
Abstract
Study Design
Comparative study.
Objectives
To compare the racial and ethnic representation of study participants in primary literature used to develop North American Spine Society (NASS) appropriate use criteria (AUCs) relative to their prevalence in the United States (US) population.
Methods
Primary literature used for the development of NASS AUCs for cervical fusion and degenerative spondylolisthesis were analyzed. Demographic characteristics of study participants were extracted and compared to their prevalence in the US population via participation-to-prevalence ratios (PPRs). A PPR of 0.8-1.2 indicated equivalent representation while a PPR <0.8 and >1.2 was considered underrepresentation and overrepresentation, respectively.
Results
There were 215 793 study participants available for demographic analysis. Most studies reported sex (38/42, 90%), but fewer studies reported race (11/42, 26%) and ethnicity (8/42, 21%). Male (PPR = 1.01, 95% CI: 0.92-1.11) and female (PPR = 0.98, 95% CI: 0.89-1.07) study participants had equivalent representation in NASS AUCs relative to their prevalence in the US population. White (PPR = 1.38, 95% CI: 1.35-1.41) and Native Hawaiian/Pacific Islander (PPR = 1.86, 95% CI: 0.42.-3.30) study participants were overrepresented, while American Indian/Alaskan Natives (PPR = 1.08, 95% CI: 0.35-1.81) were found to have equivalent representation. There was underrepresentation of Black (PPR = 0.78, 95% CI: 0.55-0.99), Hispanic (PPR = 0.25, 95% CI: 0.24-0.26) and Asian (PPR = 0.32, 95% CI: 0.01-0.63) study participants.
Conclusions
There is limited representation of racial and ethnic minorities in NASS AUCs for degenerative spine conditions, which may limit the translatability of these clinical guidelines to underrepresented groups. Future work is needed to improve racial and ethnic minority representation in clinical spine surgery research.
Keywords
Introduction
Degenerative spine disorders account for a significant percentage of United States (US) healthcare expenditure. 1 The surgical management of cervical and lumbar spinal disorders is especially costly in the US. 2 Previous literature has also highlighted variability in the treatment for these disorders, which may lead to unnecessary treatment and increased healthcare costs.3-5 As such, the North American Spine Society (NASS) has created appropriate use criteria (AUC) to guide clinical decision making for cervical fusion and degenerative spondylolisthesis.6,7
NASS AUCs were developed after comprehensive literature searches of high level-of-evidence studies in relevant topics along with the construction of common clinical scenarios for these degenerative spine conditions. Recommendations provided in NASS AUCs were developed through expert consensus, which were dependent on the available clinical evidence combined with the clinical experience of a balanced panel of raters. These recommendations serve to inform clinical decision-making in the management of degenerative spinal disorders both in the US and abroad. As such, it remains critical to understand the generalizability of these evidence-based clinical practice guidelines to increasingly diverse patient populations in the US.8,9
Thus, the purpose of this study was to determine the representation of racial and ethnic minorities within NASS AUCs for degenerative spine conditions. Based on previous research, 8 we hypothesized that racial and ethnic minorities would be underrepresented in clinical research informing NASS AUCs for cervical fusion and degenerative spondylolisthesis relative to their prevalence in the US population.
Materials And Methods
This study qualified for review exemption status based on the policies of the Institutional Review Board, as such informed consent was not required. We analyzed primary literature sources used to inform published NASS AUCs available as of July 1, 2024. This included AUCs for cervical fusion and degenerative spondylolisthesis.6,7 All cited references were analyzed for study inclusion eligibility, which required primary clinical research studies performed in the US.
Full-text journal articles were analyzed for study characteristics including presence of demographic reporting, geographic location, year of publication, journal title, funding source, and number of US patients. We utilized US federal reporting standards with regards to categories for race and ethnicity from the Office of Management and Budget (OMB). 10 OMB race categories included White, Black, Asian, American Indian/Alaska Native (AI/AN), and Native Hawaiian/Pacific Islander (NH/PI). A separate category of Other was used to account for any studies that reported Other as a race category. Non-OMB race categories consisted of White and non-White to account for the studies that did not report race according to OMB standards. Associations between race reporting method (OMB vs non-OMB) and study characteristics, including funding status (funded vs not funded), NASS AUC classification (cervical fusion vs degenerative spondylolisthesis), and level of evidence (I vs II/III), were assessed as a sensitivity analysis using Fisher’s exact test as appropriate based on cell counts. Categories for ethnicity included Hispanic/Latino and non-Hispanic/Latino. Separately, we also classified enrolled study participants into sex categories of male and female.
Participation-to-prevalence ratios (PPRs) were calculated for each demographic group present in primary spine surgery literature sources relative to their prevalence in the US population. In addition to overall PPR calculations, we separately analyzed PPRs for the subset of studies that reported race using OMB categories, which included NH/PI, AI/AN, Black, Asian, and White participants. This separate analysis ensured standardization in racial categorization and enabled accurate comparison to US Census data. Calculation of PPRs permitted the assessment of demographic representation in referenced spine literature relative to their prevalence in the US population. 11 The PPR numerator (ie, participation) was defined as demographic representation in the NASS AUCs according to referenced spine literature. The PPR denominator (ie, prevalence) was defined as demographic representation in the US population according to the 2020 US Census. 12 A PPR of 0.8-1.2 was defined as equivalent representation. Underrepresentation was defined as a PPR <0.8 while overrepresentation was defined as a PPR >1.2. Studies that did not report race or ethnicity were excluded from the respective PPR calculations, as imputing demographic data was not feasible given the heterogeneity and limited reporting across studies. This approach ensured that PPR estimates were based on reported data only.
The primary outcomes of interest were the proportion of primary literature sources with demographic reporting and PPRs for each demographic category. Descriptive statistics were employed for study characteristics. Comparisons in demographic representation between NASS AUCs were made with chi square tests. All statistical tests were performed on GraphPad 9 (Prism, Washington, D.C.) in consultation with a biostatistician and considered significant if P < 0.05.
Results
Characteristics of Clinical Studies Used to Inform North American Spine Society Appropriate Use Criteria (AUC)
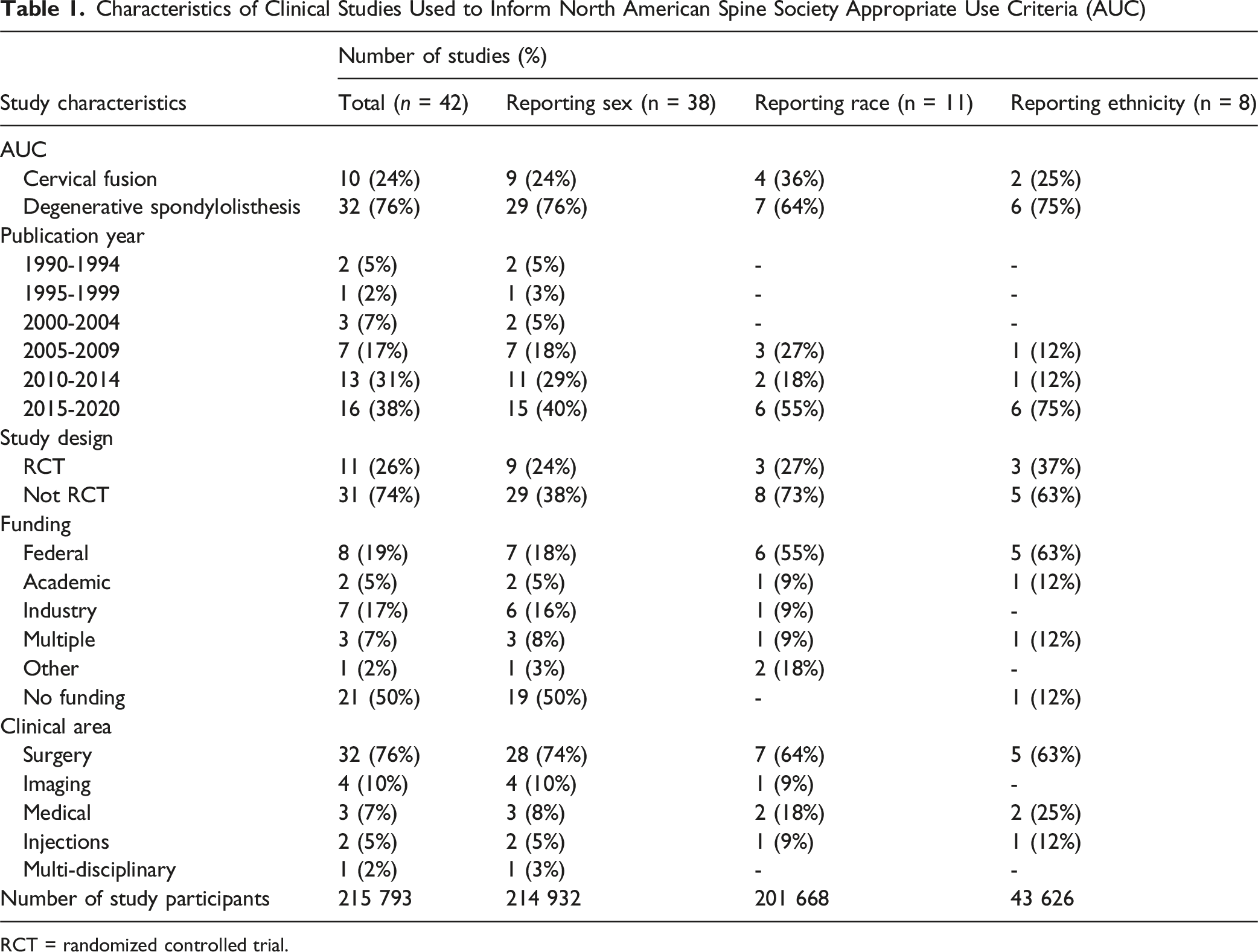
RCT = randomized controlled trial.
Clinical Studies With Race and Ethnicity Reporting Used to Inform North American Spine Society Appropriate Use Criteria (AUC)
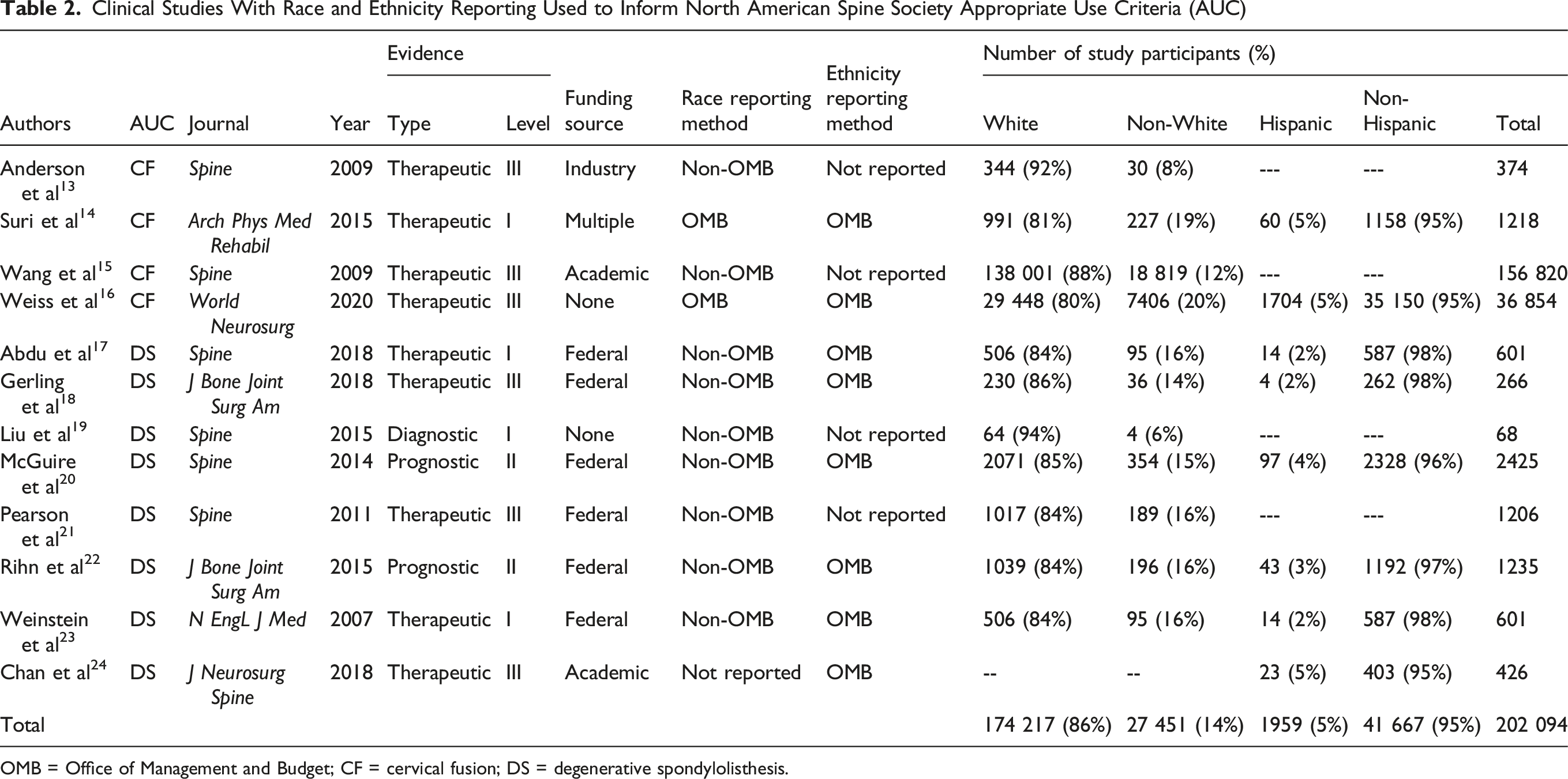
OMB = Office of Management and Budget; CF = cervical fusion; DS = degenerative spondylolisthesis.
Clinical Studies With OMB Race and Ethnicity Reporting Used to Inform North American Spine Society Appropriate Use Criteria (AUC)

OMB = Office of Management and Budget.
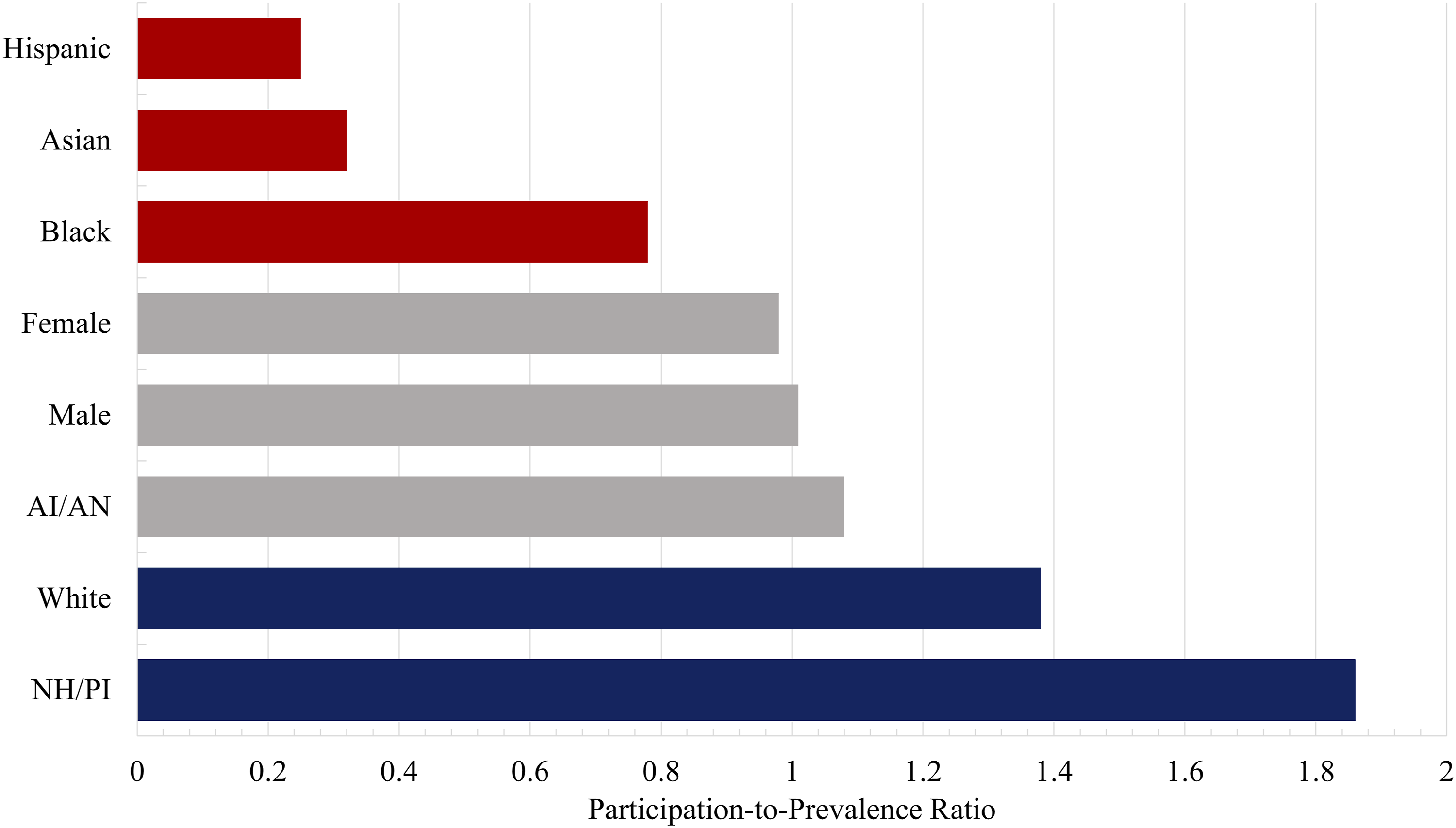
Participation-To-Prevalence Ratios for Demographic Diversity in Clinical Studies Used to Inform North American Spine Society Appropriate Use Criteria (AUC) American Indian/Alaska Native (AI/AN), and Native Hawaiian/Pacific Islander (NH/PI)
Clinical Studies With Non-OMB Race and Ethnicity Reporting Used to Inform North American Spine Society Appropriate Use Criteria (AUC)
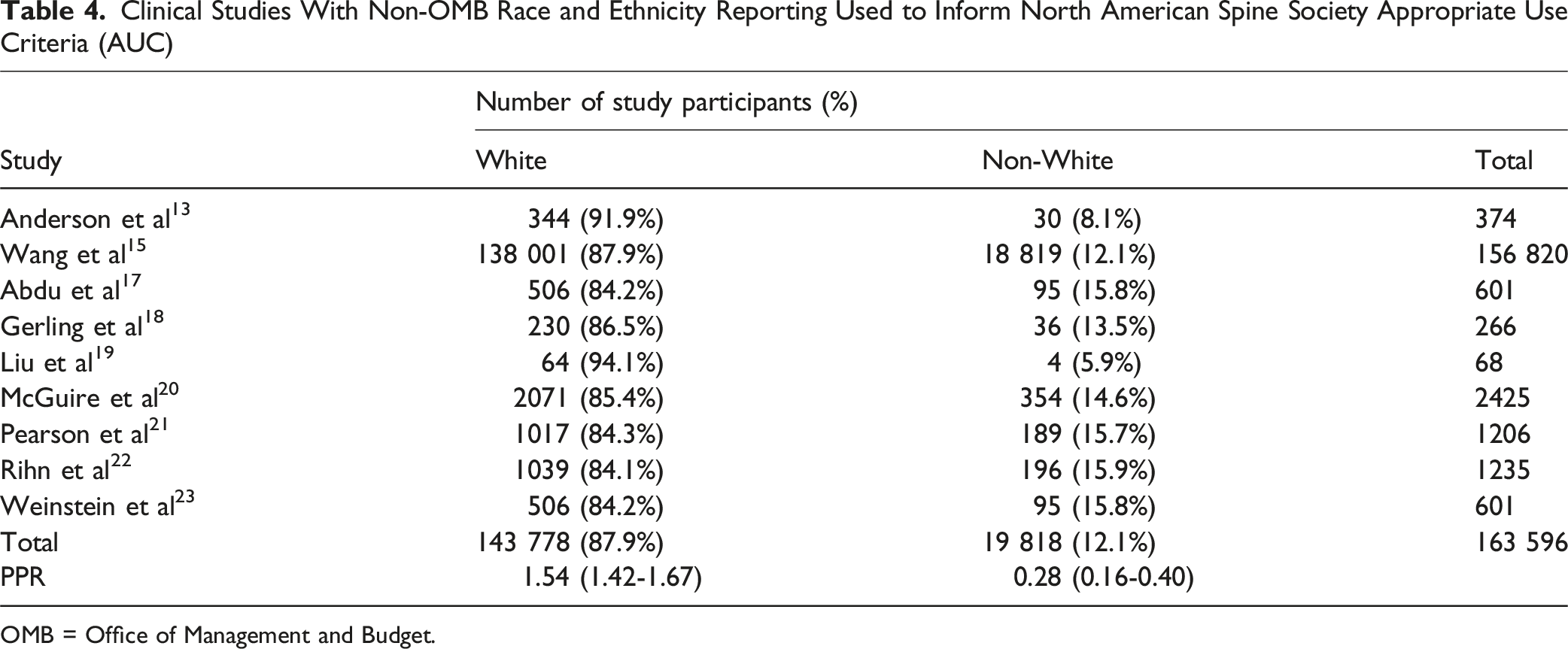
OMB = Office of Management and Budget.
Discussion
In this study, we demonstrated that racial and ethnic minority groups are underrepresented in clinical research studies used to inform NASS AUCs for cervical fusion and lumbar spondylolisthesis. While most studies reported sex, the reporting of race and ethnicity was inconsistent among clinical studies used to inform NASS AUCs. Black, Asian, and Hispanic representation was limited relative to their prevalence in the US population. Overall, these findings highlight a persistent lack of demographic reporting and adequate sampling of racial and ethnic minorities in spine surgery research. This underrepresentation may weaken the clinical evidence base for spine surgery and challenges the overall external validity and translatability of NASS AUCs to diverse patient populations in the US. The underlying causes for this underrepresentation remain unknown but may stem from a lack of awareness in the academic community, reticence of racial and ethnic minority groups to engage in clinical research, and other logistical barriers to conducting high-quality, representative clinical research in the US. Future opportunities may exist to further engage key stakeholders across the spine surgery community including academic journals, institutional review boards, principal study investigators, research funding agencies, and professional spine societies to increase the representation of racial and ethnic minority groups in spine surgery research and their derivatives including NASS AUCs.
The translatability of findings from clinical research is predicated on the equitable representation of diverse patient populations used in those clinical studies. 25 Widening musculoskeletal health disparities in the US require a careful understanding of how the presentation and management of spine disorders differ across racial and ethnic minority populations in the US. 26 Equitable participation in clinical research is critical to improve the quality of clinical evidence derived from these studies, which may also serve to address musculoskeletal health disparities experienced by minority patient populations in the US. 27 Increased awareness regarding the need to enhance racial and ethnic representation among study participants is necessary to overcome current limitations in clinical trials for spine surgery. 28 Institutional review boards should mandate the provision of strategies in clinical research proposals that serve to promote diversity, equity, and inclusion among study participants. 29 Furthermore, editors and peer-reviewers of spine surgery journals should require adequate demographic reporting and sampling in all submitted clinical studies. 30 Federal standards for racial and ethnic reporting as established by the OMB should be followed in future clinical studies in spine surgery. Principal investigators should make concerted efforts to recruit racial and ethnic minority participants into spine clinical trials while recognizing the unique recruitment challenges presented by these patient populations. 31 Appropriate sub-analyses of racial and ethnic minority groups should be required of all manuscripts, which should also control for other social determinants of health. 32 Similarly, research grant funding agencies, including those from spine surgery societies should require the inclusion of demographic reporting and adequate demographic sampling in future grant proposals with comprehensive plans to ensure the inclusion of diverse study participants.
Several additional strategies could be explored to increase the representation of racial and ethnic minorities into clinical research for spine surgery. Committee members of future NASS AUCs should carefully consider the limitations inherent in clinical studies that do not report demographic data of study participants. Previous literature has highlighted racial and ethnic differences in perceived pain, disability, and clinical outcomes among patients undergoing cervical and lumbar spine surgeries.33,34 Differences in perceived pain may influence patient reported outcomes, which in turn may lead to unique considerations in the early post-operative period for racial and ethnic minority patients. 35 These disparities can translate into differences in morbidity and mortality following spine surgery among racial and ethnic minorities. 36 These racial and ethnic disparities are not only limited to clinical outcomes following spine surgery, as racial and ethnic minorities also experience barriers to equitable access to spine care in the US.37-39 These obstacles may serve to further widen musculoskeletal healthcare disparities. Left unaddressed, the underrepresentation of racial and ethnic minority populations in NASS AUCs risks perpetuating these health disparities in spine care experienced by racial and ethnic minority patients. The overall lack of demographic reporting and inclusion of diverse patient populations in spine surgery research may ultimately undermine the ability of the spine surgery community to address these disparities.
Additional strategies should be considered to improve the representation of racial and ethnic minorities in spine surgery research. Journal editorial boards should revise author guidelines to require standardized reporting of race and ethnicity in accordance with federal recommendations, such as those from the OMB. Peer reviewers should be trained to assess demographic reporting and evaluate the adequacy of representation among study participants. Collaboration between spine surgery societies and professional organizations may help facilitate the development of infrastructure to support multi-center recruitment of underrepresented patient populations. These efforts may be further supported through targeted funding mechanisms, research awards, and the formal endorsement of inclusive research practices. Taken together, these measures may help promote greater transparency, accountability, and equity in the generation of clinical evidence used to inform NASS AUCs.
There were several limitations to this study. First, this study only analyzed the first 2 NASS AUCs created, which were for cervical fusion and lumbar spondylolisthesis. More NASS AUCs are forthcoming and results from the present study may help to inform the methodology for future iterations of NASS AUCs. Second, a significant proportion of the clinical evidence base for NASS AUCs did not report race and ethnicity, which limited our sample size. While it remains difficult to draw significant conclusions from a small sample size, it clearly exposes a deficiency in awareness on the importance of demographic reporting in the spine surgery literature. Third, the retrospective study design limited our understanding as to the etiologies for the lack of demographic representation found in our study. Future studies are needed to understand the barriers minority populations experience during inclusion in spine surgery research. The etiologies are likely multifactorial including reticence to engage with clinical research, logistical issues, and a lack of institutional awareness. Understanding these barriers should be the focus of future investigations. Despite these limitations, this study presents important insights into the current state of demographic representation among NASS AUCs and their referenced spine surgery literature.
Conclusion
In summary, there is limited inclusion of racial and ethnic minorities in the clinical evidence base used to inform NASS AUCs for degenerative spine disorders. Overwhelmingly, referenced spine literature underreport and underrecruit racial and ethnic minority populations relative to their prevalence in the US. This phenomenon has persisted over time and may undermine the generalizability and translatability of NASS AUCs to increasing racial and ethnic minority representation in the US. The overall lack of demographic reporting and inclusion may also risk perpetuating musculoskeletal health disparities as it relates to the diagnosis and management of common spinal disorders. Future opportunities may exist to improve demographic reporting and inclusion of minority populations in the primary spine literature. Additional efforts are needed to engage key stakeholders in the academic spine surgery community including study sponsors, journal editors, industry collaborators, federal funding agencies, and principal investigators to promote diversity and inclusion in spine surgery research.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
This study received review exemption based on the policies of the Institutional Review Board