quality.
Data Extraction and Synthesis
From the included studies, the following data were extracted. • Demographics (age, sex, comorbidities, fracture location) • Radiological features (fracture pattern, stability indicators) • Conservative modalities used (type of brace, duration, adjuncts like teriparatide) • Clinical outcomes (neurological status, functional recovery, union rates, complications, mortality)
Data extraction was done independently by two reviewers. Discrepancies were resolved through consensus.
Data Analysis
Due to significant heterogeneity in patient profiles, fracture morphologies, and outcome metrics, a qualitative synthesis was performed. No meta-analysis was conducted. The extracted data were tabulated to compare patterns and highlight trends in conservative management strategies across different spinal regions and SAD subtypes. Particular attention was paid to predictors of treatment success or failure, radiological indicators of stability, and mortality implications. The patients were also subclassified as groups A (conservative management in view of high surgical or anesthetic risk, polytrauma, poor general condition) and B (conservative management based on stable fracture morphology). A treatment algorithm was planned based on the results analyzed from the literature; and criteria were proposed for case-to-case decision making as well as determination of factors favoring either conservative or surgical treatment.
Results
Conservative Treatment of AO Type B3 Fractures – Reviewed Studies
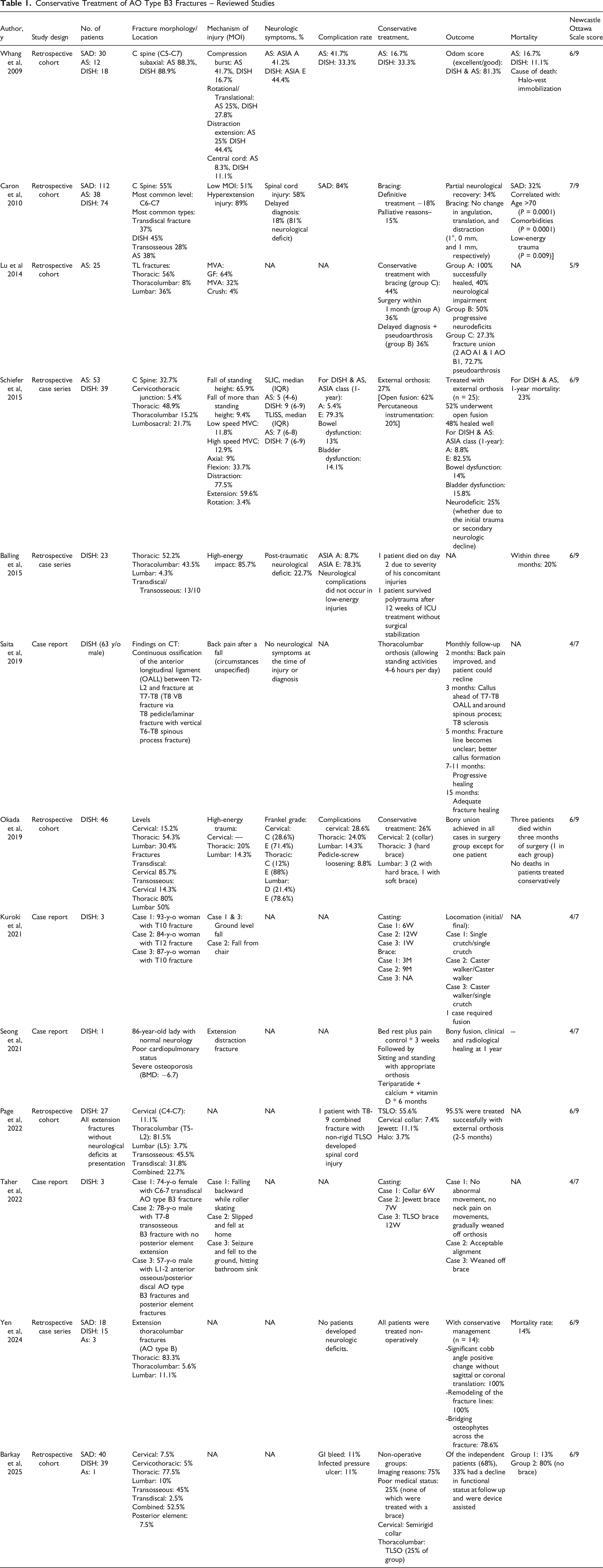
Conservatively-Treated Cohort of Spinal Fractures in Ankylosed Spine
Details of Spinal Fractures in SAD Patients Treated Conservatively
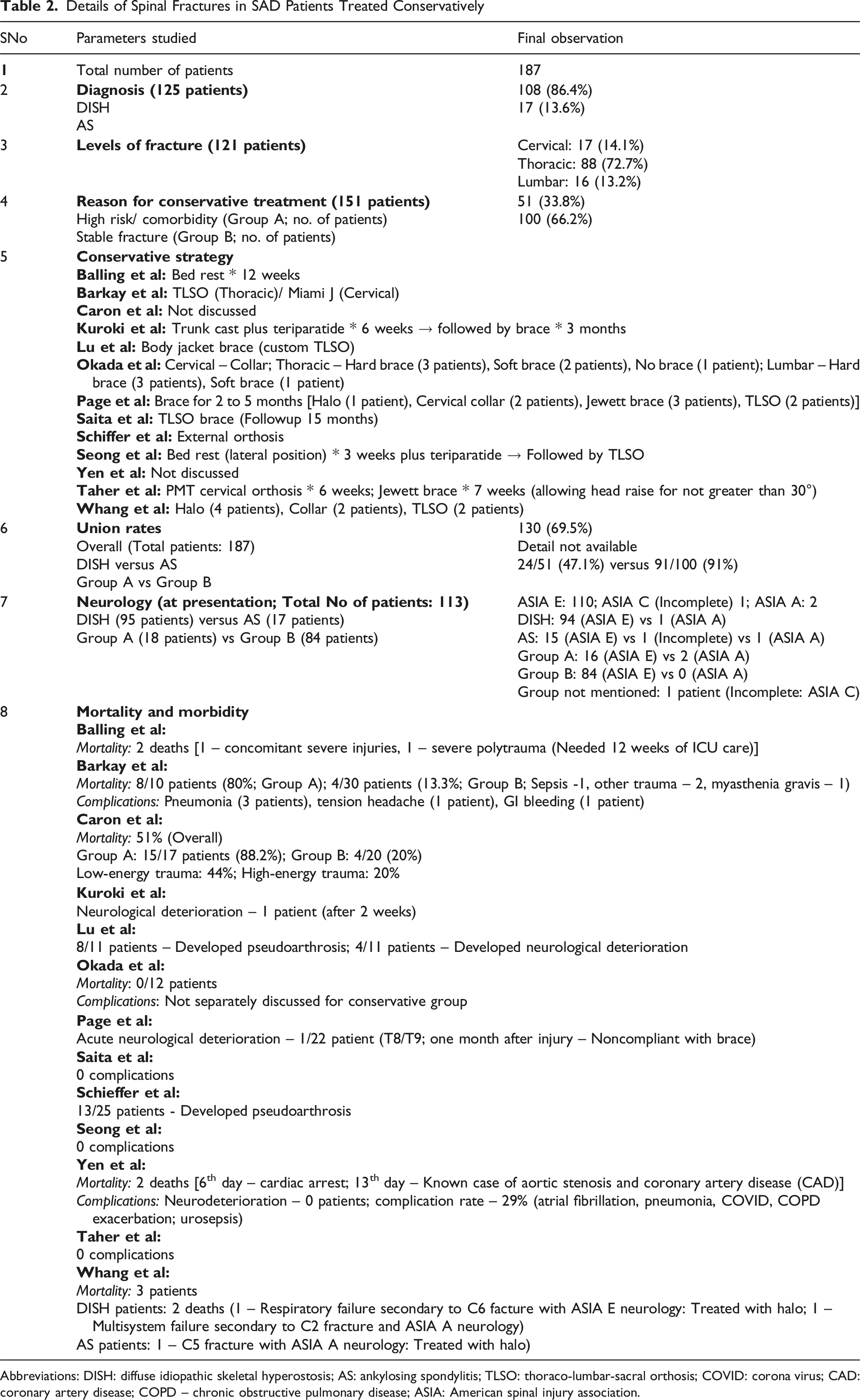
Abbreviations: DISH: diffuse idiopathic skeletal hyperostosis; AS: ankylosing spondylitis; TLSO: thoraco-lumbar-sacral orthosis; COVID: corona virus; CAD: coronary artery disease; COPD – chronic obstructive pulmonary disease; ASIA: American spinal injury association.
We could observe that, in contrast to the general opinion that conservative treatment of these potentially unstable injuries is only considered in patients who are unfit for surgery, the decision to pursue non-operative treatment in 66% of the reviewed patients was primarily made on the presumption of a stable fracture morphology.17,24,25 As one would anticipate, a majority of these conservatively-managed patents had no major neurological deficit (ASIA E) following the injury.17,24,26,27 Based on our review, there was no clear description in the included studies on whether MRI scan (or any particular MR sequences) played a significant role in their decision-making (although a majority of the included studies reported obtaining advanced, cross-sectional imaging in the form of CT and MRI in all the patients).
Strategies for Conservative Treatment
Diverse strategies were employed for conservatively treating these fractures, ranging from bedrest without any external orthosis to extensive truncal cast application12-14,17-19,21-27 (Table 2). We could observe that a general strategy was to include an initial period of bed rest (some studies described lateral position owing to the inherent global kyphosis in these patients which can predispose to translation in supine positions) until pain improves, followed by gradual mobilization with some form of external orthosis for a variable period of 6 to 12 weeks (or longer depending on the progression of fracture healing). The Halo application was associated with high complication rates across studies (especially in more debilitated individuals).17,22,24,27
Union Rates
Based on our review, the overall fracture healing rate following conservative management (187 patients) was 69.5%. The exact time to union was not consistently described in the reviewed studies. While the healing rate was only 47.1% in group A, the fractures in group B had a high union rate of 91%. Based on the available data, we could not clearly observe if the union rates varied among the different ankylosing disorders (ie, DISH vs AS).8,17,19,21,22
Morbidity and Mortality
A wide variety of complications (low- and high-morbidity events) have been described during the course of treatment in these patients. Among the adverse events directly attributable to the external orthosis, halo immobilization has been associated with the highest complication rates (such as pin-tract associated events, respiratory difficulties, aspiration pneumonia, infection, poor tolerance, etc.).14,17-19,22-24 Pseudoarthrosis and neurological deterioration are the two most serious complications impacting the overall outcome. Overall, there was a significantly higher complication rate in group A, in comparison with group B (although we could not perform any analysis based on the available data). The studies by Lu et al 22 and Schieffer et al 24 demonstrated significantly higher pseudoarthrosis and neurological complication rates, as compared to the other studies (especially the retrospective series by Barkay et al, 17 Page et al 18 and Yen et al 14 ). Neither of these studies clearly defined the criteria for fracture stability or the rationale underlying the choice of conservative management in their cohort.
Discussion
Non-surgical treatment of spinal fractures in SAD has been associated with diverse complications and risks.2,17,18,22-24 Bed rest in patients with AS and DISH enhances the chances of pulmonary adversities, decubitus ulcers and deep venous thrombosis (DVT).2,28 Cervical traction, if not prudently employed, can lead to uncontrolled translation of the fractured spinal column and consequent neurological complications.2,29 Halo-vest appliances in SAD patients with cervical injuries may be poorly tolerated, owing to their elderly age, cervicothoracic kyphosis, pulmonary complications (due to chest wall immobilization and high aspiration risk), and pressure sores. In addition, any conservative treatment can result in diverse complications, including loss of alignment, loss of fracture reduction, non-union or pseudoarthrosis (Andersson lesion) and neuro-deficit.2,29,30 Previous studies have also highlighted the inherent selection bias in conducting studies 30 that compare the outcomes between surgical and non-surgical treatments in SAD,2,8,17 since the more severe fracture patterns directly necessitate more aggressive management. In this context, the current study was planned to clearly define the role of conservative treatment in these challenging fractures.
Pathological Diagnosis in SAD
In 1950, Forestier and RotesQuerol described the peculiar radiological characteristics of bony ongrowths and hyperostosis in the thoracic spine (mainly), with occasional extension of these osseous formations across the entire spinal column bridging the intervening intervertebral discs.31,32 These osseous structures typically arise anterolateral to the vertebral bodies and spread cranially in a candle-flame manner. Although initially described as senile ankylosing hyperostosis, the condition was also increasingly observed in younger individuals. 12 In addition to the well-described involvement of the axial skeleton, multiple extra-skeletal manifestations of the disease such as calcifications or ossifications of ligaments and tendon insertions (enthesopathy) were identified. The term “diffuse idiopathic skeletal hyperostosis (DISH) was thus coined to define this condition.33,34
Unlike AS, apart from spinal stiffness, the clinical symptoms are typically minimal in DISH. 12 In the study by Balling et al, 12 DISH was defined by the radiological criteria put forth by Resnick and Niwayama 34 : a. Flowing calcification and ossification anterolaterally involving ≥4 contiguous vertebrae with or without spondylophytes, b. Absence of degenerative disc disease, with reasonably preserved intervertebral disc height, c. Absence of facetal joint ankylosis; and absence of erosion/sclerosis/fusion of the sacroiliac (SI) joints. AS is typically diagnosed by Modified New York criteria, 35 although none of the reviewed studies had specifically defined any criteria for inclusion in their studies.
Characteristics of SAD Fractures
Fractures in SAD are inherently complicated and challenging due to a variety of reasons. In the study by Caron et al, 19 among the 122 spine fractures (112 consecutive patients), a majority involved the C6-C7 level, 89% were secondary to hyperextension injuries, and 37% were transdiscal in morphology. These fractures were complicated by relatively poor patient health (at least one comorbidity in 81%), high neurological injuries (58%); and a significantly higher prevalence of delayed diagnosis (18%). In a recent study, 23 transdiscal fractures in DISH patients were more commonly encountered in cervical injuries, while delayed diagnosis, transosseous fractures and posterior column ankylosis were commonly observed in thoracolumbar (TL) fractures.
Surgical Management of SAD Fractures and the Challenges Encountered
In general, surgery has been associated with good outcomes in these fractures, especially in patients with neurological involvement.2,8 In the study by Lu et al, 22 9 [out of 25 patients – 4 (44.3%) and 5 (31.3%) presented with high-energy and low-energy trauma, respectively] presented with neurological deficit; among whom, 4 (44.3%) improved after surgery. In the study by Okada et al, 23 following surgery, there was an improvement in the neurological status in 35.3% of patients, while the neurological status deteriorated in 5.9%.
However, surgery in these patients is fraught with multiple complications and adversities. In the study by Caron et al, 19 84% of surgically-treated patients developed at least one complication. The overall mortality following fractures in ankylosed spine was 32%, and correlated with elderly age (>70 years), associated comorbidity, and low-energy mechanism of injury (MOI). In the study by Schiefer et al, 24 following surgical intervention, the overall complication risk, neurological deterioration, and 1-year mortality rate were reported as 7.6%, 8.6% and 23%, respectively.
In another study by Lu et al, 22 the overall complication rate following surgical intervention in SAD fractures was 40.9%. Although all fractures healed after surgery, multiple complications including respiratory failure, empyema, deep retroperitoneal wound infection, chronic osteomyelitis, implant failure and surgical site infection, were observed. In the study by Balling et al 12 [involving 21 surgically-managed hyperextension injuries (HEI) in SAD], there was a high association with concomitant extraspinal injuries (including polytrauma in 71.4%) and neurological complications (22.7%). The overall mean duration of hospital stay was 35 ± 29 days, and the 3-month mortality rate was 20% (mean age of the deceased cohort was 80.7 ± 5.1 years). Thus, surgical management of these fractures is highly challenging, with reasonably high morbidity and mortality rates.
Role of MRI in SAD Fractures
In a retrospective study by Tavolaro et al, 36 MRI could identify major spinal injuries in 3.2% of patients with SAD, in addition to those diagnosed using CT alone. Such additional findings were demonstrated to substantially modify the original treatment plan. Among these injuries, one was a fracture (bony disruption) which was initially missed on CT. All the remaining injuries, specifically picked up MRI, were disco-ligamentous injuries through non-ossified or mobile disc spaces or intraspinal pathologies (eg, hematoma). In this context, they recommended that the routine use of MRI could be limited to patients with non-ankylosed, intervening spinal levels. These levels are typically predisposed to major disco-ligamentous injuries. In addition, MRI can be helpful in patients with neurological deficits, in order to rule out intraspinal compressive pathologies.
Which Fractures in SAD are Best Managed Conservatively? – Our Recommendations
A majority of our recommendations regarding fractures in ankylosed spine are based on 3 retrospective studies (by Barkay et al 17 Page et al 18 and Yen et al 14 ). Schiefer et al 24 showed that 84.4% of spinal fractures in ankylosed spines were three-column injuries. However, not all the levels were completely fused; and fractures involving the intervening non-ankylosed or minimally-ankylosed levels might not involve all the 3 columns (which can be relatively more stable).
A majority of fractures in these kyphosed, fused spines are secondary to a hyperextension mechanism. In the study by Schiefer et al, 24 the diverse possible injury mechanisms in SAD fractures were discussed: distraction (77.5%), extension (59%) and flexion (34%) forces. Certain other studies have demonstrated that a small proportion of fractures (especially at levels with incomplete ankylosis) in these patients can be secondary to compressive injuries (including burst fractures: AO types A1, A3, A4), flexion-distraction injuries (AO B1, B2).2,8,12,17-19,21-24,29 These fractures are also innately more stable than hyperextension injuries in the fully ankylosed spines.
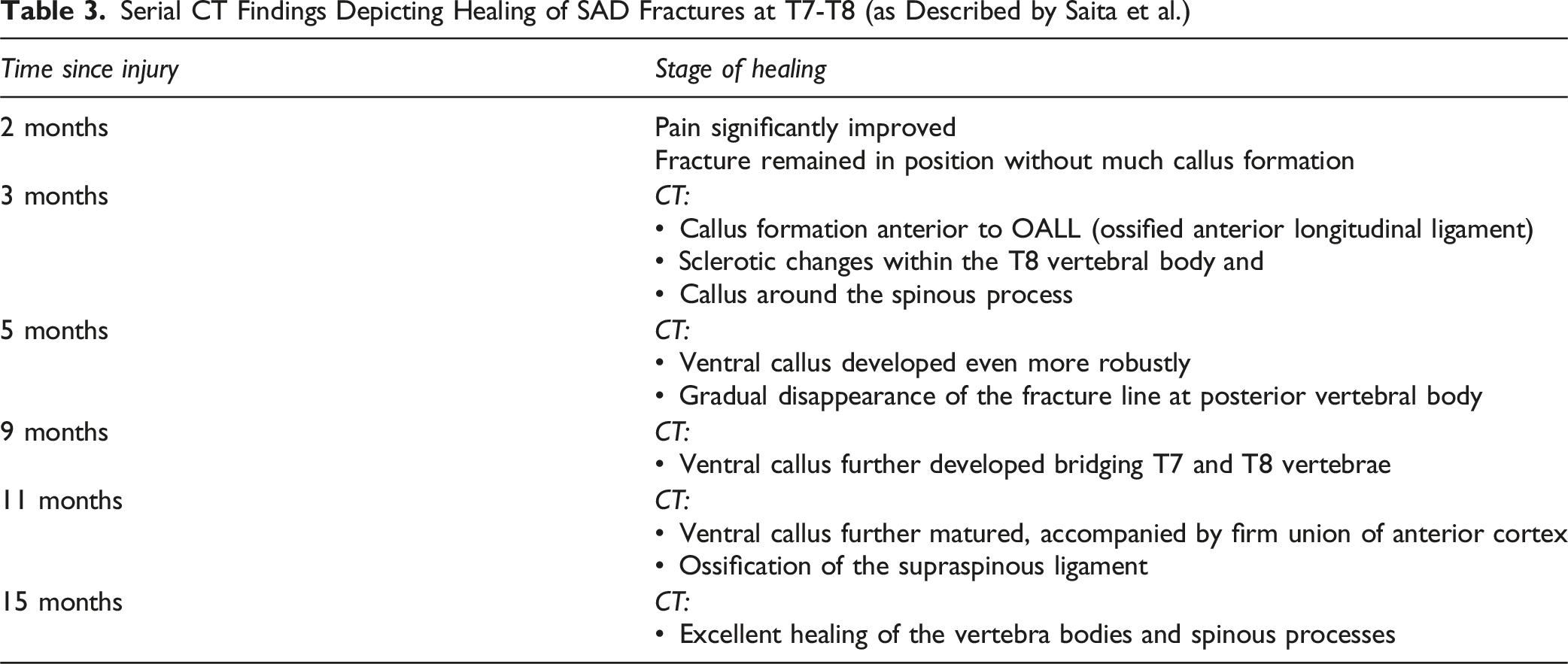
Serial CT Findings Depicting Healing of SAD Fractures at T7-T8 (as Described by Saita et al.)
Rationale Underlying the Decision-Making Criteria
A deeper understanding of the interplay between fracture morphology, biological healing potential and biomechanical stability is essential to explain why some SAD fractures respond favourably to conservative treatment, while others fail. In fully-ankylosed spine, the posterior tension band (PTB), comprising the spinous processes, laminae, interspinous and supraspinous ligaments, as well as posterior paraspinous musculature, acts as a unified structural complex which resists distractive and translational deformations.2,19,24 When this complex remains intact, extension-type AO B3 fractures tend to behave as “hinge-extension injuries”, in which the posterior elements act as a stable pivot point. This configuration mitigates the shear stresses across the anterior cortical gap and promotes compressive loading during upright posture, both of which favour callus formation and osseous bridging.14,18,25 Conversely, fractures with posterior column (PC) disruption experience unopposed extension forces, greater instability and higher rates of delayed displacement or pseudoarthrosis.22,24
Beyond the role of PTB, several additional biomechanical and biological factors contribute to the divergent healing profiles observed in conservatively-managed SAD fractures. The pattern and completeness of spinal ankylosis exert a major influence on fracture stability. In DISH, where ossification predominantly involves anterior longitudinal ligament (ALL) and produces flowing anterolateral osteophytes; hyperextension injuries often propagate through a long lever arm, yet maintain broad osseous contact surfaces, which may facilitate bony bridging once external support is provided.12,34 In contrast, AS is characterized by symmetric ligamentous ossification, facet ankylosis and progressive osteoporosis, resulting in stiffer yet more brittle spinal segments which may fail through narrower planes. Such fractures are more susceptible to displacement, pseudoarthrosis and delayed instability. In addition, AS patients often exhibit systemic inflammation, and heightened risk of epidural pathology.2,19,30 Fracture morphology also plays a critical role: while trans-osseous fractures afford greater intrinsic stability and larger biological surface area for fracture union; trans-discal and mixed osseous-discal injuries rely on the limited healing ability of the fibrocartilaginous tissues and therefore demonstrate less predictable healing behaviour.14,18,19 In addition, elderly patients with multimorbidity frequently have compromised bone density and micro-vascularity, which may further decrease their healing potential and enhancing the risk of non-union or progressive deformity.2,12,30 These biomechanical and biological considerations help in explaining why conservative treatment tends to succeed primarily in younger, healthier patients with stable, trans-osseous and incompletely ankylosed injury patterns; while fractures occurring in globally ankylosed, osteoporotic spines or those that traverse disc spaces are at markedly enhanced risk of treatment failure.2,19,22,24
Advanced Imaging in Decision Making
Criteria for Conservative Management in SAD Fractures
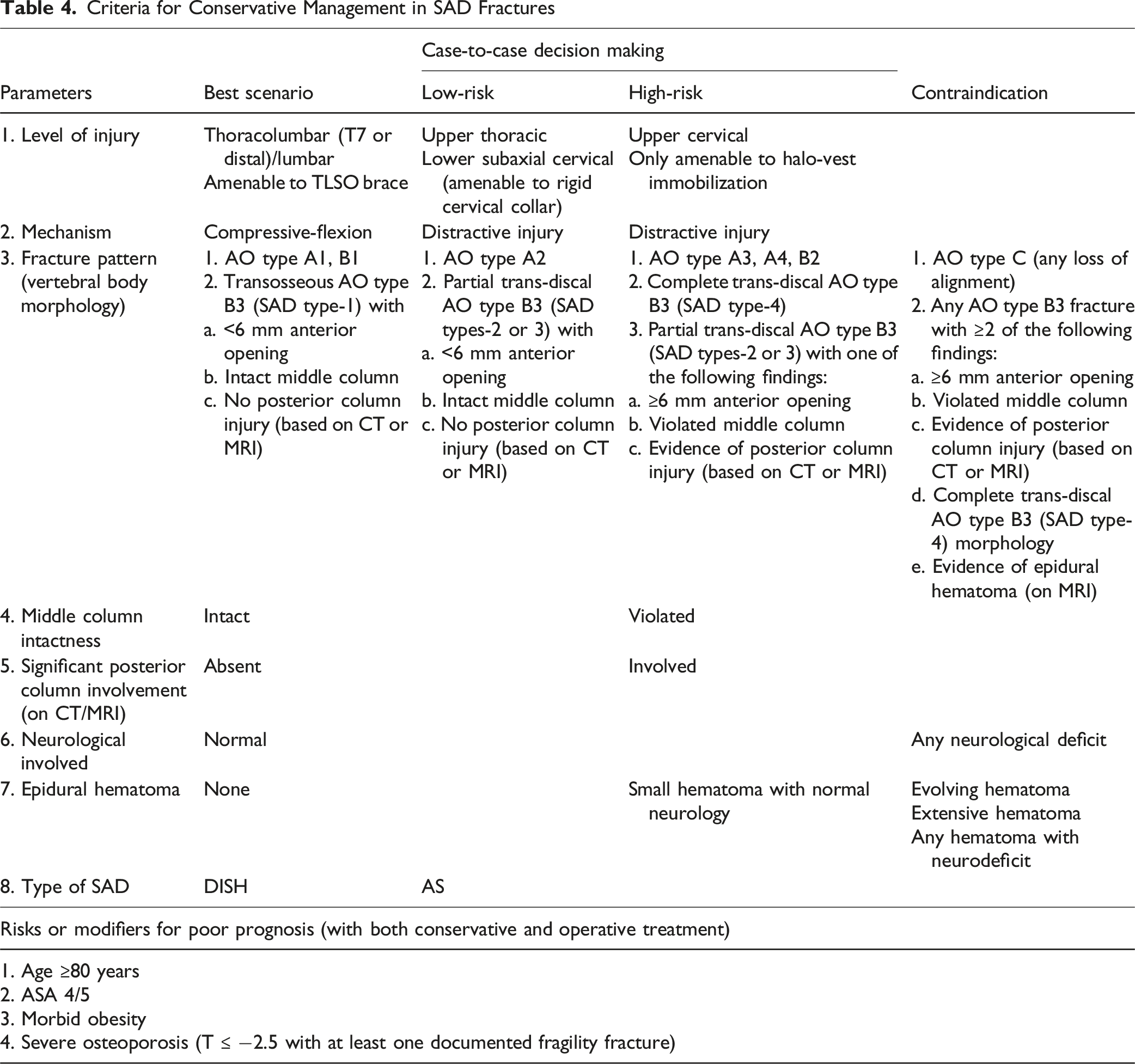
Criteria for Conservative Management in SAD Fractures
Based on the review, we have postulated a set of criteria to define stability in these fractures (Table 4): a. Level of injury (cervical – more unstable than thoracic/TL), b. Mechanism of injury (distractive -more unstable than compressive forces), c. Fracture pattern (AO type B3 injury, in a majority of cases), d. Intactness of the middle column, e. Posterior column [or posterior tension band (PTB)] intactness, f. Presence of neurological involvement, g. Presence of epidural hematoma on MRI; and h. Underlying pathology (DISH vs AS). Any displacement (AO type C) is a contraindication to conservative treatment. AS has been associated with greater systemic comorbidities, cervical level of injury and relatively higher complication rates (and therefore, was given a slightly more guarded prognosis). Although compromised general health (old age, higher comorbid illness, morbid obesity and severe osteoporosis) is associated with poor outcome following both conservative and surgical interventions, these parameters are not contraindications to any form of treatment.
In AO type B3 fractures, some of the radiological findings are associated with better outcomes following conservative treatment: a. Anterior opening less than 6 mm, b. Intact middle and posterior columns, and c. Complete trans-osseous (better than partial trans-osseous and trans-discal) fracture morphology.
Our Recommendations Regarding Strategy for Conservative Treatment of Spinal Fractures in SAD
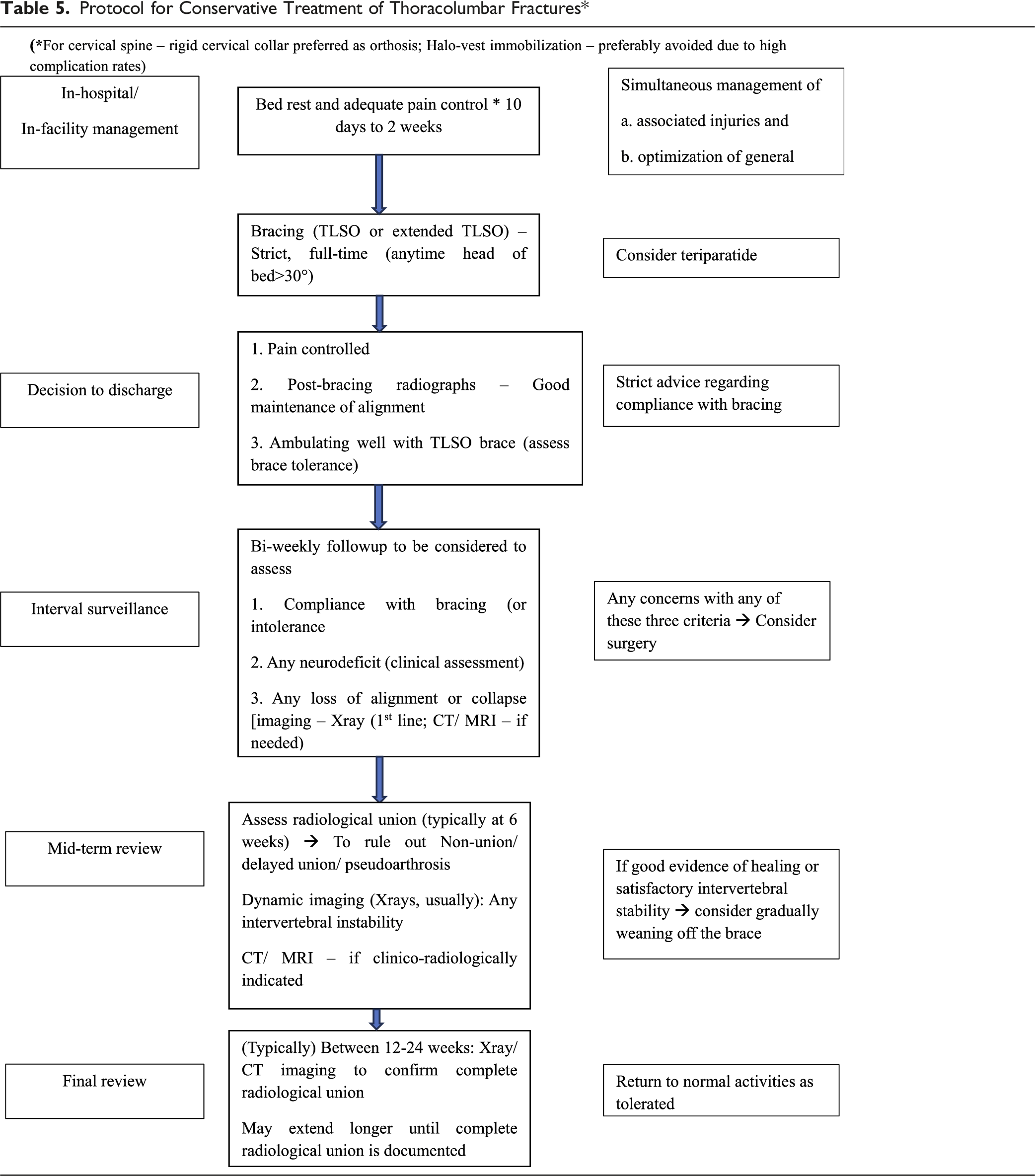
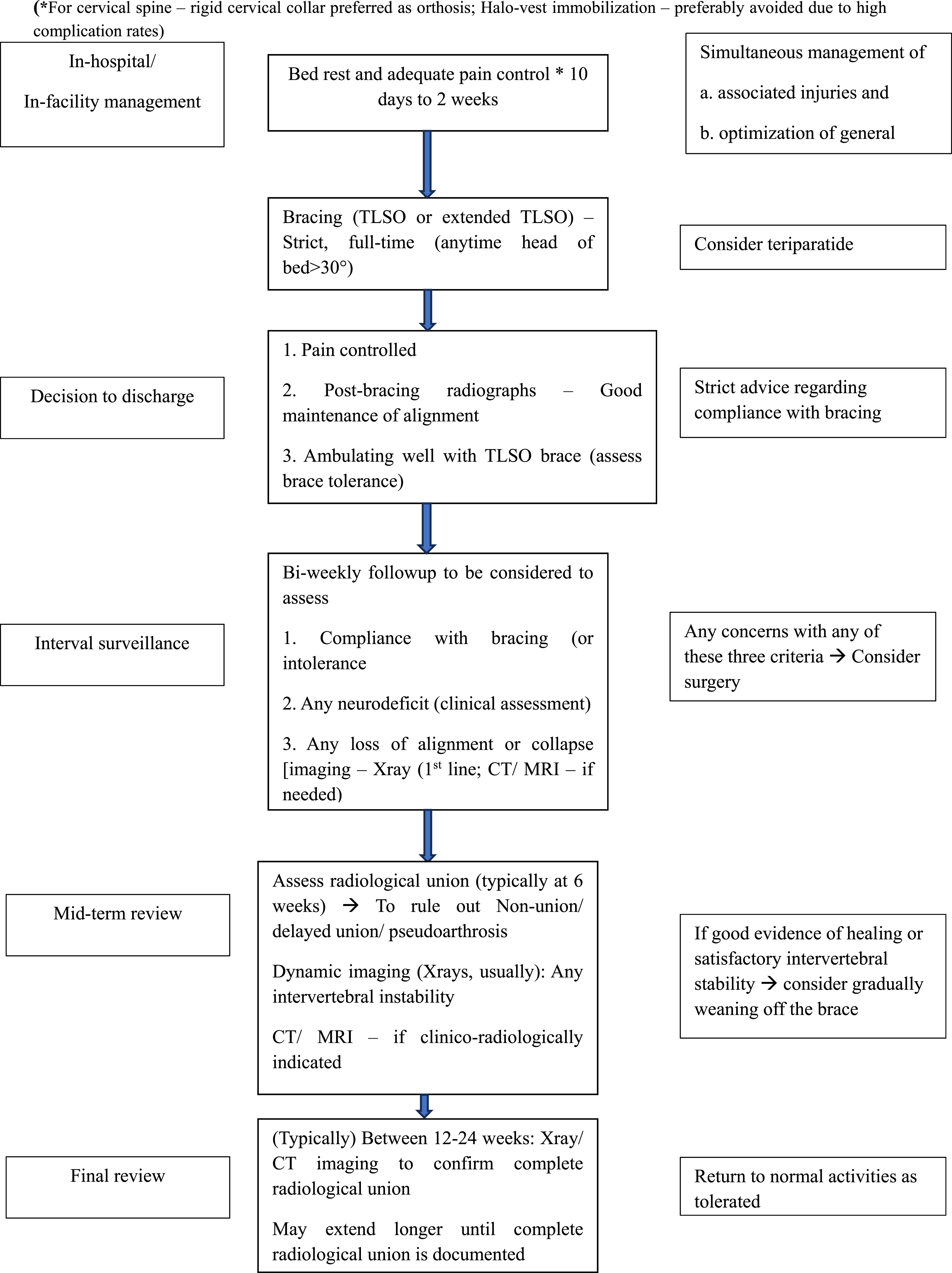
Protocol for Conservative Treatment of Thoracolumbar Fractures*
Limitations
Although the present review proposes preliminary criteria and a treatment algorithm for selecting patients with SAD fractures, who may be suitable for conservative management; these recommendations must be interpreted within the context of significant evidence limitations. The available literature is composed predominantly of case reports and small retrospective series, with only three studies providing moderate-quality cohort data. While these cohorts consistently demonstrate high union rates, most notably a 91% healing rate among patients with radiographically stable fractures; the absence of prospective designs, control groups, standardized imaging protocols, and uniform fracture classification substantially limits the generalizability of the findings. There is paucity of long-term functional outcome data [including limited availability of validated quality-of-life (QoL) metrics, patient-reported outcome measures (PROM), gait or mobility outcome] in the included studies. As such, the proposed criteria and treatment protocol are intended as a pragmatic, experience-based framework to aid clinical reasoning rather than as validated guidelines. Further multi-center prospective studies with harmonized definitions of stability, standardized imaging criteria, and long-term functional outcome assessment are essential before these recommendations can be adopted universally.
A significant challenge during the review was the marked heterogeneity in fracture classification across the reviewed studies [AO/OTA system vs Caron classification (trans-discal or trans-osseous) vs Scheifer/SAD morphology-based categorization]. These systems are nit interchangeable and many studies provided incomplete or ambiguous descriptions of fracture patterns, making uniform reclassification impossible. Future studies must prioritize the use of a standardized, reproducible classification criteria to enable meaningful comparative analysis and enhance the quality of evidence in this complex patient population (Figure 1). PRISMA flow diagram of inclusion of studies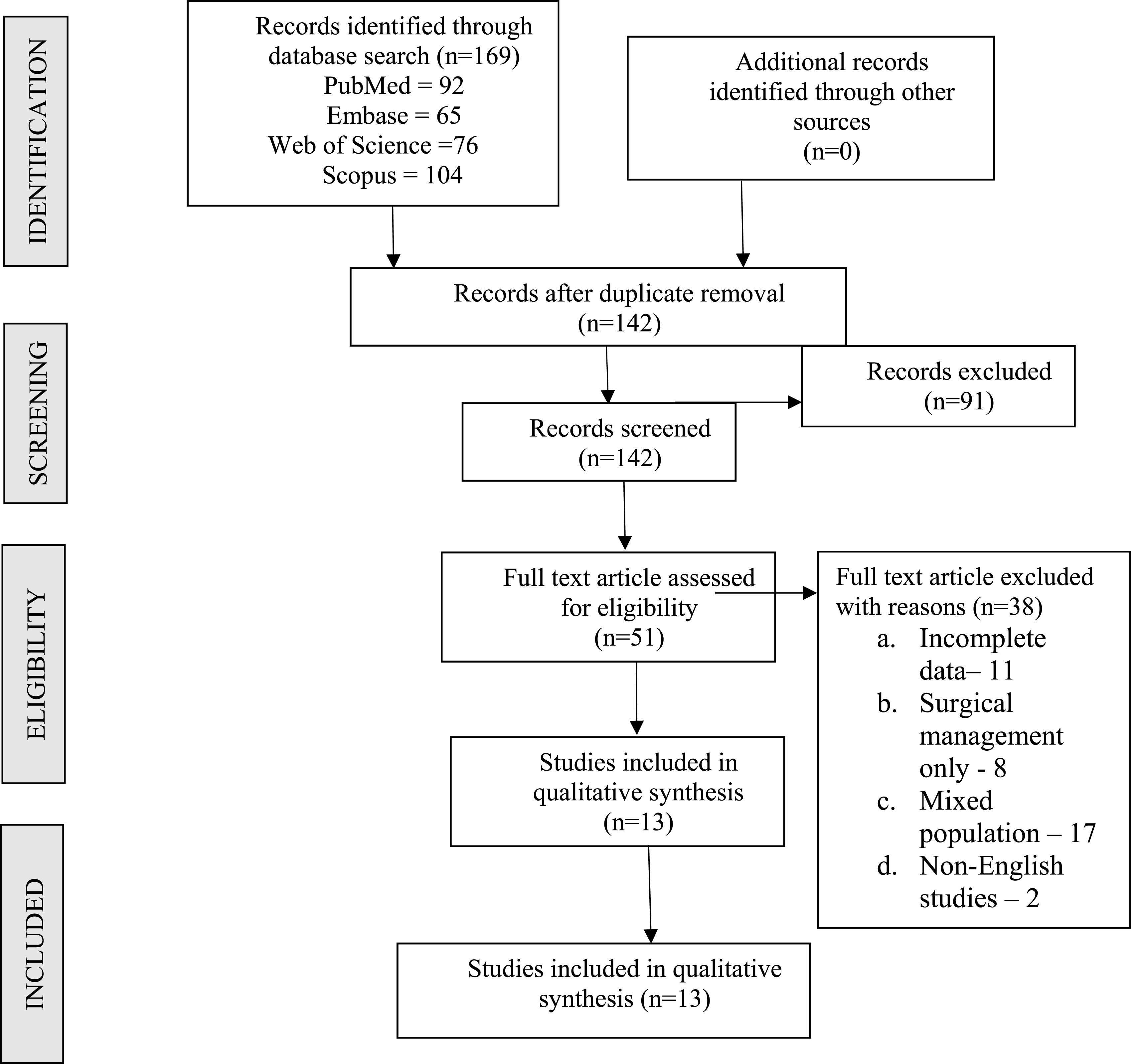
Conclusion
Conservative treatment is a viable option for the management of stable spinal fractures in patients with SAD. The fracture healing with external orthosis is good in such stable injury patterns (especially in young patients with good general condition). The complication rates (and even mortality) are significantly higher in patients with poor general condition, although healthier patients fare much better. Based on our analysis of the reviewed data, we have put forth criteria for decision-making and protocol for conservative management of these fractures.
Footnotes
Author Contributions
VK - Conceptualization, literature search, manuscript writing and editing. HT, ES - manuscript writing and editing. SM - Conceptualization, literature search, manuscript writing. LH, ST, SRRM - Literature search, manuscript writing, references, editing and supervision. All have approved the final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LH reports a relationship with Eminent Spine that includes: consulting or advisory. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.