
Abstract
Study Design
Prospective Cohort Study.
Objectives
The rapidly evolving landscape of cancer care alters the prognostic accuracy of established scoring systems for metastatic spinal tumors. This study aimed to provide a contemporary assessment of patient survival and examine the independent and complementary roles of the new Katagiri score (a systemic prognostic tool) and the Spinal Instability Neoplastic Score (SINS, a mechanical instability tool) in predicting 6-month mortality, laying a foundation for future combined prognostic model development.
Methods
We prospectively analyzed 151 patients with metastatic spinal tumors treated between 2021 and 2023. Demographic, clinical, and treatment data, including the new Katagiri score and SINS, were collected. The primary endpoint was 6-month mortality, which was evaluated using trend tests, correlation, and multivariate logistic regression.
Results
The 6-month mortality rate was 25.17%. Higher scores in both the new Katagiri score and the SINS were significantly associated with an increased risk of 6-month mortality. Notably, no significant correlation was observed between the total Katagiri score and the total SINS. Stratified analyses showed that prognostic factors for early mortality differed across new Katagiri score risk groups, with varying influences from specific Katagiri score items, SINS components, and spinal metastasis levels. SINS-related factors had a significant impact in the high-risk group.
Conclusions
The new Katagiri score and SINS independently predicted 6-month mortality in our cohort. Our findings suggest that considering both complementary measures may further refine prognostic assessment, providing a rationale for future prospective model development and validation.
Keywords
Introduction
Spinal metastasis is a major clinical problem, occurring in approximately 30% of cancer patients and often leading to severe pain, pathological fractures, and neurological complications.1,2 These complications greatly reduce a patient’s ability to perform daily activities, lower quality of life, and place a heavy burden on healthcare systems. 3 Managing spinal metastases therefore requires a team approach, with treatments such as radiation therapy, systemic drugs, and surgery chosen for each patient.4-6 To address this challenge, our institution started a multidisciplinary Bone Metastasis Cancer Board (BMCB) in 2021, where patients are registered prospectively to allow thorough evaluation and personalized treatment planning. A key part of this approach is accurately estimating life expectancy, which is critical for deciding which treatments are appropriate.
Predicting outcomes for patients with spinal metastases has often relied on scoring systems that combine various clinical and pathological factors.7,8 One widely used tool is the new Katagiri score, which estimates overall survival by evaluating systemic factors such as the type of primary cancer, the extent of disease in the organs and bones, and the patient’s general health. This score helps classify patients into broad risk groups. 9 Meanwhile, the Spinal Instability Neoplastic Score (SINS) was developed to assess a different, but equally important, aspect of spinal metastasis: the risk of mechanical instability.10,11 SINS focuses on local anatomical and biomechanical factors to guide decisions about spinal stabilization, helping to prevent pain and neurological problems caused by structural failure. Both scoring systems have been very useful in their own areas, but recent advances in cancer treatment have changed the situation dramatically. 12 The widespread use of targeted drugs and immune checkpoint inhibitors has greatly improved survival for some cancers, 13 changing the natural course of the disease and potentially reducing the accuracy of older prognostic models. This makes it important not only to update our survival data but also to rethink how we build and use predictive models.
An important but underexplored issue is how systemic prognosis and local mechanical instability interact. These two factors may influence each other; for example, rapidly progressing systemic disease could accelerate local bone destruction, while severe untreated spinal instability could lower a patient’s performance status and negatively affect survival prognosis. However, the exact relationship between a patient’s systemic disease burden, as measured by the new Katagiri score, and their risk of spinal structural failure, as measured by SINS, remains unclear. Investigating this relationship is a key step toward developing a more comprehensive prognostic model.
Determining the optimal prognostic threshold for surgical intervention is fundamental to clinical practice. While a life expectancy of less than 3 months has traditionally been a benchmark guiding decisions against major surgery, the universal applicability of this threshold is being re-evaluated in the era of modern systemic therapies that have improved survival outcomes. 14 Consequently, a prognosis of 6 months has emerged as a more pragmatic and clinically relevant threshold for guiding decisions on major surgical interventions, such as spinal separation or reconstruction surgery.15,16 This timeframe is considered more reasonable as it allows patients sufficient time to recover from the operation and experience a meaningful improvement in their quality of life, justifying the risks and costs associated with invasive procedures. Furthermore, the new Katagiri score itself was originally validated using 6-month survival as a key endpoint, 9 making this timepoint essential for assessing its contemporary performance and comparing it with the original data.
The primary goal of this study was to provide an up-to-date assessment of treatment outcomes and survival for patients with spinal metastases in the current era of cancer therapy. Specifically, we focused on 6-month survival as our primary endpoint, as this time frame represents a critical threshold for clinical decision-making regarding major surgical interventions in the modern therapeutic landscape. A secondary, more novel objective was to examine the relationship between the new Katagiri score and SINS. We hypothesized that these two scores might reflect different but complementary aspects of a patient’s overall risk. By exploring this hypothesis, we aimed to provide the basis for a combined, more reliable prognostic model that could give a more accurate prediction of survival and guide clinical decision-making for this challenging patient group.
Materials and Methods
Study Population and Design
This study was designed as a prospective observational study conducted at a single institution. To minimize selection bias, we implemented a systematic enrollment protocol. All patients with metastatic bone tumors referred to our orthopedic surgery department or discussed at our institution’s multidisciplinary Bone Metastasis Cancer Board (BMCB) between April 2021 and June 2023 were prospectively and consecutively enrolled in our institutional registry. This initial cohort consisted of 213 patients. The inclusion criteria for this specific analysis were patients with radiographically confirmed spinal metastases. The exclusion criteria were: (1) patients with metastatic bone disease that did not involve the spine (e.g., metastases confined to the extremities) (n = 49), and (2) loss to follow-up or inability to determine final outcomes (n = 13). After applying these criteria, a total of 151 patients were included in the final analysis. The study protocol was approved by our Institutional Review Board (IRB approval number 24010-02), and written informed consent was obtained from all participants prior to their enrollment.
Data Collection
Baseline demographic and clinical data were prospectively collected from our institutional database. These data included age, sex, and primary cancer type. We also recorded detailed information regarding treatments administered for metastatic spinal tumors, such as the use of surgery, radiation therapy, molecularly-targeted drugs, and bone modifying agents.
Clinical and Functional Assessments
The patient’s general functional condition was assessed at initial diagnosis and at the final follow-up using the Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) (Supplemental Table 1). 17 Neurological status was evaluated at the same time points using the Frankel classification system, 18 which grades the severity of spinal cord injury.
Prognostic and Stability Scoring Systems
Two established scoring systems were used to assess spinal stability and prognosis at enrollment. The Spinal Instability Neoplastic Score (SINS) evaluated the mechanical stability of the metastatic spine (Supplemental Table 2). 10 SINS includes six radiographic and clinical parameters: lesion location (cervical, thoracic, or lumbar), level of pain, type of bone lesion (lytic, mixed, or blastic), degree of spinal alignment deformity, extent of vertebral body collapse, and involvement of the posterolateral spinal elements. Total scores range from 0 to 18 and classify the spine as stable (0-6), potentially unstable (7-12), or unstable (13-18) (Supplemental Table 3). For patients with metastases at multiple spinal levels, the highest SINS score, representing the most unstable level, was used for analysis.
The new Katagiri score was utilized to estimate the patient’s overall survival prognosis (Supplemental Table 4). 9 This scoring system is composed of six distinct components: the type of primary cancer, the presence of visceral metastases, abnormalities in laboratory data, performance status, history of prior chemotherapy, and the presence of multiple skeletal metastases. The total score ranges from 0 to 10. Based on their total score, patients were stratified into 3 prognostic categories: low-risk (a score of 0-3), intermediate-risk (4-6), and high-risk (7-10) (Supplemental Table 5).
Outcome Measures
The primary outcome for this study was 6-month mortality, defined as death from any cause (i.e., all-cause mortality) within 6 months of patient enrollment. This endpoint was prospectively chosen because it represents a key decision-making threshold for surgical intervention in patients with spinal metastases, a rationale that is now explained in detail in the Introduction. Vital status at the final follow-up was determined through a systematic review of our institutional electronic health records. For patients whose status was not clear from the records, direct contact was made with the patient or their family via telephone to confirm their status. Secondary outcomes included 3-month mortality and the change in ECOG PS and Frankel grade from the initial assessment to the final follow-up, allowing for evaluation of functional and neurological preservation or deterioration over time.
Statistical Analysis
All statistical analyses were performed using JMP Pro 14 software (SAS Institute, Inc., Cary, NC, USA). A P-value of less than .05 was considered statistically significant. First, we tested the normality of all continuous variables using the Shapiro-Wilk test. Continuous variables are presented as the mean ± standard deviation (SD), and categorical variables are presented as counts (n) and percentages (%). To compare characteristics between two independent groups, appropriate statistical tests were used. For continuous variables, the Student’s t-test was applied to normally distributed data, while the Wilcoxon rank-sum test was used for data that were not normally distributed. For categorical variables, the chi-square test was used, and if any expected cell count was less than 5, Fisher’s exact test was applied instead. The Cochran-Armitage trend test was used to evaluate trends in the proportion of patients who died within 6 months across the ordered categories of the new Katagiri score and SINS. To identify independent predictors for 6-month mortality, a multivariate logistic regression analysis was performed. The final model included the new Katagiri score (as a continuous variable representing per 1-point increase), the SINS score (as a continuous variable representing per 1-point increase), serum albumin, the Prognostic Nutritional Index (PNI), and initial ECOG PS as covariates. Finally, we examined the relationship between the total SINS and the new Katagiri score. To assess a linear relationship between these two continuous variables, simple linear regression analysis was performed to derive the regression equation and the coefficient of determination (R2).
Results
Patient Demographics and Clinical Characteristics
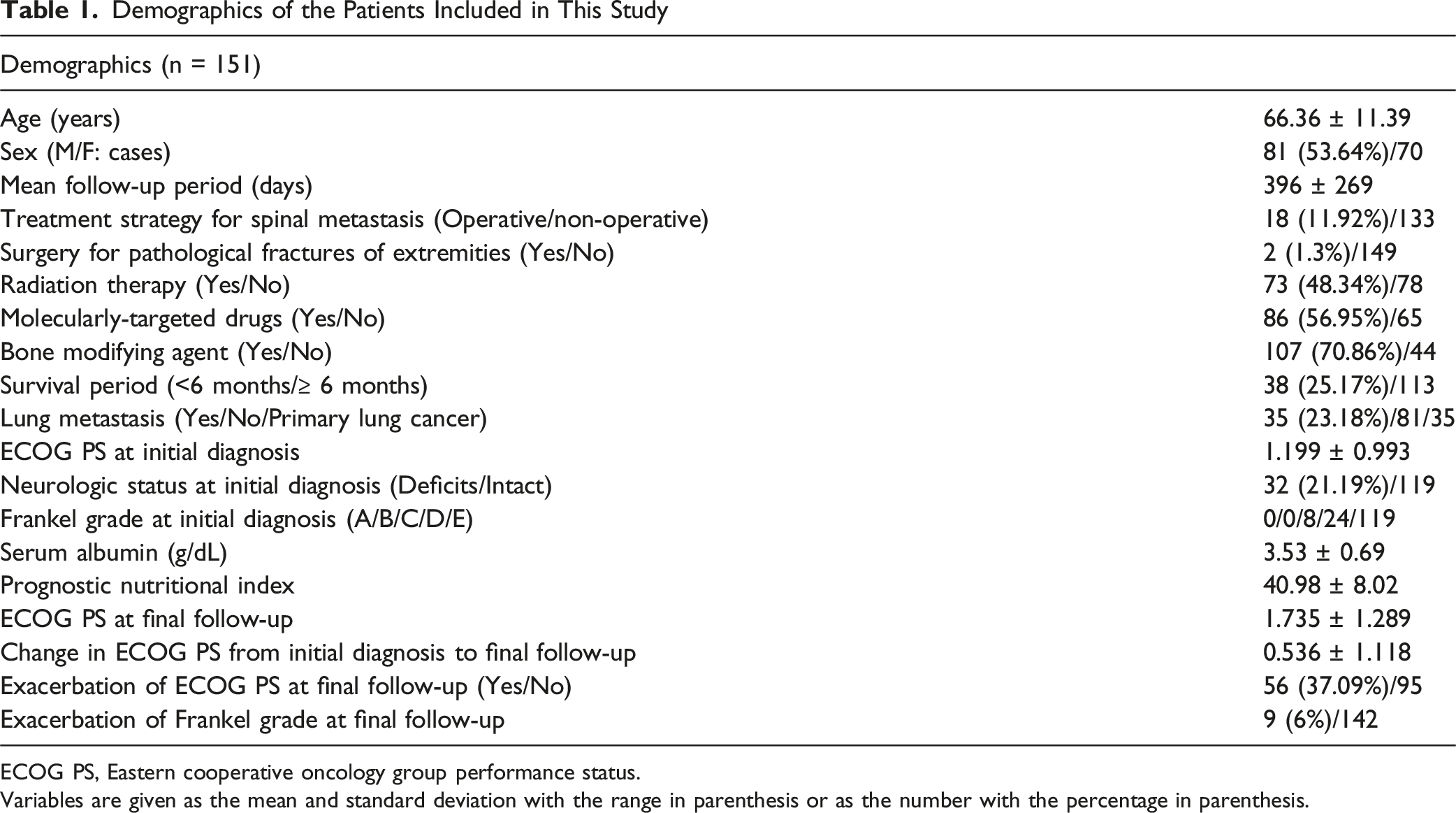
A total of 151 patients were included in this study. The mean age at enrollment was 66.36 ± 11.39 years. The cohort included 81 male patients (53.64%) and 70 female patients, with a mean follow-up of 396 ± 269 days. The most common primary cancers were lung cancer (n = 35), breast cancer (n = 20), and prostate cancer (n = 18), a distribution consistent with previous reports (Figure 1A).
19
Additionally, 35 patients (23.18%) had lung metastases from other primary sites. Thirty-eight patients (25.17%) died within 6 months of enrollment. Systemic and local treatments included radiation therapy (n = 73, 48.34%), molecularly-targeted drugs (n = 86, 56.95%), and bone-modifying agents (n = 107, 70.86%). Surgical treatment was performed for spinal metastases in 18 patients (11.92%) and for concomitant pathological fractures of the extremities in two patients (1.3%). At initial diagnosis, the mean Eastern Cooperative Oncology Group Performance Status (ECOG PS) was 1.199 ± 0.993. Thirty-two patients (21.19%) had neurological deficits, with a Frankel grade of C in 8 patients and D in 24 patients. The remaining 119 patients were neurologically intact (Frankel grade E), and no patients were classified as grade A or B. The mean serum albumin level was 3.53 g/dL, and the mean PNI was 40.98. At final follow-up, the mean ECOG PS had worsened to 1.735 ± 1.289, representing an average decline of 0.536 ± 1.118 from baseline. ECOG PS deterioration was observed in 56 patients (37.09%), and the Frankel grade worsened in nine patients (6%). All demographic and clinical characteristics are summarized in Table 1. Primary cancer sites of all patients included in the study (n = 151). (A) The chart shows the distribution of primary cancers in the entire cohort. Lung cancer (23.2%, n = 35) was the most common, followed by breast cancer (13.2%, n = 20) and prostate cancer (11.9%, n = 18). The remaining patients had other types of cancer Demographics of the Patients Included in This Study ECOG PS, Eastern cooperative oncology group performance status. Variables are given as the mean and standard deviation with the range in parenthesis or as the number with the percentage in parenthesis.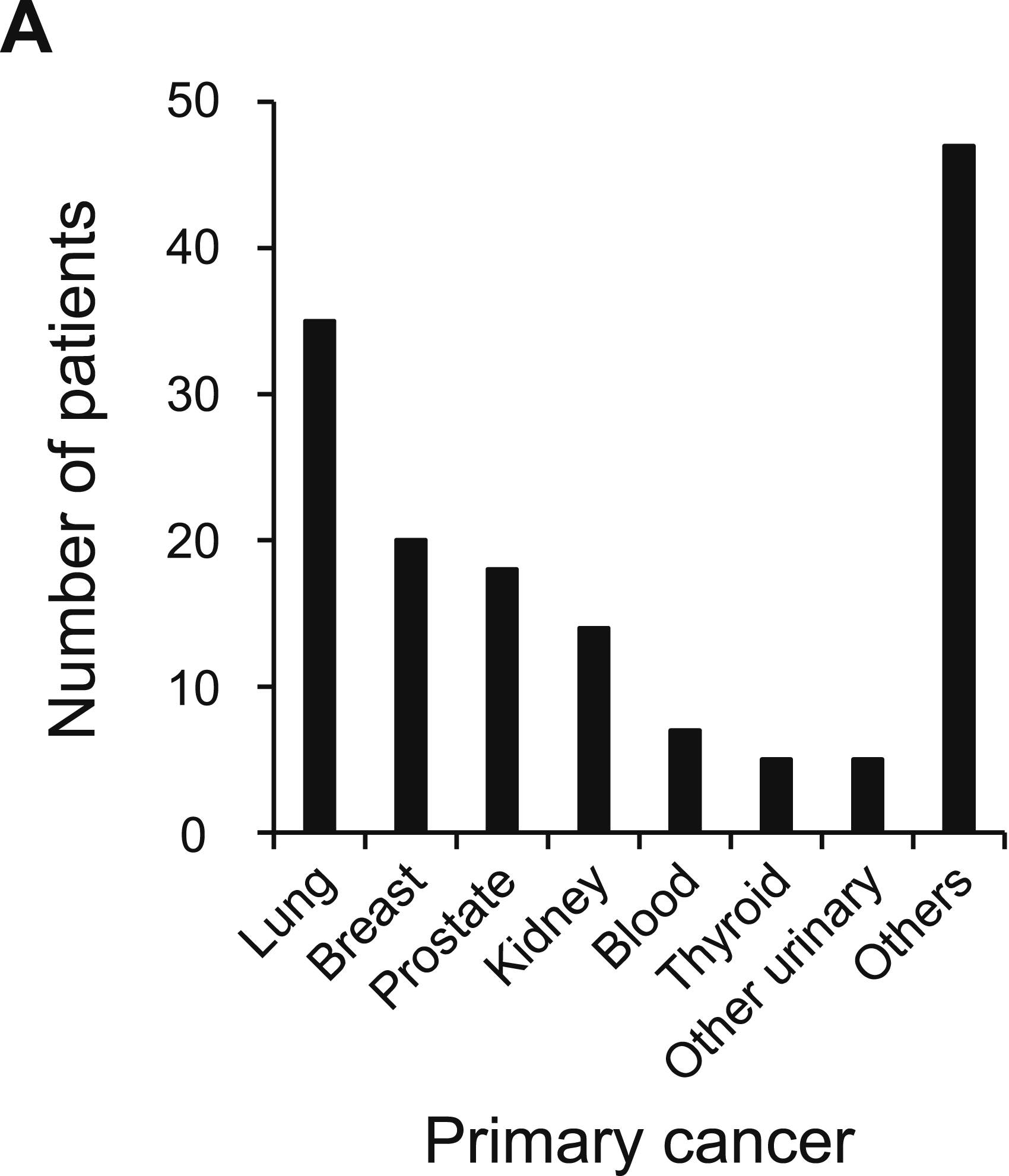
Prognostic Analysis of Survival Using Scoring Systems
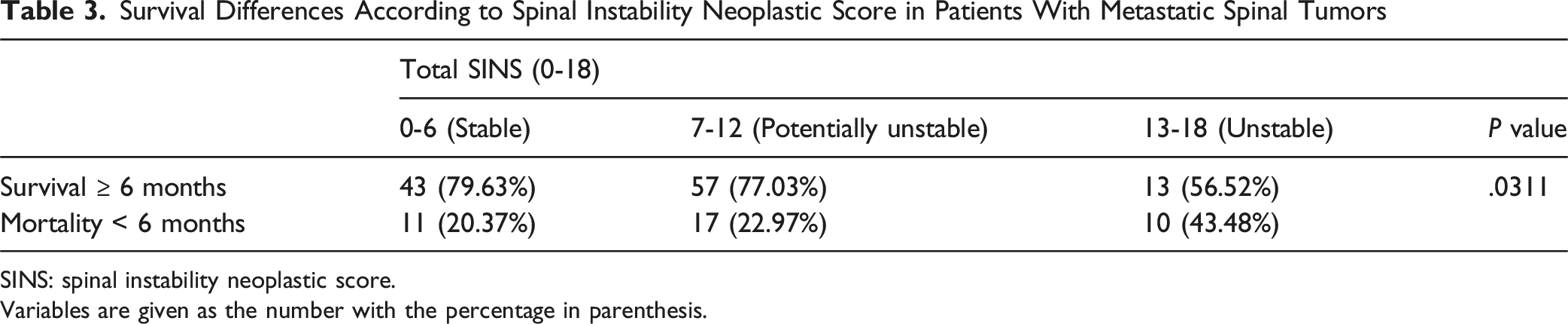
To analyze the prognosis of patients with metastatic spinal tumors, we first generated a Kaplan-Meier survival curve for the entire cohort (n = 151). The analysis showed that a quarter of the patients (25.17%, n = 38) died within 6 months of enrollment (Figure 2A). Next, we examined survival differences based on the new Katagiri score. A trend test confirmed that the proportion of patients who died within 6 months increased significantly with worsening risk category: low-risk (3.23%), intermediate-risk (21.25%), and high-risk (50%) (P < .0001) (Figure 2B, Table 2). We then assessed the relationship between SINS and survival. Although SINS primarily measures spinal instability and its association with survival prognosis is unclear, our analysis showed a significant trend: the rate of mortality within 6 months increased as the SINS category progressed from stable (20.37%), to potentially unstable (22.97%), and to unstable (43.48%) (P = .0311) (Figure 2C, Table 3). To further explore the utility of these scores in predicting shorter-term outcomes, we also analyzed survival at 3 months. A similar significant trend was observed. For the new Katagiri score, 3-month mortality was 0% in the low-risk group, 11.25% in the intermediate-risk group, and 30% in the high-risk group (P = .0002) (Supplemental Table 6). Likewise, for SINS, 3-month mortality rates were 7.41% for stable, 15.07% for potentially unstable, and 26.09% for unstable spines (P = .0297) (Supplemental Table 7). These findings confirm that both scoring systems are also effective in stratifying patients at risk for very early mortality. Kaplan-Meier survival curves. (A) Survival curve for the entire cohort (n = 151). Early mortality was notable, with 25.2% of patients (n = 38) dying within 6 months of enrollment. (B) Survival curves stratified by the new Katagiri score. Patients were divided into three prognostic groups: low-risk (score 0-3, n = 40), intermediate-risk (score 4-6, n = 80), and high-risk (score 7-10, n = 31). The curves show that a higher Katagiri score was associated with shorter survival. (C) Survival curves stratified by the Spinal Instability Neoplastic Score (SINS). Patients were classified as stable (SINS 0-6, n = 54), potentially unstable (SINS 7-12, n = 74), or unstable (SINS 13-18, n = 23). Survival probability decreased as SINS indicated greater instability. SINS: Spinal Instability Neoplastic Score Survival Differences According to Katagiri Prognostic Score in Patients With Metastatic Spinal Tumors Variables are given as the number with the percentage in parenthesis. Survival Differences According to Spinal Instability Neoplastic Score in Patients With Metastatic Spinal Tumors SINS: spinal instability neoplastic score. Variables are given as the number with the percentage in parenthesis.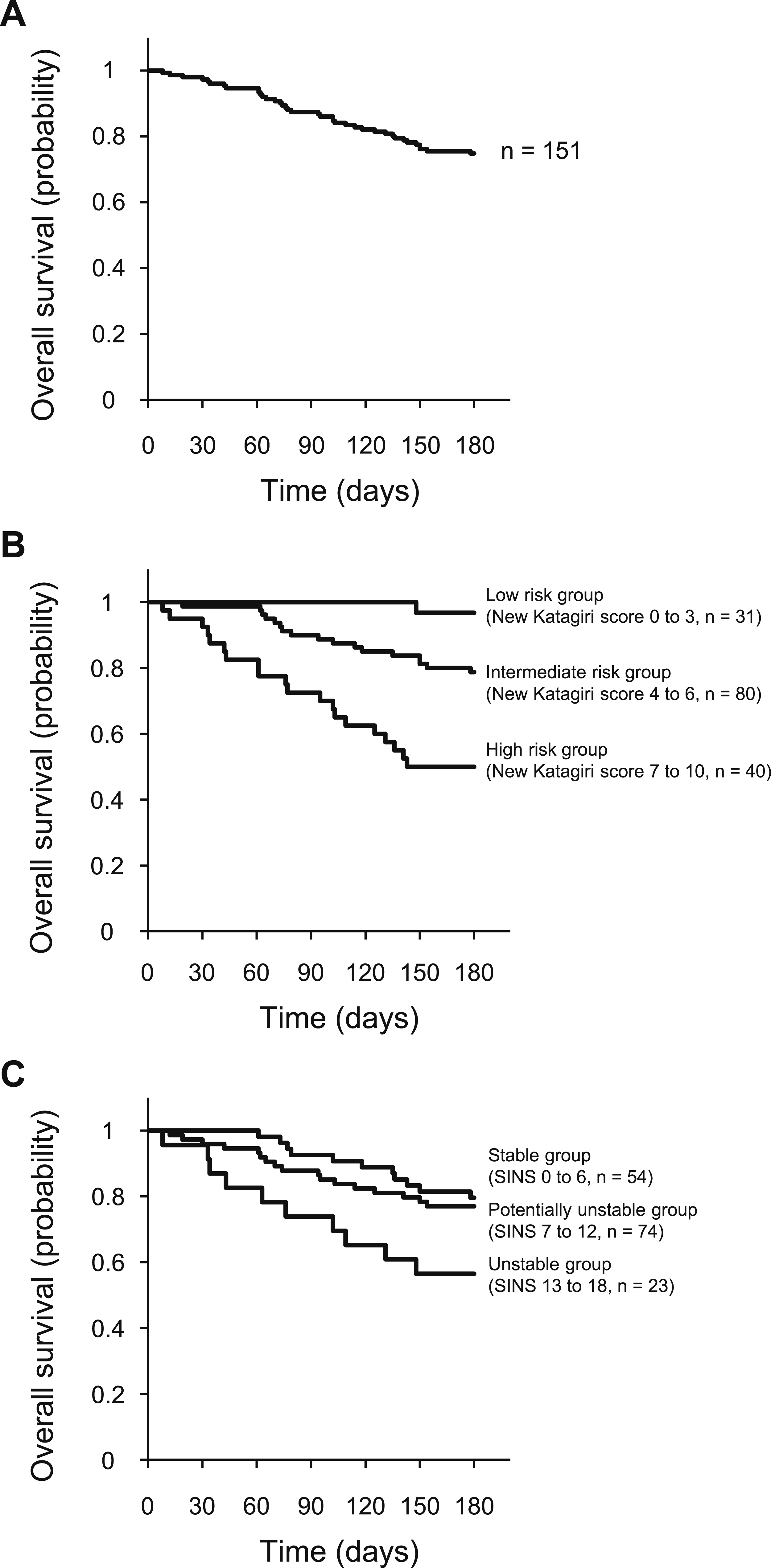

Independent Prognostic Value of the New Katagiri Score and SINS
Multivariate Logistic Regression Analysis for Predictors of 6-Month Mortality
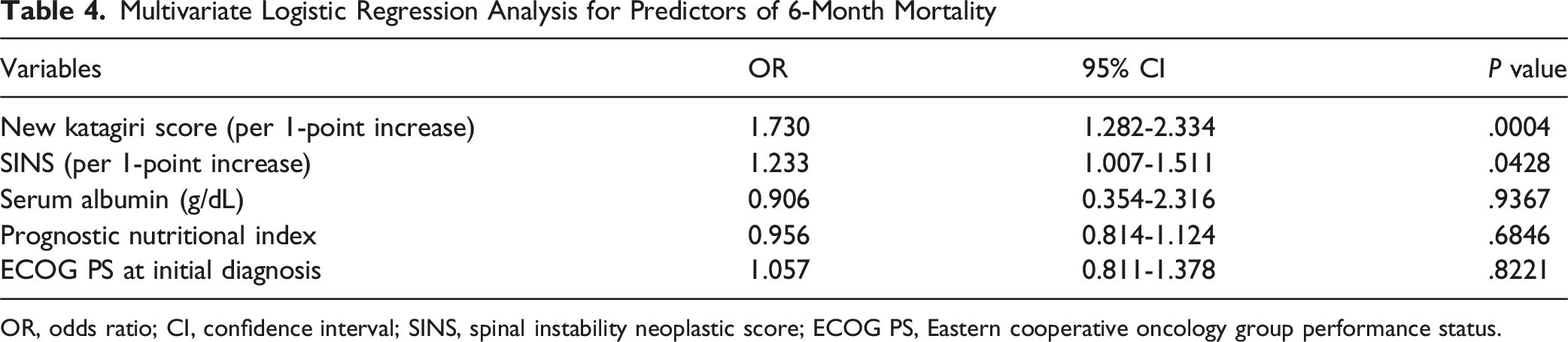
OR, odds ratio; CI, confidence interval; SINS, spinal instability neoplastic score; ECOG PS, Eastern cooperative oncology group performance status.
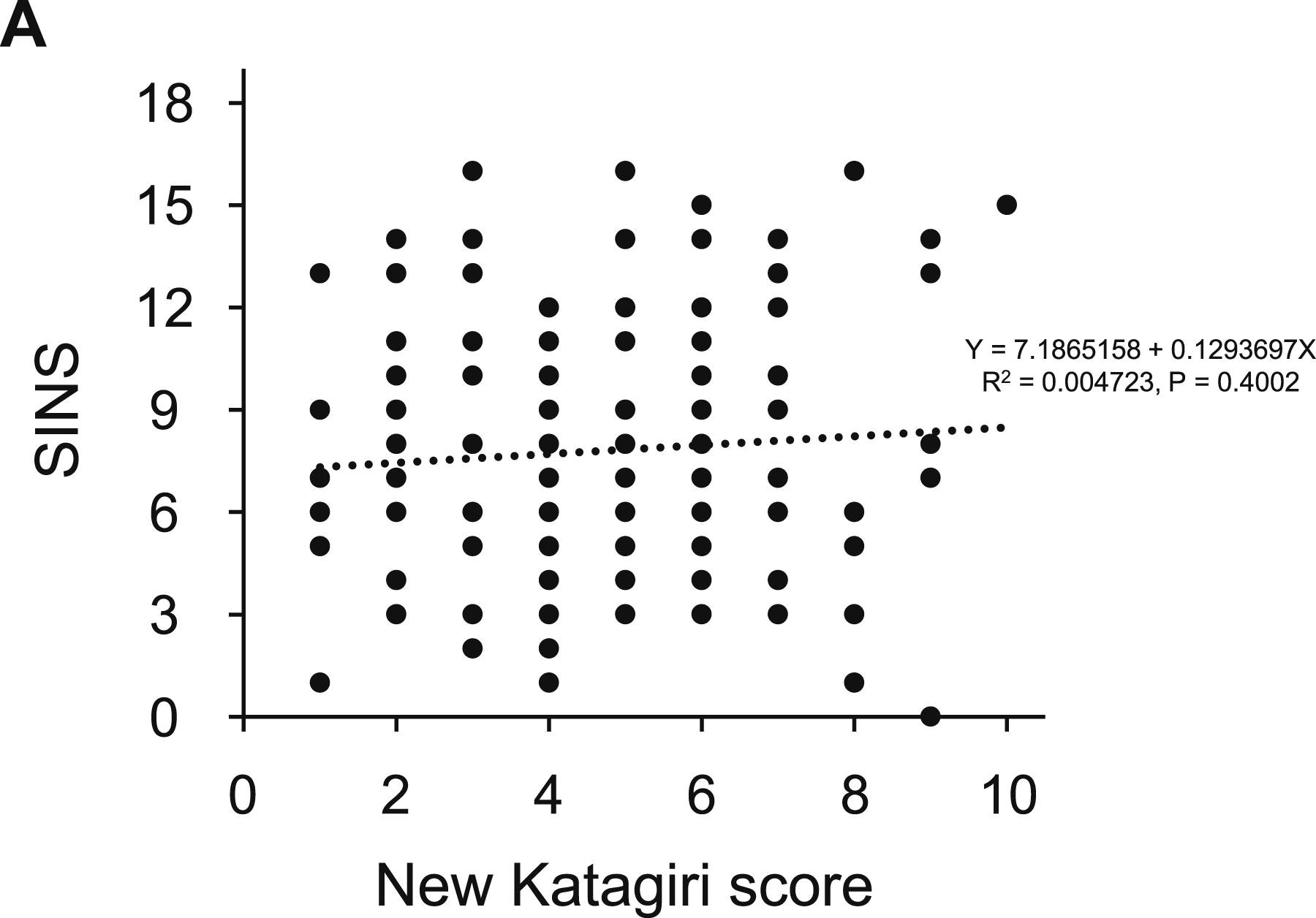
Correlation analysis between the Spinal Instability Neoplastic Score (SINS) and the new Katagiri score. (A) This scatter plot shows the relationship between total SINS (assessing mechanical instability) and the new Katagiri score (assessing survival prognosis). Linear regression analysis showed no significant correlation between the 2 scores, indicating that spinal instability and overall survival prognosis are independent factors in this patient population (Y = 7.1865158 + 0.1293697X, R2 = 0.004723, P = .4002)
Refining the Prognostic Value of the New Katagiri Score
Categorization in Groups Divided by 6-Month Life Expectancy According to SINS and New Katagiri Score (n = 151)
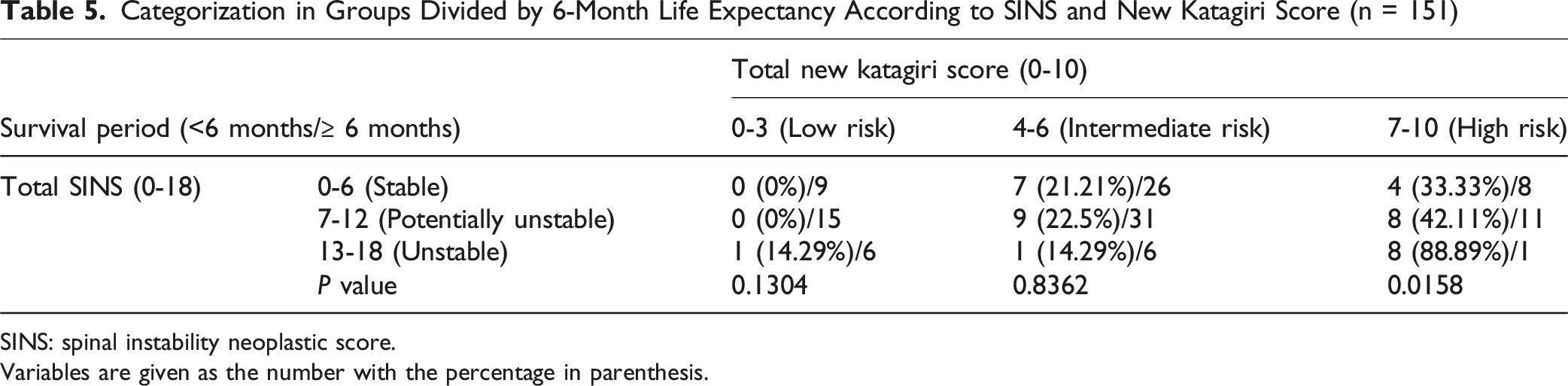
SINS: spinal instability neoplastic score.
Variables are given as the number with the percentage in parenthesis.
Differences in Demographics Between Mortality < 6 months Group and Survival ≥ 6 months Group, Classified as High Risk of the New Katagiri Score (n = 40)
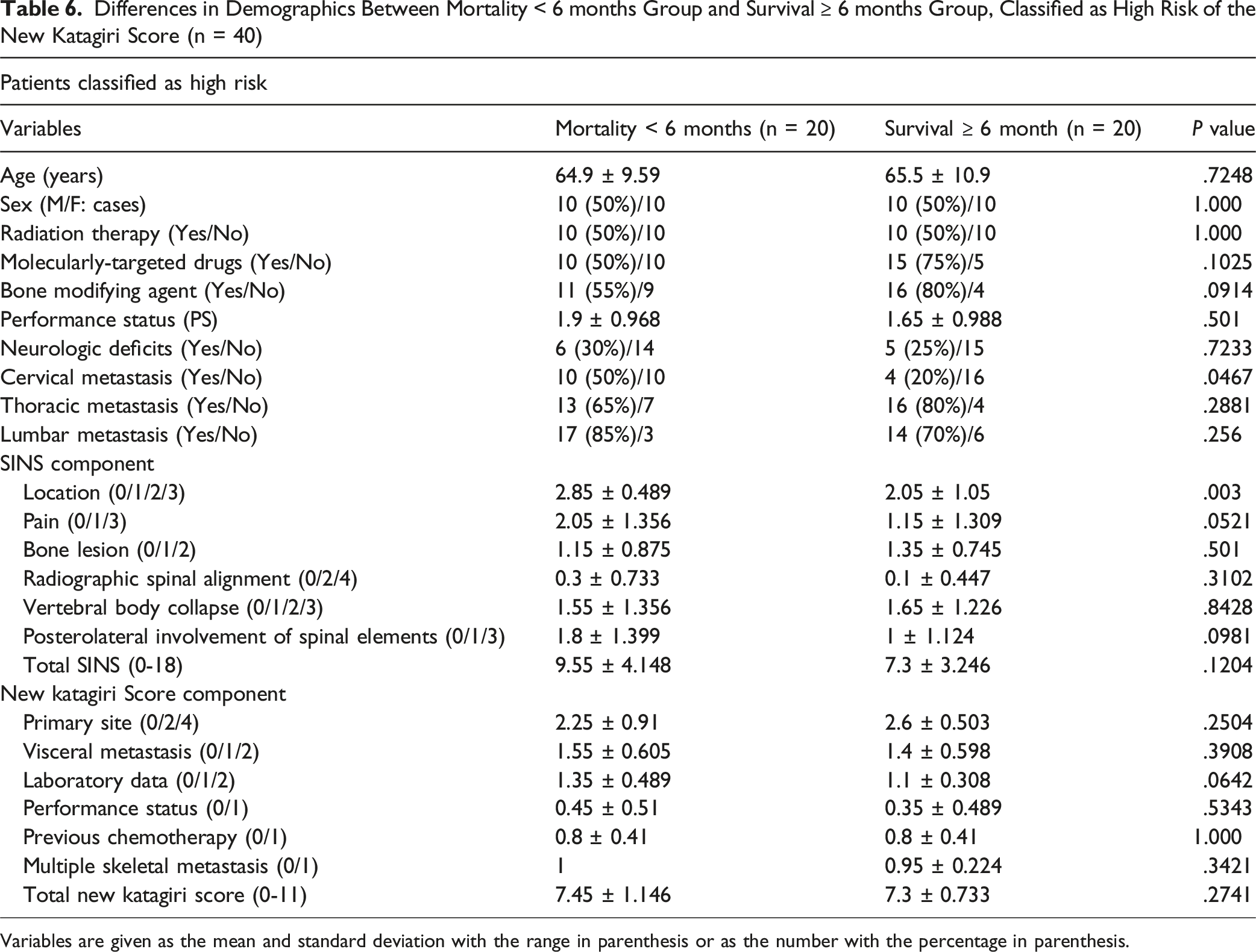
Variables are given as the mean and standard deviation with the range in parenthesis or as the number with the percentage in parenthesis.
Analysis of Surgical Intervention and Clinical Outcomes
Demographic Difference Between Operative and Non-Operative Groups
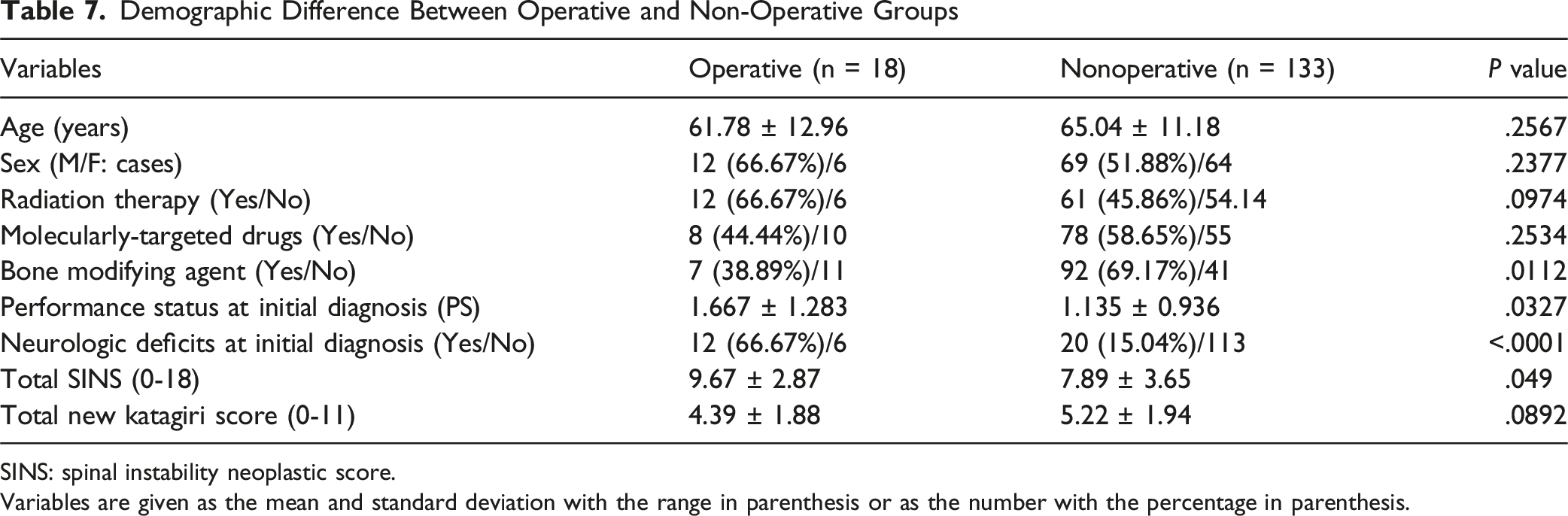
SINS: spinal instability neoplastic score.
Variables are given as the mean and standard deviation with the range in parenthesis or as the number with the percentage in parenthesis.
Clinical Outcomes in Operative and Nonoperative Groups
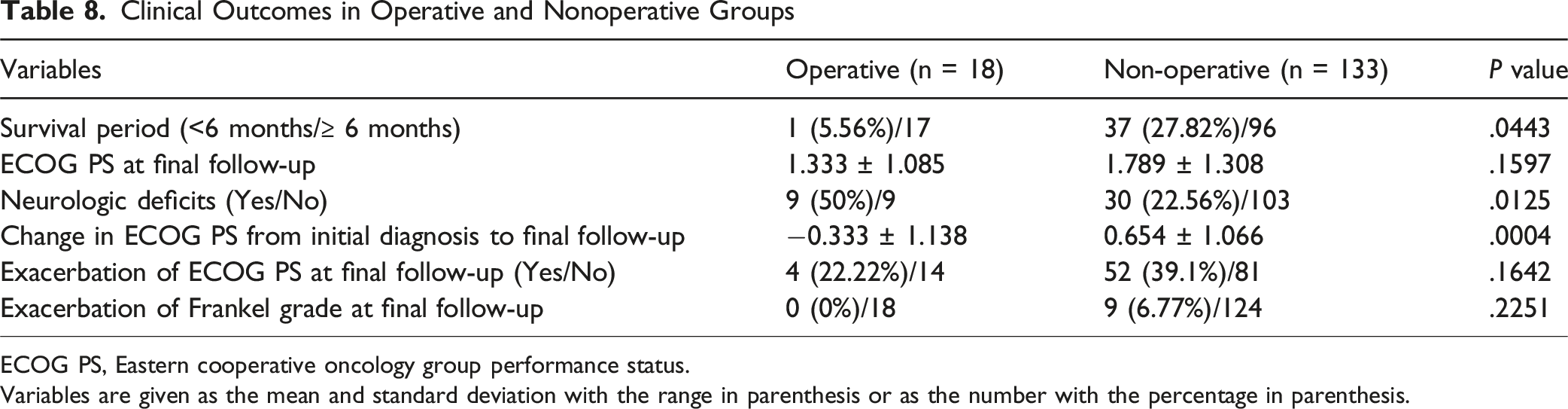
ECOG PS, Eastern cooperative oncology group performance status.
Variables are given as the mean and standard deviation with the range in parenthesis or as the number with the percentage in parenthesis.
Discussion
This study provides an updated view of the prognosis for patients with metastatic spinal tumors in the era of modern systemic therapies. Our main findings show that established scoring systems, such as the new Katagiri score and SINS, remain useful, but their predictive accuracy and the way they interact offer important insights. We found that one-quarter of patients still die within 6 months, yet survival has significantly improved for some patients who were previously considered to have the worst prognosis.
A key finding of our study, consistent with the original report by Katagiri et al., is that a higher new Katagiri score is clearly linked to poorer 6-month survival, confirming its continued value as a prognostic tool. 20 However, we observed a notable difference in the high-risk group. In our cohort, the 6-month survival rate for high-risk patients was 50.0%, almost double the 26.9% reported in the original 2014 study. 9 This marked improvement in survival among the most severe cases suggests that the natural course of advanced cancer is changing. This change is likely due to major advances in systemic cancer therapies over the past decade.21,22 The widespread use of molecularly-targeted drugs and immunotherapies, which were less common when the Katagiri score was first developed, 23 has significantly improved outcomes for many cancers. As a result, prognostic models created in earlier treatment eras may no longer reflect current patient outcomes accurately, highlighting the need for regular updates and re-evaluation.
Another important finding was the significant association between SINS and 6-month survival. This indicates that severe spinal instability, reflected by a high SINS score, may lead to a poorer prognosis. This could result from an increased risk of neurological deficits, which then reduces performance status and limits options for further treatment. Our results are consistent with previous research, such as the study by Oliveira et al., which found a correlation between SINS and the Tokuhashi score, another commonly used prognostic tool. 24 These findings support the idea that local biomechanical factors not only affect quality of life but also have a clear impact on early survival.
The lack of correlation between the new Katagiri score and SINS, coupled with their independent predictive power for 6-month mortality, reveals a critical distinction in the assessment of patients with spinal metastases. The new Katagiri score effectively quantifies systemic disease burden, reflecting the aggressiveness of the primary tumor, presence of visceral metastases, and overall physiological reserve. In contrast, SINS precisely evaluates the localized mechanical integrity of the spine, focusing on the risk of structural failure and its immediate sequelae. These distinct yet equally vital aspects underscore why the scores do not correlate; they measure fundamentally different, though ultimately interconnected, threats to a patient’s well-being and early survival. This independence has profound pathophysiological and clinical implications for 6-month mortality prediction. While systemic factors dictate the overall trajectory of the cancer, local spinal instability can catastrophically accelerate decline, particularly in patients already struggling with advanced disease. For instance, in individuals with a high Katagiri score (indicating a poor systemic prognosis), high SINS scores—especially those involving the cervical spine—can lead to severe pain, neurological deficits (e.g., upper and lower extremity paralysis), and a precipitous decline in activities of daily living (ADL). This loss of ambulation and self-care capacity can rapidly result in a deterioration of general physical condition and reduced mobility during the clinical course. 25 Such overall functional decline, potentially compounded by nutritional compromise, could critically limit further systemic treatment options and hasten 6-month mortality. Even if baseline performance status or nutritional markers were not independently significant predictors in the overall multivariate model, their rapid decline during the course of illness due to uncontrolled local issues is a plausible mechanism for poor outcomes. 26 Our subgroup analysis within the Katagiri high-risk group further supports this interaction: while Katagiri components themselves did not differentiate survival within this group, cervical spine metastasis and the SINS “location” component emerged as significant factors for early mortality (Table 6). This demonstrates that local mechanical issues can become critical drivers of 6-month mortality in systemically vulnerable patients, highlighting the necessity of assessing both systemic and local factors. These findings underscore that the independent assessment of both systemic disease burden and local mechanical instability is crucial for comprehensive prognostic evaluation. Our stratified analysis, particularly within the high-risk Katagiri group, showed that SINS was able to further distinguish patient outcomes. For example, patients with both a high-risk Katagiri score and an ‘unstable’ SINS classification demonstrated an exceptionally high 6-month mortality rate of 88.9% (Table 5). This provides compelling evidence that integrating these two complementary scores holds significant promise for developing a more precise and reliable prognostic model, offering improved risk stratification compared to using either score alone. Looking ahead, emerging technologies such as artificial intelligence may further enhance the development of such prognostic tools by integrating complex clinical, imaging, and molecular data.27,28 Based on the results of this study, factors such as the site of metastasis (including the presence of cervical spine involvement), the type of primary cancer, and abnormalities in laboratory data may carry considerable weight as prognostic predictors in future integrated models.
The improving prognosis and the observed benefits of surgery suggest that the indications for operative treatment of spinal metastases may be broader than previously thought. 29 Even patients with a very short life expectancy of less than 3 months can still benefit from surgery, experiencing improvements in pain, quality of life, and overall satisfaction, 30 showing that surgery should not be automatically ruled out in these cases. However, expanding surgical indications requires timely and accurate patient assessment. In this context, a multidisciplinary BMCB plays a key role. Implementing a BMCB can help identify patients at risk of paralysis or worsening performance status early. 31 Early surgical intervention, before irreversible neurological damage occurs, is critical for better outcomes, and our proposed integrated scoring model could serve as a useful tool to guide decision-making within the multidisciplinary review board.
This study has several limitations. First, there is an inherent selection bias in comparing the operative and nonoperative groups, because the decision to perform surgery depends on complex clinical judgments that cannot be fully reflected by the scoring systems. Second, the cohort included a wide variety of primary cancer types, introducing heterogeneity, and the sample size was too small to allow robust subgroup analyses for each individual cancer type. Finally, our primary prognostic endpoint was limited to a 6-month cutoff. Examining survival at other time points, such as 3 months or 1 year,32,33 could provide a more complete picture of prognosis. Although the present study demonstrated that the new Katagiri score and SINS independently contributed to prognostic stratification without mutual correlation, we did not construct or statistically validate a combined predictive model. Therefore, the implication that combining the two systems could improve predictive accuracy should be interpreted as a hypothesis rather than a conclusion. Our findings indicate only that systemic disease burden and mechanical instability provide complementary prognostic information for estimating 6-month survival. Future studies with prospective cohorts and formal model-development methodologies will be required to determine whether integrating these scoring systems can yield a clinically applicable prognostic tool.
Conclusion
The prognosis for patients with metastatic spinal tumors is evolving, especially with the introduction of modern systemic therapies. Our findings show that surgery can provide meaningful functional and neurological benefits, suggesting that more patients may be candidates for surgical treatment. The new Katagiri score and SINS each contributed independently to estimating 6-month survival in patients with spinal metastases. Although we did not validate a combined predictive model, our results suggest that considering both systemic prognosis and mechanical instability may be helpful in clinical decision-making. Further research is needed to explore whether integrating these scoring systems can support the development of an improved prognostic framework.
Supplemental Material
Supplemental Material - Updating Prognostic Assessment for Spinal Metastases With a Combined Model of the Spinal Instability Neoplastic Score and the New Katagiri Score
Supplemental Material for Updating Prognostic Assessment for Spinal Metastases With a Combined Model of the Spinal Instability Neoplastic Score and the New Katagiri Score by Kazuya Yokota, MD, PhD, Yuzo Kugimoto, MD, Kiyoshi Tarukado, MD, PhD, Kazu Kobayakawa, MD, PhD, Hirokazu Saiwai, MD, PhD, Kenichi Kawaguchi, MD, PhD, Makoto Endo, MD, PhD, Toshifumi Fujiwara, MD, PhD, Akira Nabeshima, MD, PhD, Nobuhiko Yokoyama, MD, PhD, Yasuharu Nakashima in Global Spine Journal
Footnotes
Ethical Consideration
This study was conducted in accordance with institutional ethical standards and was approved by the appropriate ethics committee (IRB approval number 24010-02).
Consent to Participate
Written informed consent was obtained from all participants prior to enrollment.
Author Contributions
Conception and design: Kazuya Yokota.
Acquisition of data: Kazuya Yokota, Yuzo Kugimoto, Kiyoshi Tarukado, Kazu Kobayakawa, Hirokazu Saiwai, Kenichi Kawaguchi, Makoto Endo, Toshifumi Fujiwara, Akira Nabeshima, and Nobuhiko Yokoyama.
Interpretation of data: Kazuya Yokota.
Study supervision: Yasuharu Nakashima.
Drafting of the manuscript: Kazuya Yokota.
Critical revision of the manuscript: Kazuya Yokota.
The final version of the manuscript has been approved by all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Japan Society for the Promotion of Science (Grant Number: JP21K16671, awarded to Dr Kazuya Yokota); the General Insurance Association of Japan (awarded to Dr Kazuya Yokota); Nakatomi Foundation (awarded to Dr Kazuya Yokota); NSK Nakanishi Foundation (awarded to Dr Kazuya Yokota); and ZENKYOREN (National Mutual Insurance Federation of Agricultural Cooperatives) (awarded to Dr Kazuya Yokota). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request. Due to privacy or ethical restrictions, the data are not publicly available but may be shared for academic purposes.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.