
Abstract
Study Design
Retrospective Cohort Study.
Objectives
To evaluate the prognostic utility of preoperative laboratory values (PLVs) in predicting 30-day postoperative outcomes among patients undergoing single-level vertebral fracture fixation.
Methods
The ACS-NSQIP database (2015-2020) was queried to identify adults who underwent single-level vertebral fracture fusion. Patients were stratified by PLV categories using clinically relevant hypo- and hyper-thresholds. Outcomes included 30-day mortality, major complications, Clavien-Dindo IV complications, non-home discharge (NHD), readmission, reoperation, and extended length of stay. Multivariate logistic regression adjusted for demographics and comorbidities was used to assess associations between PLVs and adverse outcomes.
Results
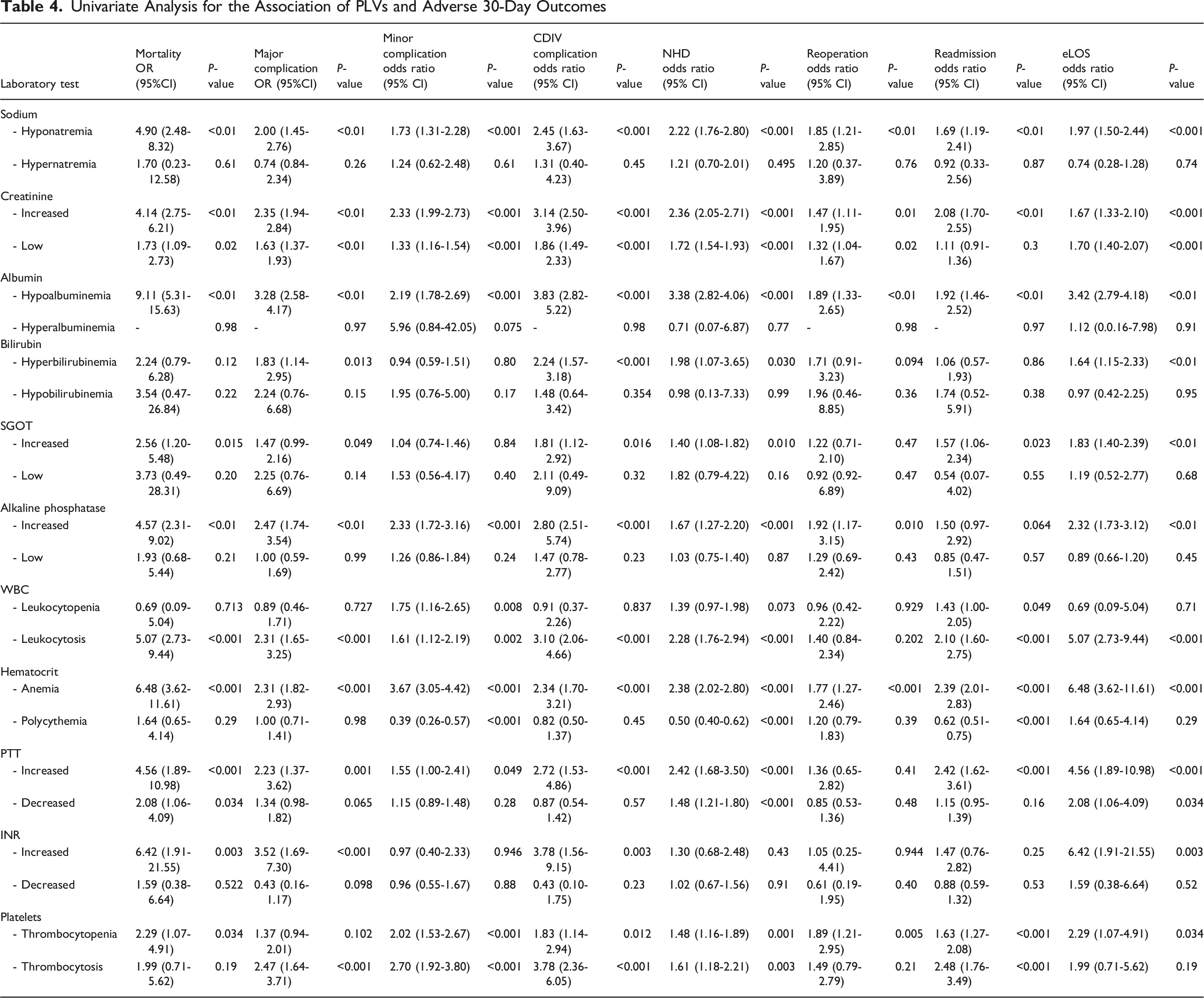
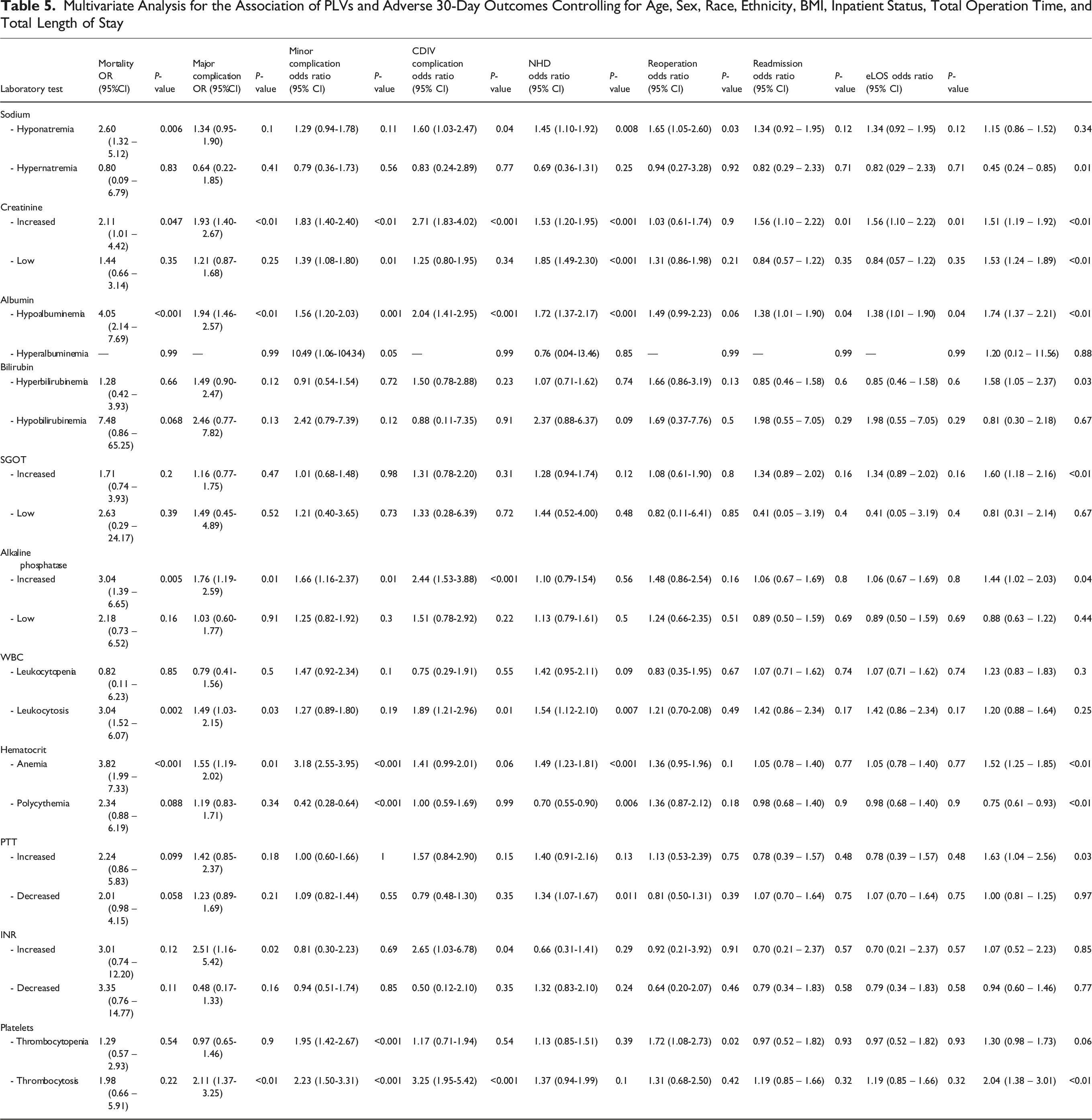
A total of 4005 patients were identified. Hypoalbuminemia emerged as the strongest independent predictor of poor outcomes, including mortality (OR 4.05, 95% CI 2.14-7.69, P < 0.001), major complications (OR 1.94, 95% CI 1.46-2.57, P < 0.01), and NHD (OR 1.72, 95% CI 1.37-2.17, P < 0.001). Elevated creatinine and leukocytosis were significantly associated with increased mortality (P = 0.047) and Clavien-Dindo IV complications (P < 0.001), while preoperative anemia predicted prolonged hospitalization (P < 0.01).
Conclusions
Among patients undergoing single-level vertebral fixation for fracture, hypoalbuminemia is the most consistent predictor of adverse 30-day outcomes. Elevated creatinine, leukocytosis, and anemia also confer independent risks for specific complications. Incorporating PLVs into preoperative risk stratification may enhance patient counseling, optimize perioperative planning, and identify candidates for targeted prehabilitation.
Keywords
Introduction
In the United States, vertebral fractures affect approximately 1.5 million individuals annually, with traumatic injuries, osteoporosis, infection, and neoplasms as underlying etiology behind the majority of cases. 1 Among these, single-level fractures represent a significant subset often resulting in prolonged pain, disability, and diminished quality of life. 2 While nonoperative management, including bracing, analgesia, and activity modification, is preferred for stable fractures, definitive surgical fixation is frequently required for unstable fractures or cases with neurologic compromise.3,4 Although surgery is often pursued to minimize instability and protect vulnerable patients, the risks associated with surgical intervention can be significant. Postoperative complications, such as infection, hardware failure, and delayed neurologic recovery, contribute to morbidity, extended hospital stays, and increased healthcare expenditures.2,5-7 Given the complexities of managing these injuries, the decision between operative and non-operative treatment remains nuanced and patient-specific with a holistic informed consent process undertaken between patient and physician. A comprehensive preoperative risk stratification framework inclusive of PLV in conjunction with anatomic imaging modalities and physical examination may assist surgeons in identifying which patients are more likely to derive benefit from surgery vs conservative management, ultimately guiding treatment plans and aligning expectations.
Existing studies have identified demographic and clinical factors such as age, frailty, bone mineral density, and medical comorbidities as independent predictors of adverse outcomes following spine fracture surgery.8-10 However, the role of preoperative laboratory values (PLVs) in predicting outcomes remains underexplored. Preliminary research suggests that markers of nutritional status, inflammation, and coagulation may correlate with surgical complications and recovery trajectories, but these findings have been limited to small, single-center cohorts or broader populations outside of spine fracture surgery.11-13 That is to say, to date, no large-scale study has systematically evaluated the predictive utility of PLVs for single-level spine fracture outcomes, creating a paucity in evidence-based risk assessment tools.
This study aims to address this gap by analyzing the association between PLVs and 30-day outcomes in patients undergoing surgical management of single-level vertebral fractures. Using a national surgical database, we seek to identify laboratory-derived biomarkers that enhance preoperative risk stratification and ultimately inform clinical decision-making and improve patient-centered care.
Methods
Study Design
This study analyzed data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database covering the years 2015 to 2020. The ACS-NSQIP is a rigorously validated, multi-center database that records comprehensive preoperative, intraoperative, and postoperative variables across a wide range of surgical specialties. Data are contributed by over 700 participating hospitals and are abstracted by trained clinical reviewers to maintain quality and consistency. 14 All analyses were performed using a HIPAA-compliant Participant Use File. All methods utilized in this study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 15
Patient Selection
Patients included were aged ≥18 years undergoing fusion surgeries for single-level vertebral fracture and were identified using Current Procedural Terminology (CPT) codes 22326-22328 and 22600-22612, encompassing open posterior treatment or reduction of vertebral fractures/dislocations (22326-22328) and posterior or posterolateral spinal fusion at the cervical, thoracic, or lumbar levels (22600,22 610, 22612). Corresponding diagnoses were captured using ICD-10 codes S12.x, S22.x, S32.x, M48.5x, and M84.x as well as ICD-9 codes 805.x and 733.1x. Exclusion criteria included patients with missing lab values, incomplete functional status data, incomplete operative data, and a diagnosis of metastatic spinal neoplasms or an acute spinal cord injury.
Preoperative Lab Values
PLVs were extracted for all patients undergoing surgical management of single-level vertebral fractures. Abnormal values were categorized using expanded thresholds informed by previously published NSQIP-based literature, with additional stratification to capture both low and high deviations from normal reference ranges.16,17 The evaluated parameters included: sodium (hyponatremia <135 mEq/L; hypernatremia >145 mEq/L), creatinine (low <0.65 mg/dL; increased >1.35 mg/dL), albumin (hypoalbuminemia <3.5 g/dL; hyperalbuminemia >5.4 g/dL), total bilirubin (hypobilirubinemia <0.2 mg/dL; hyperbilirubinemia >1.2 mg/dL), SGOT/AST (low <9 U/L; increased >45 U/L), and alkaline phosphatase (low <45 U/L; increased >140 U/L). Additional hematologic markers included white blood cell count (leukocytopenia <4 ×103/mm3; leukocytosis >12 ×103/mm3), hematocrit (anemia <36%; polycythemia >45%), platelet count (thrombocytopenia <150 ×103/μL; thrombocytosis >400 ×103/μL), partial thromboplastin time (PTT) (decreased <25 s; increased >40 s), and international normalized ratio (INR) (decreased <0.9; increased >1.5).
Outcomes and Variables of Interest
Case variables included demographics (age, sex, race, and ethnicity), preoperative factors (eg, diabetes, hypertension, and smoker status), and postoperative outcomes (eg, pneumonia, unplanned intubation, and cardiac arrest). Major complications were defined as deep surgical site infection (SSI), organ space SSI, wound dehiscence, prolonged ventilation ≥48 hours, pulmonary embolism, cerebrovascular accident, renal failure, myocardial infarction, cardiac arrest, bleeding requiring transfusion, sepsis, septic shock, pneumonia, and unplanned reintubation. Minor complications included intra- or postoperative blood transfusion, renal insufficiency, or urinary tract infection. Extended length of stay (eLOS) was defined as hospitalization exceeding the 75th percentile of the cohort (>7 days). Clavien-Dindo IV (CDIV) complications refer to life-threatening postoperative events resulting from single or multi-organ failure. These include conditions such as heart failure, respiratory failure requiring intubation, intracranial hemorrhage or ischemic stroke, and renal failure requiring dialysis. Perioperative Acute Condition Score (PACS) was defined as the cumulative burden of acute preoperative illness by summing binary NSQIP “present at time of surgery” indicators for sepsis, systemic inflammatory response syndrome (SIRS), acute renal failure, ventilator dependence, and pneumonia. The Charlson Comorbidity Index (CCI) was calculated for each patient to quantify baseline comorbidity burden, incorporating weighted scores for chronic conditions such as cardiovascular disease, diabetes, malignancy, and organ dysfunction as defined by NSQIP variables. 18 Sensitivity analyses excluding PACS and subgroup analysis to evaluate differences in PLV association with adverse outcomes in elective and non-elective cases were performed to evaluate stability of associations. The NSQIP elective surgery designation was applied when patients presented from home or a non-hospital living situation for a scheduled operation on the day of surgery. Cases were marked non-elective if patients were admitted from the emergency department, another acute care facility, or hospitalized beforehand for optimization or emergent indications. This definition, introduced in 2011, standardizes elective case classification to identify patients well enough to present directly for surgery.
Statistical Analysis
Continuous variables were summarized using medians with interquartile ranges (IQR), while categorical variables were reported as frequencies and percentages. Univariate and multivariate analyses were conducted to evaluate PLVs as predictors of outcomes. Multivariate models were adjusted for relevant covariates, including age, sex, race, ethnicity, BMI, inpatient status, total operation time, elective status, ASA, and CCI. Results from logistic regressions are presented as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). Statistical significance was defined as a two-sided P-value <0.05. All statistical analyses were conducted using RStudio and SPSS version 28 (IBM Corp., Armonk, NY).
Results
Demographic and Clinical Characteristics
Baseline Demographic Variables, Clinical Characteristics, and Postoperative Outcomes of Single-Level Vertebral Fracture Patients
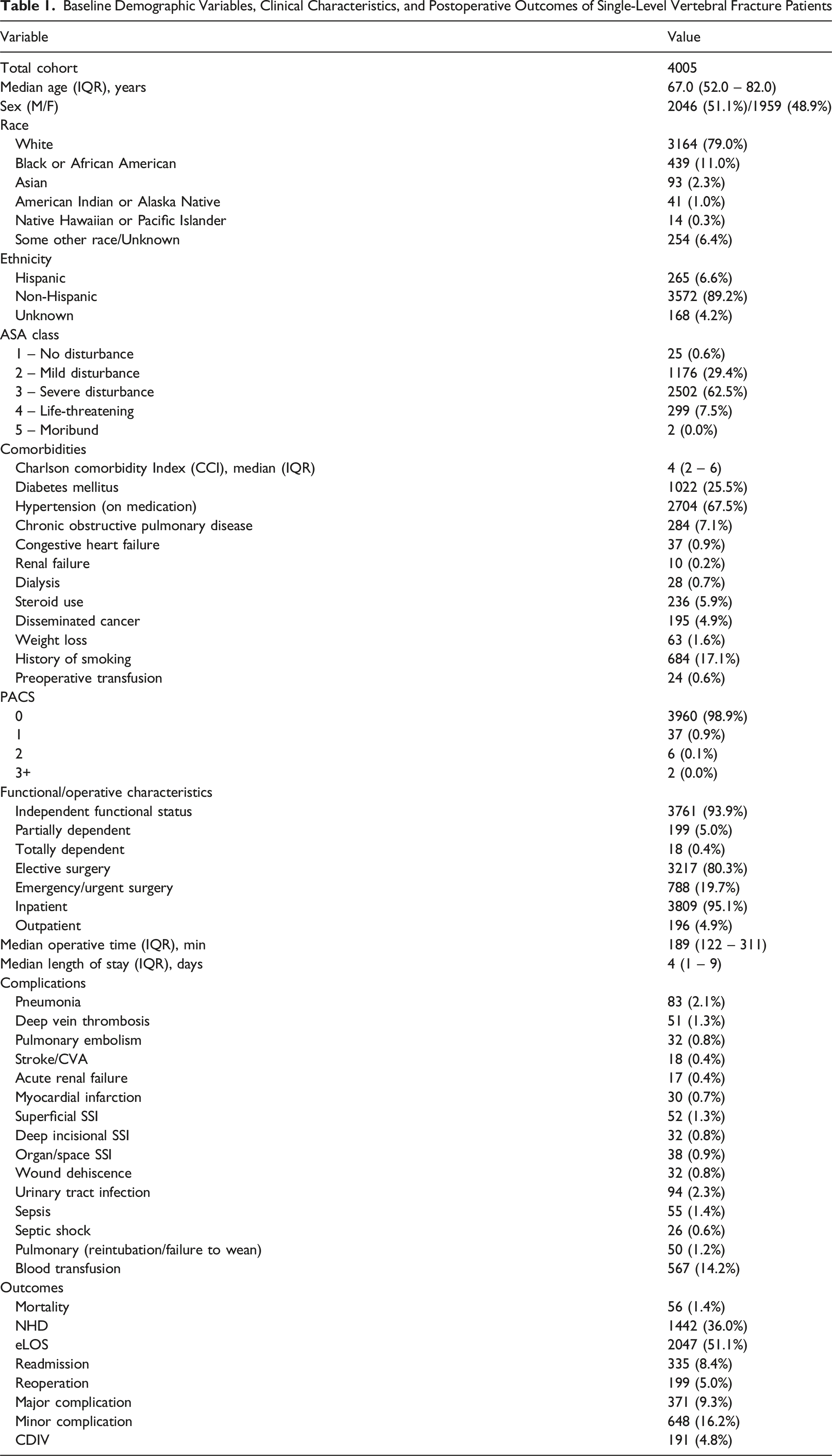
The most common preoperative comorbidities were hypertension (67.5%), diabetes mellitus (25.5%), and a history of smoking (17.1%). The median CCI was 4 (IQR: 2), and ASA Class III or higher was documented in 2803 (70.0%) of patients.
Regarding PACS, the majority of patients had a score of 0 (98.9%), while 0.9% had a score of 1, 0.1% had a score of 2, and <0.1% had a score of 3 or greater.
Major complications were observed in 371 (9.3%), and minor complications in 648 (16.2%). CDIV complications were observed in 191 (4.8%). Reoperation occurred in 199 (5.0%) patients, and 335 (8.4%) were readmitted. A total of 1442 (36.0%) patients were discharged to a non-home destination, and 2047 (51.1%) experienced an extended length of stay. Mortality was reported in 56 (1.4%) patients.
PLV Characteristics
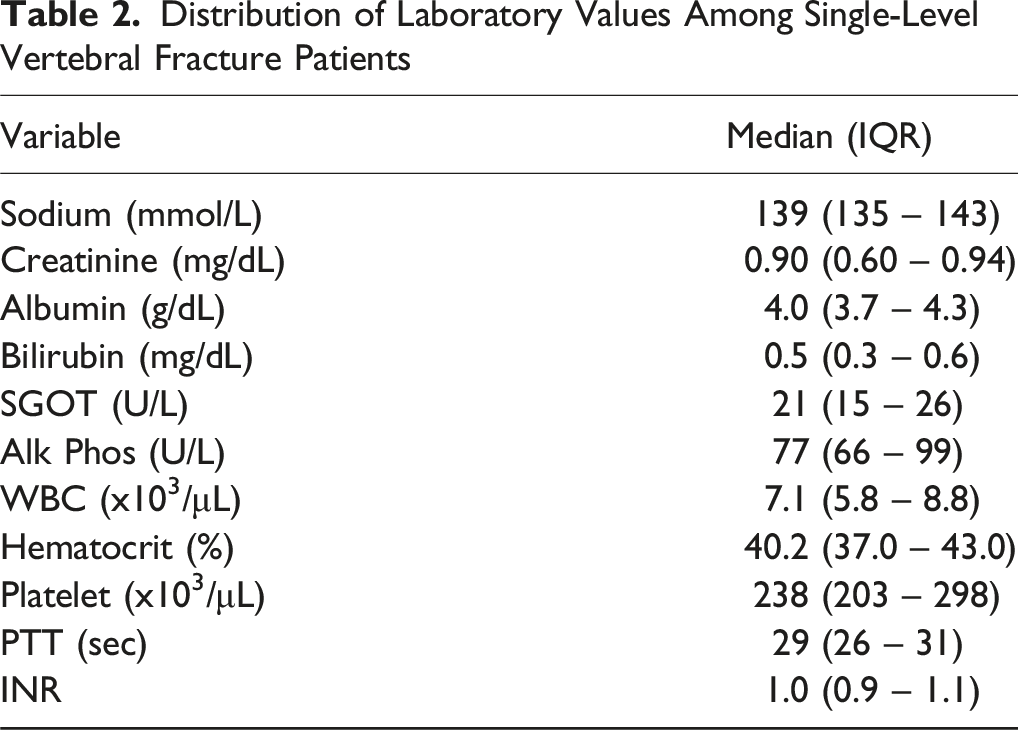
Distribution of Laboratory Values Among Single-Level Vertebral Fracture Patients
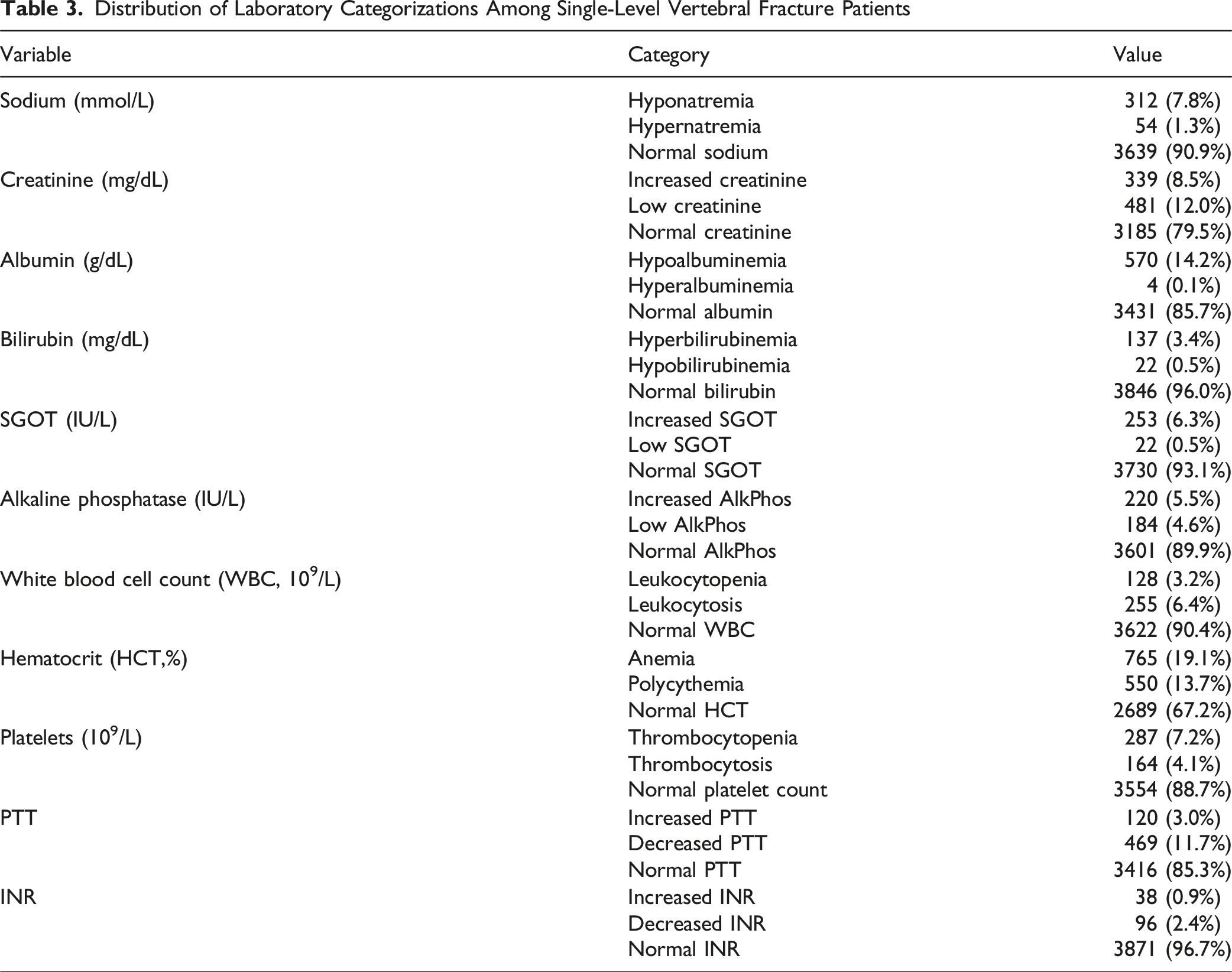
Distribution of Laboratory Categorizations Among Single-Level Vertebral Fracture Patients
Univariate Analysis
Univariate Analysis for the Association of PLVs and Adverse 30-Day Outcomes
Multivariate Analysis
Multivariate Analysis for the Association of PLVs and Adverse 30-Day Outcomes Controlling for Age, Sex, Race, Ethnicity, BMI, Inpatient Status, Total Operation Time, and Total Length of Stay
Sensitivity and Subgroup Analysis
Sensitivity analyses excluding PACS variables and stratifying by operative urgency (elective vs non-elective) demonstrated the robustness of these associations (Supplemental Tables 1 and 2). Across both subgroups, hypoalbuminemia, elevated creatinine, and anemia remained independent predictors of mortality, major complications, NHD, and eLOS. In non-elective cases, increased creatinine (OR 2.77, 95% CI 1.52-5.05, P < 0.001) and hypoalbuminemia (OR 2.90, 95% CI 1.30-6.47, P = 0.01) were the strongest predictors of mortality. Elective subgroup analysis confirmed consistent associations for hypoalbuminemia (OR 3.70, 95% CI 1.95-7.10, P < 0.001) and anemia (OR 3.70, 95% CI 1.85-7.30, P < 0.001). Exclusion of PACS did not materially alter the direction or magnitude of effects.
Discussion
Our ACS-NSQIP analysis found that preoperative hypoalbuminemia was the most consistent predictor of mortality, major complications, readmission, eLOS, and NHD following single-level vertebral fixation in adults. Elevated preoperative creatinine and leukocytosis also independently predicted increased mortality and CDIV complications, while anemia correlated with increased morbidities and longer hospital stays. Other PLVs, such as hyperbilirubinemia and thrombocytosis, were predictive of singular outcomes but demonstrated limited consistency across others. Thus, to our knowledge this study represents the first to present national-level data describing the utility of PLVs for preoperative risk stratification in those patients sustaining vertebral fractures. Incorporating these findings into a spine surgeon’s assessment of patients sustaining vertebral fractures may strengthen the utility of their preoperative risk assessment and provide the surgeon with the ability to provide patient-centric care.
Of all surveyed PLVs, significantly decreased serum albumin persistently predicted adverse post-surgical events. Hypoalbuminemia itself is a marker of malnutrition, inflammation, and lower physiologic reserve, with a well-established relation to hospital morbidity and mortality.19-21 In particular, low serum albumin has been associated with increased risks of sepsis, reintubation, and mortality in spinal surgery for metastatic disease, as well as in a variety of non-spinal procedures such as thyroidectomy.22,23 Due to its roles in osmotic equilibrium, biochemical transport, free radical neutralization, and relation to frailty, low albumin levels result in detriments to wound healing and immune health that predispose patients to postoperative complications and mortality.24,25 In a study by Adogwa et al, serum albumin of less than 3.5 g/dL independently predicted both 30-day complications and mortality in degenerative spine procedures, in lieu with our findings. 26 Furthermore, it is important to consider that these vertebral fractures often occur in older populations, with high-risk comorbidities such as osteoporosis or systemic illness, thus more likely to have poor PLV status. 27 Preoperative immobility and sarcopenia, together with the substantial involvement of spine surgery, likely contextualize hypoalbuminemia as an indicator of systemic vulnerability, reflecting both pre-existing risk and acute physiologic decompensation. 28 Given its prognostic significance, routine preoperative assessment of serum albumin and nutritional markers should be considered to identify modifiable risk in vulnerable patients. In cases of borderline surgical indication, medical optimization, including nutritional support, may provide clinical benefit by enhancing physiologic reserve and improving operative candidacy. 28
Elevated creatinine, anemia, and leukocytosis were additionally found to be independently associated with adverse outcomes following fixation for single-level vertebral fractures. Poor renal function implicates processes such as hemostasis, immunity, and fluid balance, with Purvis et al. documenting the relationship between low GFR and elevated creatinine with increased short-term morbidity rates following lumbar fusions in patients not requiring hemodialysis, consistent with our findings for single-level fixation. 29 Renal impairment alters fluid balance, impairs platelet function, and diminishes the clearance of anesthetics and antibiotics, all of which may compound perioperative risk. 30 Moreover, complications, readmissions, and non-home discharges were significantly increased in patients with anemia, likely due to reduced oxygen delivery and impaired wound healing following surgery. 31 Importantly, anemia is a modifiable condition, and recent work by Ranucci et al. in cardiac surgery patients demonstrated that correcting anemia preoperatively reduced intensive care and hospital stays. 32 This aligns with a growing body of spine literature demonstrating that preoperative anemia independently predicts higher rates of perioperative transfusion, infection, prolonged length of stay, and mortality across both elective and emergent spinal procedures, supporting the notion that prehabilitation and medical optimization may offer tangible benefit in similarly vulnerable spine surgery populations.33,34 Leukocytosis as a marker of inflammation or infection elucidates potential for our finding of increased Clavien IV complications and readmissions, suggesting that leukocytosis may serve as a proxy for underlying systemic inflammation or occult infection, which may predispose patients to cascading organ dysfunction after surgery. 35 Collectively, these biomarkers reflect distinct physiologic systems impairments that can predispose vertebral fracture patients to adverse outcomes following surgery. While the individual associations between PLVs and adverse outcomes are well established, our study is among the first to demonstrate their prognostic value specifically in patients undergoing surgical fixation for single-level vertebral fractures, a heterogeneously treated population. By contextualizing these lab values within this specific surgical indication, our findings offer practical insight that may inform case selection, guide surgical timing, and support individualized risk stratification protocols moving forward. However, as highlighted in our subgroup analysis, many patients presenting with vertebral fractures undergo non-elective surgery, limiting opportunities for preoperative optimization. In these cases, nutritional status often reflects the patient’s acute physiological stress rather than modifiable chronic malnutrition. Nevertheless, routine assessment of serum albumin both preoperatively and postoperatively may help identify high-risk patients early in their recovery course.
PLVs are simple, low-cost, and universally obtained during preoperative surgical and anesthetic assessments. Their predictive associations with a wide spectrum of adverse outcomes and ease of assimilation, support their integration into preoperative evaluation tools and risk stratification models for spine surgery. The significantly poor outcomes in single-level vertebral fixation outcomes in patients with preoperative hypoalbuminemia, anemia, and leukocytosis indicate that certain PLVs can serve as simple, yet integral biomarkers to enhance risk stratification and inform patient management. Integrating these data into operative vs conservative management discussions between surgeons and patients may reduce adverse outcomes in high-risk patients, and optimize resource allocation. Incorporating routine preoperative screening for albumin, hematocrit, and white blood cell count, even in time-constrained emergent cases, can help stratify patients by physiological reserve and inflammatory burden before surgery. Identifying such abnormalities early enables clinicians to anticipate perioperative risks, adjust fluid and transfusion thresholds, and tailor anesthetic and hemodynamic management accordingly. 36 Given patients may not have time for preoperative optimization for PLV, identification preoperatively, can allow for interventions in the postoperative setting such as early dietary supplementation, enteral nutrition support, close monitoring of albumin trends, erythropoiesis-stimulating therapy, fluid optimization, and infection screening could be potential targets for improvement based on these biomarkers.37-39 By integrating PLV thresholds into a standardized pathway, preoperative screening, optimization, and discharge planning, clinicians may further mitigate the 9.3% major complication rate and 1.4% mortality observed in this cohort.
Limitations
Our study has several important limitations. First, this was a retrospective database study, which inherently introduces the risk of selection bias, coding inaccuracies, and unmeasured confounding. Radiographic parameters, fracture morphology, fracture type, and specific indications for surgical fixation (eg, mechanical instability, neurologic compromise) were not uniformly captured, limiting our ability to adjust for fracture severity or operative decision-making nuances. Second, 80% of analyzed cases were classified as elective procedures, which may reflect both the lower-energy nature of single-level vertebral fractures and potential database coding practices; this could bias the cohort toward healthier patients or those optimized preoperatively, thus underestimating the effect of abnormal PLVs on outcomes in truly emergent settings. Third, our analysis was restricted to 30-day outcomes, precluding the assessment of long-term complications, functional recovery, or mortality beyond the immediate postoperative period. Fourth, although multivariate adjustments were performed for available demographic and comorbidity variables, unmeasured patient-level factors such as socioeconomic status, access to perioperative optimization, frailty indices, and nutritional interventions may confound the associations we observed. Additionally, misclassification of elective vs non-elective status may have occurred, which could introduce classification bias into the presented findings. Finally, PLVs themselves can be influenced by acute illness or injury-related stress responses, meaning that some abnormal values may reflect transient physiologic derangements rather than chronic health status, which could attenuate their predictive specificity.
Conclusion
Preoperative hypoalbuminemia, anemia, and elevated creatinine are independent predictors of adverse 30-day outcomes following single-level vertebral fixation, with hypoalbuminemia consistently predicting mortality, major complications, and non-home discharges. Prospective validation and incorporation into clinical pathways may improve risk assessment and perioperative care.
Supplemental Material
Supplemental Material - Prehab the Labs: Predicting Surgical Outcomes in Spine Fractures Through Preoperative Lab Values
Supplemental Material for Prehab the Labs: Predicting Surgical Outcomes in Spine Fractures Through Preoperative Lab Values by Omar Sbaih, Gabrielle L. Dykhouse, Hikmat R. Chmait, Nithin Gupta, Mark Miller, Matthew Meade, Ruchir Nanavati, William DiCiurcio, Christopher Kepler, Barrett Woods in Global Spine Journal
Footnotes
Ethical Consideration
This study was determined to be exempt from Institutional Review Board (IRB) review as it utilized de-identified patient data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. No direct patient contact or identifiable private information was involved.
Consent to Participate
Not applicable - patient consent was not required for use of de-identified database records.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP). Restrictions apply to the availability of these data, which were used under license for the current study, and so they are not publicly available. Data are, however, available from the authors upon reasonable request and with permission from the ACS-NSQIP.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.