
Abstract
Study Design
Prospective Study.
Objectives
Degenerative lumbar central spinal stenosis (DLCCS) commonly affects the elderly, causing back and leg pain that often necessitates surgical intervention. Perioperative tranexamic acid (TXA) effectively reduces blood loss in lumbar instrumented fusion surgeries. Its effectiveness in elderly patients undergoing posterolateral lumbar instrumented fusion and posterior decompression for DLCCS remains insufficiently investigated. This study aims to evaluate the potential benefits of TXA in these surgical interventions.
Methods
170 patients with DLCCS that underwent posterolateral lumbar instrumented fusion with posterior decompression at two consecutive vertebral levels were included. Patients were divided into two groups: Group A (87) without intravenous TXA and Group B (83) with intravenous TXA 30 minutes preoperatively. Outcomes included intraoperative blood loss, postoperative drainage, transfusion rates, surgical duration, initiation of mobilization and hospital stay.
Results
No significant differences were found in patients’ baseline demographics. Surgical duration was significantly shorter in the TXA group (103.6 ± 9.8 min vs 128.6 ± 8.2 min, P < 0.001). Intraoperative blood loss was lower in the TXA group (462.7 ± 92.0 mL vs 864.4 ± 157.0 mL, P < 0.001), as was postoperative drainage (85.2 ± 47.6 mL vs 207.4 ± 153.5 mL, P < 0.001). Postoperative transfusion was required in 3 TXA patients vs 27 in the non-TXA group (P < 0.001). TXA patients mobilized earlier (7.4 ± 3.4 hours vs 12.1 ± 8.1 hours, P < 0.001) and had a shorter hospital stay (2.1 ± 0.4 days vs 2.6 ± 0.9 days, P < 0.001).
Conclusions
Preoperative TXA administration in this spinal surgery improved surgical and postoperative outcomes and should be considered more.
Introduction
Degenerative lumbar central spinal stenosis (DLCCS) is a common and debilitating condition that causes low back and leg pain in elderly individuals (>65 years old), affecting approximately 103 million people worldwide, leading to functional limitations and reduced quality of life.1-3 Patients with DLCCS who do not respond to conservative treatment (pain medication, physical therapy) for a period longer than 3 to 6 months, accompanied by imaging findings indicative of severe spinal stenosis, are candidates for surgical treatment.4-6 Posterolateral lumbar instrumented fusion combined with posterior decompression is one of the treatment methods for this condition, offering excellent clinical and functional outcomes with fewer postoperative complications, reduced blood loss, and shorter hospital stays compared to other surgical techniques (eg, lumbar circumferential fusion, posterior lumbar interbody fusion).7,8
Although this procedure results in less blood loss compared to other surgical options, blood loss remains a concern for the surgeons. In their effort to reduce perioperative blood loss in these spinal surgeries, the spinal surgeons proposed the use of tranexamic acid (ΤΧΑ). 9 TXA is an antifibrinolytic agent that inhibits plasminogen to plasmin conversion by competing for lysine binding sites to prevent fibrin clot breakdown.10,11 TXA is typically administered orally, topically, or intravenously, and it is effective in reducing intraoperative blood loss and the need for transfusions in spinal surgery.9,12 Although studies have demonstrated the effectiveness of TXA in various types of instrumented lumbar fusion, there is a gap in the literature regarding its efficacy in posterolateral lumbar instrumented fusion with posterior decompression in elderly patients who suffer from a DLCCS at two consecutive levels. 12
Given the limited data in the existing literature concerning the efficacy of ΤΧΑ in posterolateral lumbar instrumented fusion for elderly patients with DLCCS at two consecutive levels, the objective of our study was to examine the potential benefits of TXA administration in these particular surgical interventions. Specifically, we prospectively compared whether the preoperative administration or non-administration of TXA in two respective groups of patients who underwent posterolateral lumbar instrumented fusion affects specific parameters related to intraoperative and postoperative blood loss, the need for blood transfusion, the duration of surgery, the onset of postoperative mobilization, as well as the length of hospital stay.
Materials and Methods
Study Population
The patients who participated in our study suffered from DLCCS and underwent posterolateral lumbar instrumented fusion and posterior decompression, based on scientific indications according to clinical and radiological evaluation. All patients provided us with written consent to participate in the study after being informed about its purpose. The study protocol was reviewed and approved by the Institutional Review Board of the Interbalkan European Medical Center in Thessaloniki, Greece (Approval Number: 1712/13.04.2022). This study refers to patients who are a subgroup of total patients of this protocol on involved hospital. All procedures were conducted in full compliance with the Ethical Principles for Medical Research Involving Human Subjects, as established in the 1964 Declaration of Helsinki and its subsequent amendments, including the 2013 revision.
Inclusion and Exclusion Criteria
Inclusion criteria were (1) DLCCS of grade C and D according to the Schizas classification [Magnetic Resonance Imaging (MRI) findings] at two consecutive vertebral levels, with accompanying symptoms (>6 months) that did not improve with conservative treatment (pain management and physiotherapy), (2) patients aged 66 to 75 years and (3) patients with normal coagulation laboratory tests [Prothrombin Time (PT), International Normalized Ration (INR), and Activated Partial Thromboplastin Time (APTT)].
Exclusion criteria were (1) traumatic lumbar central spinal stenosis, (2) degenerative lumbar scoliosis (Cobb angle> 20°), (3) history of malignancy, (4) hematologic disease, cardiovascular diseases, or coagulation disorders, (5) patients who are receiving anticoagulant therapy or antiepileptic therapy, (6) previous surgery on the lumbar spine, (7) spinal infection, (8) other specific spinal conditions (eg, ankylosing spondylitis or neurologic disorders) and (9) known allergies to TXA.
Methods- Study Design
All patients underwent successful posterolateral lumbar instrumented fusion and posterior decompression due to DLCCS at two consecutive vertebral levels during the period from April 2022 to January 2024. We divided the patients into two groups based on the administration or non-administration of TXA intravenously 30 minutes before the start of the surgical procedure. Group A includes patients who did not receive preoperative TXA, while Group B includes patients who received preoperative TXA (bolus with a dose of 10 mg/kg). We evaluated how the administration or non-administration of TXA affected: (i) the duration of the surgical procedure, (ii) intraoperative blood loss at the surgical site measuring the volumes in ml collected in the suction devices (no hemostatic agents were used intraoperatively in the surgical field), (iii) postoperative blood loss from drainages, (iv) the need for blood transfusion in patients, (v) the time to initiation of patient mobilization, and (vi) the length of hospital stay until patient discharge. The transfusion threshold was defined as hemoglobin <7 g/dL for patients without vascular or renal comorbidities, and <8 g/dL for those with vascular disease or renal impairment. Continuous communication was maintained between the surgeon and the anesthesiologist, carefully balancing the risks of transfusion against those associated with hemorrhage and blood loss, while consistently taking into account the patients’ overall clinical condition.
Surgical Technique
Under general anesthesia, the patients were positioned on a Jackson table in a prone position. Fluoroscopic guidance was used to determine the two consecutive levels of the surgical procedure in the lumbar spine. A standard posterior approach was performed, involving skin incision, subcutaneous tissue dissection, and bilateral subperiosteal dissection of the paravertebral musculature.
13
The facet joints and transverse processes were then identified and prepared, and the entry points for the transpedicular screws were determined. Under constant fluoroscopic navigation, a total of 6 transpedicular screws were placed. Subsequently, posterior decompression with laminectomy-flavectomy was performed, while foraminotomy of the corresponding levels was performed where required. The posterolateral lumbar instrumented fusion was completed by placing titanium rods (6 mm) and autologous bone, along with hydroxyapatite putty (Figure 1). A drainage was placed in each procedure and the wound was closed in layers as per standard procedure. All patients were neurologically assessed immediately after surgery and then transferred to the monitoring unit for 30 minutes before returning to the ward. Lateral (A) and anteroposterior (B) intraoperative fluoroscopic views. The completion of the two consecutive levels (L3- L5) posterolateral lumbar instrumented fusion (transpedicular screws and rods)
Statistical Analysis
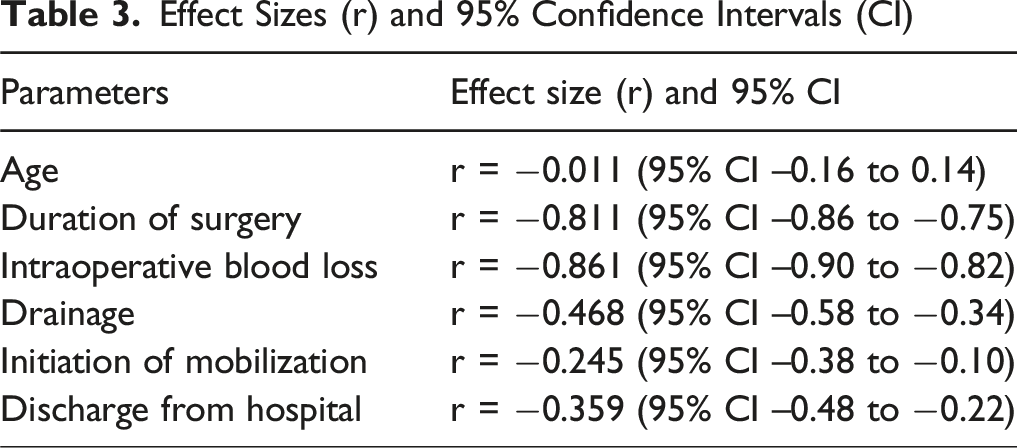
Collected data were analyzed using SPSS (Version 24.0). Continuous variables were expressed as mean and standard deviation (SD), and categorical variables as percentages. Normality was assessed using Shapiro–Wilk, Kolmogorov–Smirnov, and Q–Q plots. The Mann–Whitney U-test was used to compare continuous variables in independent samples with non-normal distribution, with the population divided into two categories. All continuous variables significantly deviated from normality (all P < 0.001) and are therefore presented as median (IQR). Pearson’s χ2 (cross-tabulation) was used to compare categorical variables. The level of significance was set at P < 0.05. Effect sizes (r) and 95% confidence intervals (CI) were computed using Z/√N and Fisher’s z transformation.
Results
Demographic Characteristics of the Patients

CONSORT Flow Diagram
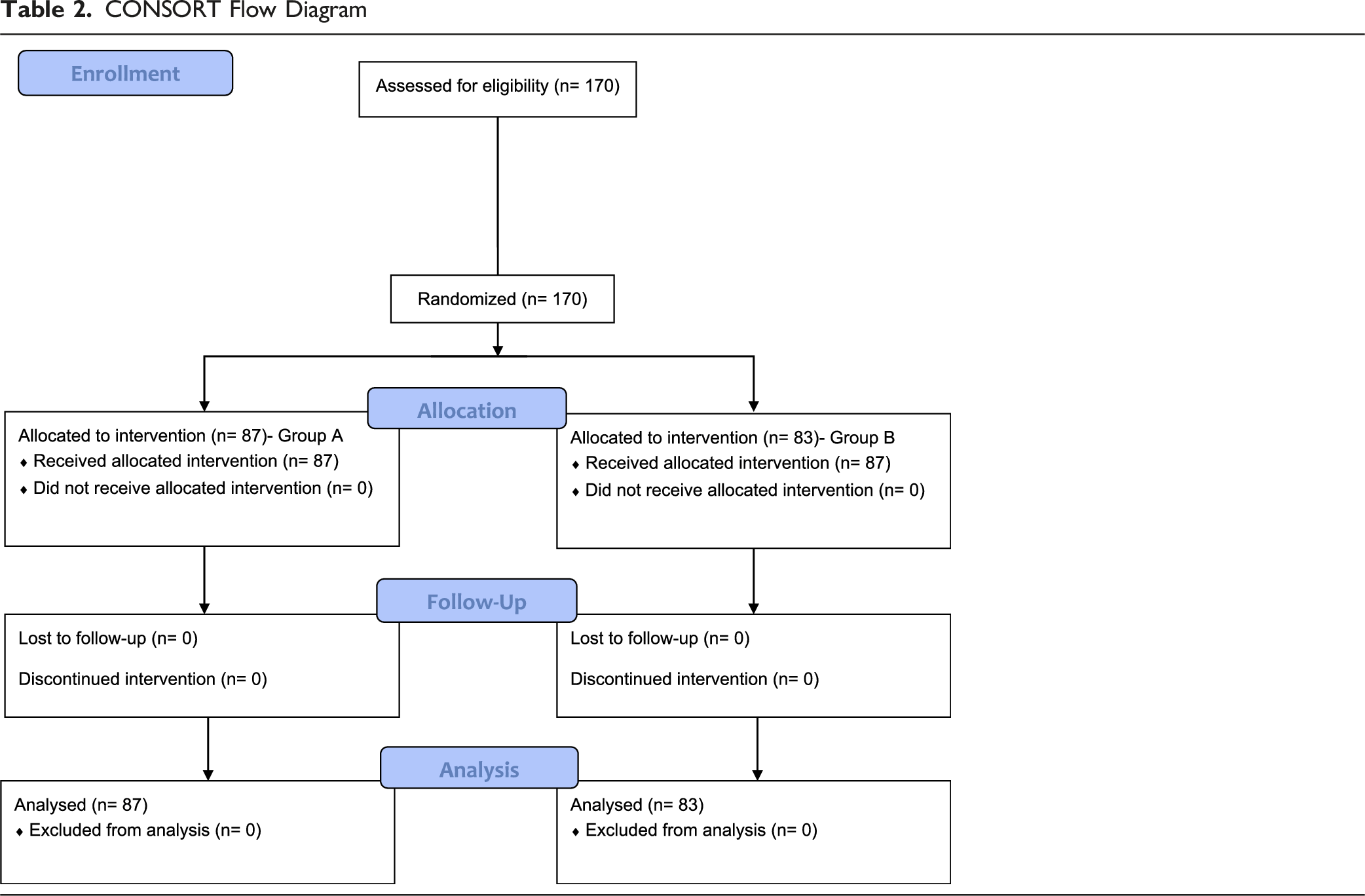

In Group A, the mean body mass index (BMI) was 27 ± 2, whereas in Group B, the mean BMI was 27 ± 4. Among Group A, 26 (30%) patients were smokers, compared to 27 (33%) patients in Group B. None of the participants were receiving pharmacological treatment for osteoporosis. Regarding the spinal levels at which surgical intervention was performed, 72% of procedures (63 patients) in Group A involved the L3–L5 levels and 28% (24 patients) involved L2–L4, whereas in Group B, 74% (61 patients) involved L3–L5 and 26% (22 patients) involved L2–L4. No osteotomies were performed in any of the patients. No statistically significant differences were observed between the two groups with respect to these parameters.
Effect Sizes (r) and 95% Confidence Intervals (CI)
The primary endpoint was intraoperative blood loss. Secondary endpoints included drainage, time to initiate mobilization, length of hospital stay, and postoperative transfusion. Secondary endpoints were considered exploratory because multiple comparisons were performed.
Operation-Related Parameters and Clinical Outcomes

Mean values of the parameters accompanied by Standard Deviation (SD) for the patient groups.
*Statistically significant P-values are highlighted in bold.

Values and diagrams of the parameters we studied for the two groups separately. A: Duration of surgery, B: Intraoperative blood loss, C: Drainage, D: Discharge from hospital
The mean intraoperative blood loss from the surgical field was 864.4 (SD ± 157.0) ml and 462.7 (SD ± 92.0) ml for Group A and Group B, respectively (Table 4). A statistically significant difference (P < 0.001) was observed in this parameter between the two groups (Figure 2B). Evaluating the postoperative blood loss from the drainages (which were removed 24 hours postoperatively in all patients), the mean amount of drainage in Group A was 207.4 (SD ± 153.5) ml, while in Group B it was 85.2 (SD ± 47.6) ml (Table 4). A statistically significant difference (P < 0.001) in postoperative blood loss was also observed between the two groups (Figure 2C).
In Group A, a total of 27 patients received postoperative transfusion, whereas only 3 patients in Group B required transfusion (Figure 3). The statistical analysis showed a statistically significant difference (P < 0.001) between the two patient groups. It is noteworthy that no patients in either group received an intraoperative transfusion. The distribution of patients who received blood transfusion postoperatively in each group
Patients who did not receive blood transfusion were mobilized approximately 6-8 hours after surgery, while those who required blood transfusion began mobilization 24 hours after surgery. As indicated by our statistical data, the mean time to initiate mobilization for patients in Group A was 12.1 (SD ± 8.1) hours, while the corresponding time for patients in Group B was 7.4 (SD ± 3.4) hours (Table 4). A statistically significant difference was observed between the two groups in this parameter as well (P < 0.001).
Studying the time each group of patients was discharged from the hospital, it was found that patients in Group A had an average length of hospital stay of 2.6 (SD ± 0.9) days, while patients in Group B had an average length of stay of 2.1 (SD ± 0.4) days (Table 4). A statistically significant difference (P < 0.001) in the length of stay between the two groups was observed (Figure 2D).
In multivariable logistic regression, duration of surgery remained the only independent predictor of transfusion. TXA did not retain significance after adjustment (P = 0.348), likely due to collinearity. The unadjusted association remained strong (χ2 P < 0.001).
Discussion
The use of perioperative TXA has been a widely accepted practice across multiple orthopedic subspecialties.14,15 It has also been studied in certain spinal surgeries; however, there is limited available literature to determine its clinical utility in posterolateral lumbar instrumented fusion and posterior decompression due to DLCCS at two consecutive vertebral levels in the elderly patients. In this study, we aimed to bridge that gap and examined the effect of TXA on intraoperative blood loss, postoperative drainage, postoperative transfusion rates, initiation of patient mobilization, time to discharge and the duration of surgery.
Our study suggests that TXA administration was associated with shorter operative time and reduced blood loss. Since intraoperative blood loss from the surgical field was lower in the TXA group, we observed that less time was spent on hemostasis during the surgery. These results likely led to a shorter duration of the surgery. Based on our results, the administration of TXA led to lower amounts of postoperative blood loss in patients who received it preoperatively. Following the established criteria for blood transfusion in patients undergoing surgery, fewer patients in the TXA group required transfusion. Therefore, we conclude that the preoperative administration of TXA significantly reduced the number of transfusions. 16 These data are consistent with the intraoperative and postoperative blood losses from the surgical field, as patients with less blood loss required a limited number of transfusions. In addition, we suggest that the need for blood transfusion delayed the initiation of patient mobilization by the physiotherapists. It appears that patients who did not receive preoperative TXA were delayed in their discharge from the hospital, which can be attributed to their delayed mobilization and increased need for postoperative blood transfusion.
The existing literature includes data on the preoperative use of TXA in surgeries performed on patients with spinal stenosis who have undergone instrumented fusion and decompression. Wang et al, 17 in a randomized controlled trial, included 60 patients with degenerative lumbar instability with stenosis who underwent Posterior Lumbar Interbody Fusion (PLIF). Thirty of these patients received preoperative TXA, and the authors evaluated postoperative blood loss in comparison to the other 30 patients who did not receive preoperative TXA. Postoperative blood loss in the TXA group was significantly lower than in the control group by 13.0%. This is consistent with our study, where postoperative blood loss from drainages was higher in the group of patients who did not receive TXA.
Perioperative blood loss was also evaluated in patients who underwent multilevel lumbar laminectomy and lumbar posterior spinal fusion with transforaminal intervertebral fusion, who received preoperative intravenous TXA. In this specific retrospective cohort study, Lotan et al 18 concluded that the preoperative administration of TXA led to less intraoperative and postoperative blood loss and recommends the routine administration of preoperative TXA as efficacious and safe in reducing perioperative blood loss in these spinal surgeries.
In another randomized clinical trial involving 50 patients who underwent laminectomy (for ≥2 levels) with posterolateral lumbar instrumented fusion, the 25 patients who received intravenous preoperative TXA had lower blood loss both intraoperatively and postoperatively compared to those who did not receive TXA. 9 This current bibliographic reference further supports our findings, as in addition to the lower postoperative blood loss observed in our patients who received TXA, intraoperative blood loss was also lower in this group. The same study referenced earlier concludes that TXA use reduces the need for packed cell transfusions and shortens the length of hospitalization. 9 In our study, only 3 patients from the group that received TXA required postoperative blood transfusions. This affects cost savings for hospitals and surgeons and improves blood resources available for other critical patients. Additionally, the length of hospitalization for these patients was statistically significantly shorter, with a mean discharge time of 2.1 days. This reduction holds its importance in high-volume surgical settings and patient satisfaction rates, especially in elderly patients who benefit more from quicker returns to daily activities.19,20
However, the variability in transfusion practices might impact on the results, as institutional protocols and surgeon preferences influence the numbers. There is a recent study by Setliff et al 21 that didn’t find a reduction in transfusion rates with TXA use, which contrasts with ours. It is important for the spinal surgery community to consider the different types of dosing regiments or administration timings, so we can collectively get to an agreement on what is best for the patients’ outcome.
These results are clinically significant to the existing literature, as they demonstrate a decrease in the need for blood transfusions and faster postoperative recovery, as indicated by our study. The postoperative initiation of patient mobilization was also highlighted in our study, supporting another key benefit of TXA use, as patients in the TXA group mobilized approximately 4.7 hours earlier than those who did not receive TXA. Patient mobilization was carried out with the assistance of a physiotherapist and the use of a lumbar brace. Mobilization focused on walking while avoiding trunk flexion, extension, and rotational movements. Earlier mobilization is often overlooked but a critical factor in reducing risks of complications such as deep vein thrombosis or pulmonary embolism due to prolonged hospital stay. 3 Our study is the first to report that patients who received TXA were mobilized earlier.
Furthermore, we also presented the mean duration of surgery in the TXA group, which was 25 minutes less than in the non-TXA group. Reduced operative times equal to better use of hospital resources and lower surgical costs. Larson et al and Hui et al both researched the effect of TXA in spinal surgeries on the operative time and concluded in agreement with our study that TXA improves surgical efficiency by decreasing the mean operative time.22,23 While Larson et al 22 focused mainly on the general benefits of TXA, our study adds to theirs by also addressing a high-risk population. Hatter et al 12 did not find any significant differences in mean operative time, which is most probably due to the fact that TXA is mostly utilized in more complex surgeries compared to non-TXA surgeries, which can influence the consistency of this specific outcome.
It should be stated that our study has some limitations, including: (1) a single-center study, (2) the surgeries were performed by a specific surgical group, (3) a relatively small sample size, (4) the lack of randomization and (5) deficiency in the recording of American Society of Anesthesiologists (ASA) scores and Enhanced Recovery After Surgery (ERAS) parameters. It is also worth noting that we did not study the risk of potential venous thrombosis in the two groups, which is another limitation of our study. Further research should focus on prospective, multicenter studies to investigate the potential role of TXA in elderly patients with spinal stenosis at two consecutive levels undergoing posterolateral lumbar instrumented fusion and decompression. Additionally, results from multiple surgical teams would be particularly valuable. Suggestion for a pragmatic randomized controlled trial (RCT) or propensity-matched, multicenter cohort with standardized transfusion and ERAS protocols to validate these findings. Nevertheless, the results of our study can safely conclude that the use of TXA has a significant impact on the outcome in these elderly patients and should be considered more.
Supplemental Material
Supplemental material - Tranexamic Acid in Posterolateral Lumbar Instrumented Fusion for Central Spinal Stenosis: A Clinical Study
Supplemental material for Tranexamic Acid in Posterolateral Lumbar Instrumented Fusion for Central Spinal Stenosis: A Clinical Study by Stylianos Kapetanakis, Mikail Chatzivasiliadis, Georgios Charitoudis, Nikolaos Gkantsinikoudis, Christos Cholevas, Constantinos Chaniotakis in Global Spine Journal.
Supplemental Material
Supplemental material - Tranexamic Acid in Posterolateral Lumbar Instrumented Fusion for Central Spinal Stenosis: A Clinical Study
Supplemental material for Tranexamic Acid in Posterolateral Lumbar Instrumented Fusion for Central Spinal Stenosis: A Clinical Study by Stylianos Kapetanakis, Mikail Chatzivasiliadis, Georgios Charitoudis, Nikolaos Gkantsinikoudis, Christos Cholevas, Constantinos Chaniotakis in Global Spine Journal.
Footnotes
Ethical Considerations
All patients provided us with written consent to participate in the study after being informed about its purpose. The study protocol was reviewed and approved by the Institutional Review Board of the Interbalkan European Medical Center in Thessaloniki, Greece (Approval Number: 1712/13.04.2022).
Consent to Participate
This study refers to patients who are a subgroup of total patients of this protocol on involved hospital. All procedures were conducted in full compliance with the Ethical Principles for Medical Research Involving Human Subjects, as established in the 1964 Declaration of Helsinki and its subsequent amendments, including the 2013 revision.
Author Contributions
Conceptualization: S.K., M.C., C.C.; Methodology: S.K., M.C., G.C., N.G., C.C., C.C.; Statistical analysis: G.C., C.C.; Investigation: S.K., M.C., G.C., N.G., C.C., C.C.; Data curation: S.K., M.C., G.C., N.G., C.C.; Writing- original draft preparation: S.K., M.C., C.C,; Writing-review and editing: S.K., M.C., C.C.; Visualization: S.K., M.C., G.C., N.G., C.C, C.C.; Supervision: S.K., C.C. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that supports the findings of this study are available from the corresponding author, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.