
Abstract
Objective
To investigate the clinical significance of alpha-fetoprotein and carbohydrate antigen 19-9 as potential predictors of outcomes in patients with acute liver failure.
Methods
We conducted a retrospective analysis of 208 patients with acute liver failure admitted to the intensive care unit between 2009 and 2023. Serum alpha-fetoprotein and carbohydrate antigen 19-9 levels were measured on Days 1 and 3, and their prognostic value was evaluated using logistic regression and receiver operating characteristic curve analyses. Patients were stratified by etiologies to assess biomarker performance across different causes of acute liver failure.
Results
Nonsurvivors had significantly lower alpha-fetoprotein levels and higher carbohydrate antigen 19-9 levels than survivors on Days 1 and 3 (all p < 0.05). Alpha-fetoprotein levels increased over time in both groups, whereas carbohydrate antigen 19-9 levels increased in nonsurvivors and decreased in survivors. The combination of carbohydrate antigen 19-9 with the Model for End-Stage Liver Disease score significantly improved prognostic accuracy, with an area under the curve value of 0.828, compared with 0.784 for alpha-fetoprotein combined with Model for End-Stage Liver Disease score. Etiology-specific analysis revealed that carbohydrate antigen 19-9 showed the best predictive performance in acetaminophen-induced acute liver failure (area under the curve value = 0.885), whereas alpha-fetoprotein showed better predictive performance in viral hepatitis-associated acute liver failure (area under the curve value = 0.880).
Conclusions
Alpha-fetoprotein is a protective prognostic factor, whereas carbohydrate antigen 19-9 enhances outcome prediction, particularly when combined with Model for End-Stage Liver Disease score. Etiology-specific biomarker performance supports tailored prognostic approaches in the management of acute liver failure.
Keywords
Introduction
Acute liver failure (ALF) is a life-threatening condition characterized by rapid and extensive hepatocyte death. The primary manifestations of ALF include prolonged international normalized prothrombin time ratios and hepatic encephalopathy (HE). Although the mortality rate has improved over the past few decades,1–2 only approximately 40% of patients with ALF can recover without liver transplantation. 3 Predicting outcomes for patients with ALF using current prognostic models remains challenging. Consequently, physicians have long sought a singular biomarker that could effectively predict the prognosis of patients with ALF.
Numerous prognostic models have been proposed over the years, including the well-known King’s College Criteria, Model for End-Stage Liver Disease (MELD), and MELD combined with the serum sodium concentration (MELD-Na). However, these models often fail to accurately predict outcomes. In particular, these models cannot identify patients who are likely to die and may thus require transplantation. 4 To increase prognostic accuracy, researchers have aimed to identify a single biomarker that is uniquely associated with the onset and progression of liver failure.
Alpha-fetoprotein (AFP) is expressed at relatively high levels in the fetal liver, 5 and serum AFP levels are elevated in many adult patients with hepatocellular carcinoma and chronic hepatitis. 6 Following liver injury, elevated AFP levels appear to be associated with liver regeneration, 7 possibly due to the presence of immature hepatoblasts that exhibit characteristics similar to those of fetal hepatocytes. Recently, AFP has been utilized as a prognostic marker for patients with ALF, with high AFP levels tending to predict a favorable prognosis for these patients. 8 Similarly, carbohydrate antigen 19-9 (CA19-9) has been linked to increased hepatocyte turnover, as observed in patients with acute injury, chronic hepatitis, cirrhosis, extrahepatic jaundice, and cholangitis. Although AFP is a well-established prognostic marker in ALF, reflecting hepatocyte regeneration, the role of CA19-9—a tumor marker primarily associated with gastrointestinal malignancies—remains unexplored in ALF. ALF is characterized by a high incidence of hepatocellular necrosis and damage, which leads to the release of CA19-9 into the circulation. 9 Furthermore, as liver cells attempt to recover and regenerate, the levels of CA19-9 increase during cell proliferation and repair. 10 A case report by Sapmaz et al. indicated that markedly elevated serum CA19-9 levels may be observed in patients with benign liver diseases, such as autoimmune hepatitis. 11 Additionally, a recent study identified CA19-9 as a marker of nonmalignant hepatocytic ductal transformation in patients with ALF. 12
Previous research has highlighted the effectiveness of AFP in predicting outcomes for patients experiencing non-acetaminophen (APAP)-induced ALF, especially when AFP is utilized alongside established clinical scoring systems. 13 Conversely, CA19-9, a key marker of gastrointestinal tumors, plays a role in cell proliferation and repair but has not been extensively studied as a prognostic indicator for patients with ALF. We recorded the dynamic changes in AFP and CA19-9 levels over Days 1–3 and evaluated their combined use with the MELD score to improve prognostic accuracy. Additionally, we stratified patients by etiologies of ALF. We hypothesized that CA19-9, a potential marker of biliary injury, complements AFP in predicting ALF outcomes, offering a novel dual-biomarker approach for risk stratification tailored to specific etiologies.
Materials and methods
Study design and patients
This retrospective observational study enrolled 228 patients with ALF from January 2009 to March 2023 in the Department of Critical Care Medicine, the Fifth Medical Center, PLA General Hospital, Beijing, China. All patients met the diagnostic criteria for ALF, as outlined in the Guidelines for the Diagnosis and Treatment of Liver Failure (2024 Edition) established by the Chinese Medical Association. 14 Individuals aged <18 years; pregnant women; patients diagnosed with liver cancer or other malignant tumors in any organ; and those with severe underlying conditions, such as heart, lung, kidney, or blood diseases, were excluded from the study. Patients lacking data on serial (Days 1 and 3) serum AFP and CA19-9 levels were excluded. Finally, a total of 208 patients were included in the study analysis. The detailed statistics are presented in Figure 1. The final study cohort was divided into two groups based on 28-day mortality during hospitalization in the intensive care unit (ICU): survival group and nonsurvival group.

Flow diagram of the participants analyzed. AFP: alpha-fetoprotein; ALF: acute liver failure; CA19-9: carbohydrate antigen 19-9.
The Ethics Committee of the Fifth Medical Centre of PLA General Hospital (Beijing, China) granted exemption of ethics approval for this retrospective study (Approval Notice #KY-2024-10-163-1). This study was conducted in accordance with the Helsinki Declaration of 1975 as revised in 2024. All enrolled patients received etiological treatment and comprehensive medical therapy. The reporting of this study conforms to the REporting recommendations for tumor MARKer prognostic studies (REMARK) guidelines. 15
Data collection
In accordance with the research protocol, baseline characteristics and laboratory data were collected from the patients. All anonymized data were obtained and documented retrospectively via the hospital information system, ensuring complete protection of the patients’ personal details. All patient identifiers were removed prior to analysis. The baseline characteristics included age, sex, etiology, and adverse events. The laboratory indicators assessed in this study primarily included the serum levels of AFP and CA19-9. As our hospital specializes in liver disease treatment, blood tests for these indicators were performed on Days 1 and 3 after ICU admission. Furthermore, illness severity was evaluated via established scoring systems, namely, the MELD score and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score, both of which are critical for determining patient prognosis and guiding treatment decisions.
Statistical analyses
The normality of the data was evaluated via the Shapiro–Wilk method. Categorical variables were represented as counts (percentages), whereas continuous variables were presented as means (standard deviations) or medians (interquartile ranges). The variance ratio test (F test) was used to compare differences among categorical variables, and differences between continuous variables were assessed via the two-tailed Mann–Whitney test. To predict survival outcomes, we constructed logistic regression models that included serum levels of AFP and CA19-9 at ICU admission, MELD scores, and their combined effects. The results were reported as odds ratios (ORs) along with their corresponding 95% confidence intervals (CIs). Additionally, to assess the predictive power of various risk factors for prognosis, receiver operating characteristic (ROC) curves were generated, and the area under the curve (AUC) value was determined. An AUC value of ≥0.8 was considered to indicate very good predictive value, whereas an AUC value of 0.6–0.8 suggested a certain level of clinical application value. The Hosmer–Lemeshow test was conducted to verify the calibration of the model. All statistical analyses were performed via IBM© SPSS, where a p-value of <0.05 was considered to indicate statistical significance. The statistical code is available upon request.
Results
Baseline characteristics
A total of 208 patients met the inclusion criteria for ALF at the Fifth Medical Center of PLA Hospital from January 2009 to March 2023 (Figure 1). Among these patients, 30.3% (n = 63) survived, whereas 69.7% (n = 145) did not survive. As indicated in Table 1, the median age of all patients was 45.0 years. The median age of the survival group was 43.5 years, whereas that of the nonsurvival group was 45.0 years. The proportion of male patients in the final study cohort was 36.4%, with 25.7% in the survival group and 41.1% in the nonsurvival group. The proportion of male patients did not significantly differ between the two groups. Viral hepatitis was identified as the etiology in 43 (20.7%) patients, APAP poisoning in 67 (32.2%) patients, traditional Chinese medicine (TCM) use in 41 (19.7%) patients, alcoholic liver disease in 5 (2.4%) patients, unknown causes in 20 (9.6%) patients, and other causes in 34 (15.4%) patients. No significant differences were observed in common etiological factors, with the exception of unknown or other causes, between the two groups.
Patient demographics.
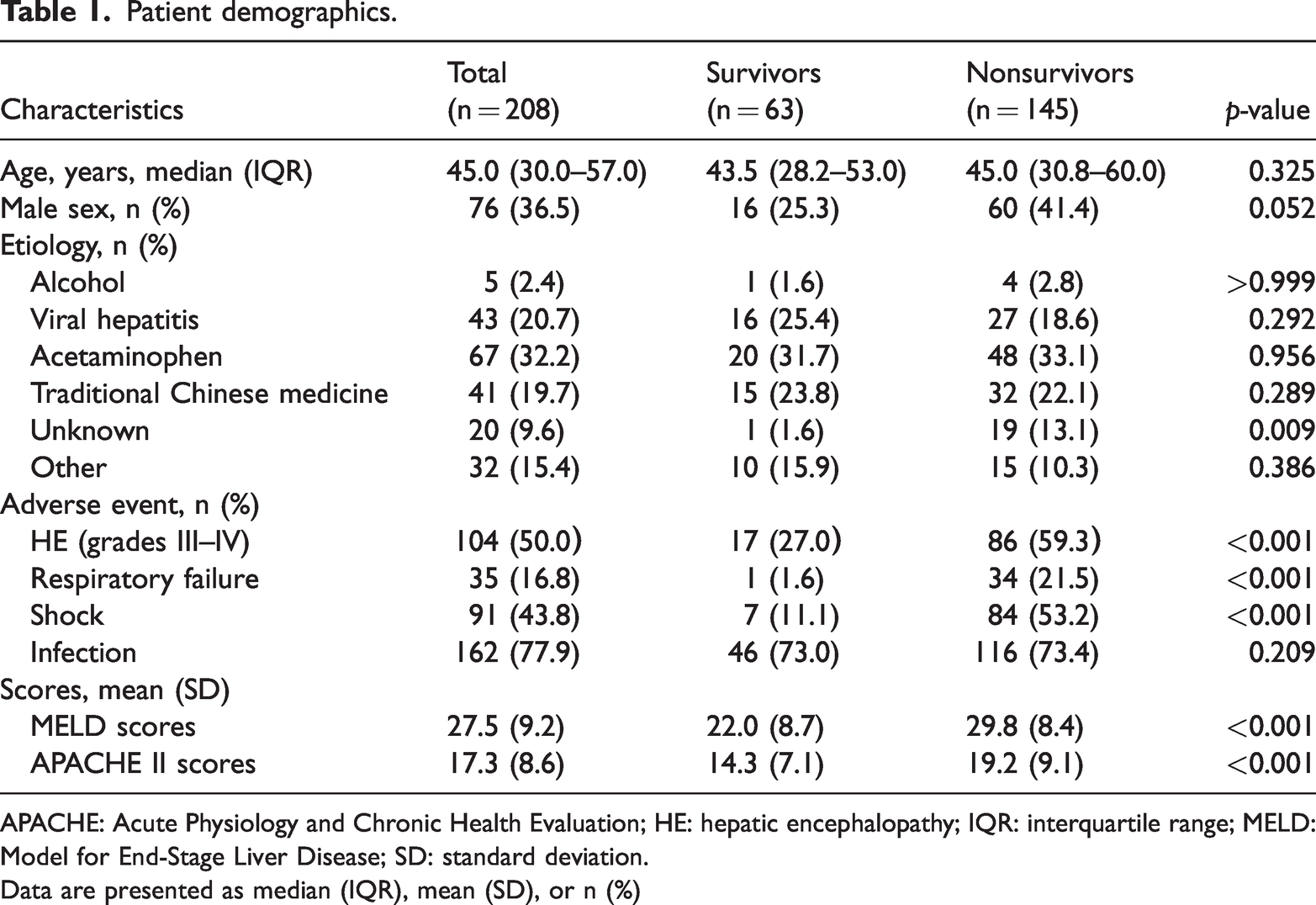
APACHE: Acute Physiology and Chronic Health Evaluation; HE: hepatic encephalopathy; IQR: interquartile range; MELD: Model for End-Stage Liver Disease; SD: standard deviation.
Data are presented as median (IQR), mean (SD), or n (%)
The adverse events considered in this study included HE, respiratory failure, shock, and infection. The proportion of patients with grades III–IV HE was significantly lower in the survival group than in the nonsurvival group (27.1% vs. 59.5%, p < 0.001). Similarly, the proportion of patients with respiratory failure was significantly lower in the survival group than in the nonsurvival group (1.6% vs. 21.5%, p < 0.001). A comparable trend was observed in the incidence of shock between the two groups (11.1% vs. 53.2%, p < 0.001). Moreover, the proportion of patients with infection did not significantly differ between the two groups (65.7% vs. 73.4%, p = 0.209). The survival group had significantly lower MELD scores than the nonsurvival group (22.0 ± 8.7 vs. 29.8 ± 8.4, p < 0.001). Furthermore, the APACHE II score was significantly lower in the survival group than in the nonsurvival group (14.3 ± 7.1 vs. 19.2 ± 9.1, p < 0.001).
Comparison of serum AFP and CA19-9 levels between the two groups
Figure 2 shows the serum AFP and CA19-9 levels on admission in both patient groups. Patients in the survival group had significantly higher AFP levels on admission (p = 0.03) (Figure 2(a)). In contrast, patients in the nonsurvival group had higher CA19-9 levels on admission (Figure 2(b)). The CA19-9 levels significantly differed between the survival and nonsurvival groups (p < 0.01). Figure 3 shows the dynamic changes in the serum AFP (Figure 3(a)) and CA19-9 (Figure 3(b)) levels on Days 1 and 3 following ICU admission in the two groups. The serum AFP levels in both groups tended to increase from Day 1 to Day 3. Furthermore, the serum CA19-9 levels tended to increase in the nonsurvival group over the same period, whereas a decreasing trend was observed in the survival group. Notably, the serum AFP levels in the survival group were significantly greater than those in the nonsurvival group on Days 1 and 3 (all p < 0.05) (Figure 3(a)). Conversely, the serum CA19-9 levels were significantly lower in the survival group than in the nonsurvival group on both Days 1 and 3 (all p < 0.01) (Figure 3(b)).

Analysis of AFP and CA199 levels at admission as predictors of outcomes in patients with ALF. (a) AFP levels at admission were significantly higher in the survival group (p = 0.03) and (b) CA199 levels at admission were significantly different between the survival and nonsurvival groups. The nonsurvival group had higher CA199 levels (p < 0.01). AFP: alpha-fetoprotein; CA19-9: carbohydrate antigen 19-9; ALF: acute liver failure.
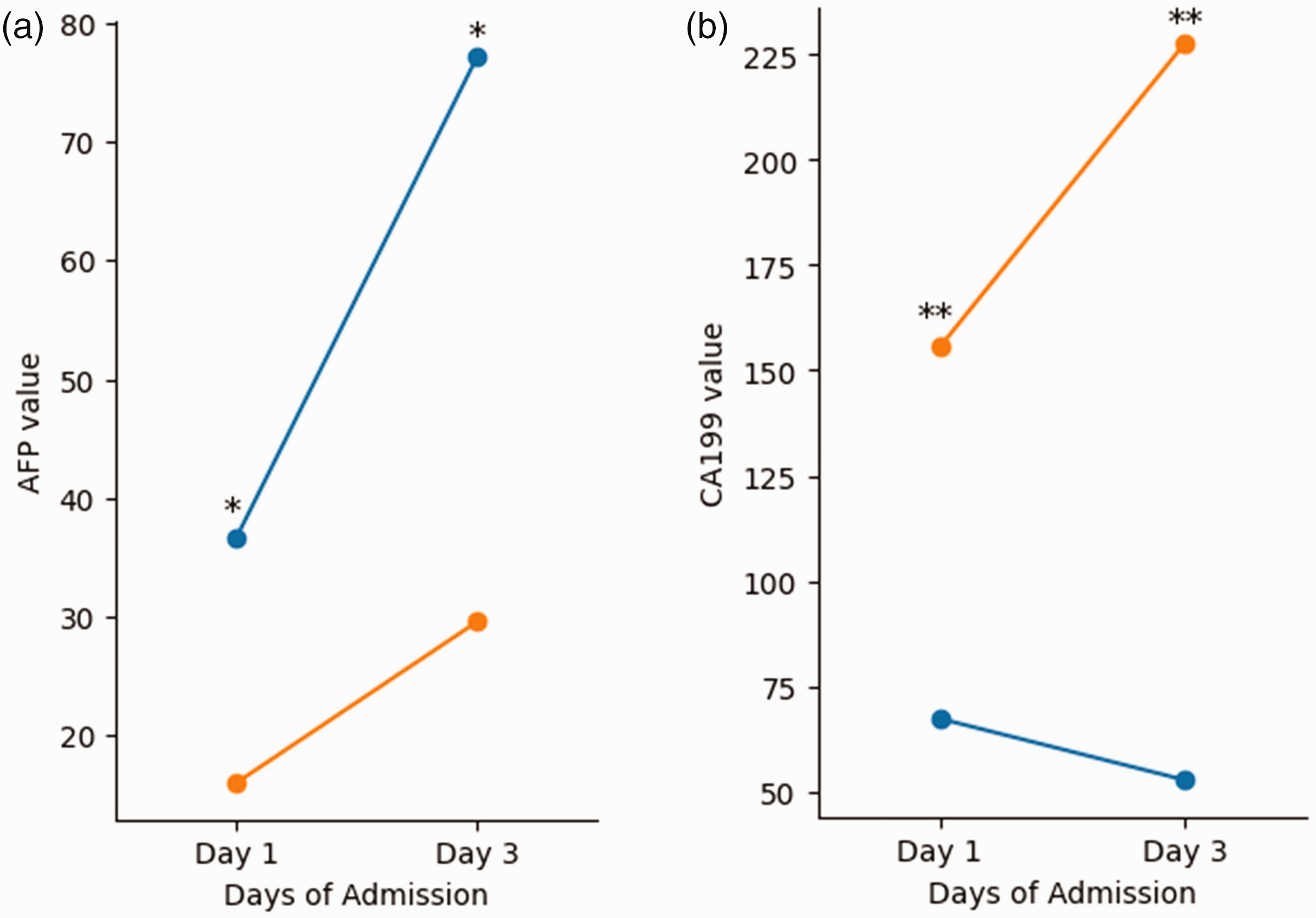
CA19-9 and AFP levels on Days 1 and 3 in the survival and nonsurvival groups. (a) Serum AFP levels and (b) serum CA19-9 levels. *p-value <0.05, **p-value <0.01. CA19-9: carbohydrate antigen 19-9; AFP: alpha-fetoprotein.
Associations between serum AFP levels at ICU admission, MELD scores, and outcomes
A multivariate logistic regression analysis was conducted to investigate the associations between serum AFP levels at ICU admission, MELD scores, and patient outcomes, as presented in Table 2. The results demonstrated that the serum AFP level, MELD score, and their combination were significantly associated with 28-day mortality (p = 0.002, p < 0.001, and p < 0.001, respectively). Additionally, the results of the ROC curve analysis revealed that the combination of serum AFP levels and MELD scores yielded an AUC value of 0.784 when used to predict patient prognosis, which was significantly greater than that of either measure used independently (Figure 4(a)). Specifically, the AUC value for the MELD score was 0.782, whereas that for the serum AFP level was 0.628. When evaluated individually, the serum AFP level demonstrated a sensitivity of 68.1% and a specificity of 55.4%, whereas the MELD score exhibited a sensitivity of 78.0% and a specificity of 67.7%. Notably, the combination of serum AFP level and MELD score showed improved sensitivity and specificity, reaching 83.0% and 68.6%, respectively (Table 3).
Multivariate logistic regression analysis of prognostic factors in acute liver failure.

OR: odds ratio; AFP: alpha-fetoprotein; CA19-9: carbohydrate antigen 19-9; MELD: Model for End-Stage Liver Disease; CI: confidence interval.

The ROC curve of serum AFP and CA19-9 levels at ICU admission, MELD scores, and their combination for predicting 28-day mortality. (a) Serum AFP levels, MELD scores, and their combination and (b) serum CA19-9 levels, MELD scores, and their combination. ROC: receiver operating characteristic; AFP: alpha-fetoprotein; CA19-9: carbohydrate antigen 19-9; MELD: Model for End-Stage Liver Disease.
Serum AFP levels at ICU admission and MELD scores for the prognostic prediction of patient outcomes.

AFP: alpha-fetoprotein; MELD: Model for End-Stage Liver Disease; AUC: area under the curve; CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value.
DeLong test was used to compare the AUC difference between the combined model and MELD alone.
Associations between serum CA19-9 levels at ICU admission, MELD scores, and outcomes
Table 2 also indicates a significant association between serum CA19-9 levels at ICU admission, MELD scores, and their combination with 28-day mortality, as determined by multivariate logistic regression analysis (p = 0.002, p < 0.001, and p < 0.001, respectively). Moreover, ROC curve analysis revealed that the combination of serum CA19-9 levels and MELD scores yielded an AUC value of 0.828 for predicting patient prognosis, which was markedly greater than that of either factor when analyzed separately (Figure 4(b)). Specifically, the AUC value for the MELD score was 0.773, whereas that for the serum CA19-9 level was 0.665. The Hosmer–Lemeshow test for the CA19-9+MELD model revealed a p-value of 0.42, indicating good model fit. A post-hoc power analysis confirmed the presence of 89% power to detect AUC differences ≥0.1. When assessed independently, the serum CA19-9 level exhibited a sensitivity of 49.4% and a specificity of 77.8%, whereas the MELD sore had a sensitivity of 62.1% and a specificity of 80.0%. Importantly, combining serum CA19-9 levels with the MELD score led to increased sensitivity and specificity, reaching 83.9% and 84.2%, respectively (Table 4).
Serum CA19-9 levels at ICU admission and MELD scores for the prognostic prediction of patient outcomes.

CA19-9: carbohydrate antigen 19-9; MELD: Model for End-Stage Liver Disease; AUC: area under the curve; PPV: positive predictive value; NPV: negative predictive value.
Etiology-specific analysis
Subgroup analyses stratified by etiology revealed significant variations in the prognostic performance of AFP and CA19-9 (Table 5, Figure 5). In APAP-induced ALF, the combination of CA19-9 and MELD demonstrated the highest predictive accuracy (AUC = 0.885), followed by AFP+MELD (AUC = 0.684). For viral hepatitis-associated ALF, AFP alone showed the strongest discriminative power (AUC = 0.880), whereas CA19-9+MELD yielded an AUC value of 0.765. In TCM-induced ALF, both AFP+MELD (AUC = 0.846) and CA19-9+MELD (AUC = 0.842) showed comparable performance. Baseline characteristics further highlighted the following differences among etiologies: patients with viral hepatitis were older (51.8 ± 13.5 years) with higher baseline alanine aminotransferase (median: 1293 U/L) and aspartate aminotransferase levels (1160 U/L), whereas TCM-induced ALF cases presented with pronounced hyperbilirubinemia (median serum total bilirubin level: 390.4 µmol/L).
Comparison of AUC values among different etiology subgroups.

AUC: area under the curve; AFP: alpha-fetoprotein; CA19-9: carbohydrate antigen 19-9; MELD: Model for End-Stage Liver Disease; APAP: APAP: acetaminophen
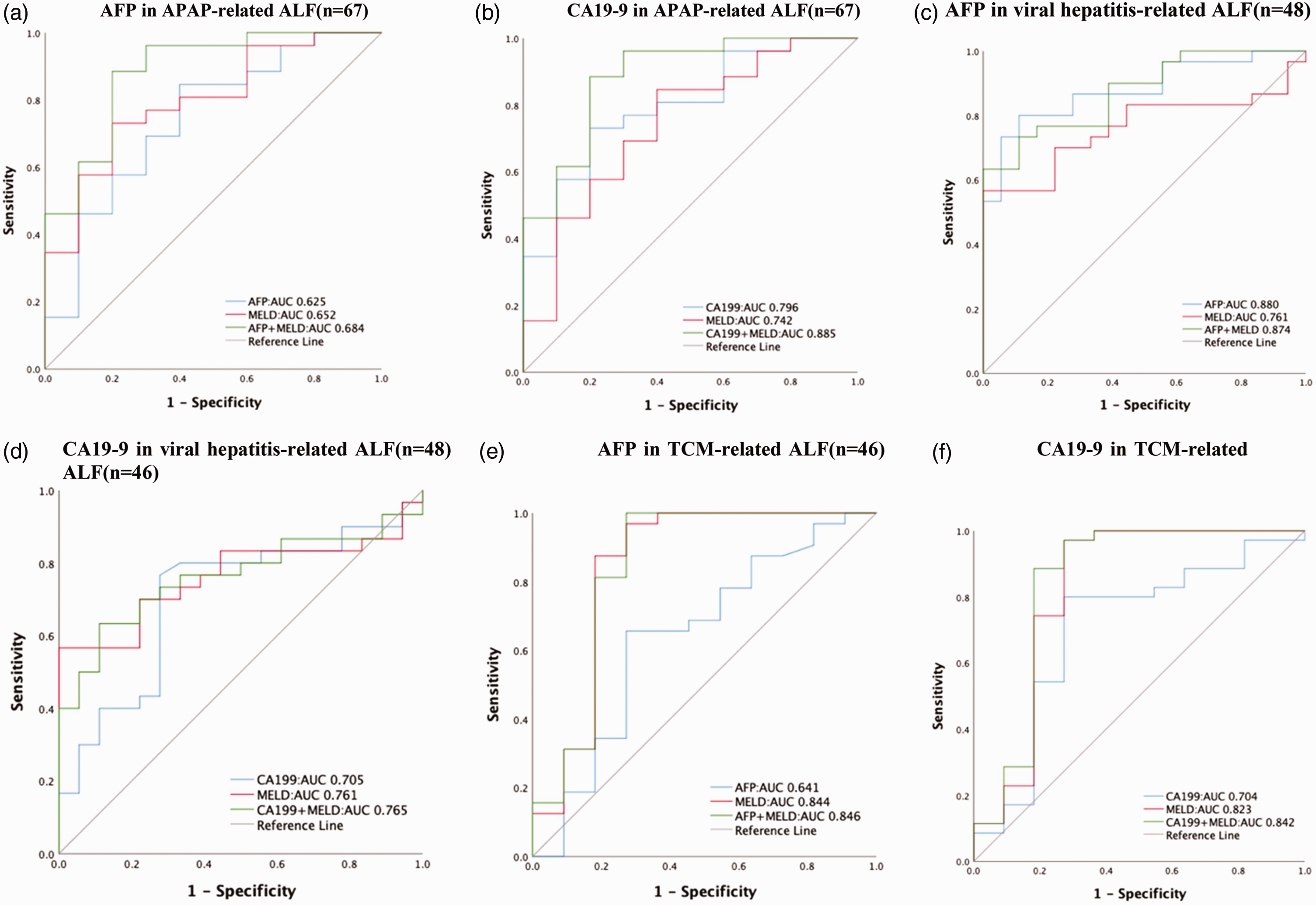
The ROC curve of serum AFP and CA19-9 levels for assessment of the risk level of 28-day mortality in different etiologies. (a) AFP in APAP-induced ALF (n = 67); (b) CA19-9 in APAP-induced ALF (n = 67); (c) AFP in viral hepatitis-associated ALF (n = 48); (d) CA19-9 in viral hepatitis-associated ALF (n = 48); (e) AFP in TCM-induced ALF (n = 46) and (f) CA19-9 in TCM-induced ALF (n = 46). ROC: receiver operating characteristic; AFP: alpha-fetoprotein; CA19-9: carbohydrate antigen 19-9; APAP: acetaminophen; ALF: acute liver failure; TCM: traditional Chinese medicine.
Discussion
This study confirms the protective role of AFP in ALF prognosis and, for the first time, demonstrates the prognostic significance of CA19-9. By documenting dynamic changes in AFP and CA19-9 levels over the first 3 days of ICU admission, we revealed distinct trends between survivors and nonsurvivors. Combining these biomarkers with the MELD score provides a robust and clinically actionable risk stratification tool. Importantly, our etiology-specific analyses offer novel insights into the differential performance of AFP and CA19-9 across various causes of ALF.
AFP is a glycoprotein synthesized by hepatoblasts in the developing fetal liver and yolk sac during embryogenesis. 16 Following birth, AFP expression decreases significantly; however, it can be re-expressed later in life during liver regeneration or in specific pediatric and adult malignancies. 17
In acute liver injury, elevated AFP levels may be due to the regenerative and repair response of hepatocytes. 18 The role of AFP as a prognostic biomarker in ALF has been previously established, with multiple studies demonstrating its association with hepatocyte regeneration and improved outcomes. Recent research has linked AFP levels to outcomes in patients with non-APAP–induced ALF. 19 Varshney et al. revealed that increased AFP levels indicate hepatic regeneration, which improves ALF prognoses. 20 In our study, we found that AFP levels were elevated earlier in patients with ALF and were associated with an improved prognosis, which is consistent with previous findings.19,21 However, our study enhances this understanding by demonstrating that AFP levels dynamically increase over the first three days of ICU admission in survivors, highlighting the importance of serial measurements for prognostic assessment. The fluctuations in AFP levels among patients suffering from ALF and their prognostic significance during the initial phase of liver failure have not been extensively explored. In our study, we focused on dynamically detecting changes in serum AFP levels from Day 1 to Day 3 following ICU admission. Serum AFP levels increased in patients with ALF within 3 days of ICU admission, especially survivors, who had considerably greater AFP levels than nonsurvivors. Serum AFP levels significantly predicted the 28-day mortality. Our study also performed etiology-specific analyses, revealing AFP’s performance across different causes of ALF. It showed that CA19-9 excels in APAP-induced ALF, while AFP performs better in viral hepatitis-associated ALF. Based on these findings, we are inclined to conclude that AFP may serve as a protective factor against this disease, with elevated AFP levels indicating a favorable prognosis.
CA19-9 is a glycoprotein secreted by the pancreas, biliary system, and other gastrointestinal tissues and is mainly used for the detection of pancreatic cancer. However, elevated levels of CA19-9 are not limited to malignant tumors but have also been detected in various benign liver diseases. 22 Fukasawa et al. found that CA19-9 levels were significantly elevated in cholestatic liver diseases such as primary biliary cholangitis and primary sclerosing cholangitis, which may be caused by bile retention due to biliary obstruction, biliary damage, and epithelial cell inflammation. 23 Sapmaz et al. reported a correlation between CA19-9 levels and autoimmune hepatitis. 24 In patients with ALF, Halme et al. identified CA19-9 as a marker of nonmalignant hepatocellular biliary transformation. 25 Bertino et al. also revealed that CA19-9 levels may be elevated in patients with cirrhosis and chronic hepatitis. 26 This may be due to hepatocyte dysfunction and increased pressure on the biliary system, leading to increased CA19-9 secretion. 27 These are consistent with our findings, suggesting that elevated CA19-9 levels are correlated with the severity of liver lesions in patients with ALF. In this study, we found that CA19-9 levels significantly differed between survivors and nonsurvivors within 3 days of ICU admission for ALF, with levels escalating in nonsurvivors and diminishing in survivors. Moreover, we revealed that combining CA19-9 with MELD scores improved the predictive power for 28-day mortality, suggesting CA19-9’s potential as a novel prognostic marker for ALF.
In patients with ALF, the mechanism by which changes in CA19-9 levels affect patient prognosis remains unclear, which may be due to the following reasons. First, elevated levels of CA19-9 correlate with biliary system stress and injury, reflecting the severity of biliary obstruction and the ability to recover in cholestatic disease. In ALF, the health of the biliary system has a critical impact on liver function and patient prognosis. CA19-9 may also reflect hepatic inflammation, influencing ALF progression and prognosis.
Our study shows that AFP levels are linked to improved outcomes in non-APAP–induced ALF, aligning with previous findings. However, recent research has identified additional biomarkers with similar or better prognostic accuracy, both alone and combined with the MELD score, for APAP- and non-APAP–induced ALF. For instance, Karvellas et al. 28 demonstrated that elevated fatty acid-binding protein 1 levels were correlated with poorer survival in APAP-induced ALF. McGill et al. 29 reported that mitochondrial biomarkers such as glutamate dehydrogenase and mitochondrial DNA fragments can predict outcomes in APAP-induced ALF. Vazquez et al. 30 identified lactate dehydrogenase as a prognostic marker, while Kwan et al. 31 showed that CPS1 levels enhance prognostic accuracy when combined with the ALFSG Prognostic Index in APAP-induced ALF. These findings suggest that combining multiple biomarkers can improve prognostic precision. Notably, chemokine (C-X-C motif) ligand 14 (CXCL14), a recently discovered biomarker, has shown promise in predicting negative outcomes in APAP-induced ALF. 32 Unlike AFP, which is primarily associated with non-APAP–induced ALF, CXCL14 is specifically linked to APAP-induced liver injury through its role in hepatocyte senescence and impaired regeneration. This suggests that CXCL14 can complement AFP in a broader prognostic panel, particularly for APAP-induced ALF.
Our etiology-specific analysis revealed distinct patterns in the prognostic performance of AFP and CA19-9 across different ALF causes. CA19-9 combined with MELD showed superior accuracy in APAP-induced ALF (AUC = 0.885), whereas AFP alone performed best in viral hepatitis-associated ALF (AUC = 0.880). In TCM-induced ALF, both biomarkers showed balanced performance (AFP+MELD: AUC = 0.846; CA19-9+MELD: AUC = 0.842). The strong performance of CA19-9 in APAP-induced ALF may reflect its role as a marker of biliary injury, a key feature of APAP toxicity. 28 In contrast, AFP’s predictive value in viral hepatitis-associated ALF likely stems from its association with hepatocyte regeneration, which is robust in viral hepatitis due to immune-mediated viral clearance and repair. 33 The balanced performance in TCM-induced ALF may result from the mixed hepatocellular and cholestatic injury patterns typical of herbal hepatotoxicity. 34 These findings highlight the need for tailored prognostic approaches in ALF management, particularly where distinct injury mechanisms dominate.
Several limitations of this study are important to acknowledge. First, the study cohort was restricted to patients who lived beyond the third day of ICU admission, with certain individuals eliminated due to mortality or liver transplantation within 72 h of admission, thereby impacting the generalizability of the findings. Second, the quantity of serum samples for each treatment group was limited, and we exclusively documented AFP and CA19-9 levels within 3 days of ICU admission; the predictive significance of serum levels at longer intervals requires further investigation. Third, despite the significant correlations with survival observed in our study, the substantial overlap between the survival and nonsurvival groups limits the clinical utility of these parameters as true prognostic biomarkers. We suggested further research to identify more effective biomarkers.
Moreover, serum levels of AFP and CA19-9 may be influenced by patients’ pretreatment conditions and pharmacological interventions; subsequent research should more effectively account for these confounding variables and incorporate larger sample sizes. Nonetheless, the precise etiologies of alterations in CA19-9 and AFP levels in individuals with ALF require additional exploration, and we offered novel insights for prognostic evaluation in ALF.
Conclusion
This study highlights the prognostic value of serum AFP and CA19-9 levels in patients with ALF admitted to the ICU. Consistent with prior research, AFP serves as a protective factor, whereas CA19-9 emerges as a novel prognostic marker, significantly improving outcome prediction when combined with the MELD score. Etiology-specific analyses revealed distinct biomarker performance patterns: CA19-9 excels in APAP-induced ALF, whereas AFP performs better in viral hepatitis-associated ALF. These findings underscore the importance of tailored prognostic approaches based on underlying injury mechanisms. Clinically, this study provides valuable insights for assessing the need for liver transplantation or other interventions. Future studies should validate these findings in larger cohorts and explore the integration of additional liver function markers, such as alanine transaminase, total bilirubin, and coagulation parameters, to enhance prognostic accuracy.
Footnotes
Acknowledgements
We express our sincere gratitude to the experts and colleagues of the ICU Department of the Ethics Committee of the Fifth Medical Center of the Chinese PLA General Hospital for their valuable contributions. Furthermore, we are thankful for the profound feedback from our colleagues and the editorial team, which played a significant role in enhancing this study.
Authors’ contribution
Rui Qi drafted the initial manuscript, collected data, and performed statistical. analyses; Xin Wang contributed to statistical analysis and manuscript revision; Zhidan Kuang and Dan Chang assisted with data collection and management; Xueyi Shang and Lin Fang reviewed and edited the manuscript; Jinsong Mu designed the study, supervised the writing process, and approved the final version. All authors critically reviewed the manuscript and approved its submission for publication.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
No potential conflicts of interest were reported by the authors.
Funding
The study was supported by the National Key R&D Program of China (No.2022YFA1103501).
Institutional review board statement
This investigation was approved by the Ethics Committee of the Fifth Medical Center of the Chinese PLA General Hospital. No. KY-2024-10-163-1.
Informed consent statement
Due to the retrospective design of the study, the requirement for written informed consent was waived.