
Abstract
Study Design
Retrospective comparative study.
Objective
Neuromuscular scoliosis (NMS) is a complex deformity requiring individualized surgical strategies focused on improving sitting balance and quality of life. This study aimed to evaluate the clinical efficacy and safety of multilevel asymmetrical Ponte osteotomy (MAPO) in NMS patients, compared to conventional posterior fusion without osteotomy.
Methods
A retrospective review was conducted on 90 patients with NMS who underwent posterior spinal correction between 2015 and 2021. Patients were divided into a MAPO group (n = 52) and a control group (n = 38). Radiographic parameters and health-related quality of life (SRS-22) were assessed preoperatively, postoperatively, and at ≥2-year follow-up. Perioperative data, including operative time, blood loss, transfusion volume, and complications, were analyzed.
Results
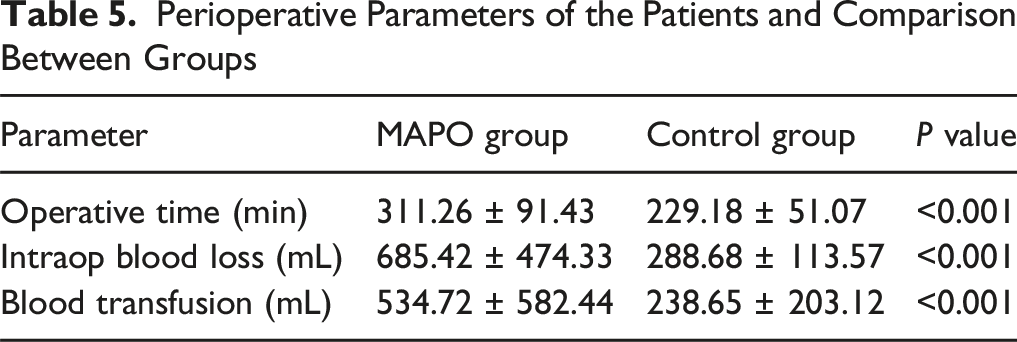
Baseline characteristics were comparable. The MAPO group achieved significantly greater correction in major curve angle (49.75% vs 46.34%, P = 0.031), pelvic obliquity (25.26% vs 20.81%, P = 0.048), and sagittal vertical axis (33.99% vs 30.08%, P = 0.045). Postoperative satisfaction (4.43 ± 0.55 vs 4.11 ± 0.57, P = 0.026) and function scores (4.39 ± 0.48 vs 4.10 ± 0.61, P = 0.040) were also significantly higher in the MAPO group. However, MAPO was associated with longer operative time (311 vs 229 min, P < 0.001), greater blood loss (685 vs 289 mL, P < 0.001), and a trend toward increased complications, including wound issues and CSF leaks.
Conclusions
MAPO offers improved deformity correction and higher patient satisfaction compared to non-osteotomy procedures in NMS, though with increased surgical complexity. It may serve as a valuable option for selected patients when balancing benefits and risks.
Introduction
Scoliosis Research Society Classification of Neuromuscular Scoliosis
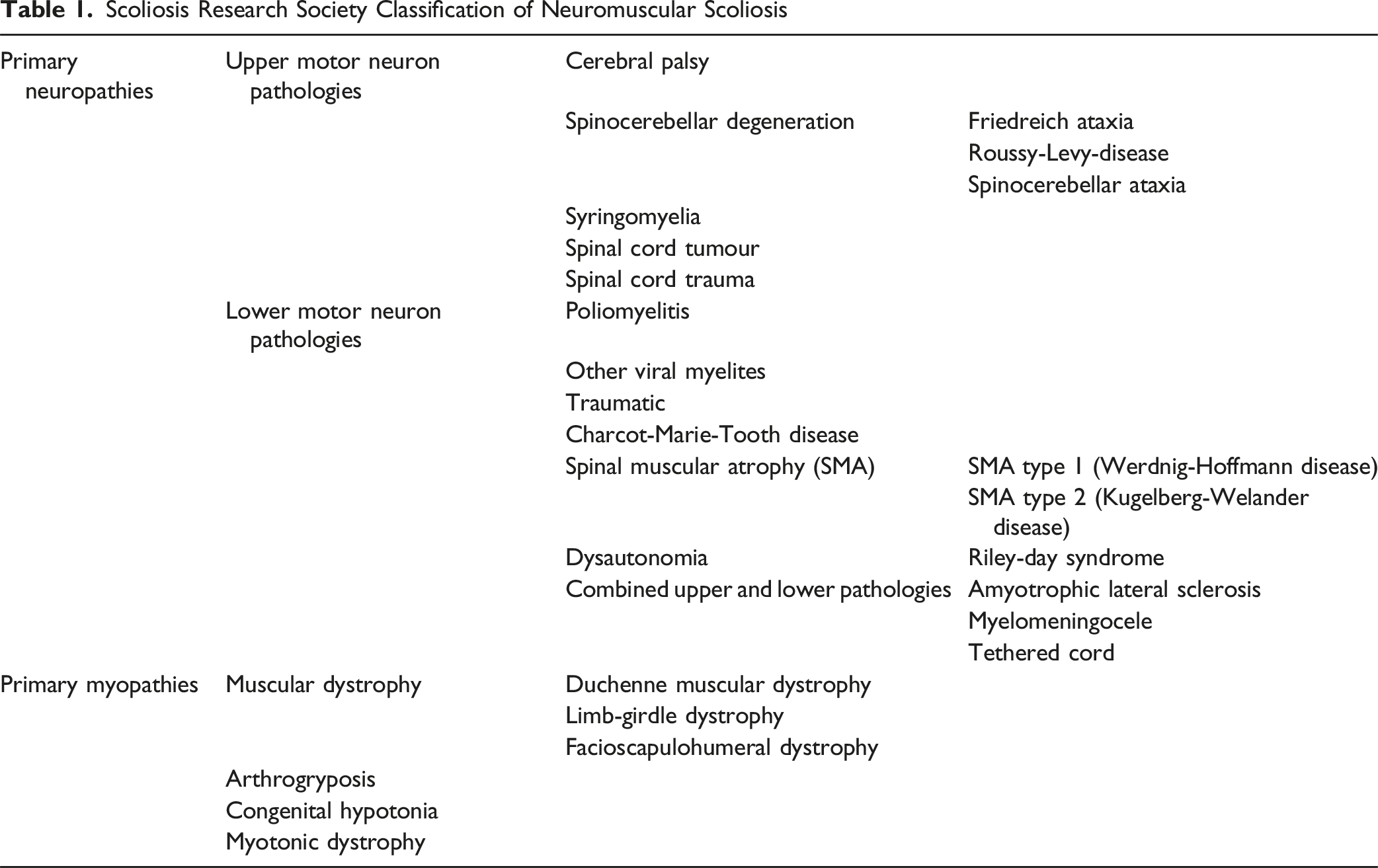
Ponte osteotomy, first described by Ponte in 1984, is a posterior column osteotomy technique designed to enhance spinal flexibility and correction, particularly in rigid deformities.7,8 The procedure involves resection of the posterior vertebral elements—including spinous processes, laminae, and facets—to allow angular correction, primarily in the sagittal plane. 9 It has gained widespread use in the management of adolescent idiopathic scoliosis and adult spinal deformities, due to its relatively low morbidity and capacity for segmental correction.10-12 However, its application in neuromuscular scoliosis remains limited and under-investigated.
To address the limitations of conventional Ponte osteotomy, a modified technique—Multilevel Asymmetrical Ponte Osteotomy (MAPO)—has been introduced in recent years.13,14 MAPO involves performing osteotomies over multiple segments, with asymmetrical resection favoring the convex side to generate non-parallel gaps, thereby enabling three-dimensional correction without increasing osteotomy grade. This technique has demonstrated promising results in treating rigid curves while avoiding the higher complication rates associated with vertebral column resection.
Although small cohort studies have explored the role of posterior column osteotomies in NMS, there remains a lack of large-scale or long-term data specifically evaluating the efficacy and safety of MAPO in this unique patient population. Further evidence is needed to determine whether the benefits observed in idiopathic or adult rigid curves can be translated to neuromuscular cases.
Methods
This retrospective study was conducted in accordance with the STROCSS (Strengthening the Reporting of Cohort Studies in Surgery) guidelines, ensuring rigorous methodological design and transparent reporting standards. 15
Patients
Patients diagnosed with neuromuscular scoliosis who underwent posterior spinal correction surgery at our institution between January 2015 and December 2021 were retrospectively reviewed. Inclusion criteria were: (1) diagnosis of neuromuscular scoliosis; (2) having received either multilevel asymmetrical Ponte osteotomy (MAPO, MAPO group) or conventional posterior spinal fusion without osteotomy (control group). Exclusion criteria included: (1) prior spinal surgery; (2) incomplete medical records; (3) follow-up duration of less than two years; or (4) use of a higher-grade osteotomy technique (eg, pedicle subtraction or vertebral column resection).
A total of 116 patients were initially identified. After applying the exclusion criteria, 26 patients were excluded: 12 due to inadequate follow-up, 9 due to incomplete documentation, 3 with a history of prior spinal surgery, and 2 who had undergone higher-grade osteotomies. Ultimately, 90 patients were included in the study, comprising 52 patients in the MAPO group and 38 patients in the control group.
Ethical Statement
The study was conducted following the Declaration of Helsinki and was approved by our hospital’s Institutional Review Board (2024-ke-964). Prior to surgery, informed consent was obtained from all patients or their legal guardians.
Surgical Procedure
All surgeries were performed by a single surgical team specializing in spinal deformities. After induction of general anesthesia, patients were positioned prone on a surgical table. A midline posterior incision was made, followed by subperiosteal exposure of the posterior elements from the upper instrumented vertebra (UIV) to the lower instrumented vertebra (LIV). Bilateral pedicle screws were inserted on both the convex and concave sides according to preoperative surgical planning.
In the MAPO group, patients underwent multilevel asymmetrical Ponte osteotomies as previously described by Zhang et al13,14 Osteotomy levels were typically centered on the apex of the main curve and extended to one or two adjacent segments based on segmental rigidity. Prior to osteotomy, segmental mobility was assessed using towel clamps. The posterior elements—including spinous processes, laminae, and facet joints—were resected using osteotomes, rongeurs, and Kerrison punches. The extent of resection was deliberately wider on the convex side to create non-parallel osteotomy gaps, allowing for asymmetric closure and enhanced coronal correction. The ligamentum flavum was entirely removed, and the epidural space was exposed to facilitate mobility. Two pre-contoured rods were inserted, and deformity correction was achieved through sequential manual compression, distraction, segmental translation, and rod derotation. The posterior column was then compressed starting from the apex and extending outward to close the residual gaps and restore sagittal alignment.
In the control group, patients underwent standard posterior spinal fusion with pedicle screw instrumentation but without any osteotomies or posterior column resections.
Intraoperative neuromonitoring using somatosensory-evoked potentials (SSEP) and wake-up tests were utilized throughout all procedures to minimize the risk of neurological complications. 16
Data Collection
Demographic and clinical data—including age, sex, body mass index (BMI), and underlying neuromuscular diagnosis—were retrieved from electronic medical records. Radiographic parameters were assessed at three time points: preoperatively, immediately postoperatively, and at the final follow-up (minimum of two years). The following radiographic variables were evaluated: major curve (MC), thoracic kyphosis (TK), lumbar lordosis (LL), pelvic tilt (PT), sacral slope (SS), pelvic incidence (PI), pelvic incidence minus lumbar lordosis (PI–LL), pelvic obliquity (PO), apical vertebral translation (AVT), coronal balance distance (CBD), shoulder balance, and sagittal vertical axis (SVA). Perioperative parameters included operative time, estimated intraoperative blood loss, and volume of blood transfusion, which comprised both allogeneic and autologous blood components, including intraoperative cell salvage. Routine radiographic follow-up was performed at scheduled intervals up to 2 years to monitor fusion status and instrumentation integrity. All complications occurring during the perioperative or follow-up period were documented and categorized into wound-related complications, neurological deficits, cerebrospinal fluid (CSF) leaks, pulmonary complications, infections, gastrointestinal disturbances, and unplanned revision surgeries. Complications were classified a priori as major (neurological deficit, cerebrospinal fluid leak requiring reoperation, pulmonary complication, revision surgery) or minor (wound complications, superficial infection, gastrointestinal events). The timing (perioperative vs follow-up) and any reintervention were recorded.
Fusion Assessment
Fusion was assessed clinically and radiographically at 3, 6, 12, and 24 months using standardized full-spine anteroposterior and lateral radiographs. Radiographic fusion was operationally defined as continuous posterior bridging bone across instrumented levels together with absence of hardware lucency, implant migration, or progressive segmental motion. Pseudarthrosis was suspected in the presence of persistent/progressive axial pain, local tenderness, hardware-related symptoms, or interval loss of correction (>5° between consecutive visits); equivocal cases underwent closer clinical review and repeat radiographs. Implant failure was defined as rod fracture, screw breakage, loosening, or migration on serial imaging.
Follow-up
All patients were followed at regular postoperative intervals of 3, 6, 12, and 24 months. At each visit, both clinical and radiographic outcomes were systematically assessed. Radiographic evaluations included full spine standing anteroposterior and lateral radiographs to assess coronal and sagittal alignment, instrumentation integrity, and fusion status.
Clinical outcomes were measured using the Scoliosis Research Society-22 (SRS-22) questionnaire, which assesses five domains: pain, self-image, function, mental health, and satisfaction with management.17-19 Although originally developed for adolescent idiopathic scoliosis, the SRS-22 remains a widely used tool in spinal deformity research. The SRS-22 questionnaire was administered at baseline and at 2-year follow-up under physician supervision, with caregiver assistance provided for patients with communication or cognitive limitations.
Statistical Analysis
All statistical analyses were performed using SPSS software (version 25.0; IBM Corp., Armonk, NY, USA). Continuous variables were presented as means ± standard deviations and compared using the independent samples t-test or Mann–Whitney U test, depending on data distribution. Categorical variables were expressed as counts and percentages and analyzed using the chi-square test or Fisher’s exact test where appropriate. A two-tailed P-value <0.05 was considered statistically significant.
The primary outcome measures were the differences in radiographic correction parameters and SRS-22 domain scores between the MAPO and control groups at the final follow-up. Secondary outcomes included perioperative variables (operative time, blood loss, transfusion volume) and complication rates.
Results
Baseline Characteristics
Patient Demographics and Radiographic Parameters Comparison
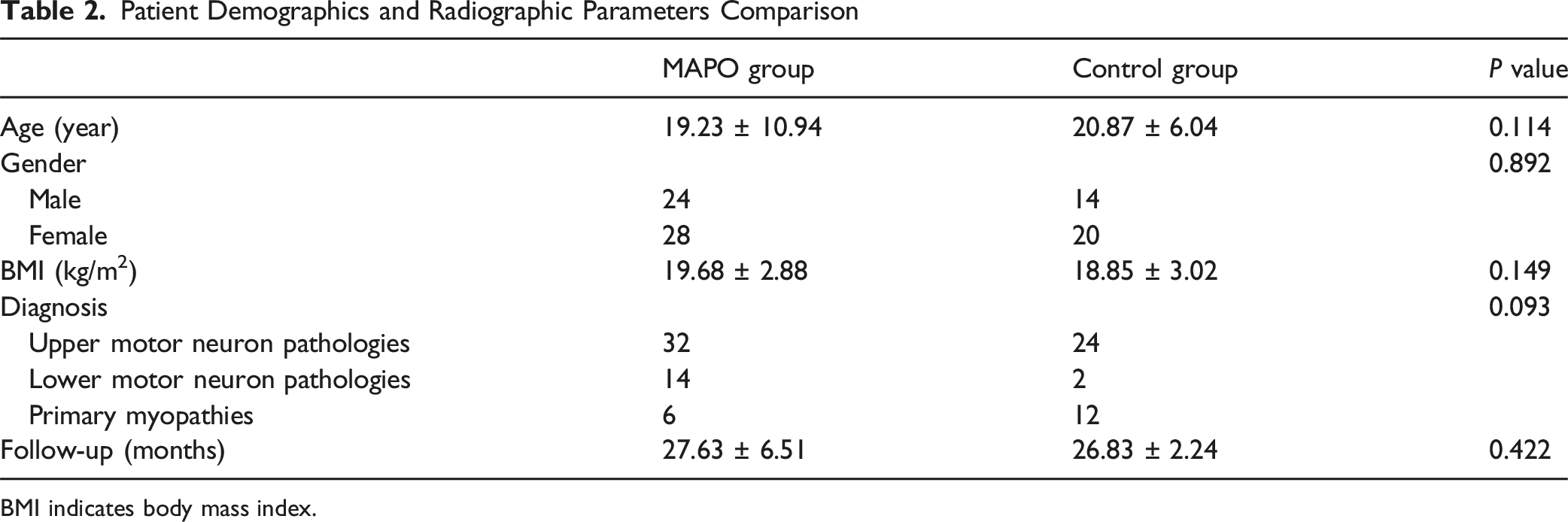
BMI indicates body mass index.
Distribution of NMS Diagnoses in the MAPO and Control Groups
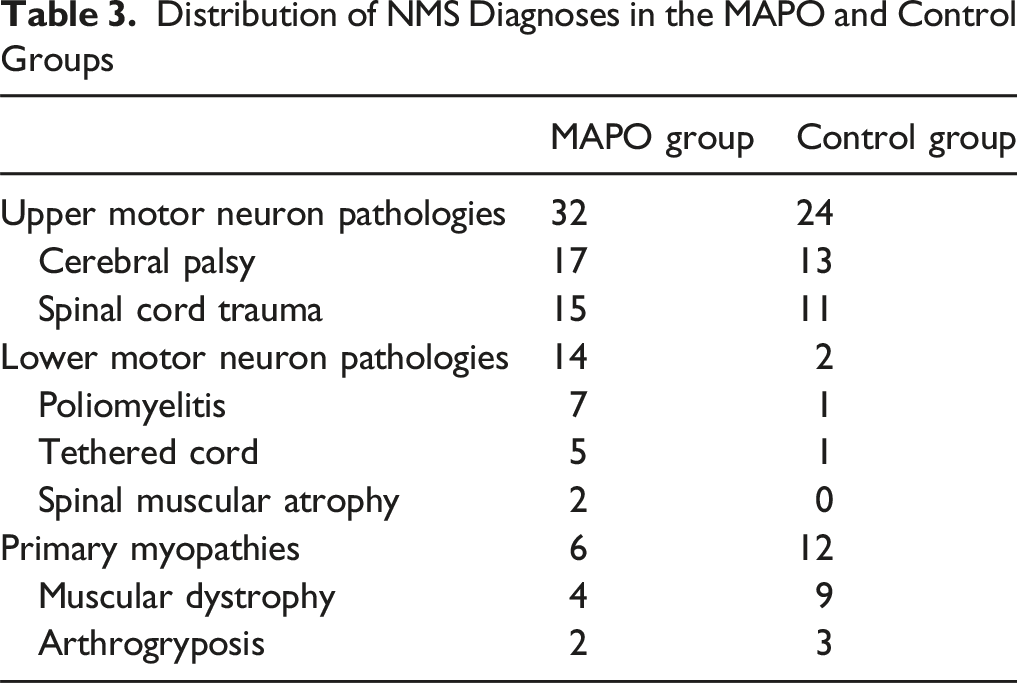
These findings indicate that both groups were generally comparable in demographic and baseline clinical characteristics, although mild differences in the types of neuromuscular pathology may still warrant consideration when interpreting treatment outcomes.
Radiographic Analysis
Radiographic Parameters of the Patients and Comparison Between Groups
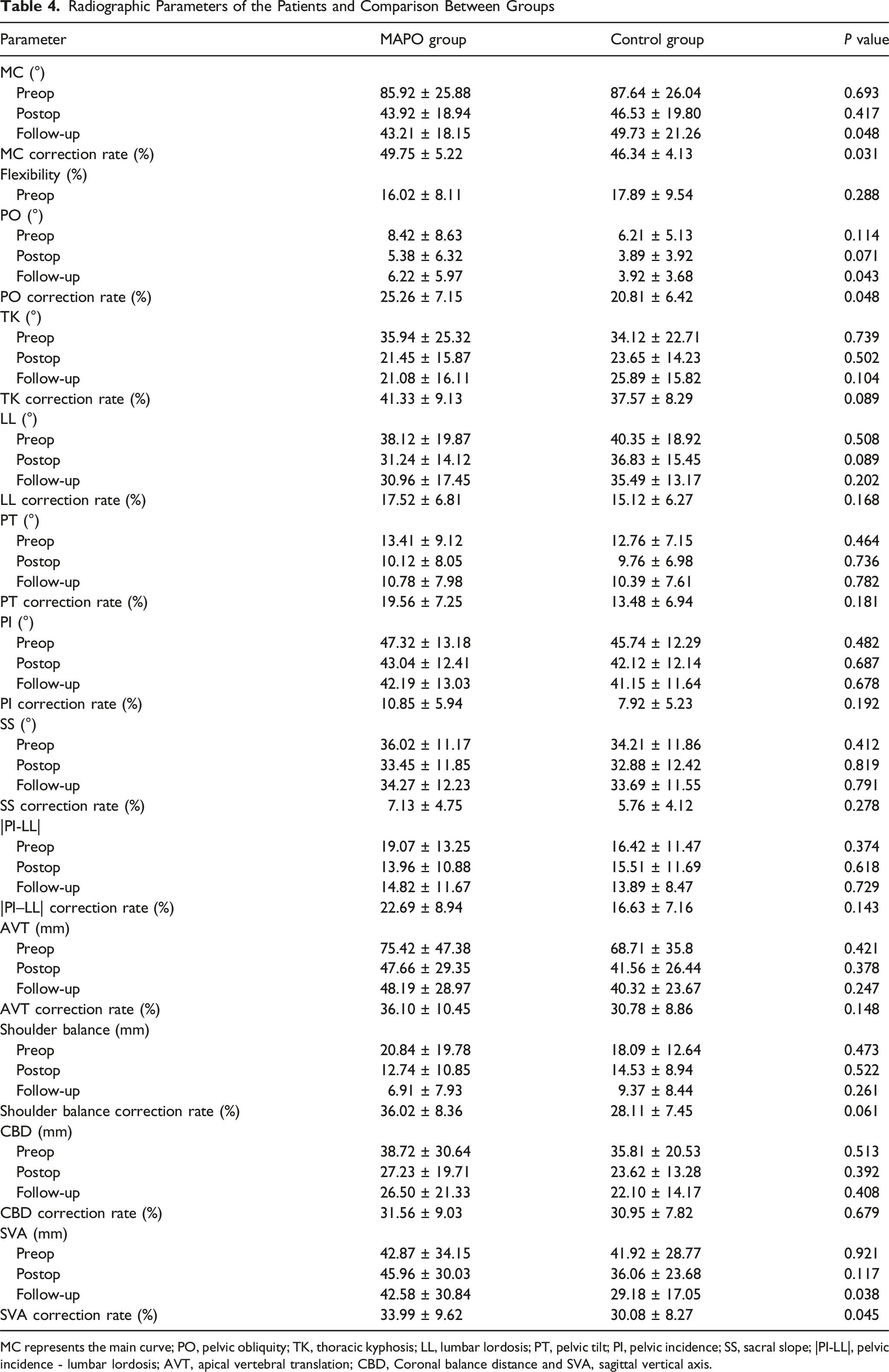
MC represents the main curve; PO, pelvic obliquity; TK, thoracic kyphosis; LL, lumbar lordosis; PT, pelvic tilt; PI, pelvic incidence; SS, sacral slope; |PI-LL|, pelvic incidence - lumbar lordosis; AVT, apical vertebral translation; CBD, Coronal balance distance and SVA, sagittal vertical axis.
PO also showed favorable correction in the MAPO group. Although preoperative PO was not significantly different (8.42 ± 8.63° vs 6.21 ± 5.13°; P = 0.114), postoperative (5.38 ± 6.32° vs 3.89 ± 3.92°; P = 0.071) and follow-up values (6.22 ± 5.97° vs 3.92 ± 3.68°; P = 0.043) indicated improved alignment. The PO correction rate was significantly greater in the MAPO group (25.26 ± 7.15%) than in the control group (20.81 ± 6.42%; P = 0.048).
TK and LL showed no significant intergroup differences across all time points. TK correction rates were 41.33 ± 9.13% in the MAPO group and 37.57 ± 8.29% in the control group (P = 0.089), while LL correction rates were 17.52 ± 6.81% and 15.12 ± 6.27%, respectively (P = 0.168).
PT, PI, and SS showed comparable trends. Although preoperative values differed slightly, all postoperative and follow-up comparisons were nonsignificant. The correction rates for PT, PI, and SS did not differ significantly between groups.
Global sagittal and coronal alignment parameters also reflected differences. The CBD showed no significant difference preoperatively (38.72 ± 30.64 mm vs 35.81 ± 20.53 mm; P = 0.513), and this persisted postoperatively and at follow-up. Similarly, AVT and shoulder balance measurements were not significantly different between groups.
However, the SVA at final follow-up was significantly greater in the MAPO group (42.58 ± 30.84 mm) than in the control group (29.18 ± 17.05 mm; P = 0.038), though preoperative and postoperative values were comparable. The SVA correction rate also favored the MAPO group (33.99 ± 9.62% vs 30.08 ± 8.27%; P = 0.045).
These radiographic findings indicate that while many parameters were similar between groups, MAPO provided superior correction of the main curve and pelvic obliquity, and more favorable outcomes in sagittal balance correction, underscoring its biomechanical and clinical advantage.
A representative case of a 10-year-old male with Chiari malformation and syringomyelia demonstrated a 71% correction of an 87° main curve using the MAPO technique, with a 6 cm increase in spinal height (T1–S1) postoperatively (Figure 1). A representative case of a 10-year-old male who presented with a 9-year history of back asymmetry, which had progressively worsened over the past year. Preoperative MRI revealed syringomyelia and Chiari malformation with cerebellar tonsillar herniation. The patient underwent a staged procedure: posterior fossa decompression with duraplasty, followed by posterior spinal fusion from T3 to L3 using the MAPO technique. The main thoracic curve of 87° was corrected to 25°, achieving a 71% correction rate, with a T1–S1 height gain of 6 cm
Perioperative Data
Perioperative Parameters of the Patients and Comparison Between Groups
Complications
Complications
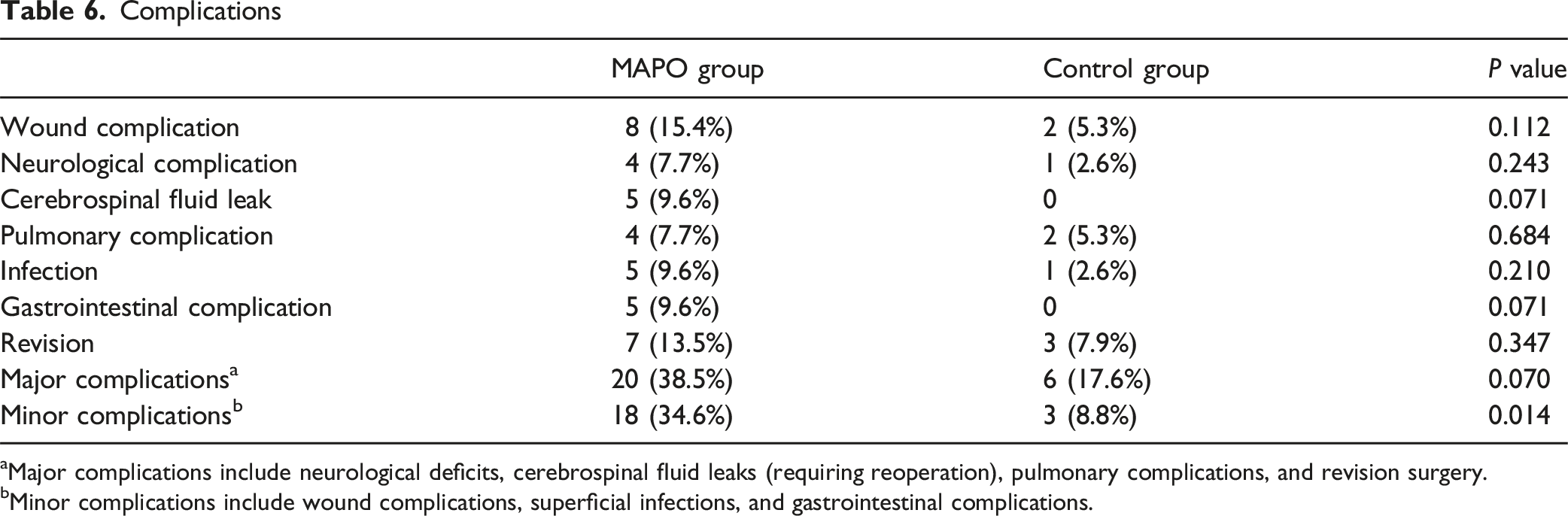
aMajor complications include neurological deficits, cerebrospinal fluid leaks (requiring reoperation), pulmonary complications, and revision surgery.
bMinor complications include wound complications, superficial infections, and gastrointestinal complications.
Clinical Outcomes
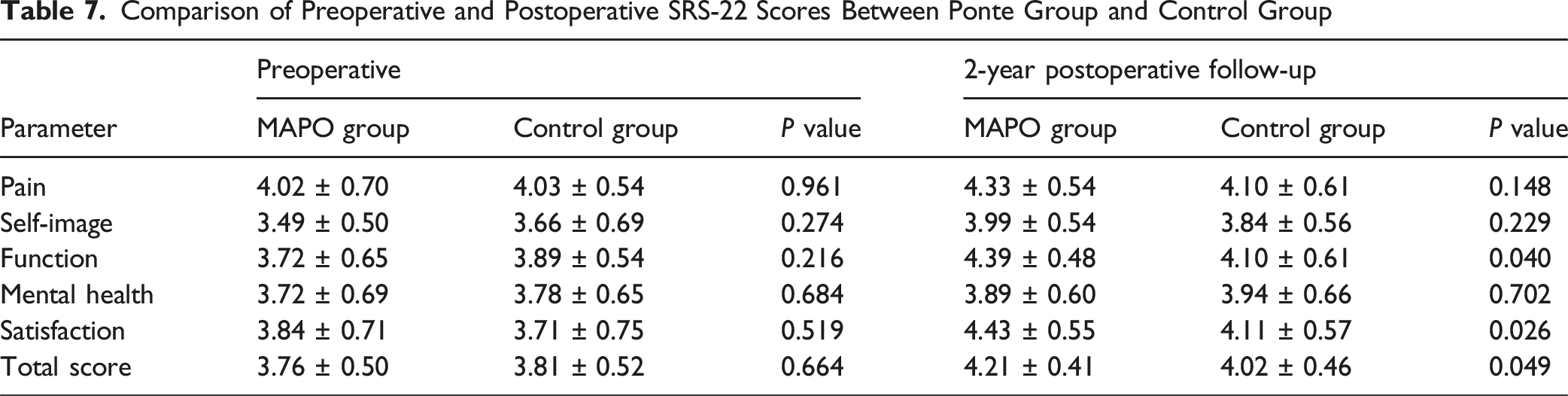
Both the MAPO and control groups demonstrated improvements in SRS-22 scores from the preoperative period to the 2-year postoperative follow-up, indicating enhanced health-related quality of life after surgery. Preoperatively, no statistically significant differences were observed between the groups in domains of pain (MAPO: 4.02 ± 0.70 vs control: 4.03 ± 0.54, P = 0.961), self-image (3.49 ± 0.50 vs 3.66 ± 0.69, P = 0.274), function (3.72 ± 0.65 vs 3.89 ± 0.54, P = 0.216), mental health (3.72 ± 0.69 vs 3.78 ± 0.65, P = 0.684), or satisfaction (3.84 ± 0.71 vs 3.71 ± 0.75, P = 0.519).
At the 2-year follow-up, the MAPO group reported significantly higher satisfaction scores (4.43 ± 0.55) than the control group (4.11 ± 0.57, P = 0.026). Additionally, the MAPO group showed higher mean scores in function (4.39 ± 0.48 vs 4.10 ± 0.61, P = 0.040) and total score (4.21 ± 0.41 vs 4.02 ± 0.46, P = 0.049), both reaching statistical significance. Although postoperative scores for pain, self-image, and mental health were numerically higher in the MAPO group, these differences did not reach significance.
Comparison of Preoperative and Postoperative SRS-22 Scores Between Ponte Group and Control Group
Discussion
The present study demonstrated that patients with NMS treated with MAPO experienced notable improvements in both clinical and radiographic outcomes compared to those who underwent conventional posterior spinal fusion without osteotomy. Specifically, the MAPO group exhibited higher postoperative SRS-22 scores in the domains of pain, function, and satisfaction, reflecting better subjective recovery. In terms of radiographic correction, MAPO significantly improved key parameters such as pelvic obliquity and coronal balance, which are critical for sitting posture, trunk symmetry, and quality of life in NMS patients. However, the MAPO group also demonstrated a trend toward higher complication rates, particularly in wound-related and gastrointestinal events, suggesting that while MAPO offers enhanced deformity correction, it may come at the cost of increased surgical complexity. Although overall complication rates tended to be higher in the MAPO cohort—particularly for minor events—this pattern likely reflects the greater invasiveness and longer operative time inherent to multilevel osteotomy. Importantly, these differences did not translate into a higher burden of reoperation or lasting morbidity. With targeted perioperative optimization (nutritional support, blood-loss reduction strategies, meticulous wound care, and early rehabilitation), risks can be mitigated. Therefore, the radiographic and functional benefits of MAPO should be weighed against a manageable increase in minor complications.
In the management of NMS, current evidence underscores that the primary surgical goal is to enhance patient quality of life and functional status rather than merely maximize radiographic correction. 20 Studies have shown that while substantial deformity correction can be achieved in NMS using posterior column procedures like Ponte osteotomies – with significant improvements in Cobb angle and pelvic obliquity and restoration of near-normal sagittal alignment – these gains do not come at the cost of high complication rates. 21 On the contrary, Ponte-based techniques in NMS have been associated with low morbidity, with reports of no intraoperative neurological injuries or implant-related complications in carefully managed series. 21 Building on this principle, the MAPO has emerged as an innovative strategy for rigid or complex curves. Its rationale lies in achieving adequate curve flexibility through multiple posterior column releases, thereby attaining correction comparable to that of more aggressive three-column osteotomies (eg, pedicle subtraction osteotomy or vertebral column resection) while markedly reducing surgical risk.13,14 Comparative analyses in severe, rigid scoliosis have confirmed that MAPO can obtain similar coronal and sagittal correction as a single-level VCR, with equivalent improvements in patient-reported outcomes (such as SRS-22 scores and Oswestry Disability Index). 14 Notably, the MAPO technique offers these outcomes with significantly less operative time, lower blood loss, and a dramatically lower complication incidence than VCR. High-grade osteotomies like PSO or VCR, while effective for severe deformities, carry substantially greater risks – including a higher likelihood of neurological injury 22 – and thus are often reserved for only the most intractable cases. In contrast, by leveraging multiple asymmetrical Ponte osteotomies, surgeons can maximize deformity correction and spinopelvic balance in NMS without exposing patients to the excessive trauma and complication profile inherent to 3-column osteotomies. This balance of efficacy and safety makes MAPO a compelling and judicious advancement in the treatment of NMS, aligning surgical intervention with the paramount goal of improved postoperative quality of life.
To maximize the therapeutic benefits of MAPO while minimizing the associated surgical risks, meticulous perioperative management is essential. Preoperative planning should not only include routine radiographic assessments but also advanced techniques such as 3D reconstruction and simulation modeling to anticipate anatomical challenges, particularly in patients with severe pelvic obliquity or rigid curves. 23 Identifying high-risk factors—such as poor nutritional status, pulmonary dysfunction, or prior surgical history—is critical to optimizing patient selection and tailoring intraoperative strategies. Intraoperatively, maintaining hemodynamic stability and minimizing blood loss, including the use of cell salvage systems, can reduce transfusion-related complications. Postoperatively, enhanced recovery protocols, early nutritional support, and vigilant monitoring for wound-related or neurological complications are necessary to improve outcomes. These measures collectively ensure that the structural advantages of MAPO—namely, improved deformity correction without the morbidity of three-column osteotomies—are translated into safe and meaningful clinical benefits for patients with neuromuscular scoliosis.
The indication for multilevel asymmetrical Ponte osteotomy was individualized. Patients with severe curves (>70°), pronounced pelvic obliquity, or limited correction (<30% improvement on bending or traction radiographs) were more likely to benefit from MAPO. Although many neuromuscular scoliosis patients present with hypotonic, relatively flexible curves, those with rigid deformities or asymmetric pelvic imbalance may require osteotomy to achieve adequate correction and balance. When contemplating MAPO, we weigh the expected incremental correctional benefit against patient-specific perioperative risk. The anticipated benefit is estimated from bending/traction radiographs and three-dimensional planning (including the projected gain in correction and pelvic obliquity reduction, and the likelihood of achieving a stable seated posture). Risk appraisal incorporates operative time and blood-loss exposure, nutritional status and skin integrity, respiratory reserve, and overall frailty, alongside the availability of risk-mitigation strategies such as standardized perioperative pathways, multidisciplinary management, and 3D printing–based planning. In our cohort, the higher complication signal with MAPO was largely driven by minor events and did not translate into excess reoperation or lasting morbidity. Decisions are ultimately made through shared decision-making between the surgical team and the patient, with caregiver involvement as appropriate.
Three-dimensional simulation and printing were integrated into the preoperative planning process for all patients in this cohort. Patient-specific 3D models of the spine and pelvis enabled the surgical team to visualize complex deformities, determine osteotomy levels, estimate asymmetric wedge dimensions, and anticipate correction of pelvic obliquity. These models also facilitated advance rod contouring and verification of screw trajectories, thereby reducing intraoperative uncertainty and improving execution accuracy. The application of 3D planning tools may thus enhance the safety and reproducibility of MAPO, particularly in patients with rigid curves or severe lumbopelvic imbalance.
Despite the encouraging results, several limitations of this study should be acknowledged. First, there was heterogeneity in the distribution of neuromuscular conditions between groups. Patients with upper motor neuron disorders often exhibit spasticity and pelvic obliquity, whereas those with lower motor neuron disorders or primary myopathies typically present with hypotonia and more flexible curves. These distinctions may influence curve stiffness, correction potential, and complication risk. Although the diagnostic distribution did not differ significantly at baseline, its potential clinical impact remains relevant, and our results should be interpreted with caution. Second, we did not perform multivariable regression modeling. The relatively modest sample size and limited number of events—especially within diagnostic subgroups and specific complication categories—would likely result in overfitting and unstable estimates; therefore, only univariate comparisons were reported. Another limitation concerns the use of the SRS-22 questionnaire. Although SRS-22 is widely adopted in scoliosis research, it was originally designed for adolescent idiopathic scoliosis and may not fully capture quality-of-life domains that are particularly relevant in neuromuscular scoliosis, such as seated balance, pressure relief, and caregiver dependence. In our cohort, questionnaires were completed under physician supervision with caregiver assistance when necessary, which is consistent with prior reports but does not fully overcome the tool’s limitations. Future work should focus on the development and validation of neuromuscular scoliosis–specific outcome measures. Another limitation is that propensity score matching was not applied. Although considered, the relatively modest sample size and diagnostic heterogeneity limited its feasibility, as matching would have substantially reduced the effective sample size and statistical power. Larger multicenter studies will be better positioned to use such techniques to further strengthen group comparability. Large-scale prospective studies are also needed to further assess the safety, efficacy, and long-term impact of MAPO in this complex patient group.
Looking ahead, future research should prioritize prospective multicenter trials with larger sample sizes and longer follow-up to confirm the long-term safety and efficacy of MAPO. Equally important is the development and validation of neuromuscular scoliosis–specific patient-reported outcome measures, which could better capture clinically relevant aspects such as seated balance, pressure relief, and caregiver dependence. Such efforts will further refine surgical decision-making and improve outcome assessment in this complex patient population.
Conclusion
This study demonstrates that MAPO is an effective surgical strategy for selected patients with neuromuscular scoliosis, offering improved spinal alignment and enhanced patient-reported outcomes without resorting to higher-grade osteotomies. By balancing surgical efficacy and invasiveness, MAPO represents a valuable option in managing the complex spinal deformities of NMS. Nonetheless, careful patient selection and comprehensive perioperative management remain crucial. Further prospective, large-scale studies are warranted to validate its long-term benefits and to guide the development of disease-specific outcome measures tailored to the unique needs of the NMS population.
Footnotes
Ethical Approval
This study adhered to ethical guidelines and was approved by the Beijing Chaoyang Hospital Institutional Review Board. Informed consent was obtained from all patients prior to the use of their medical records for research purposes. All data were anoymized by removing names, identification numbers and other direct identifiers, and each case was assigned a unique study code to ensure patient condifentiality.
Consent for Publication
Consent to publish images that may potentially include identifiable human faces was obtained from the individuals or their legal guardians, ensuring compliance with applicable ethical standards.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the National Key Research and Development Program of China (Grant No. 2022YFC2407206) and Beijing Municipal Health Commission (BJRITO-RDP).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No datasets were generated or analysed during the current study.