
Abstract

We thank the authors for their thoughtful and constructive comments regarding our study. 1 Their remarks highlight important considerations in interpreting rod fracture (RF) risk and its biological underpinnings.
Pseudarthrosis and Multivariate Modeling
We fully agree that pseudarthrosis possibly represents a major contributor to mechanical construct failure. However, we would like to clarify that our study did not aim to evaluate pseudarthrosis as a predictive factor, since standardized postoperative CT imaging was not available for asymptomatic patients. Including this variable in multivariate analysis would have introduced significant ascertainment bias due to nonuniform imaging.
Additional Analysis of Predictors of RF in Adult Spinal Deformity
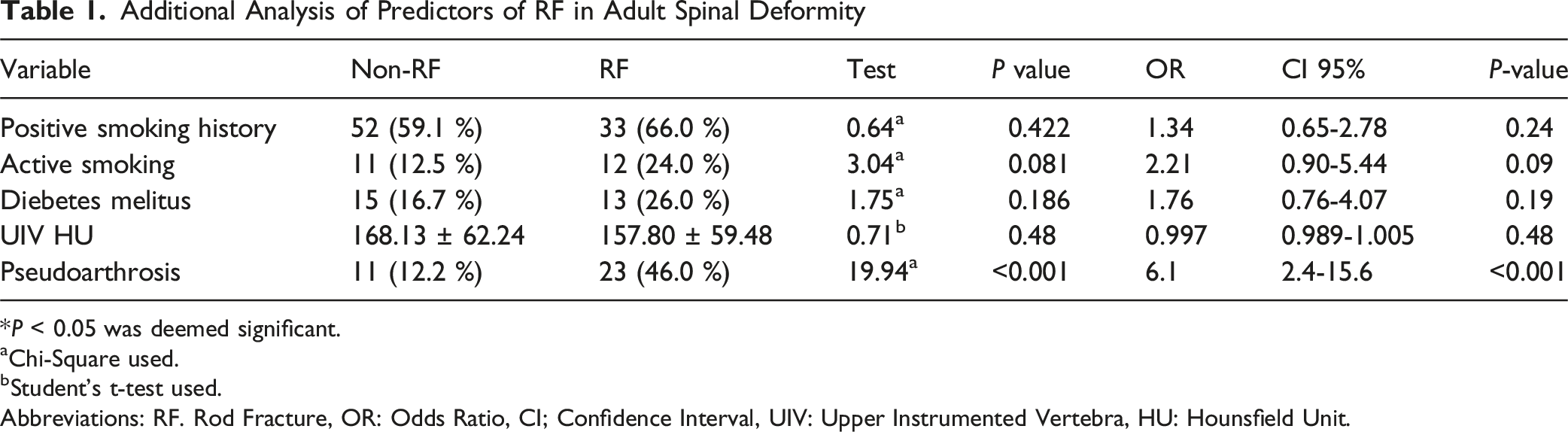
*P < 0.05 was deemed significant.
aChi-Square used.
bStudent’s t-test used.
Abbreviations: RF. Rod Fracture, OR: Odds Ratio, CI; Confidence Interval, UIV: Upper Instrumented Vertebra, HU: Hounsfield Unit.
Unfortunately, the absence of standardized postoperative CT evaluation is a common limitation among retrospective studies, as intermittent CT imaging is not routinely included in the standard postoperative management of adult deformity surgery. With this study, we aim to provide an incentive for future prospective investigations incorporating systematic fusion assessment to better delineate the interplay between fusion biology, construct design, and RF risk.
Anterior Column Manipulation and Biological Factors
We acknowledge that anterior lumbar interbody fusion and anterior column realignment may influence RF risk both mechanically and biologically. Even after controlling for sagittal correction and construct design, these procedures may impose additional stress on posterior instrumentation. Upon further review of our data, both positive smoking history and active smoking were comparable between groups (positive smoking history: 59.1 % vs 66.0 %, OR = 1.34, 95 % CI 0.65-2.78, P = 0.42; active smoking: 12.5 % vs 24.0 %, OR = 2.21, 95 % CI 0.90-5.44, P = 0.09). While these differences did not reach statistical significance, we acknowledge a positive trend toward higher rates of active smoking in the RF group. Similarly, diabetes prevalence showed no significant difference (16.7 % vs 26.0 %, OR = 1.76, 95 % CI 0.76-4.07, P = 0.19). While DEXA scan results were not available for all patients, we conducted preoperative CT-based Hounsfield unit (HU) analyses of the upper instrumented vertebrae to assess bone density and potential junctional failure risk. The vertebral body HU has been shown to serve as a surrogate marker for bone density,6,7 and values were overall comparable between both groups (168.13 ± 62.24 vs 157.80 ± 59.48, OR = 0.997, 95 % CI 0.989-1.005), indicating similar bone quality (Table 1). These findings support the conclusion that comorbidities and bone health were largely balanced in our study. However, while not fully evident in our study, we recognize that intrinsic variability in fusion biology and tissue healing likely underlies the complex and multifactorial nature of RF.
Fracture Localization and Construct Geometry
Assessment of the exact position of each fracture was unfortunately not logistically feasible in our cohort. However, we emphasized that the observed reduction in RF risk with multi-rod constructs is likely attributable to their intended effect on load distribution across the construct. We thank the authors for raising this point and fully agree that further detailed analyses, including finite-element modeling and advanced imaging, would be valuable to confirm and expand upon these findings.
Terminology Regarding Opioid Use
We appreciate the clarification regarding the use of the term “dependency.” Our analysis measured duration of postoperative opioid use rather than clinical dependence. The phrase “continued opioid use” more accurately describes the variable and will be used in future reports.
In summary, we thank the authors for their collegial and insightful feedback. Their remarks underscore critical aspects, including pseudarthrosis, smoking, diabetes, and bone health, that complement and reinforce the broader context of our findings and enrich the discussion. We agree that advancing this field will depend on standardized fusion assessment, comprehensive bone quality evaluation, and well-designed prospective studies to refine the understanding of RF mechanisms in adult spinal deformity surgery.