
Abstract
Study Design
Prospective controlled study.
Objectives
To evaluate the impact of an augmented reality (AR) visualization system on surgeon workload and ergonomics during endoscopic spine surgery, compared to conventional display monitors.
Methods
Ten experienced endoscopic spine surgeons (five neurosurgeons and five orthopedic surgeons; mean age 54 years) each performed 20 surgeries: the first 10 using traditional displays and the following 10 with a novel AR system. A step-by-step guide for AR system setup and utilization is provided. Workload was assessed using the NASA Task Load Index (NASA-TLX), and ergonomics were evaluated using the Rapid Upper Limb Assessment (RULA) score after each procedure. Paired t-tests or Wilcoxon signed-rank tests were used to compare traditional and AR systems, with normality assessed via the Shapiro-Wilk test.
Results
Use of the AR system resulted in significantly lower NASA-TLX scores, particularly in physical demand, effort, and performance domains (P < 0.001). RULA scores improved substantially, decreasing from a mean of 6.0 with traditional displays to 3.0 with AR (P < 0.001), indicating improved ergonomic posture. All surgeons demonstrated consistent reductions in perceived workload and ergonomic risk when utilizing the AR system.
Conclusions
Integration of an AR visualization system in endoscopic spine surgery significantly reduces cognitive workload and improves ergonomic posture compared to traditional displays. These findings suggest that AR technology may enhance surgical efficiency, promote surgeon well-being, and support the long-term sustainability of minimally invasive spinal procedures.
Introduction
Endoscopic surgery has gained increasing popularity and acceptance over the past 10 years. 1 Its high-quality imaging combined with minimal invasiveness has made it an attractive technique for spinal surgeons. 2 However, intraoperative orientation is a key factor in performing these procedures and remains one of the main challenges in the learning curve. 3 To address this, surgeons need access to a large amount of information: the patient’s CT scan, MRI, fluoroscopic images, and the video feed from the endoscopic camera. Additionally, in complex cases, a 3D reconstruction of the spine may be required, potentially necessitating up to five different displays simultaneously.
This setup makes achieving a comfortable and ergonomic environment in the operating room (OR) challenging. Video systems are expensive and require substantial physical space. To ensure versatility, high-definition displays must be mounted on supports that allow six degrees of movement and can be easily repositioned.
We developed a low-cost augmented reality (AR) system to improve ergonomics in the OR, displaying all necessary surgical information on virtual screens that can be easily adapted to the surgeon’s needs. This publication presents a comparison of ergonomics and workload between the AR system and conventional displays, accompanied by a step-by-step guide for its installation and setup.
Materials and Methods
Institutional Review Board (IRB) approval and informed consent were not required for this study, as no patient-specific data, interventions, or identifiable information were collected or analyzed. The study exclusively assessed surgeon-reported outcomes and observational ergonomic assessments during routine clinical practice, without altering standard surgical procedures or impacting patient care. All participating surgeons voluntarily agreed to provide workload and ergonomic data for research purposes.
Study Design and Participants
This was a prospective, controlled, within-subject study designed to compare the effects of an augmented reality (AR) visualization system vs traditional display monitors on surgeon workload and ergonomics during endoscopic spine surgery. Ten experienced endoscopic spine surgeons participated in the study, including five neurosurgeons and five orthopedic spine surgeons. The mean age of the participants was 54 years. All surgeons were proficient in uniportal endoscopic lumbar procedures and had performed more than 500 such cases prior to the study.
Surgical Protocol
Each surgeon performed a total of 20 lumbar endoscopic procedures. 10 surgeries were conducted using conventional high-definition two-dimensional monitors (control condition), and other 10 surgeries were performed using a novel AR visualization system, which projected the endoscopic feed directly into the surgeon’s field of view through a head-mounted display. The operated cases maintained a consistent level of complexity, all being classified as “Ia” according to the Endospine Academy chart. 4 All procedures were performed in a standardized operating room setup and under similar anesthetic protocols.
Headset Set-Up
The proposed system was designed to provide the surgeon with all the necessary information to perform effective and safe endoscopic procedures, even in anatomically complex cases. To achieve this, the headset received information in two different ways: • Patient images (MRI, CT, 3D models) were uploaded and opened directly on the headset using native software. • The endoscopic camera’s video feed was connected via cable to a computer, which then transmitted it over a Wi-Fi network to the headset through a screen mirroring system.
This information flow was summarized in Figure 1. A complete step-by-step guide was provided in Annex A. Information Flow in the AR System is Depicted. At the Top of the Diagram are the Connections Required to Wirelessly Receive the Endoscopic Camera’s Image on the Headset (X-ray Image is Optional). At the Bottom of the Diagram is the Preoperative Loading of Software and Medical Images onto the Headset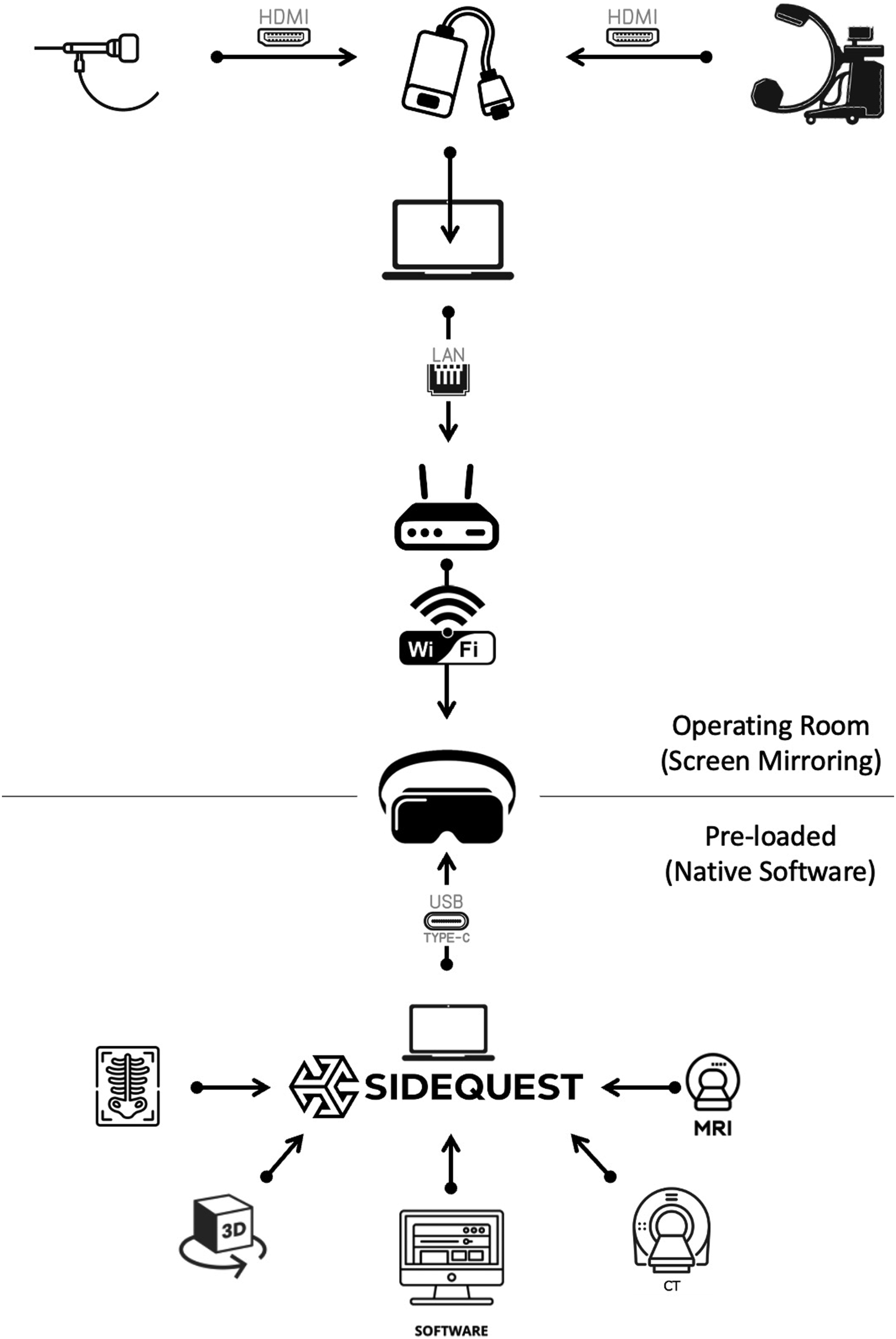
Headset Use
The headstrap was mounted and configured for headset AR usage. The distance between the headset and the surgeon’s face was adjusted to allow the use of prescription lenses. Since no Virtual Reality (VR) environment was employed, no light isolation mask was required, thereby also reducing the risk of VR-induced motion sickness. An image of the surgeon using the headset is shown in Figure 2. Intraoperative Use of the AR System. Note that the Surgeon’s Neck and Head Can Remain Neutral and Relaxed or Be Adjusted Without Relying on Physical Monitors
Although the headset may seem to obstruct the vision range, the AR system captures the surroundings using 4 different cameras. Figures 3 and 4 were captured from the headset, showing a clear view of the surgical environment. Different Virtual Display Setups are Shown. As Stated, Dimensions and Positions can be Freely Adjusted Without Limitations. In the Background of the Image, a Physical Reference Monitor Can be Seen AR 3D Model of the Patient’s Spine, Generated from a CT Scan. The Model can be Decomposed into Individual Vertebrae, and Both the Size and Position of Each Component Can be Adjusted as Needed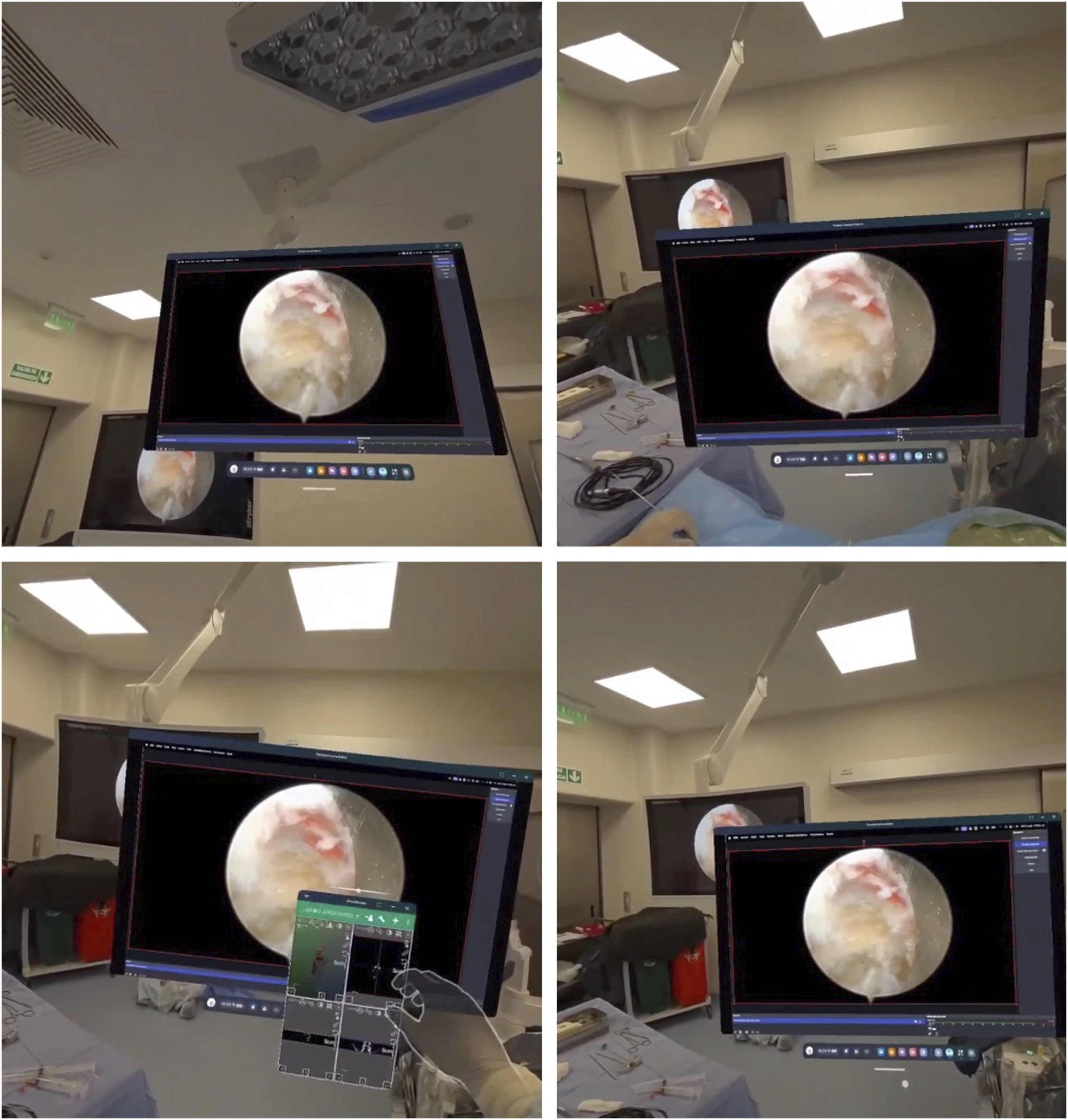

Outcome Measures
Workload Assessment
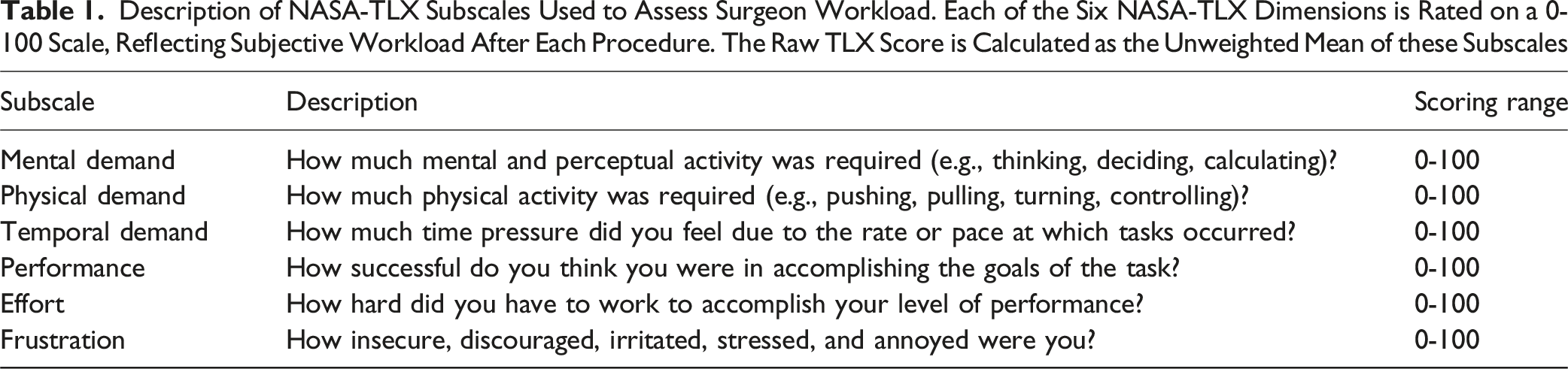
Description of NASA-TLX Subscales Used to Assess Surgeon Workload. Each of the Six NASA-TLX Dimensions is Rated on a 0-100 Scale, Reflecting Subjective Workload After Each Procedure. The Raw TLX Score is Calculated as the Unweighted Mean of these Subscales
Ergonomic Assessment
Ergonomic risk was evaluated using the Rapid Upper Limb Assessment (RULA),
6
a standardized observational tool that scores posture, force, and repetition to estimate biomechanical risk. RULA assessments were performed by an independent observer based on intraoperative pictures taken from 3 different angles (Figure 5), using a standardized scoring template. Scores ranged from 1 (minimal risk) to 7 (very high risk), with higher scores indicating poorer ergonomic conditions. RULA Score Measurements Using Intraoperative Pictures from Three Different Angles. A, B and C: Surgery Using Conventional Displays. D, E and F: Procedure Using the AR Device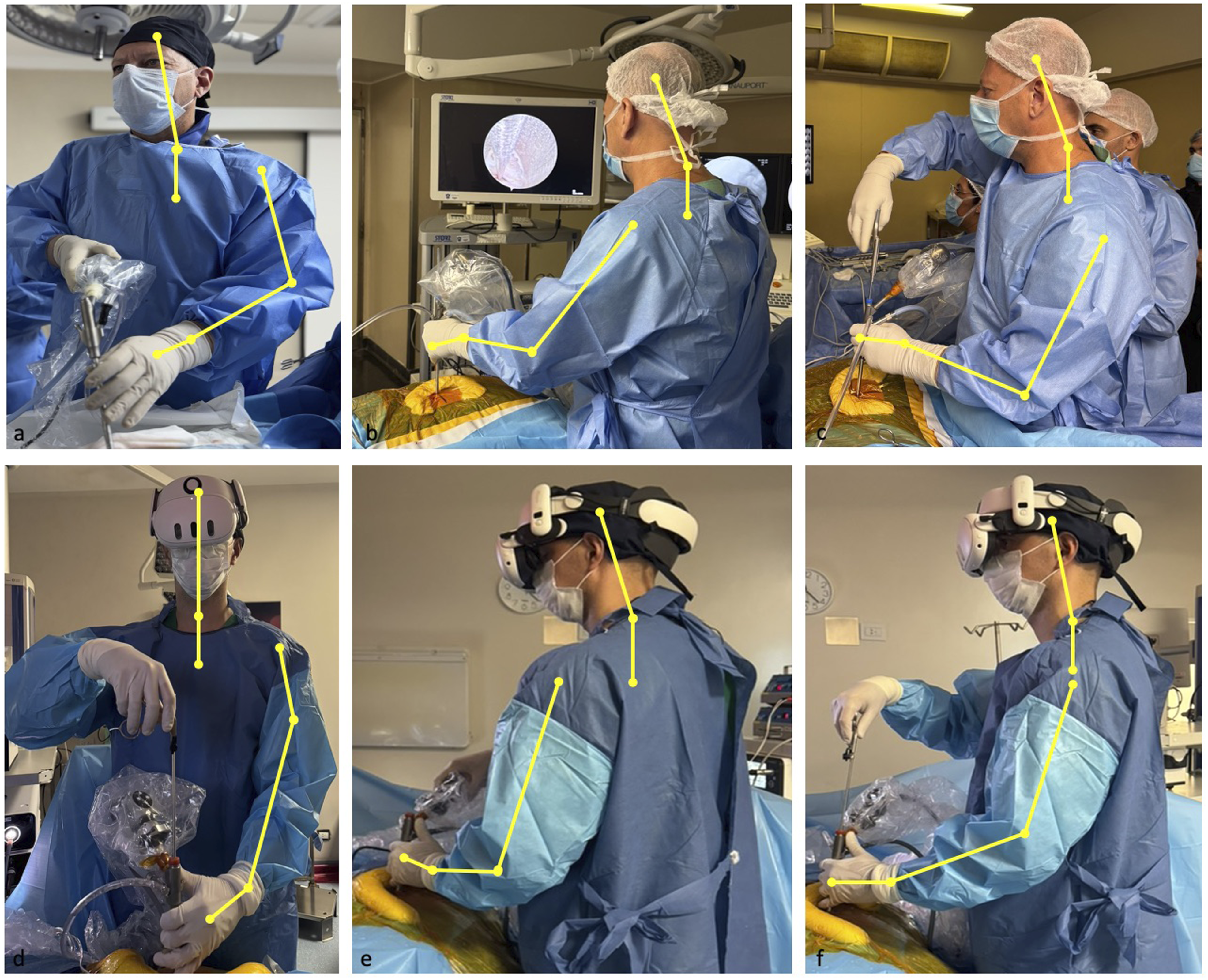
Statistical Analysis
For each surgeon, mean scores were calculated separately for the 10 surgeries performed under each condition (Traditional and AR). Paired statistical comparisons were conducted using the paired-sample t-test for normally distributed differences, and the Wilcoxon signed-rank test otherwise. Normality of the paired differences was assessed using the Shapiro-Wilk test. Descriptive statistics are presented as means ± standard deviations. All statistical tests were two-tailed, with a significance threshold set at P < 0.05.
Results
Surgical Procedures
All procedures performed in this study were single-level lumbosacral discectomies, corresponding to category IA in the Endospine Academy complexity classification. This ensured procedural homogeneity and minimized variability in workload and ergonomic demands. Intraoperative complications, including dural tears, neural injury, or instrument-related issues, were recorded but not observed in either group.
Operative time was recorded for each procedure. The mean duration for surgeries performed with traditional displays was 59.15 ± 6.75 min, while those performed with the AR visualization system averaged 60.21 ± 6.66 min. This difference was not statistically significant (P = 0.2651), indicating that surgical duration did not differ meaningfully between groups and was unlikely to have influenced the observed differences in workload or ergonomic outcomes.
Conventional Displays Results
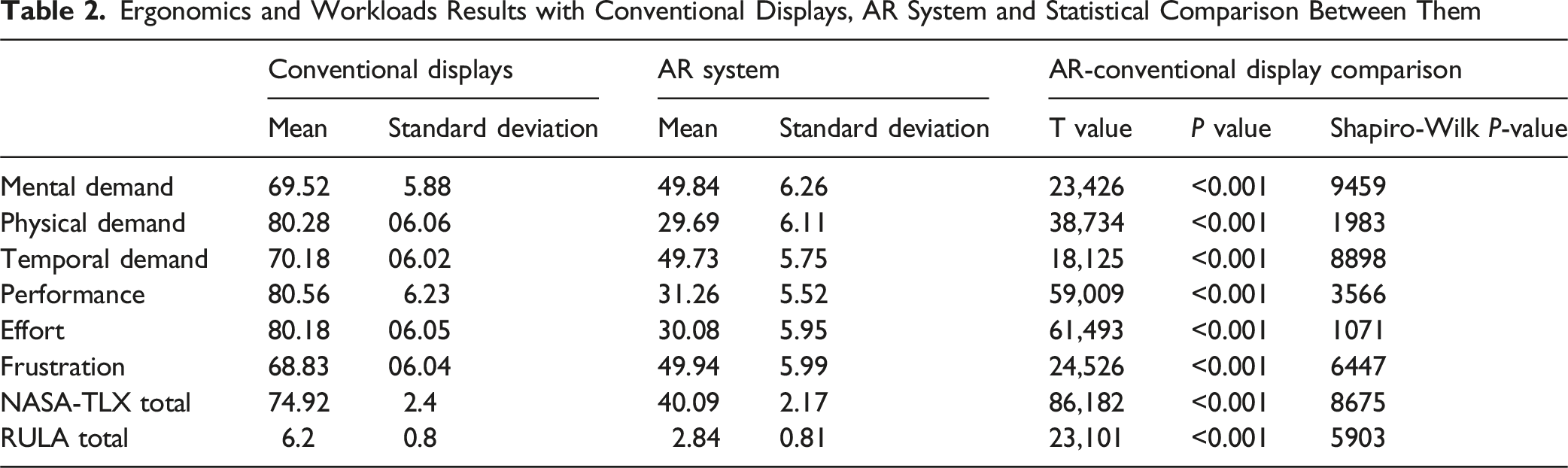
The 10 surgeries performed by each surgeon using conventional displays (100 surgeries total) showed consistently high workload and poor ergonomics. Mean values for NASA-TLX subscales were: Mental Demand = 69.5 ± 5.9, Physical Demand = 80.3 ± 6.1, Temporal Demand = 70.2 ± 6.0, Performance = 80.6 ± 6.2, and Effort = 80.2 ± 6.1. RULA scores reflected suboptimal posture with a mean of 6.0 ± 0.7. The mean total NASA-TLX (Raw-TLX) was 76.2 ± 4.9.
AR System Results
The mean setup time on the OR was 7 min. The setup was done while anesthetic induction was performed.
Compared to the conventional display results, the 100 surgeries performed with the AR visualization system demonstrated substantial improvements. The mean values for Mental Demand, Physical Demand, and Effort were markedly reduced to 49.8 ± 6.3, 29.7 ± 6.1, and 30.1 ± 6.0, respectively. Performance and Frustration scores also declined. RULA scores dropped significantly to a mean of 3.0 ± 0.8, indicating improved ergonomic posture. The mean total NASA-TLX dropped to 40.3 ± 4.9, underscoring a substantial reduction in perceived workload.
Conventional Display - AR System Comparison
To assess the impact of the AR visualization system on surgeon workload and ergonomics in each surgeon, we compared the mean values of NASA-TLX dimensions and RULA scores across two conditions: the 10 surgeries performed with conventional displays and the 10 surgeries performed with the AR system. Each surgeon served as their own control.
Normality of the paired differences was verified using the Shapiro-Wilk test for each variable. In all cases, the normality assumption was met (P > 0.05), justifying the use of paired sample t-tests. The AR system yielded statistically significant reductions across all workload dimensions—Mental Demand (P < 0.001), Physical Demand (P < 0.001), Temporal Demand (P < 0.001), Performance (P < 0.001), Effort (P < 0.001), and Frustration (P < 0.001)—as well as in the overall Raw NASA-TLX score.
Additionally, RULA scores were significantly lower under the AR condition (P < 0.001), indicating improved ergonomic posture.
Ergonomics and Workloads Results with Conventional Displays, AR System and Statistical Comparison Between Them
To assess inter-individual variability, we analyzed NASA-TLX and RULA scores separately for each surgeon. The improvement associated with the AR system was consistent across all 10 participants. These results are illustrated in Figure 6, which presents individual pre- and post-AR scores for each workload domain and ergonomic outcome. Surgeon-Specific Changes in NASA-TLX and RULA Scores Between Visualization Systems. Each Line Represents an Individual Surgeon’s Average Score under Traditional Display (Left) and Augmented Reality (AR) System (Right). Left Panel: NASA-TLX Total Workload Score. Right Panel: RULA Ergonomic Risk Score. A Consistent Reduction in Both Metrics is Observed Across All Surgeons When Using the AR System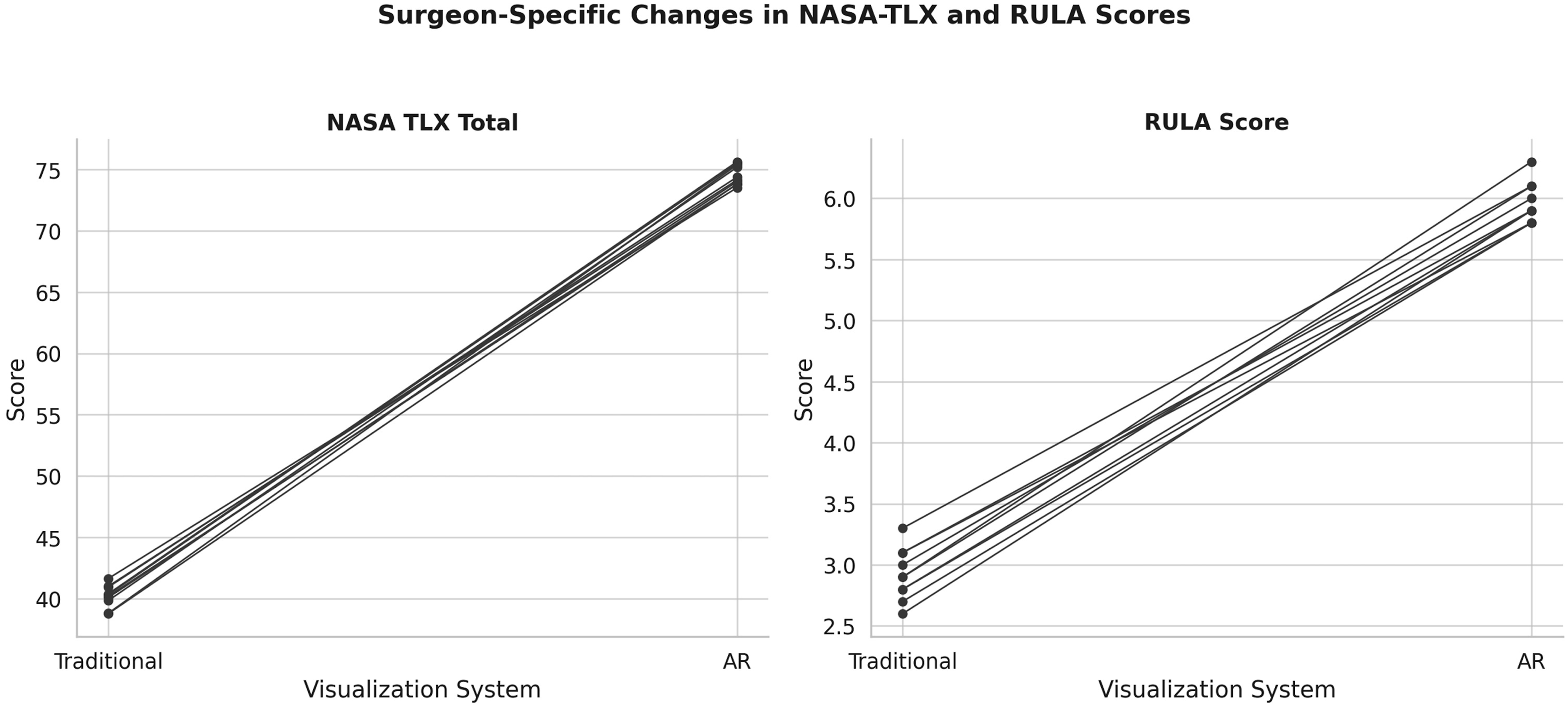
Discussion
Orthopedic arthroplasty surgery, a discipline that shares many characteristics with endoscopic spine surgery, has extensive experience using augmented reality technologies. The earliest applications focused on the usefulness of 3D models in education,7-9 enabling the transmission of complex concepts more effectively than 2D images. However, once the potential of this technology was established, its use expanded into daily practice10-12: surgical training, 13 analysis of complex fractures, 14 patient-physician communication,15,16 preoperative planning, image-assisted surgery,17,18 and remote peer-to-peer consultation. 19
Although there are significant differences between these two surgical fields, their similarities suggest that the lessons learned in orthopedic arthroplasty can serve as a starting point for applying AR in endoscopic spine surgery.
This study demonstrates the advantages of integrating AR technology into intraoperative settings. This novel application of AR in endoscopic spine surgery could allow surgeons to do the surgery comfortably and improve ergonomics, allowing the surgery to be done in optimal condition while having complete control over the information on virtual displays and virtual 3D objects.
Across all NASA-TLX workload dimensions, the use of AR led to a statistically significant reduction in perceived demand, particularly in the domains of physical demand, effort, and performance. These improvements suggest that the AR interface may alleviate the musculoskeletal strain and sustained attentional effort typically associated with endoscopic procedures using conventional displays.
The NASA Task Load Index (NASA-TLX) is a validated multidimensional tool widely used in high-stakes domains, including aviation and healthcare, to quantify subjective workload across six dimensions: mental demand, physical demand, temporal demand, performance, effort, and frustration. 5 In our study, surgeons consistently reported significantly lower NASA-TLX scores when utilizing the AR visualization system. These reductions were most pronounced in the physical demand, effort, and performance domains—dimensions that are particularly relevant to the repetitive and static postures inherent to endoscopic spine surgery. The reduction in mental and temporal demands, though more modest, further suggests that AR may contribute to a more intuitive and less cognitively taxing operative workflow. This supports the hypothesis that AR systems not only enhance visual-spatial awareness but also promote a more manageable cognitive load during complex procedures.
Neck pain in spine surgeons is a problem that cannot be emphasized enough. Spine surgeons frequently experience neck and musculoskeletal problems due to prolonged static postures and repetitive head movements during surgery. 20 There are reports of arthroscopic or endoscopic surgery having a negative impact on a surgeon’s neck pain.21,22 These ergonomic challenges are exacerbated by the need to alternate focus between surgical fields and external monitors for navigation. Augmented Reality (AR) technology through head-mounted displays (HMDs), can alleviate these issues by integrating critical visual data directly into the surgeon’s field of view. This innovation reduces the physical strain associated with conventional setups and promotes long-term occupational health for surgeons. Figure 3 and Video 1 demonstrate how the surgeon can easily arrange different setups using hand gestures: Dimensions and positioning of the virtual screens can be modified at will.
Importantly, the RULA scores—which reflect real-time posture and biomechanical load—demonstrated a marked improvement under the AR condition. The Rapid Upper Limb Assessment (RULA) is a standardized observational tool designed to assess biomechanical stress and posture-related risk factors for musculoskeletal disorders. 23 It is particularly sensitive to upper extremity, neck, and trunk alignment—areas commonly affected during minimally invasive spine procedures. In our cohort, mean RULA scores dropped significantly from approximately 6.0 under conventional display conditions to 3.0 with the AR system, indicating a shift from “high risk” to “low risk” ergonomic categories. This finding is critical, as previous literature has linked high RULA scores with increased incidence of cumulative trauma disorders among spine surgeons. By facilitating a more neutral head and neck position and minimizing lateral trunk rotation, the AR system appears to mitigate key ergonomic stressors that contribute to surgeon fatigue and occupational injury. These results advocate for the integration of ergonomic assessment tools like RULA into routine evaluation of surgical technologies.
The statistical robustness of these findings is further supported by the consistency of results across all 10 participating surgeons and the use of paired-sample t-tests, which confirmed that each individual experienced measurable benefit when transitioning to AR. These results align with previous studies in other surgical domains that have highlighted the potential of immersive and heads-up displays to reduce both physical and cognitive burdens in complex procedures.24-27 Collectively, these findings suggest that AR technology is not merely a visual aid but a transformative tool with the potential to redefine the ergonomic and cognitive landscape of endoscopic spine surgery. Further studies with larger samples and long-term follow-up are warranted to assess whether these intraoperative improvements translate into reduced fatigue, fewer occupational injuries, and improved surgical outcomes over time. However, these advantages have to be balanced with the discomfort and difficulties that the study participants reported: headset discomfort, image lagging, and difficulties with the AR interface. These problems were overcomed by different means: Headset discomfort was alleviated by adapting the headstrap to the individual surgeon. The selected head strap has a built-in fan system that cools the surgeon’s forehead, improving the surgeon’s experience in warm environments. Image lagging occurred when no dedicated WiFi network was created. Switching to a new, exclusive network solved the problem. Difficulties with the AR interface were noted, especially with the hand gestures to control the 3D model. Both this problem and headset discomfort diminished by the end of the study.
Although Endoscopic spine surgery is gaining popularity, it is also recognized for its steep learning curve, driven by the need for precise hand-eye coordination, spatial awareness, and instrument manipulation within limited anatomical spaces. 28 The AR can support surgeons in mastering these skills by providing real-time augmented overlays of the surgical field. These overlays enhance spatial understanding and assist in navigating complex anatomy. Unlike traditional 2D imaging, which requires mental reconstruction of anatomical structures, AR/MR allows for immersive visualization of 3D models of the spine. This leads to improved recognition of key anatomical landmarks, facilitating precise identification of pathology needed to be handled. Figure 4 and Video 2 show the 3D model of a patient’s spine, generated from a CT scan and used intraoperatively to guide the surgeon. While there are existing experiences using physical 3D models printed in resin for similar purposes, AR technology enables the model to be separated into individual pieces with a simple hand gesture, adjust vertebra size at will, and remove it from the field of view once it is no longer needed.
One of the standout features of AR is its potential for remote collaboration. Surgeons can share their augmented view of the surgical field with colleagues in different locations, enabling real-time consultation and decision-making. Furthermore, this approach improves access to advanced surgical techniques, allowing surgeons in resource-limited settings to benefit from global expertise.
AR systems are becoming increasingly affordable as technology evolves. Unlike traditional navigation systems that require substantial capital investment in hardware and software, many AR platforms can leverage commercially available devices, such as head-mounted displays (HMDs). The setup presented in the current publication costs under 1.000 United States Dollars. This lower cost of entry makes this technology more accessible to a wider range of healthcare facilities, including smaller hospitals or resource-limited settings.
We believe that the future of AR in endoscopic spine surgery will center on workflow optimization and technological refinement.
29
Key areas for development include: 1. Seamless Integration: Enhancing the usability of AR systems by automating processes such as image registration and calibration to reduce intraoperative setup times. 2. Dedicated Applications: Creating specialized applications tailored to spine surgery, including dynamic anatomy visualization, automated pathology identification, and real-time surgical guidance. 3. Enhanced Accuracy: More validation studies are required to ensure the precision and reliability of AR platforms in real-world surgical settings. 4. Instrument Tracking: Integration with advanced tracking systems to monitor surgical instruments within the augmented field, improving accuracy in complex anatomy or advanced procedures. 5. Surgical training: AR serves as an invaluable tool for surgical education. Trainees can practice complex procedures in a virtual or augmented environment. By integrating AR into training programs, residents and fellows can better understand surgical techniques and anatomy. 6. AI Integration: Leveraging artificial intelligence to provide intraoperative decision-support features, transforming endoscopic spine surgery into an even more precise surgery.
Limitations
This study has several limitations that reduce the generalizability of the results. Although it included 200 procedures in total, the number of participants was low, which may affect the generalizability of the findings. Additionally, both NASA-TLX and RULA rely on subjective or observational data, which may be influenced by user expectations or assessment variability. Finally, while the study demonstrates intraoperative benefits, it did not evaluate long-term clinical outcomes or occupational health impacts, which merit further investigation.
While the improvement in cervical posture with the AR head-mounted display was anticipated and supported by the data, we acknowledge that RULA scores—particularly those reflecting upper limb posture—may also be influenced by external factors such as instrument positioning, table height, or operating room configuration. Although these variables were standardized as much as possible, they represent a potential source of variability that should be considered when interpreting upper limb ergonomics.
Conclusion
Augmented Reality (AR) technology is now widely accessible and offers a valuable addition to spine surgery practice. This study demonstrates that integrating an AR visualization system in endoscopic spine surgery significantly reduces both perceived workload and ergonomic strain compared to conventional displays. Surgeons reported lower NASA-TLX scores, particularly in physical demand, effort, and performance, alongside improved RULA scores, indicating better postural ergonomics. These findings suggest that AR enhances the surgical environment by promoting safer posture, reducing cognitive and physical burden, and potentially improving surgeon well-being and procedural sustainability. Further research is needed to evaluate its long-term impact on clinical outcomes and occupational health.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material - Low-Cost Augmented Reality System in Endoscopic Spine Surgery: Analysis of Surgeon Ergonomics, Perceived Workload and A Step-by-Step Guide for Implementation
Supplemental Material for Low-Cost Augmented Reality System in Endoscopic Spine Surgery: Analysis of Surgeon Ergonomics, Perceived Workload and A Step-by-Step Guide for Implementation by Facundo Van Isseldyk, Piya Chavalparit, Julio Bassani, Lisandro Rodriguez Sattler, Marcus Serra, Jefferson Leal, Cristian Correa Valencia, Alberto Gotfryd, Jeronimo Milano, Alfredo Guiroy, and Jin Sung Kim in Global Spine Journal in Global Spine Journal
Footnotes
Acknowledgments
This study was organized by the AO Spine Latin America Minimally Invasive Spine Study Group. AO Spine is a clinical division of the AO Foundation, which is an independent, medically-guided, non-profit organization. Study support was provided directly through AO Spine Latin America for data collection, data analysis, and proofreading.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Competing Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jin Sung Kim serves as consultant for RIWOSpine, (GmbH, Germany), Nexon Medical AG, (Switzerland), and Elliquence, LLC (USA).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.