
Abstract
Study Design
Prospective, single-center cadaveric study.
Objectives
To evaluate the accuracy of augmented reality (AR) head-mounted display navigation using a 2D-3D registration method for pedicle screw placement that integrates preoperative CT scans with intraoperative X-ray images, eliminating the need for intraoperative 3D imaging.
Methods
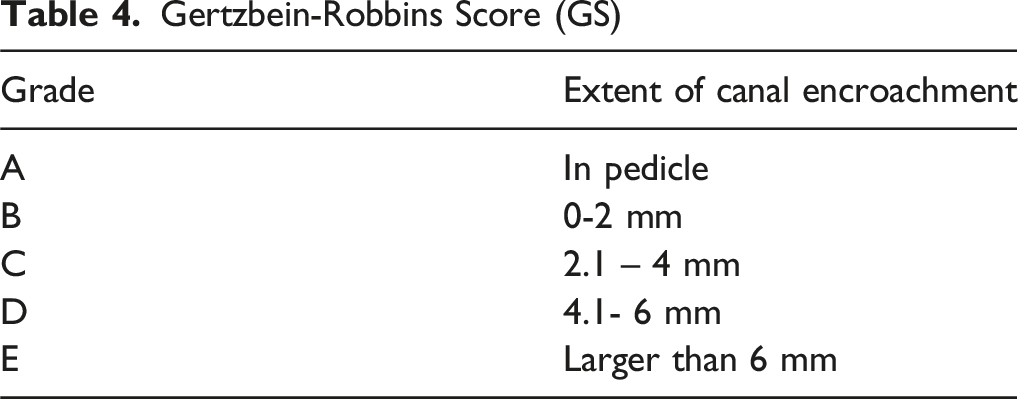
A prospective, single-center cadaveric study was conducted using six human cadaveric specimens. Five board-certified spine surgeons placed 151 pedicle screws across cervical (n = 36), thoracic (n = 54), lumbar (n = 41), and sacroiliac (n = 20) regions using an AR navigation system. The system utilized preoperative CT scans registered with intraoperative X-ray images. Accuracy was assessed stereotactically (angular and translational errors) and clinically (Gertzbein-Robbins and Heary classifications).
Results
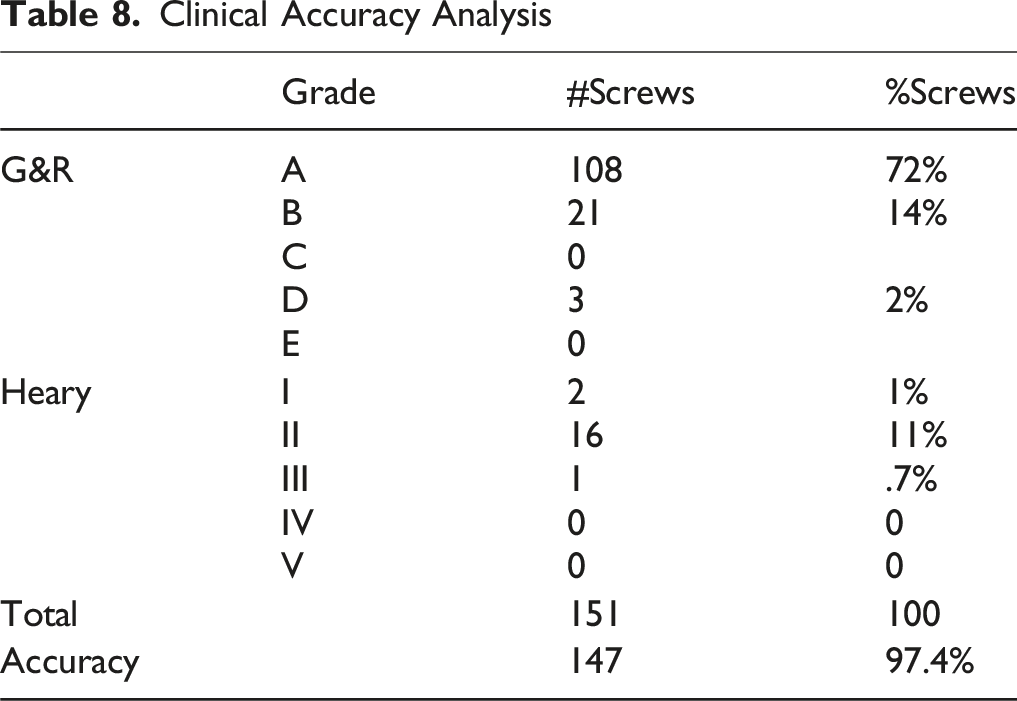
Of 151 pedicle screws placed, 147 (97.4%) were accurately positioned in the “safe zone” (Gertzbein-Robbins grades A/B or Heary classifications I/II). The 99% upper bound limit for angular errors was <3 and translational errors was < 3 mm in both axial and sagittal planes across all vertebral levels.
Conclusions
The 2D-3D registration methodology with AR visualization demonstrates high accuracy for pedicle screw placement comparable to conventional navigation techniques. This approach effectively addresses key limitations of existing navigation paradigms while maintaining high accuracy standards without requiring intraoperative 3D imaging capabilities. AR-assisted navigation with 2D-3D registration represents a promising technological advancement that may enhance the precision and efficiency of spinal instrumentation procedures.
Keywords
Introduction
Pedicle screws are routinely utilized for spinal stabilization and immobilization to augment spinal fusions. Traditionally, these screws are placed via the freehand technique, wherein anatomical landmarks serve as guides for pedicle screw insertion. 1 Although freehand pedicle screw placement has demonstrated high accuracy rates, reported accuracies have varied significantly, with some studies indicating rates as low as 53%-74.9%.2,3 Achieving precise pedicle screw placement is crucial for surgical success, as misplacement increases the risk of significant morbidity. Medial breaches into the spinal canal may lead to neurological deficits due to spinal cord injury, while superior and inferior misplacements involving the interpedicular foramina pose risks to nerve roots.4,5 Additionally, anterolateral perforations can cause potential vascular and visceral complications, affecting structures such as the aorta, major vessels, esophagus, and trachea. 6 To mitigate these risks, multiple navigation methods have been developed, including fluoroscopy-assisted, CT image-guided, and robot-assisted techniques. 7
Among modalities, robotic and CT-based navigation systems have been reported to yield the highest accuracy in pedicle screw placement.8,9 However, using 3D CT image navigation systems for placing screws requires implementing costly intra-operative 3D CT scanner in the operating room. In contrast, C-arm fluoroscopy is the most widely used intraoperative imaging modality, providing rapid and serial visualization of 2D images in real time. Fluoroscopy lacks the 3D spatial resolution required for precise trajectory planning. Biplanar fluoroscopy, involving simultaneous AP and lateral projections, is often required for minimally invasive procedures. 10 However, these 2D C-arm images do not provide the comprehensive 3D anatomic information needed for optimal trajectory planning, making trajectory accuracy more challenging. Thus, integrating 3D CT data with intraoperative Xray imaging, referred to as the 2D-3D registration method, could enhance navigation accuracy without necessitating an intraoperative 3D CT scanner.
Despite the advantages of robotic and CT-guided navigation, several challenges remain, including line-of-sight interruptions, steep learning curves, and limited flexibility in robotic systems relative to surgeon intuition and control.11,12 To address these limitations, augmented reality head-mounted displays (AR-HMDs) have been introduced as a novel approach to intraoperative navigation. AR-HMDs offer the potential to overcome conventional navigation limitations by overlaying real-time surgical navigation data directly onto the operator’s field of view, thereby reducing attention shifts and improving procedural efficiency. 1
In this study, we present a cadaveric evaluation of AR-HMD-based image-guided navigation utilizing the 2D-3D registration method, which integrates preoperative 3D CT scans with intraoperative 2D X-ray images. This approach eliminates the necessity for intraoperative 3D CT imaging, potentially making advanced navigation more accessible in a broader range of surgical settings. The primary objective of this study is to evaluate the accuracy of pedicle screw placement using AR-HMD navigation and validate the use of 2D-3D registration.
Methods
Cadaveric Trial Design
The study was conducted in compliance with the ethical guidelines for human cadaver studies at Augmedics headquarters (Chicago, Illinois). A prospective, single-center cadaveric study was conducted for evaluating pedicle screw placement accuracy utilizing the 2D-3D registration method for an AR navigation system. The AR navigation system utilized during the study was established by Augmedics (xvision, Augmedics Ltd) and has been validated in similar studies using intraoperative CT registration method.
13
The 2D3D registration method is a spinal navigation technique that aligns intraoperative X-ray images with preoperative 3D CT scans to enable accurate instrument guidance. This is achieved by capturing intraoperative X-rays and comparing geometric parameters such as distance, image center, and distortion between a C-arm ring adaptor and a fixed C-marker placed on the cadaver (Figure 1). (A) Cadaver Study Set-Up including C-Arm Augmedics XVS System and a Cadaver on an OR-Table. (B) The C-Arm Ring Adapter is Reusable and Fixated to 12″ or 9″ Round C-Arm’s X-Ray Image Intensifier. The Double Plate Ring Adapter Enables the Calculation of Different X-Ray Parameters Such as Distance Between the X-Ray Emitter and Detector, Image Center and Image Distortion, which are Required as Part of the 2D-3D Registration Process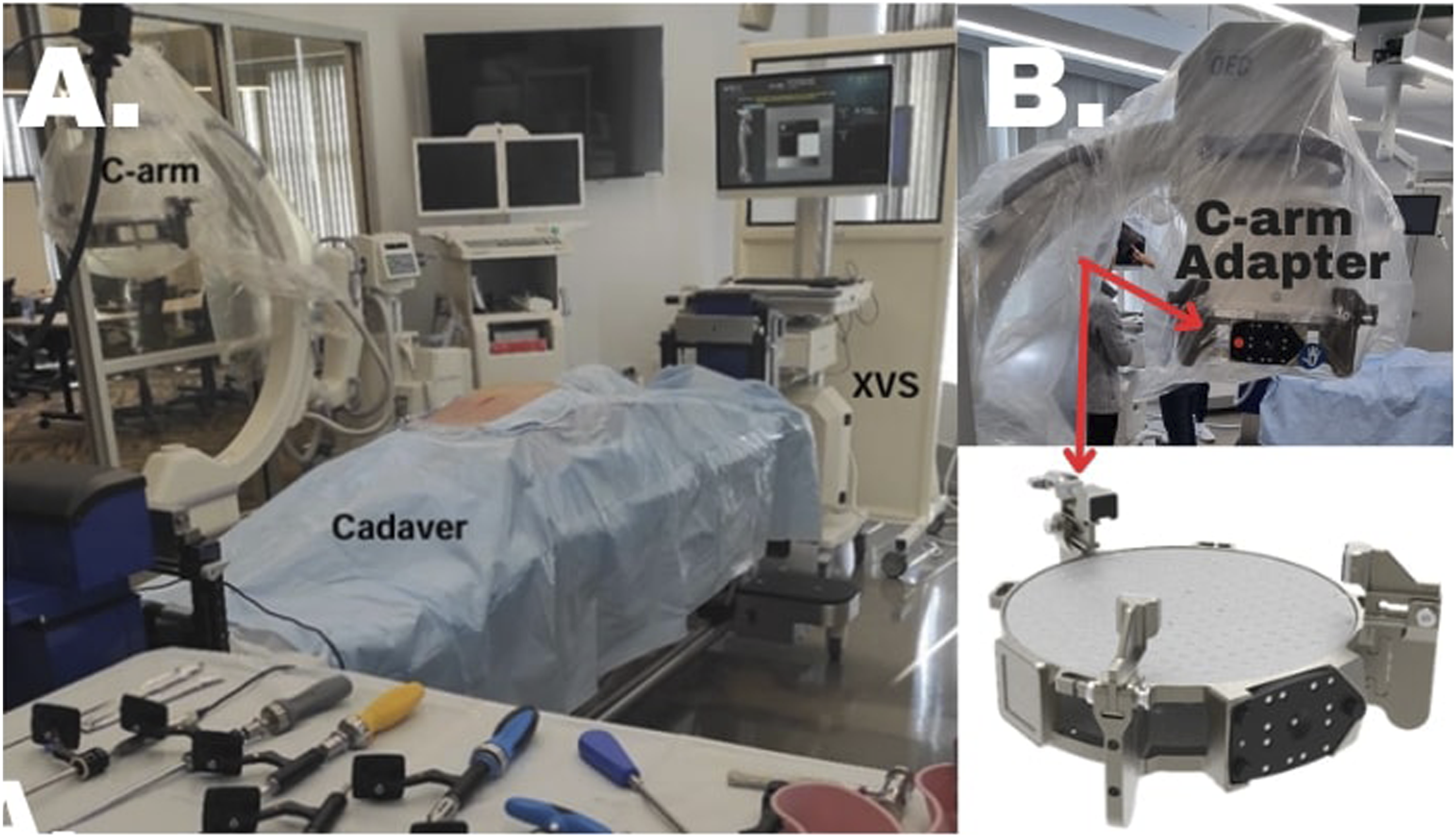
Six complete human cadaveric torsos (5 males, 1 female) were procured for the investigation. No specimens had history of previous spine surgery or significant anatomical deformity that would interfere with standard instrumentation techniques.
Surgeon’s Information

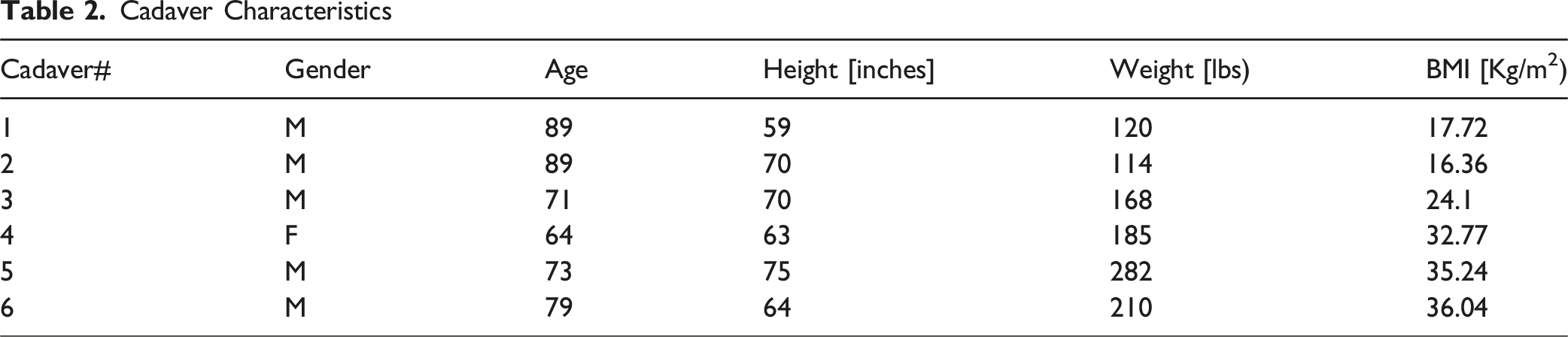
Cadaver Characteristics
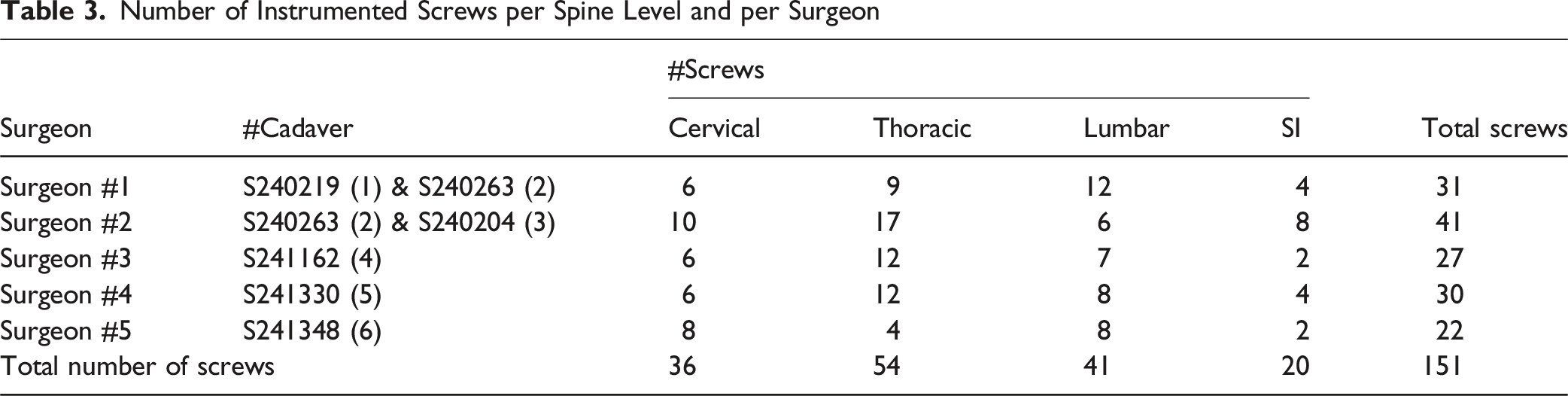
Number of Instrumented Screws per Spine Level and per Surgeon
Each human cadaver was placed supine on an OR table and then scanned pre-operatively using a CT scanner (Siemens Somatom Persepctive CT Scanner) with parameters set to bone setting and with 1 mm slicing and spacing. Pedicles were measured from these scans to guide optimal pedicle screw selection.
Registration Method & Pedicle Screw Navigation Method
The xvision-Spine System (XVS) was utilized for this investigation. The AR navigation platform consists of a head-mounted display (HMD) with eye projection technology that superimposes navigation information directly into the surgeon’s visual field which allows for real-time navigation.
The operating surgeon wore the AR headset continuously throughout all 151 pedicle screw trajectories, consistent with practices reported in similar cadaveric and early clinical series utilizing comparable AR systems. Minor practical challenges were noted but did not interrupt procedures: users reported mild neck fatigue after approximately 60 minutes of continuous headset use, aligning with ergonomic considerations commonly associated with head-mounted AR devices. Importantly, no surgeon needed to remove the headset or pause the procedure due to discomfort or visibility concerns. Additionally, the system’s tracking latency was consistently under 34 ms (as per the manufacturer’s specifications), making latency imperceptible during guidewire insertion. Simple intraoperative adjustments, such as tightening the headset retention strap, further optimized comfort without compromising sterility or workflow.
The 2D3D registration methodology employs an approach integrating pre-operative CT data with intra-operative Xray imaging. Pre-operative 3D CT scans were taken of all cadaver specimens. Pedicle thickness was measured in advance and optimally sized screws were selected. A patient marker was attached to the cadaver’s anatomy using a spinous process clamp and/or percutaneous iliac pin, serving as a reference frame for system. A C-arm ring adapter was utilized for acquiring two intra-operative X-ray images. Registration between the 3D pre-operative CT scan and Intra-operative Xray was performed, and the virtual model was created and visually overlayed in the HMD via the XVS system (Figures 1A and B).
Following registration, instrumentation was performed either open or percutaneously/minimally invasive, per surgeon’s discretion. A landmark check was used prior to each instrumentation. Each surgeon placed screws in different spine segments (cervical, thoracic, lumbar, and sacroiliac). Entry point selection was guided by AR XVS navigation display with visualization of both axial and sagittal trajectories (Figure 2). At the end of the instrumentation of each cadaver, a 3D post-op scan was performed to enable off-line evaluation of the positioning of the screws. Augmedics XVS System Guiding Pedicle Screw Placement With Real-Time 3D Navigation. Sagittal and Axial Views Show Alignment of Virtual and Actual Trajectories at Thoracic Levels
Accuracy & Clinical Analysis
Gertzbein-Robbins Score (GS)
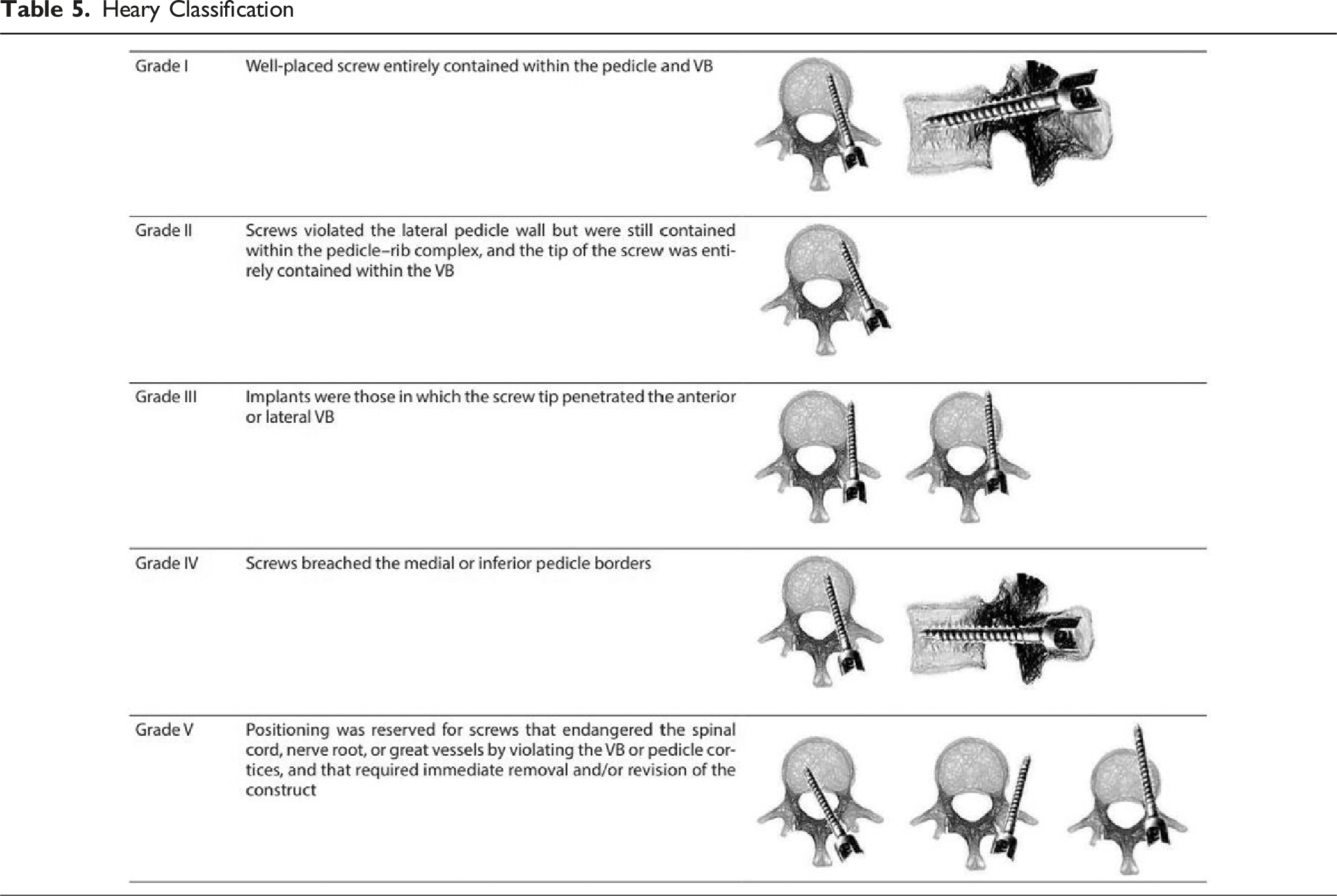
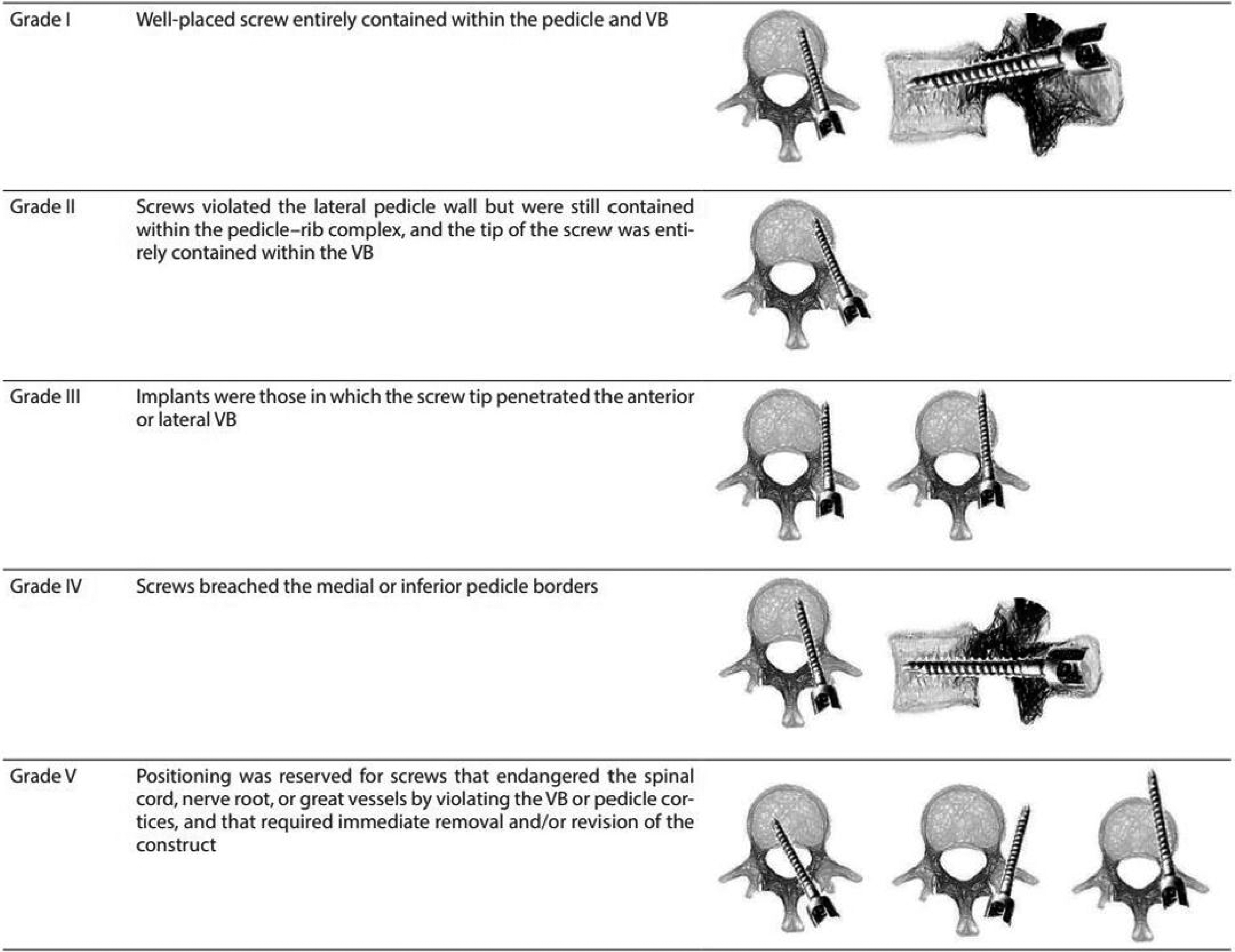
Heary Classification
Stereotactic Accuracy Analysis
The absolute navigation precision was quantified by comparing final screw positions on postoperative CT images with virtual screw trajectories recorded during navigation. Measurements were performed using 3D slicer software and errors were calculated in both angular and sagittal planes. Anatomical reference lines were established in both planes. The axial virtual screw angle is the angle between the virtual screw axis and the anatomical line (β, Figure 3A). The axial post-operative screw angle is defined as the angle made by the positioned screw axis with the anatomical line (β1, Figure 3C). The angular error in the axial plane was then computed as the difference between the two angles (β1- β). The sagittal angular error was calculated utilizing the same method except with the vertebral body acting as the anatomical line (Figure 3B and D). Measurement of Translational and Angular Errors in the Axial (A + C) and Sagittal (B + D) Planes. Comparison is Made Between Intraoperative Navigation Images of Virtual Screw (Blue Line in A + B), and Final Screw Position on Postoperative CT (C + D). Examples of Recommended Anatomical Lines are Drawn in White: Axial Plane (A + C) - Mid-sagittal Line (Bisecting the Vertebral Body); Sagittal Plane (B + D) - Along the Superior Endplate. Translational Error is Computed as (d1−d); Angular Error is Computed as (β1− β)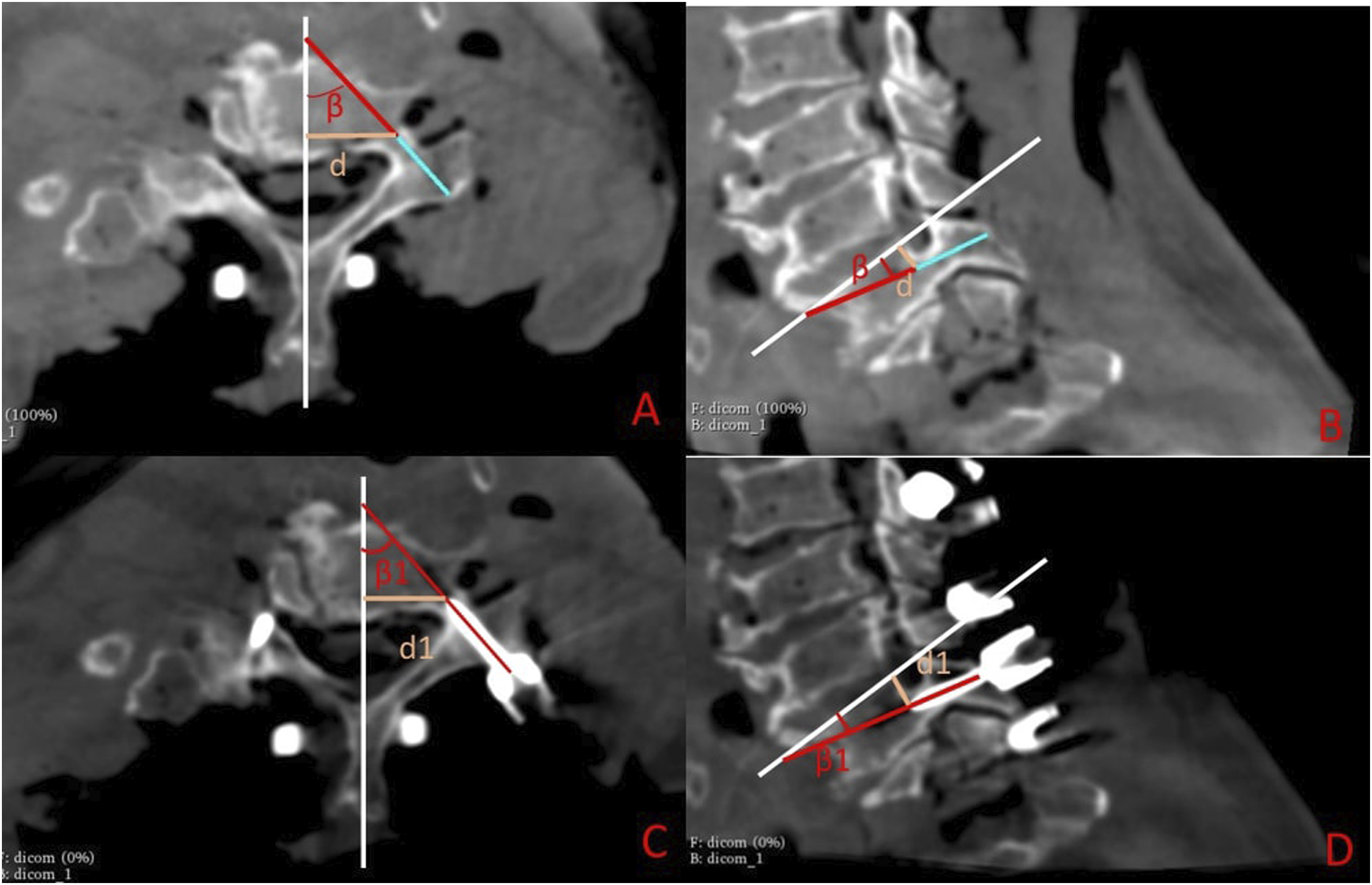
Our study also calculated translational error by measuring a perpendicular line between the tip of the virtual screw and the anatomical line in the axial plane (d, Figure 3A). Similarly, a perpendicular line between the tip of the positioned screw and the anatomical line was drawn and denoted as “d1” (Figure 1C). The translational error in the axial plane was computed as the difference between the lengths of these two lines: (d1-d). The calculation of the translational error in the sagittal plane was done similarly, relative to the relevant anatomical line.
Clinical Accuracy Analysis
The clinical accuracy of screw placement was evaluated by analyzing postoperative CT scans by 2 independent US board certified radiologists. In case of disagreement between the two radiologists, a third radiologist was requested to provide the assessment. Accuracy was calculated as the number of screws graded A and B or I and II according to the G&R and Heary scales respectively, divided by the total number of screws placed (percentage).
Results
Cadaver Demographics and Surgeon Information
A total of 151 pedicle screws were inserted across six cadaveric by five surgeons. The surgeons had an average of 14 years’ experience, ranging from 9-33 years (Table 1). They also had an average of 2.7 years’ experience with navigation systems, ranging from 1-4 years. There was no significant performance difference observed between the different surgeons with varied years of experience with navigation systems. There were 5 male and 1 female cadavers, with an average age of 77.5, average height of 66.8 inches and mean BMI of 27.1 Kg/m2 (Table 2).
Accuracy Analysis
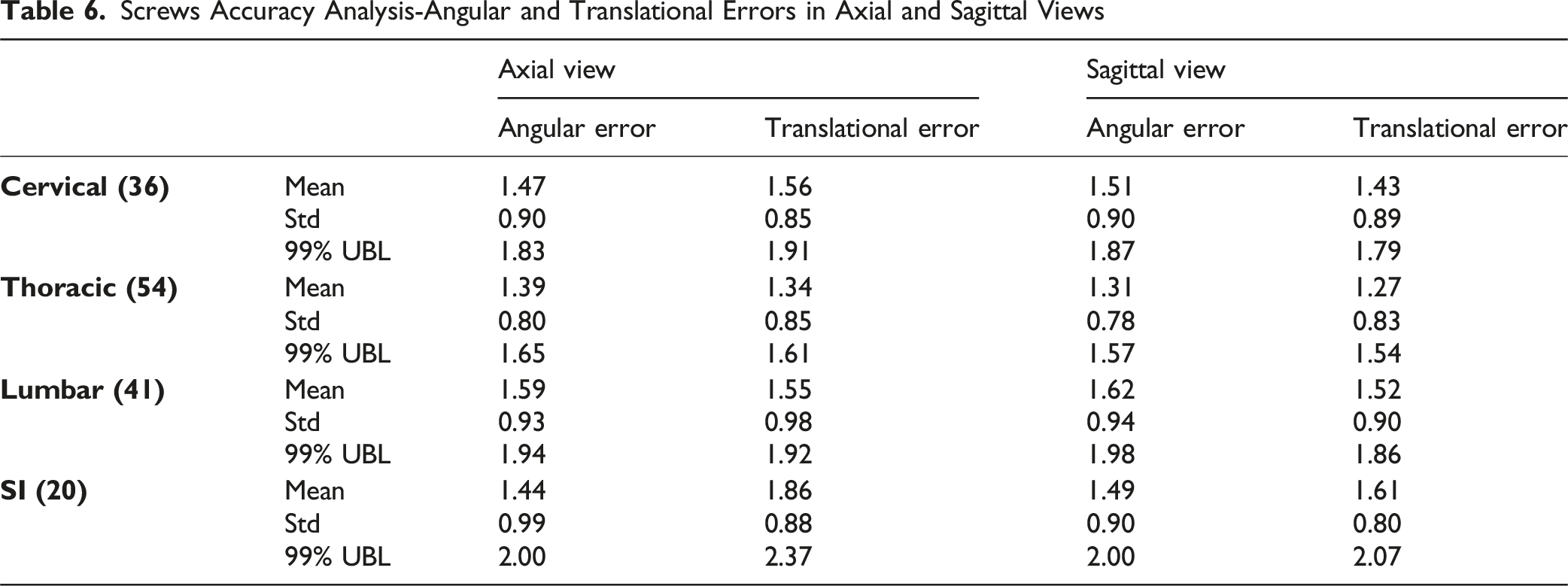
Screws Accuracy Analysis-Angular and Translational Errors in Axial and Sagittal Views
Overall XVS Accuracy Results

Clinical Accuracy Analysis
Discussion
Spinal Surgery Navigation and 2D3D Registration
The progression from conventional freehand technique to computer-navigated and robotic-assisted pedicle screw placement represents a significant evolution in spine surgery.8,14 The many iterations of this technology has improved pedicle screw insertion accuracy and patient safety.12,14 Despite these advancements, the current navigation systems have inherent limitations, including attention shift, line-of sight interruptions and procedural inflexibility.15,16 Our assessment of pedicle screw accuracy using the novel 2D3D method with AR potentially addresses these limitations while maintaining high accuracy. This technological interaction of registration technology may have important implications for clinical practice and future technological development.
Recent literature demonstrates substantial methodological advancement in registration techniques with varied surgical applications and approaches within spine surgery. Elmi-Terander et al, 17 pioneered an augmented reality system utilizing intraoperative cone-beam CT and optical tracking, achieving 94.1% accuracy in pedicle screw placement. Khan et al (2022) evaluated robotic registration systems to achieve 98.3% accuracy with intraoperative CT-guided trajectory planning. 18 Burström et al 19 (2019) introduced optical tracking methodologies with comparable accuracy metrics but varied implementation approaches. Liebmann et al, 20 demonstrate in ex-vivo surgery that specialized cameras that capture depth and color can accurately and efficiently reconstruct 3D anatomical structures. Collectively, these studies demonstrate advancement in registration and navigation-with improvements in accuracy, reduced radiation exposure and overall surgical workflow. The 2D3D registration method provides an alternative solution by utilizing pre-operative CT datasets registered with intra-operative x-rays and providing comparable accuracy without requiring intra-operative 3D imaging acquisition.
The broader literature shows that modern AR navigation can now rival top-tier robotic platforms. A large clinical series of more than 200 patients demonstrated 99.1 % Grade A/B accuracy with head-mounted AR, virtually indistinguishable from the 99.6 % achieved with robotic assistance in the same setting. Similarly, a cadaveric comparison of stereoscopic projector-based AR vs a leading robotic system recorded mean positional errors of 1.1 mm and 1.3 mm, respectively. Our own proof-of-concept (151 trajectories, 98.7 % Grade A/B) therefore falls squarely within this high-accuracy range while avoiding the capital cost, floor-space footprint, and setup time inherent to robotic solutions—highlighting the practical advantages of frameless 2D–3D registration delivered through a lightweight head-mounted display.
The most directly comparable methodology to ours was conducted by Khan et al, who demonstrated 98.1% accuracy (Gertzbein-Robbins grade A) using CT-to-fluoroscopy registration for robotic-assisted pedicle screw placement. 18 The current study demonstrates comparable results (98.1 % compared to 97.4% accuracy rates) to these established techniques while addressing interface limitations through intra-operative X ray imaging and augmented reality visualization.
Technical Differentiation and Clinical Implications
The primary innovation of our 2D-3D registration approach resides in its capacity to accurately merge preoperative CT datasets with intraoperative Xray imaging while providing direct retinal projection to the surgeon via augmented reality. This methodology offers several significant advantages over conventional navigation paradigms. First, the system eliminates the capital investment requirements for intraoperative 3D imaging capabilities, as the registration algorithm effectively correlates preoperative CT data with standard Xray images accessible in most surgical facilities. This represents a substantial cost advantage while maintaining comparable accuracy metrics (99% upper bound limits of 1.47 and 1.47° in axial and sagittal planes, respectively).
The 2D3D approach also demonstrates potential for substantial radiation exposure reduction compared to alternative navigation methodologies. The new technology we present negates the need for intra-op CT scans which likely reduces radiation. 18 While not directly comparable to conventional navigation methods, the 2D-3D system demonstrates significant potential for radiation reduction by minimizing fluoroscopic imaging requirements during spinal instrumentation. Each cadaveric spine required two low-dose fluoroscopic images for 2D-3D registration (mean 1.8 ± 0.2 exposures per specimen), yielding an estimated cumulative exposure of ≈ 1.2 mGy for the registration sequence about a 25 % reduction relative to conventional free-hand protocols that typically rely on multiple fluoroscopic acquisitions during screw placement. Because actual dosimetry was not recorded in this experiment, we acknowledge this as a limitation and recommend that future clinical studies include formal dose measurements to validate these preliminary estimates.
Furthermore, by merging 2D3D with augmented reality implementation, it addresses the attention shift requirement inherent in conventional navigation systems, where surgeons must redirect focus between the surgical field and remote displays. This integration of visualization and registration may contribute to the observed accuracy rates while potentially reducing cognitive load during complex procedures. 16 Unlike robotic navigation systems requiring fixed spatial relationships between tracking arrays and anatomical targets, our registration methodology demonstrates adaptability to intraoperative anatomical shifts through dynamic tracking of fiducial patient markers relative to the AR headset. The AR-HMD allows the surgeon more surgical and situational flexibility compared to rigid robotic navigation with preset trajectories. 11
Limitations & Future Considerations
The 2D3D registration approach represents an advancement in navigation technology by effectively integrating complementary imaging modalities while addressing radiation exposure, surgical time, and surgeon adaptability. Despite its innovation, several methodological aspects warrant consideration when interpreting these results. The cadaveric study design, while providing excellent control over experimental variables, cannot fully replicate the complexities of clinical settings, including tissue dynamics, patient movement, and intraoperative bleeding. Moreover, a larger sample size in real-life clinical setting would further validate accuracy in this registration method. Additionally, the controlled cadaveric environment may represent optimal conditions not always achievable in clinical practice. The predominantly male and advanced-age specimen demographics represent an inherent limitation in generalizability. Additionally, all participating surgeons had at least one year of navigation experience supplemented by specific training on the 2D-3D system. Further investigation is required to delineate the learning curve associated with this registration methodology compared to conventional techniques.
While our study validates the 2D-3D registration methodology for pedicle screw placement, further research should evaluate its application to more complex procedures such as interbody fusion or deformity correction. The convergence of technologies across robotics, imaging, optical tracking, and data processing suggests potential for synergistic integration that may further enhance surgical efficiency and safety.
Implementation of this technology in clinical practice will require comprehensive assessment of cost-effectiveness, workflow integration, and training requirements. Although our findings suggest favorable usability characteristics, formal evaluation of learning curves and training protocols will be essential for effective implementation. Prospective clinical trials with long-term outcome assessment will be necessary to determine whether the observed accuracy translates to improved clinical outcomes and reduced complication rates.
Conclusion
The 2D-3D registration methodology with augmented reality visualization demonstrates comparable accuracy to previously published intra-op CT modalities. This approach effectively addresses key limitations of existing navigation paradigms while maintaining high accuracy standards and potentially reducing radiation exposure. These findings suggest that AR-assisted navigation with 2D-3D registration represents a promising technological advancement that may enhance the precision and efficiency of spinal instrumentation procedures.
Footnotes
Ethical Considerations
Cadaveric testing was performed under Augmedics internal anatomical-research protocols DHF-VAR-000018 and DHF-VAR-000020.
Informed Consent
Donor specimens were obtained through the UC Davis Willed Body Program with documented informed consent for research use.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in-kind by Augmedics, including provision of the augmented reality navigation system, imaging equipment, and technical assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.