
Abstract
Study Design
Retrospective cohort study.
Objectives
To update national estimates of in-hospital mortality after lumbar fusion, characterize when deaths occur during hospitalization, and identify independent predictors of mortality.
Methods
Adult (≥18 years) lumbar fusion hospitalizations in the National Inpatient Sample (NIS) from 2016 to 2022 were analyzed. The primary outcome was in-hospital mortality. Secondary outcomes included hospital-day timing of death and survivor–decedent comparisons of comorbidity and perioperative complication profiles. Multivariable logistic regression identified independent predictors (P < 0.05).
Results
Among 1,181,465 weighted admissions, mortality was 0.11% (1290 deaths) and occurred early (approximately 50% within 7 days; >90% by ∼ 30 days). Decedents more often underwent multilevel fusion (67.8% vs 38.8%, P < 0.001), were aged ≥75 years (41.5% vs 16.5%, P < 0.001), and had higher comorbidity burden (mean Elixhauser count 3.92 vs 2.15, P < 0.001). Independent predictors included age ≥75 years (OR 4.49, P = 0.003), multilevel fusion (OR 2.09, P < 0.001), congestive heart failure (OR 4.46, P < 0.001), coagulopathy (OR 3.44, P < 0.001), neurologic disorders (OR 9.27, P < 0.001), peripheral vascular disease (OR 1.61, P = 0.031), and higher comorbidity count (per-point OR 1.16, P = 0.010). Female sex (OR 0.72, P = 0.022) and highest income quartile (OR 0.58, P = 0.009) were protective.
Conclusions
In-hospital mortality after lumbar fusion is uncommon but concentrates early and disproportionately affects older, medically complex patients undergoing multilevel procedures, supporting preoperative counseling, front-loaded perioperative risk stratification, and heightened early postoperative vigilance.
Keywords
Introduction
By 2050, the number of individuals in the United States (U.S.) who are 65 years or older is projected to more than double to 89 million. 1 As the population ages, spine surgery remains a common treatment for degenerative conditions. Procedure volumes have increased from about 800,000 in 2013 to more than 1.1 million in 2022, largely driven by lumbar and cervical fusions. 2 Although these operations often improve pain and function, they carry meaningful risks, particularly for older adults and those with multiple comorbidities. To this end, there is a growing need for careful counseling and perioperative planning. 3
Prior studies have linked mortality after lumbar fusion to demographic and clinical factors, including age, sex, race, and comorbidity burden. 4 Procedure characteristics also influence risk. Posterior and transforaminal lumbar interbody fusion have been associated with greater morbidity than anterior or lateral approaches. 5 Increasing use of complex spine procedures has been associated with higher mortality. 6 Revision lumbar fusion has been tied to longer hospitalization and higher costs, reflecting worse outcomes for patients and greater strain on health systems. 7 However, much of the existing literature relies on single-center cohorts or narrow time frames, which limits contemporary, nationwide estimates.
To address these gaps, we analyzed a large, nationally representative inpatient dataset from 2016 to 2022 to update estimates of in-hospital mortality after lumbar fusion. In this study, we aimed to: (1) estimate the national rate and timing of in-hospital death after lumbar fusion; (2) compare patient, hospital, comorbidity profiles, and perioperative complications between patients who died in-hospital and those who did not; and (3) determine independent predictors of in-hospital mortality. Overall, we hypothesized that mortality risk would be greater among older patients, those undergoing multilevel fusions, and those with substantial comorbidity burden.
Methods
Data Source
We conducted a retrospective observational study using the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS) from 2016 to 2022, a stratified sample of U.S. community hospital discharges that yields national estimates when survey weights, strata, and clusters are applied. 8 As the data are de-identified and publicly available, this study was exempt from Institutional Review Board (IRB) approval, and individual informed consent was not required.
Cohort Identification and Exclusions
We identified adult (≥18 years) hospitalizations in which a lumbar fusion procedure was performed during the index admission. We excluded nonelective admissions; records with missing or implausible age or missing essential hospital, payer, or cost fields; cases in which the index fusion was not performed on hospital day 0; and encounters with negative values for length of stay or costs. HCUP privacy rules were followed throughout, with cell counts ≤10 being suppressed.
Outcome definition
The primary outcome of interest was in-hospital mortality, defined as death occurring before discharge, based on the discharge disposition. We summarized the timing of death by hospital day among decedents and plotted the cumulative weighted percentage of total in-hospital deaths by length of stay.
Patient, Hospital, and Clinical Characteristics
Demographics included age group, sex, and race. Socioeconomic variables included ZIP code–based income quartile and primary payer. Hospital characteristics were U.S. Census region, bed size, and teaching status. Procedural complexity was classified as single-level vs multilevel fusion. Comorbidities were derived from ICD-10-CM diagnoses using Elixhauser definitions; a summary Elixhauser Comorbidity Index (ECI) was calculated as the count of present conditions. Index-admission complications were identified using validated ICD-10-CM/PCS code sets and summarized descriptively.
Statistical Analysis
All analyses incorporated the NIS complex survey design to produce nationally representative estimates with appropriate variance. Baseline characteristics were compared between survivors and decedents using survey-weighted proportions and means; group differences were assessed with Rao–Scott χ2 tests (categorical variables) and survey-weighted Wald tests (continuous variables).
To identify factors independently associated with in-hospital mortality, we fit a survey-weighted logistic regression including year, age group, sex, race/ethnicity, primary payer, income quartile, hospital region, bed size, teaching status, number of levels fused, selected Elixhauser comorbidities, and the ECI. Categorical covariates with >2 levels were modeled using indicator (dummy) variables with a prespecified reference category. Multicollinearity was assessed using variance inflation factors (VIFs) for all covariates in the final multivariable model; all VIFs were <2.5, indicating low collinearity. Complications were not included as predictors to avoid controlling for potential mediators. Because complications occur after surgery and may lie on the causal pathway to in-hospital mortality, adjusting for them could result in overadjustment and biased estimates for baseline and procedural predictors. Statistical significance was set at P < 0.05. Analyses were performed in R (version 4.4.0; R Foundation for Statistical Computing, Vienna, Austria).
Results
Cumulative Timing of In-Hospital Mortality
Among lumbar fusion admissions, deaths accumulated rapidly over the initial hospital days and then approached an asymptote with prolonged stays. Approximately half of all in-hospital deaths occurred within the first week, and greater than 90% by about one month (Figure 1). Cumulative in-hospital mortality by length of stay
Patient Characteristics by Mortality Status
Patients Demographics in Lumbar Fusion Patients
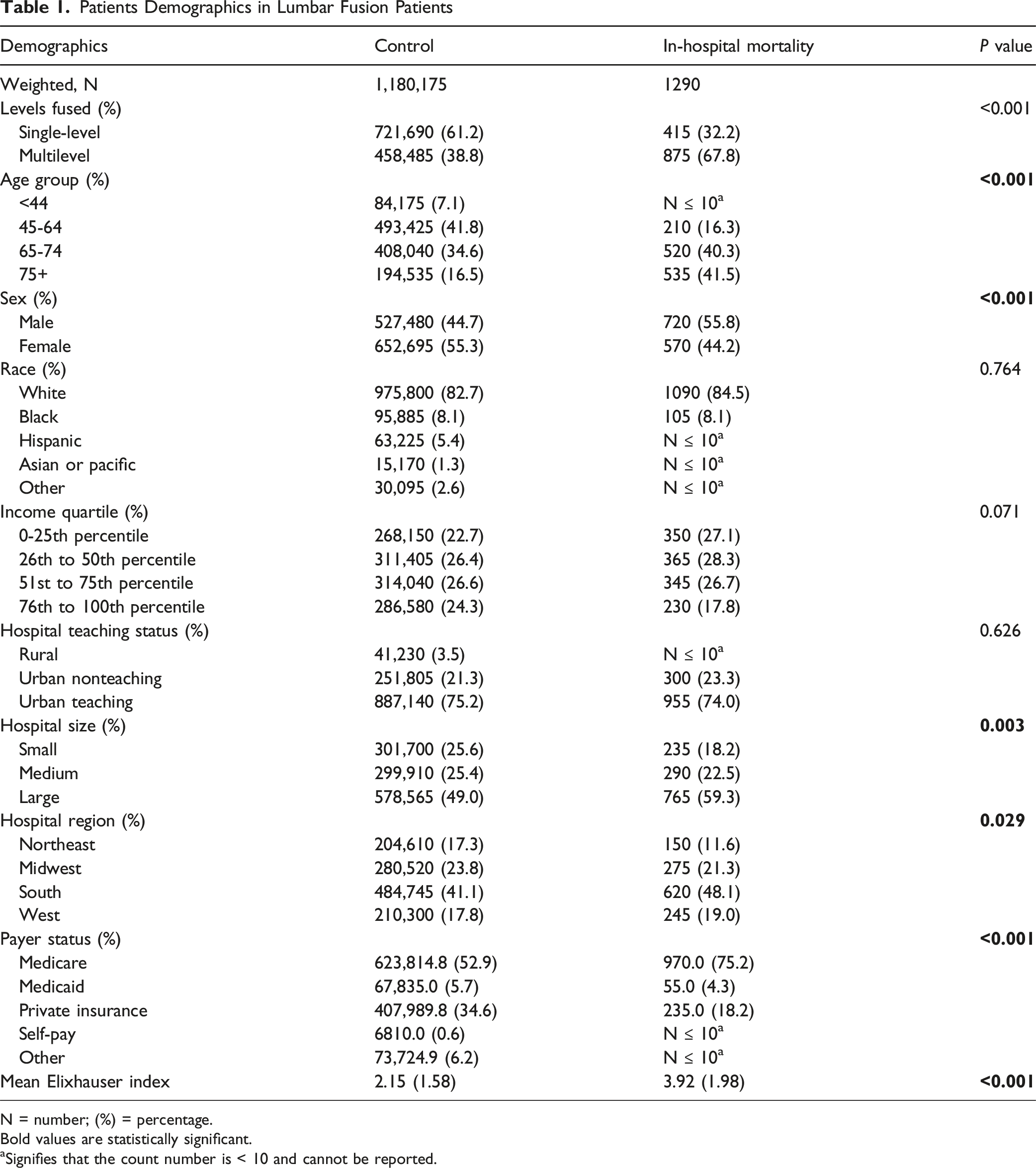
N = number; (%) = percentage.
Bold values are statistically significant.
aSignifies that the count number is < 10 and cannot be reported.
Comorbidities
Prevalence of Comorbidities
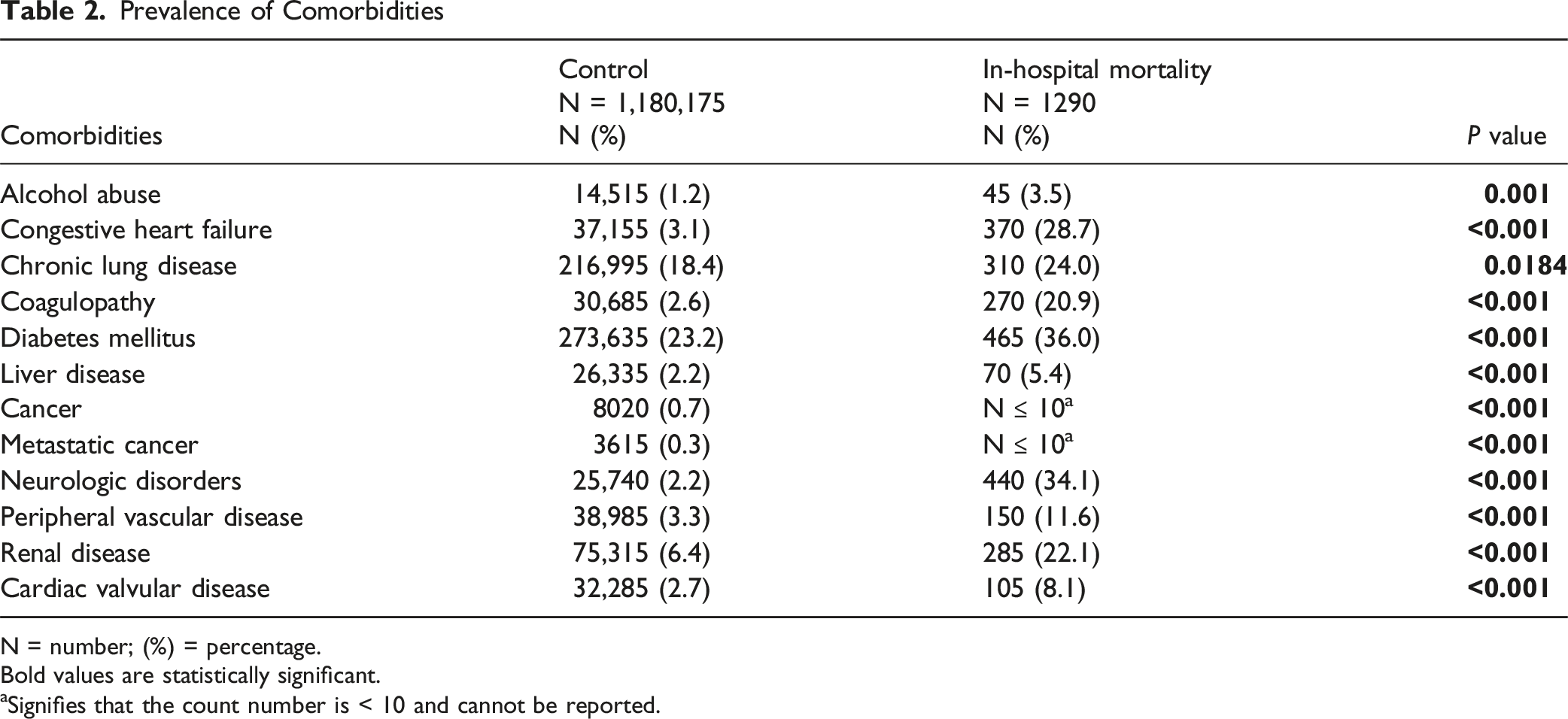
N = number; (%) = percentage.
Bold values are statistically significant.
aSignifies that the count number is < 10 and cannot be reported.
Perioperative Complications
Prevalence of Complications
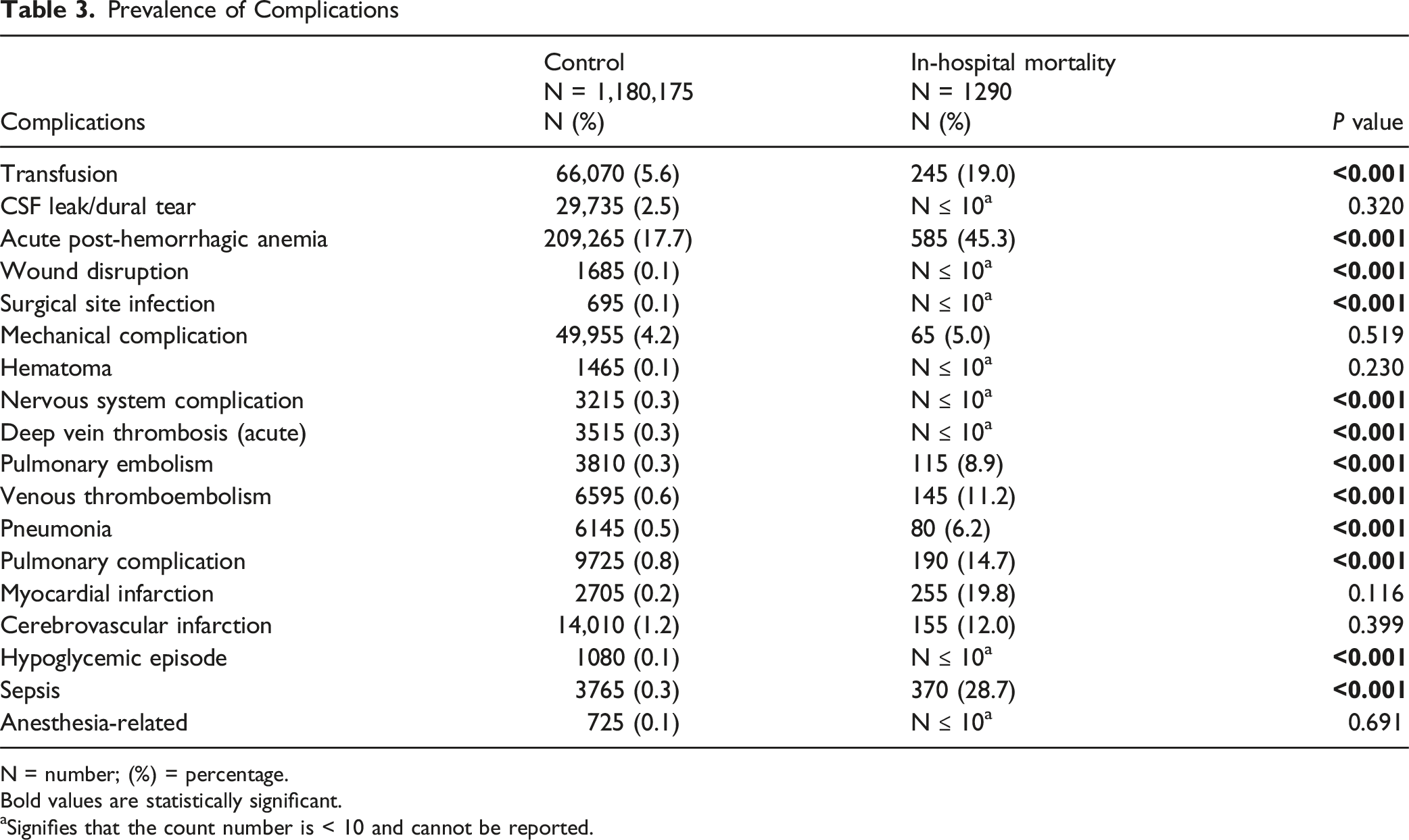
N = number; (%) = percentage.
Bold values are statistically significant.
aSignifies that the count number is < 10 and cannot be reported.
Multivariable Predictors of In-Hospital Mortality
Multivariable Analysis of Factors Associated With In-Hospital Mortality in Lumbar Fusion Patients
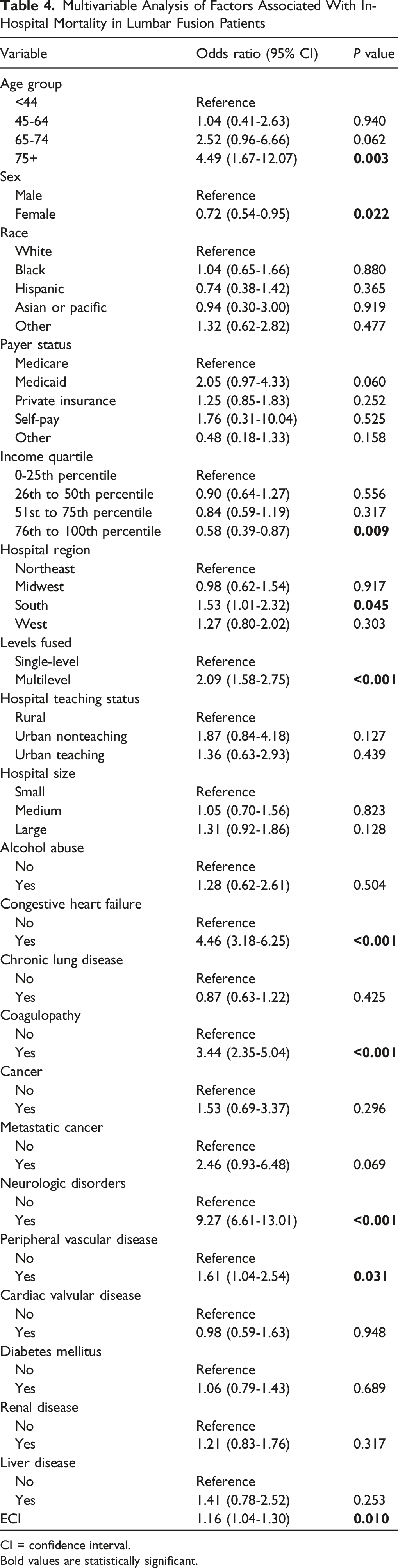
CI = confidence interval.
Bold values are statistically significant.
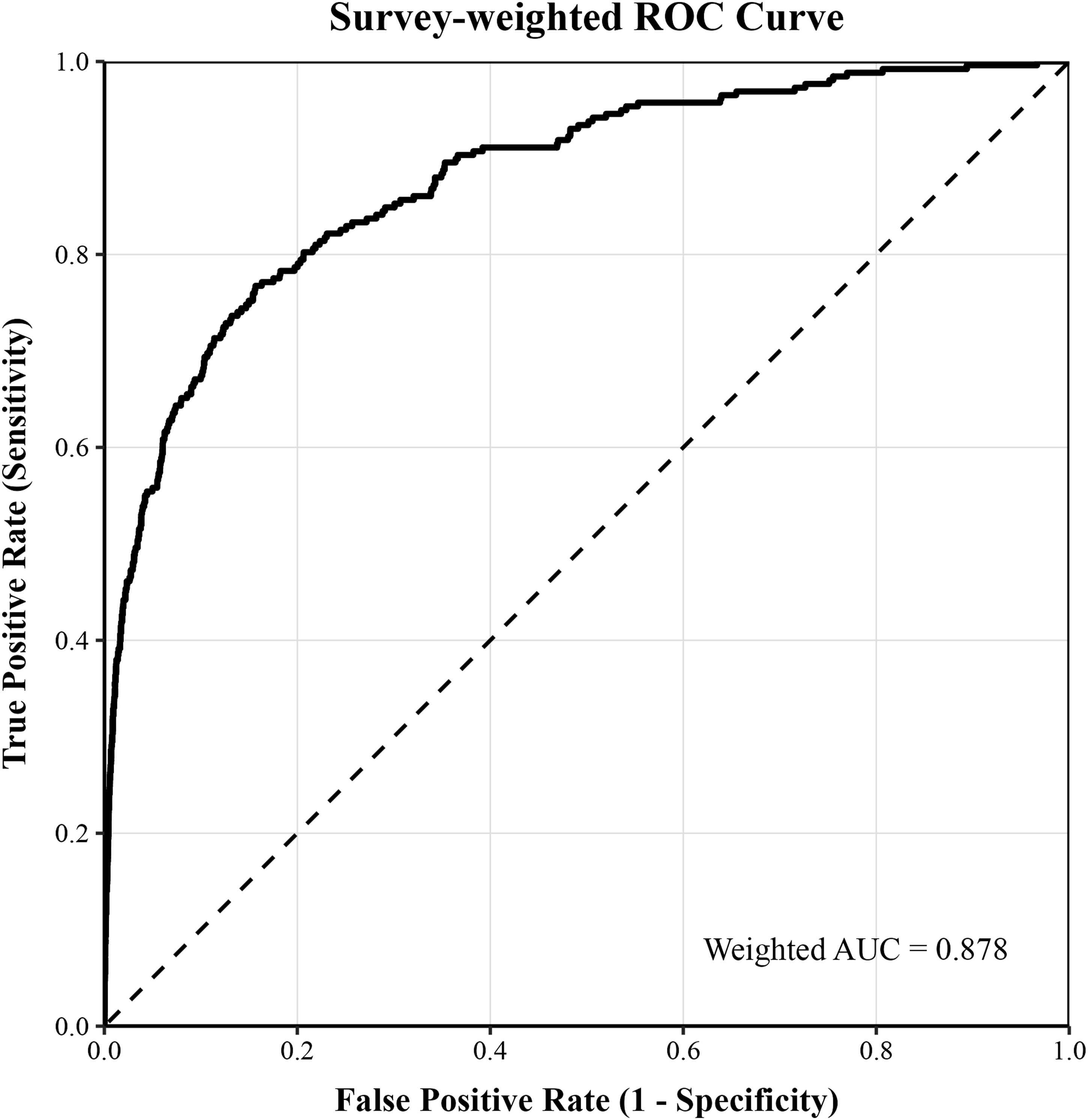
Receiver operating characteristic (ROC) curve for the multivariable model predicting in-hospital mortality
Discussion
In-hospital death after lumbar fusion is uncommon on a per-case basis but carries outsized clinical and operational consequences given the scale of spine surgery in the U.S., now exceeding a million procedures annually, and the growing proportion of older, medically complex patients. In this contemporary, nationally representative cohort from 2016 to 2022, we observed that mortality clustered early in the hospitalization, concentrated among older adults with greater comorbidity burden and those undergoing multilevel fusion. Fatal courses were marked by a distinctive complication profile (thromboembolic, pulmonary, and infectious events), suggesting that the early postoperative period is an important time to recognize evolving risk in patients with greater baseline burden and procedural complexity.
In-hospital mortality after lumbar fusion was low overall but occurred early in the hospitalization, and fatal cases frequently involved thromboembolic, pulmonary, and infectious complications. This early concentration of deaths is consistent with a prior national database study by Pumberger et al that found an average inpatient mortality rate of 0.2 percent and reported that more than half of fatalities occurred by postoperative day nine. 6 The same national analysis identified cerebrovascular events, sepsis, and pulmonary embolism as leading lethal complications. 6 The downstream burden of venous thromboembolism after spine fusion is substantial, with longer length of stay, lower odds of home discharge, higher index costs, and greater long-term utilization through 18 months. 9 These findings underscore the immediate postoperative period as an important interval for heightened vigilance and risk-aware management of thromboembolic and infectious events. Beyond the index admission, population-based data show an ongoing mortality burden in lumbar fusion cohorts, including a notable share of analgesic-related deaths over longer follow-up, underscoring the need for structured postoperative surveillance and medication stewardship. 10
Compared with survivors, patients who died were older, more medically complex, more likely to undergo multilevel fusion, and experienced higher rates of bleeding, thromboembolic, pulmonary, and infectious complications. Prior studies have shown that advanced age and comorbidity are concentrated among those who died after lumbar fusion, and octogenarians have markedly higher 90-day and one-year mortality than patients aged 65 to 79 following one to two level posterolateral fusion.6,11 Specific comorbidities that were overrepresented in the mortality cohort, such as congestive heart failure and renal disease, have been independently linked to mortality after lumbar fusion.6,12 Coagulation abnormalities are powerful predictors of serious morbidity and death after posterior lumbar fusion, including abnormal platelet count, elevated partial thromboplastin time, and elevated international normalized ratio. 13 Venous thromboembolism after spinal fusion is associated with longer hospitalization, lower rates of home discharge, and higher costs, reinforcing its clinical importance in adverse trajectories. 9 Prior studies have further shown worse inpatient safety measures for Black and Hispanic patients after lumbar fusion despite adjustment, and lower household income is associated with longer stays and lower rates of home discharge.14,15 In cohorts with chronic kidney disease, chronic steroid use did not significantly change short-term complications or mortality, highlighting that some medication-related risks may be more nuanced than comorbidity burden alone suggests. 16 This pattern aligns with the clinical profile of patients who died and suggests that bleeding–coagulation, renal, and thromboembolic pathways may be important contributors to fatal in-hospital courses.
After adjustment, older age and multilevel fusion were associated with higher odds of in-hospital death, while markers of medical and social risk remained important contributors. A prior national analysis identified older age, male sex, and large hospital size as independent predictors of inpatient death after lumbar fusion. 6 Comorbidity-specific signals that we observed are well documented: congestive heart failure and renal disease are associated with increased mortality risk, and abnormal coagulation parameters independently predict major complications and death after posterior lumbar fusion.6,12,13 Frailty stratifies risk after posterior lumbar interbody fusion in contemporary NIS cohorts, with stepwise increases in mortality and non-home discharge across Risk Analysis Index tiers. 17 Socioeconomic and systems factors also shape outcomes. Lower income is linked to more resource-intensive recoveries after lumbar fusion, and national work documents regional and hospital-level variation in cost and practice patterns for lumbar surgery that may reflect differences in pathways and resources.15,18 Evidence on surgical complexity remains nuanced, as registry data in lumbar stenosis indicate that fusion does not invariably increase complications after adjustment for age and ASA status, and a large state cohort found no excess mortality for elective one to two level constructs compared with baseline.4,19 Differences in operative technology also matter. In a contemporary NIS analysis, robotic-assisted lumbar fusion had minimal mortality overall but higher risks of blood loss anemia, acute kidney injury, and transfusion, as well as higher charges, compared with navigation-guided surgery, informing risk and resource planning. 20 From a preoperative counseling perspective, these results may help surgeons communicate individualized short-term risk — particularly for older patients with substantial comorbidity burden who may require multilevel constructs — and set expectations regarding early inpatient monitoring needs, potential complications, and discharge disposition.
This study has several potential limitations. First, reliance on the NIS database, while nationally representative at the discharge level, is subject to coding inaccuracies and lacks clinical granularity. We could not capture preoperative functional status, frailty beyond claims-derived indices, surgical approach and technique, number and staging of levels, operative time, estimated blood loss, implant selection, anesthesia details, or standardized enhanced recovery and thromboprophylaxis protocols. The database does not report cause of death and cannot link inpatient records to outpatient data, precluding assessment of readmissions, post-discharge mortality, longer-term complications, or quality of life. As with any administrative dataset, exposure and outcome misclassification is possible, including elective vs nonelective status, revision status, complication timing, and comorbidity burden. Hospital and surgeon volume, perioperative care pathways, and medication use (eg, opioid prescribing and patient adherence) were unavailable, limiting evaluation of system-level and pharmacologic contributors to risk. Our regression models intentionally excluded complications to avoid adjusting away mediators from baseline risk to death, but residual confounding may persist. Finally, survey design, weighting, and required suppression of small cells may reduce precision for rare events and limit subgroup analyses. These constraints underscore the need for prospective, multicenter studies with linked inpatient-outpatient data, standardized clinical variables, and longer follow-up to refine risk prediction, clarify causal pathways, and test targeted perioperative strategies for lumbar fusion.
Conclusion
In this nationally representative analysis, in-hospital mortality after lumbar fusion was uncommon yet concentrated early in the stay and disproportionately affected older, medically complex patients undergoing multilevel procedures. Patients over the age of 75, those who underwent multilevel fusion, and those with congestive heart failure, coagulopathy, neurologic disorders, peripheral vascular disease, or greater overall comorbidity were identified as having independent risk factors, while female sex and higher neighborhood income were protective, with regional variation also observed. These findings support front-loaded risk stratification centered on age, comorbidity burden, and fusion extent, and suggest that the early postoperative period may warrant heightened vigilance and risk-aware management of thromboembolic, pulmonary, and infectious events. Beyond perioperative planning, these predictors may support preoperative counseling and shared decision-making regarding expected short-term risk after lumbar fusion. Prospective, multicenter studies with linked inpatient-outpatient data and standardized perioperative variables are needed to refine prediction and test targeted strategies that reduce preventable early deaths after lumbar fusion.
Footnotes
ORCID iDs
Ethical Considerations
No IRB approval or informed consent was required for this review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.